
Abstract
Background
Health service providers should understand and attend to the health literacy needs of their population in view of the known association between low health literacy and poorer health outcomes. This study aimed to determine the health literacy profile of patients treated at a large private hospital in Melbourne, Australia, and any associations between this profile and socio-economic position, health behaviours, health status and use of hospital services.
Methods
A mailed survey was sent to 9173 people aged ≥18 years with a hospital admission between February and October 2014. It included the Health Literacy Questionnaire (HLQ), a multidimensional tool comprising nine independent scales, and socio-demographic and clinical questions. For both respondents and non-respondents, we also extracted residential postcode and admission and follow up details from the Patient Administrative Services database. Differences in demographic, socio-economic and hospital use patterns between respondents and non-respondents were analysed using descriptive statistics. Regression-tests were used to identify differences in health literacy between socio-economic subgroups, with the magnitude of these differences determined using Cohen’s d effect sizes.
Results
There were 3121 respondents (response rate: 35% excluding 154 returned invitations), the majority born in Australia (74.6%) and living in areas of high socio-economic advantage. Respondents were slightly older than non-respondents (mean (SD) age 65.6 (17.0) versus 60.6 (20.8) years) and included proportionately less females (51.9 versus 59.1%) but were similar with regard to other socio-demographic factors and health service use. Participants who did not speak English at home, reported lower scores across several HLQ scales, including those that measure health provider support and engagement. Those who smoked and reported low physical activity had lower scores for actively managing their health. No relationship was seen between HLQ scale scores and use of hospital services.
Conclusions
Based upon the health literacy profile of a large cohort of patients attending a large private hospital, we found no relationship between HLQ scale scores and use of hospital services. However we did identify significant health literacy needs particularly among patients whose primary language at home was not English and patients needing assistance completing the survey. Identifying ways of addressing these needs may improve patient outcomes.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Adopting mechanisms to measure and address the health literacy needs of patients is becoming an increasingly important component of patient care, particularly in the hospital setting where patients may struggle with navigating the complexities of multi-disciplinary care [1,2,3]. This change is being driven by the large body of research that has demonstrated the impact of an individual’s health literacy on their health outcomes and use of health care services. For example, low scores on instruments that test functional health literacy (an individual’s ability to read and comprehend health information with or without numeracy skills relating to health information), have been shown to be moderately associated with increased risk of hospital admission [4,5,6] re-presentation within 30 days [7], and increased emergency department (ED) presentations [6, 8, 9]. Low functional health literacy has also been associated with less use of preventive healthcare services [10], poorer ability to self-manage chronic diseases [11,12,13,14,15], and poorer health outcomes including increased mortality [11, 16,17,18].
However health literacy is a multifaceted concept that encompasses all aspects related to a person’s ability to find and use health information and navigate the healthcare system [19]. In its broadest sense, it is defined as ‘the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health’ [20]. This definition indicates the complex nature of health literacy which is influenced by a complex interaction of contextual factors including cultural and personal values, social resources, and individual motivations in addition to their functional health literacy that all influence an individual’s capacity to comprehend and act upon information related to their health.
Advancements in the field have led to the development of new measurement tools that better reflect the wider concept of health literacy, including the European Health Literacy Survey Questionnaire [21], the Swiss Health Literacy Survey [22], the Health Activities Literary Scale [23], the Critical Health Competence Test [24], and the Health Literacy Questionnaire (HLQ) [25]. The HLQ, developed in 2013, includes nine different dimensions of health literacy and its construct validity and reliability have been demonstrated in several contexts [25,26,27,28]. The nine independent scales of the HLQ generate a health literacy profile that provides detailed information about an individual’s health literacy skills and deficiencies. Use of the tool within a health service can therefore provide insights into their specific population’s health literacy needs, and help to generate actionable ideas to address them.
We recently reported on the health literacy profile of patients attending a public hospital in a low socio-economic area of Melbourne, Australia [29]. The present study was performed concurrently and its purpose was to better understand the health literacy needs of patients treated at a large private hospital in a high socio-economic area of Melbourne, Australia. The primary aim was to determine the health literacy profile of a large cohort who had been treated as inpatients using the HLQ. A second aim was to determine the associations between an individual’s health literacy, and their socio-economic position, health behaviours and health status, and their use of hospital services.
Methods
We invited 9173 patients who had been discharged from Cabrini Hospital, Malvern, a 508-bed private not-for-profit acute care hospital to participate in a mailed survey. The hospital is located in southeast Melbourne and delivers emergency, maternity, coronary care, intensive care and paediatric inpatient services. The hospital’s catchment is considered to be a population of advantage, with higher levels of income and educational attainment compared with the State of Victoria’s averages [30].
Data collection took place over 9 months from February to October 2014. Eligible patients were identified through the Patient Administrative Services (PAS) database each month. Patients were eligible to receive a survey if they had been admitted for at least 24 h in the past 30 days, aged 18 years or over, and not discharged with a diagnosis of dementia or to palliative or hospice care. In the first month, a computer generated random sample of 50 patients were sent surveys to pilot test the process. This was followed by 100 patients in the second month. From April to September, all hospitalised individuals who met the eligibility requirements were sent surveys. Overall, a total of 9173 surveys were sent.
To maximise response rates, eligible recently discharged patients were sent a pre-notification letter informing them about the survey. One week later, they were sent a personalised cover letter instructing them about the purpose of the study, the information and consent form, the survey and a reply-paid envelope. Non-respondents were sent a reminder 3 weeks after the first survey was sent. Letters explained that the survey was being conducted to help improve the standard of care at the hospital and were co-signed by the hospital’s Chief Executive Officer and the Principal Investigator (RB). They also encouraged participants to complete the survey themselves, or with help if needed. All participants were allocated a unique study ID. No information from this study was included in the patients’ medical record. Reasons for non-participation were recorded where known.
Measures
Health literacy questionnaire (HLQ)
The HLQ has 44 items covering nine domains of health literacy captured in nine independent scales: 1. Feeling understood and supported by healthcare providers, 2. Having sufficient information to manage my health, 3. Actively managing my health, 4. Social support for health, 5. Appraisal of health information, 6. Ability to actively engage with healthcare providers, 7. Navigating the healthcare system, 8. Ability to find good health information, and 9. Understanding health information well enough to know what to do.
Each scale consists of between four and six items. The first five scales are scored from 1 (strongly disagree) to 4 (strongly agree). The last four scales scored from 1 (cannot do or always difficult) to 5 (very easy). Scales are scored independently by adding the scores for each item within the scale, and dividing by the number of items within the scale.
Socio-demographic, health and hospital use variables
Self-reported socio-demographic data were collected for age, sex, height, weight, living arrangements, Aboriginal and Torres Strait Islander status, country of birth, whether or not English was the primary language spoken at home, education level, work status, internet usage, private health insurance status, household income, government benefits (if applicable), alcohol consumption, smoking status, physical activity levels, pre-existing health conditions, self-reported Emergency Department (ED) presentations in the last 12 months, and whether or not the participant had help completing the survey.
For both respondents and non-respondents, we extracted data from the PAS database including admission source, admission type, discharge destination, hospital length of stay, ED presentations and hospital admissions to any Cabrini Health acute hospital facility (Malvern or Brighton) in the 12 months following the index admission. Residential postcode was also extracted to determine Index of Relative Socio-economic Disadvantage (IRSD) status related to home address. This index is produced by the Australian Bureau of Statistics as part of the Socio-Economic Index for Areas (SEIFA) and ranks areas in Australia into deciles using census data according to relative socio-economic advantage and disadvantage [31]. Scores range from 1 to 10 with lower scores indicating more disadvantage than other areas of Australia.
Ethical considerations
Ethical approval was obtained from both the Cabrini Human Research Ethics Committee (EC00239) and the Monash University Human Research Ethics Committee (EC00234). In order to avoid potential harm or embarrassment to participants, ensure unbiased response, and maximise the response rate, the term ‘literacy’ was not used in communications with participants. A previous qualitative study of low literacy individuals found that the expression discourages individuals with low literacy from engaging in healthcare experiences and results in persistent anxiety regarding their literacy difficulties [32]. As this was a study assessing patient’s (health) literacy, participants were encouraged to complete the documents with assistance if necessary to ensure that all participants, including those with impaired literacy, clearly understood the study and could therefore provide fully informed consent.
All respondents provided written informed consent. We also requested consent to access respondents’ hospital records. Where consent was obtained we extracted re-identifiable information. For respondents who did not provide consent for their hospital records to be reviewed, and for non-respondents, only non-identifiable data were extracted. Consent for de-identified data for respondents who did not consent for their hospital records to be reviewed, and for non-respondents was deemed unnecessary by the Cabrini Human Research Ethics Committee.
Statistical analysis
Data were analysed using Stata 13 (Stata Corp). Missing values for the HLQ were imputed as described by Beauchamp et al. [33]. To determine whether survey respondents differed from non-respondents, Kruskall Wallis or t-tests, depending on data type and distributional characteristics, were used to examine differences in demographic, socio-economic and hospital use patterns between respondents and non-respondents.
For respondents who agreed to medical record access, Pearson chi-square tests were used to determine whether there were associations between health literacy and demographic, socio-economic, and hospital use variables. Where differences were found, Cohen’s d effect sizes were calculated to describe the magnitude of differences in HLQ scores and interpreted as a ‘small’ effect size if Cohen’s d was > 0.20–0.50, ‘medium’ effect size if 0.50–0.80, and ‘large’ effect size for results > 0.80 [34].
Results
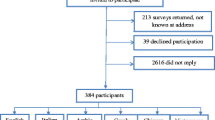
A total of 9173 surveys were sent (refer to Fig. 1). Of these, 154 were returned as the patient had died or the address was incorrect. A total of 3118 patients responded to the survey (response rate excluding non-contactable patients was 35%) and of these, 2374 (76%) consented to review of their medical records.

Recruitment process for health literacy cross sectional survey
Table 1 compares respondents and non-respondents. Respondents were older (mean age 65.6 versus 60.6 years), and proportionately less females responded (51.9% versus 59.1%). There were no significant differences between respondents and non-respondents with regard to language spoken at home, IRSD deciles (9 IQR 8, 10), length of stay, or ED presentations in the 12 months following the index hospital admission, but more respondents were readmitted to hospital in the 12 months following the index admission (37.9% versus 32.6%).
More than half (52%) of respondents were retired and most (86%), were on an annual income greater than $30,000 (Table 2). Most (78%) had at least one longstanding illness or disability, and 12% had four or more chronic conditions. Almost half (47%) had completed a tertiary education qualification and nearly all (95%) had private health insurance. Eight percent (N = 242) required assistance in completing the survey due to either physical disability or difficulties with comprehension. Study population mean scores for each HLQ scale are shown in Table 3. The lowest score was reported for ‘Appraisal of health information’ (mean (SD): 2.85 (0.53), score range 1 to 4) and the highest score was reported for ‘Understanding health information well enough to know what to do’ (mean (SD) 4.11 (0.58), score range 1 to 5).
Table 4 displays the socio-demographic, health and hospital use variables and their association with the nine scales of the HLQ. The largest effect size for difference in means was found for those that needed assistance with completing the survey, with large effect sizes found for those requiring assistance compared to those not requiring assistance for the scales ‘Finding health information’ and ‘Understanding health information well enough to know what to do;’, and small effect sizes found for ‘Actively managing my health’, ‘Appraisal of health information’, and ‘Social support for health’. Speaking a language other than English at home was associated with the largest number of health literacy scales, with those who did not speak English at home having significantly lower scores (small to medium effect sizes), than those who spoke English, for the scales ‘Health care provider support’, ‘Having sufficient information’, ‘Active engagement with healthcare professionals’, ‘Ability to find good health information’, and ‘Understanding health information well enough to know what to do’.
The scales where the largest number of differences in subgroups across socio-demographic variables were seen were ‘Ability to find good health information’ and ‘Understanding Health information well enough to know what to do’. Not speaking English at home, being unemployed, not having a tertiary qualification, receiving government benefits, having a household income less than $30,000, using the internet less than daily, having four or more chronic health conditions, and requiring assistance with the survey were all associated with lower reported scores for ‘Ability to find good health information’. With the exception of employment status, these variables also resulted in lower scores for ‘Understanding health information well enough to know what to do’.
Current smokers and/or individuals who recorded doing less than 3.5 h of physical activity per week were more likely to report lower scores for ‘Actively managing health’ compared with non-smokers and physically active individuals. Current smokers, as well as those who live alone, were also more likely to report lower ‘Social support for health’ compared with non-smokers and those who lived with others respectively. We found no relationship between HLQ scale scores and length of stay or further hospital admissions and ED presentations in the year following the index admission.
Discussion
This study describes the health literacy profile of a large cohort of patients discharged from a large private hospital in a high socio-economic area of metropolitan Melbourne. Despite living in areas of significant socio-economic advantage and high education attainment, we identified significant health literacy needs in this patient population. In particular, respondents who spoke a primary language other than English at home, and those who needed help to complete the survey, were found to have the largest number of low scores across HLQ scales. However, there was no association between greater use of hospital services and lower health literacy scores across any of the nine HLQ scales.
Our study agrees in part with previous studies that have found that socio-economic factors (low educational attainment and low income), are associated with lower levels of health literacy as measured by functional health literacy tools [35,36,37]. We found that respondents who were unemployed, with very low household incomes, and those without a completed tertiary qualification, to have significantly lower scores across some health literacy scales. However, we also found that poor health behaviours (low levels of physical activity and smoking), using the internet less than once a day, living alone, speaking a language other than English, requiring assistance to fill in the survey, and being male, were all also associated with lower scores in some scales on the health literacy questionnaire.
The strong association between speaking a primary language other than English at home and having lower scores across a number of health literacy scales has been described in previous studies [33, 36, 38]. Our research provides insight into areas of health literacy difficulty that go beyond poor reading comprehension and numeracy skills for health-related materials, and identifies that these individuals experience challenges navigating the healthcare system, and in feeling meaningfully engaged with healthcare providers. Population-based surveys have found that an individual’s health care provider is their most frequently used and most trusted source of health information [39,40,41]. Poor or no relationships with health care providers could therefore impact significantly on an individual’s access to information about their condition and their ability to manage it effectively. This suggests that ensuring that all patients with non-English backgrounds have strong relationships with at least one health care provider, and strategies to improve the navigability of the health care system, are likely to be important ways of addressing their health literacy needs.
While our finding of no association between lower health literacy scores and increased use of hospital services is in agreement with findings from a previous survey using the HLQ in a cohort of Australian public hospital patients [29], it contrasts with much of the previous research [4,5,6,7,8, 42]. There are a number of possible explanations for these discrepancies. Most of the earlier studies have used functional health literacy instruments to investigate any association between hospital service utilisation and health literacy. Our use of a multidimensional instrument that measures ability and needs separately across the different scales demonstrate that self-reported strengths in some aspects of health literacy may compensate for deficiencies in other scales. For example, it is possible that good social support like a partner with high health literacy skills, and/or strong engagement with health professionals, may compensate for an individual’s poor reading comprehension skills, resulting in sufficient capacity to self-manage without an increased need of health services. We also found that Individuals requiring assistance to fill in the survey reported greater levels of social support for health, but reported feeling less engaged with health care providers. This suggests that social support for health may be critical for helping people with low literacy skills access and engage with the healthcare system.
Strengths of our study include the very large sample size and minimal differences between respondents and non-respondents, indicating that our results are likely to be generalisable to the private hospital’s patient population. On the other hand, while we tried to reduce the risk of a biased response by not mentioning literacy in the survey invitation, those with low literacy and/or health literacy may have been less inclined to participate, which may have resulted in an overestimate of the health literacy of this population. Further, those who spoke a language other than English at home were not provided surveys in their language of origin, and this may have also influenced the way the surveys were filled out, as well as the response rate in patient group.
The early conceptualisation of health literacy as an individual’s ability to read and comprehend written health-related materials has led to a belief that it is a relatively unmodifiable ‘condition’. Most interventions directed to people with lower levels of health literacy have therefore focused on strategies that compensate for, rather than improve health literacy (such as simplifying written health information) [16, 43]. Recently, research has identified the attributes of organisations that provide services which respond to individuals with different health literacy needs [2, 44]. Future research should now focus on determining whether development of these organisation attributes, in combination with targeted approaches to address the specific health learning needs of the individual (in the context of each individual’s learning style, language and preferences), lead to improvements in patient and carer health literacy.
Conclusions
Our study has determined the health literacy profile of a large cohort of patients attending Cabrini Hospital, a large private not-for-profit hospital in Melbourne, Australia. Despite high socio-economic backgrounds, we found that those who did not speak English at home, those who required assistance completing the survey, those who lived alone, those who do not use the internet each day, and those presenting with poorer health behaviours (smoking and low physical activity), exhibited specific health literacy needs. We plan to present these data to Cabrini Health stakeholders (patients, staff and management) to elicit ideas for how the hospital can address these health literacy needs. For example the HLQ or selected scales could be included in the standard pre-admission form, health literacy could be integrated into pathway planning, and relevant staff may be required to complete a mandatory health literacy e-learning module.
Abbreviations
- ED:
-
Emergency Department
- HLQ:
-
Health Literacy Questionnaire
- IRSD:
-
Index of Relative Socio-economic Disadvantage
- PAS:
-
Patient Administrative Services
References
Australian Commission on Safety and Quality in Health Care. Health literacy. Taking action to improve safety and quality. Sydney: ACSQHC; 2014.
Brach C, Keller D, Hernandez L, Baur C, Parker R, Dreyer B, Schyve P, Lemerise A, Schillininger D. Attributes of a health literate organization. Washington, DC: Institute of Medicine; 2014.
Brega A, Barnard J, Mabachi N, Weiss B, DeWalt D, Brach C, Cifuentes M, Albright K, West D. AHRQ health literacy universal precautions toolkit. 2nd ed. Rockville: Agency for Healthcare Research and Quality; 2015.
Baker DW, Gazmararian JA, Williams MV, Scott T, Parker RM, Green D, Ren J, Peel J. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. Am J Public Health. 2002;92:1278–83.
Baker DW, Parker RM, Williams MV, Clark WS. Health literacy and the risk of hospital admission. J Gen Intern Med. 1998;13:791–8.
Cho Y, Lee S, Arozullah A, Crittenden K. Effects of health literacy on health status and health service utilization amongst the elderly. Soc Sci Med. 2008;66:1809–16.
Mitchell SE, Sadikova E, Jack BW, Paasche-Orlow MK. Health literacy and 30-day Postdischarge hospital utilization. J Health Commun. 2012;17:325–38.
Green J, Mor M, Shields A, Sevick M, Arnold R, Palevsky P, Fine M, Weisbord S. Associations of health literacy with dialysis adherence and health resource utilization in patients receiving maintenance hemodialysis. AKJD. 2013;62:73–80.
Hope C, Wu J, Tu W, Young J, Murray M. Association of medication adherence, knowledge, and skills with emergency department visits by adults 50 years or older with congestive heart failure. Am J Health Syst Pharm. 2004;61:2043–9.
Scott TL, Gazmararian JA, Williams MV, Baker DW. Health literacy and preventive health care use among Medicare enrollees in a managed care organization. Med Care. 2002;40:395–404.
Baker DW, Wolf MS, Feinglass J, Thompson JA, Gazmararian JA, Huang J. Health literacy and mortality among elderly persons. Arch Intern Med. 2007;167:1503–9.
Peterson PN, Shetterly SM, Clarke CL, Bekelman DB, Chan PS, Allen LA, Matlock DD, Magid DJ, Masoudi FA. Health literacy and outcomes among patients with heart failure. JAMA. 2011;305:1695–701.
Sudore RL, Yaffe K, Satterfield S, Harris TB, Mehta KM, Simonsick EM, Newman AB, Rosano C, Rooks R, Rubin SM. Limited literacy and mortality in the elderly: the health, aging, and body composition study. J Gen Intern Med. 2006;21:806–12.
von Wagner C, Steptoe A, Wolf MS, Wardle J. Health literacy and health actions: a review and a framework from health psychology. Health Educ Behav. 2009;36:860–77.
Devraj R, Herndon C, Griffin J. Pain awareness and medication knowledge: a health literacy evaluation. J Pain Palliat Care Pharmacother. 2013;27:19–27.
Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97–107.
Bostock S, Steptoe A. Association between low functional health literacy and mortality in older adults: longitudinal cohort study. BMJ. 2012;344:1602.
DeWalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy and health outcomes: a systematic review of the literature. J Gen Intern Med. 2004;19:1228–39.
Nutbeam D. The evolving concept of health literacy. Soc Sci Med. 2008;67:2072–8.
Stasinopoulos D, Stasinopoulos I, Pantelis M, Stasinopoulou K. Comparison of effects of a home exercise programme and a supervised exercise programme for the management of lateral elbow tendinopathy. Br J Sports Med. 2010;44:579–83.
Sørensen K, Van den Broucke S, Pelikan JM, Fullam J, Doyle G, Slonska Z, Kondilis B, Stoffels V, Osborne RH, Brand H. Measuring health literacy in populations: illuminating the design and development process of the European health literacy survey questionnaire (HLS-EU-Q). BMC Public Health. 2013;13:948.
Wang J, Thombs BD, Schmid MR. The Swiss health literacy survey: development and psychometric properties of a multidimensional instrument to assess competencies for health. Health Expect. 2014;17:396–417.
Rudd RR, Kirsch I, Yamamoto K. Literacy and health in America. Princeton: Educational Testing Service; 2004.
Steckelberg A, Hülfenhaus C, Kasper J, Rost J, Mühlhauser I. How to measure critical health competences: development and validation of the critical health competence test (CHC test). Adv Health Sci Educ. 2009;14:11–22.
Osborne RH, Batterham RW, Elsworth GR, Hawkins M, Buchbinder R. The grounded psychometric development and initial validation of the health literacy questionnaire (HLQ). BMC Public Health. 2013;13:658.
Morris RL, Soh S-E, Hill KD, Buchbinder R, Lowthian JA, Redfern J, Etherton-Beer CD, Hill A-M, Osborne RH, Arendts G, Barker AL. Measurement properties of the health literacy questionnaire (HLQ) among older adults who present to the emergency department after a fall: a Rasch analysis. BMC Health Serv Res. 2017;17:605.
Kolarcik P, Cepova E, Madarasova Geckova A, Elsworth G, Batterham R, Osborne R. Structural properties and psychometric improvements of the health literacy questionnaire in a Slovak population. Int J Public Health. 2017;62:591–604.
Maindal H, Kayser L, Norgaard O, Bo A, Elsworth G, Osborne R. Cultural adaptation and validation of the health literacy questionnaire (HLQ): robust nine-dimension Danish language confirmatory factor model. Springerplus. 2016;5:1232.
Jessup RL, Osborne RH, Beauchamp A, Buchbinder R. Health literacy of recently hospitalised patients: a cross-sectional survey using the health literacy questionnaire (HLQ). BMC Health Serv Res. 2017;17:52.
State Government of Victoria: Index of relative socioeconomic disadvantage. 2015. http://stat.data.abs.gov.au/Index.aspx?DataSetCode=ABS_SEIFA_LGA. Accessed 23 Mar 2017.
Australian Bureau of Statistics: A Socio-Economic Indexes for Areas. 2011. http://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa. Accessed 23 Mar 2017.
Easton P, Entwistle VA, Williams B. How the stigma of low literacy can impair patient-professional spoken interactions and affect health: insights from a qualitative investigation. BMC Health Serv Res. 2013;13:319.
Beauchamp A, Buchbinder R, Dodson S, Batterham RW, Elsworth GR, McPhee C, Sparkes L, Hawkins M, Osborne RH. Distribution of health literacy strengths and weaknesses across socio-demographic groups: a cross-sectional survey using the health literacy questionnaire (HLQ). BMC Public Health. 2015;15:678.
Lenhard W, Lenhard A. Hypothesis Tests for Comparing Correlaions. 2014. https://www.psychometrica.de/correlation.html. Accessed 18 Jan 2017.
Curtis LM, Wolf MS, Weiss KB, Grammer LC. The impact of health literacy and socioeconomic status on asthma disparities. J Asthma. 2012;49:178–83.
Howard DH, Sentell TL, Gazmararian JA. Impact of health literacy on socioeconomic and racial differences in health in an elderly population. J Gen Intern Med. 2006;21:857–61.
Kim S, Knight S, Tomori C, Colella K, Schoor R, Shih L, Kuzel T, Nadler R, Bennett C. Health literacy and shared decision making for prostate cancer patients with low socioeconomic status. Cancer Investig. 2001;19:684–91.
Sentell TL, Halpin HA. Importance of adult literacy in understanding health disparities. J Gen Intern Med. 2006;21:862–6.
Burns P, Jones S, Iverson D, Caputi P. Where do older Australians receive their health information? Health information sources and their perceived reliability. J Nurs Educ Pract. 2013;3:60–9.
Cotten SR, Gupta SS. Characteristics of online and offline health information seekers and factors that discriminate between them. Soc Sci Med. 2004;59:1795–806.
Fox S. The social life of health information. Washington, DC: Pew International & American Life Project; 2011.
Vandenbosch J, Van den Broucke S, Vancorenland S, Avalosse H, Verniest R, Callens M. Health literacy and the use of healthcare services in Belgium. J Epidemiol Community Health. 2016;70:1032–8.
Pignone M, Dewalt D, Sheridan S, Berkman N, Lohr K. Interventions to improve health outcomes for patients with low literacy: a systematic review. J Gen Intern Med. 2005;20:185–92.
Trezona A, Dodson S, Osborne RH. Development of the organisational health literacy responsiveness (org-HLR) framework in collaboration with health and social services professionals. BMC Health Serv Res. 2017;17:513.
Acknowledgements
The authors would like to thank the staff and patients of Cabrini Hospital for their support and participation in this study.
Funding
This research was supported by a grant from Cabrini Institute. ABeauchamp is funded by an ARC Linkage Industry Fellowship. RB is funded by an NHMRC Senior Principal Research Fellowship ID 1082138. Funding bodies were not involved in the design of the study, data collection, data analysis or writing of the manuscript.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
The study and overall design was conceived by RB, and operationalized by ABo and SP. MS undertook the statistical analysis. ABe undertook the HLQ analysis. ABo and RJ analysed and interpreted data, and wrote all drafts with contributions from all other authors. All authors contributed to the interpretation of the results. All authors critically reviewed the manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from both the Cabrini Human Research Ethics Committee (EC00239) and the Monash University Human Research Ethics Committee (EC00234). Consent to participate (for respondents who did not consent for their hospital records to be reviewed, and for non-respondents) was deemed unnecessary by the ethics department (Cabrini Human Research Ethics Committee). Cabrini Health approved access to de-identified patient information/hospital records without their consent as this was not deemed to infringe on patient confidentiality.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Bourne, A., Peerbux, S., Jessup, R. et al. Health literacy profile of recently hospitalised patients in the private hospital setting: a cross sectional survey using the Health Literacy Questionnaire (HLQ). BMC Health Serv Res 18, 877 (2018). https://doi.org/10.1186/s12913-018-3697-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-018-3697-2