
Abstract
Background
Routine health information systems (RHIS) are vital for the acquisition of data for health sector planning, monitoring, and evaluation. However, in developing countries the insufficient quality of the data produced by RHIS limits their usefulness in decision-making. As routine health information utilization is still low in Ethiopia, this study aimed to assess the magnitude of routine health data utilization and associated factors among health care professionals in some public health institutions in North Gondar, northwest Ethiopia.
Methods
An institution based cross-sectional study was conducted from March to April2017, at public health institutions of North Gondar Zone, northwest Ethiopia. A total of 720 health care professionals were selected from public health institutions using the multi-stage sampling technique. Data were collected using a structured self-administered questionnaire and an observational checklist, cleaned, coded, and entered into Epi-info version 3.5.3 and transferred into SPSS version 20 for further statistical analysis. In the multiple logistic regression analysis, a less than 0.05 P-vale was considered statistically significant.
Result
In this study, the level of good routine health information utilization among health professionals was 78.5% (95% CI: 73.2%, 84.3%). According to the multivariable logistic regression analysis, sex (AOR = 2.19, 95% CI: 1.47, 3.27), type of institution (AOR = 3.57, 95% CI: 2.39, 5.32), standard indicators (AOR = 3.28, 95% CI: 1.90, 5.65), data analysis skills (AOR = 1.90, 95% CI: 1.12, 3.23), and good governance (AOR = 1.97, 95% CI: 1.31, 2.95), were found significantly associated with a good level of health information utilization.
Conclusion
Over three-fourths of the health care professionals working at public health institutions of North Gondar utilized health information better than the respondents in previous studies. Sex, type of institution, standard indicators, data analysis skills, and governance were factors related to routine health information utilization. Therefore, standard indicators, data analysis skills and good governance are highly recommended for improving routine health data utilization of health care professionals working at public health institutions.
Similar content being viewed by others


Background
Health information system (HIS) is a system designed for the collection, processing, use, and dissemination of health related data to improve health care outcomes. It is one of the six fundamental blocks of a health care system which includes health information system resources, indicators, data sources, data management, information products, dissemination, and use [1,2,3]. HIS involves the essentials for the overall health system which informs decision making in each of the other five blocks of the system and important in improving clinical and managerial decisions for providing quality information for evidence-based health practices [4, 5]. Data generated from healthcare facilities at regular intervals (routine health information system) are vital not only for the planning, monitoring, and evaluation of health care service activities, but also for the day-to-day patient management, health education, resource allocation, disease prioritization, and decision making [1, 6]. A properly functioning routine HIS gets the right information into the right hands at the right time, enabling policymakers, managers, and service providers to make decisions based on evidence, ultimately leading to sustainable health outcomes in the community they serve [1, 7, 8].
Globally, significant human and financial resources have been invested to improve routine health information systems for planning, reporting, community health mobilization, and observing disease trends. Recently, more attention has been given to strengthen evidence-based decision through good governance, transparency, and accountability. However, health system managers in developing countries tend to miss the role of routine data in tracking the performance of health programs and the overall health system, and neglect their typically used part of the performance of evaluation of district priority health targets [3, 8,9,10]. As a result, many health systems fail to fully link evidence to decisions and suffer from a reduced ability to respond to priority health needs at all levels of the health care system [1, 11]. Health information systems in low and middle income countries face challenges of inadequate data analysis; as a result the utilization of routine data for decision making remains very weak [12,13,14]. Too often, data are sat in reports, shelves, cabinets, databases and left unanalyzed to be sufficiently utilized for policy and program improvements [15, 16].
Routine health information system is vital for operational, tactical, and strategic decision making. Utilization of information at all levels of the health system through effective data analysis, interpretation, and utilization is important. However, poor data quality (incompleteness and incorrectness), and limited use remain the major concerns [3, 17]. Most health care providers in developing countries simply report routine health data without adequate utilization and feedback, and health care providers and managers at lower levels of the health care system have minimum understanding of the benefits of information. Findings from Africa indicate that routine health information utilization remains low [18, 19], 42% in Tanzania, 59% in Uganda [20], 58% in Liberia, and 65% of the health workers in South Africa [21] use routine health data for planning, management of health commodities, detecting outbreaks, and monitoring the performance of the health system. Despite efforts made to improve Health Management and Information System, data quality and use remain inadequate at peripheral health systems which are responsible for health care delivery [17]. Studies at various places in Ethiopia reported that routine health information utilization ranged from 22.5–69% [2, 22,23,24,25,26,27,28,29].
Reports showed that routine health information utilization can be affected by organizational [1, 30], technical, and behavioral characteristics of health care professionals [1]. Among the factors reported, analysis skills [24, 31, 32], lack of culture of information use [32], lack of supervision and regular feedback [22, 24], organizational infrastructure and HMIS training [24], knowledge, work load, computer skill, computer access, availability of HMIS guidelines and formats [29], availability of human resources [33], and data quality [15] are commonly associated with routine health information utilization. A report from Uganda showed that health care workers who lack training on computer software, data management, and HMIS were unable to understand the standard indicators and quality of data, subsequently making a limited use of routine health data [34, 35].
The Federal Ministry of Health (FMoH), Ethiopia introduced an Information Revolution to strengthen the method and practice of collecting, analyzing, and disseminating information for decisions. The revolution was targeted not only at changing the techniques of data and information management but also at bringing fundamental cultural and attitude change regarding the practice of information utilization. More of the strategy promoted the utilization data generated from peripheral health care systems. However, district facility staff rarely used routine data to identify performance gaps, make plans, and monitor progress. Information used health data only for report purposes and not to drive decisions and program improvements [35, 36]. Furthermore, the inadequacy of information use among health care professionals at the study setting remains a problem. Therefore, this study aimed to assess routine health information utilization among health care professionals and its predictors in North Gondar government health institutions. The finding will help to effectively implement different health sector programs and strategies, including the Health Sector Development Program (HSDP), social and community health insurances, and health care financing to address constraints in performance fulfillment of targets at district health care level.
Methods
Study design and setting
An institution-based cross-sectional study was conducted at public health institutions of North Gondar Administrative Zone from March to April 2017. The city of Gondar is located 747 km from Addis Ababa, the capital of Ethiopia. According to the plan and program report of the administrative zone health department, there are 2244 heath care professionals working at hospitals and health centers.
Study participants, sample size, and sampling procedure
All health care professionals in selected health facilities were included in the study. Sample size was calculated using the single population proportion formula, assuming 53.3% prevalence of health information utilization in eastern Ethiopia [23], a 95% level of confidence, a 5% of margin of error, a design effect of 2, and a 5% of non-response rate. Finally, a minimum sample of 720 was obtained. In the zone, there were a total of nine hospitals and 135 health centers. Out of the total health facilities, 3 hospitals and 45 health centers were selected by the random sampling technique. Using proportional allocation technique, 720 health care professionals were selected.
Data collection tool and procedure
The questionnaire was adapted from the PRISM frame work in which behavior, technical and organizational factors were the major determinants of the utilization of routine health information systems. Knowledge, data analysis skills, attitude, and the motivation of people who collect and use health information are behavioral factors, while data collection processes, systems, forms, and methods constitute the technical factors and organizational/environmental determinants, like information culture, structure, resources, governance, roles, and responsibilities of the health system affect the utilization of routine health information systems.
Data were collected using the pretested, structured, and self-administered questionnaire and an observational checklist. A two-days training was given to nine diploma graduate nurse data collectors and three BSc graduate nurse supervisors on the objective of the study and the confidentiality of information. During the course of data collection, participants were informed about the objective and processes of the study and confidentiality of the information. Data collectors were supervised at the study site and meetings were held with research assistants at the end of every day to discuss challenges and crosscheck data completeness and accuracy Additional file 1.
Operational definition and study variables
The dependent variable, routine health information utilization, was measured by the PRISM conceptual framework on the system. It was defined as the use of routine health information for treating patients, disease prioritization, drug procurement, the day-to-day monitoring of health service activities, checking data quality, resource allocation, planning, department performance evaluation, evaluation of staff performance, selection of best experience within the health facility, sharing of health data to other facilities and stakeholders, decision making, and community mobilization and discussion. All these components of the assessment tool have likert scale measures, ranging from “strongly disagree” to “strongly agree”, finally, health workers’ mean scores were used to label health professionals’ health information utilization as “has good routine health information utilization” when they scored above the mean value, or “has poor routine health information utilization” when they scored equal to and below the mean value. Health care professionals in this study were defined as any health personnel who were collecting health data in order to utilize the information for the improvement of health status.
Data processing and analysis
Data were entered into Epi-info version 7 and exported to the Statistical Package for Social Sciences (SPSS) version 20 for further analysis. Descriptive statistics, including frequencies and proportions, were computed using the binary logistic regression model in order to summarize variables. Variables with a p-value of less than 0.2 in the bi-variable analysis were entered into the multivariable logistic regression analysis. Both Crude Odds (COR) and Adjusted Odds Ratios (AOR) with 95% confidence interval were estimated to show the strength of associations. Finally, a p-value of less than 0.05 in the multivariable logistic regression analysis was used to identify variables significantly associated with the utilization of routine health information.
Results
Socio-demographic and behavioral characteristics
A total of 720 healthcare professionals were included in the study, giving response rate 100%. Just over half (52.1%) of the respondents were male health care professionals, 64.2% of whom were diploma graduate nurses. Slightly more than half (50.4%) nurses took part in this study than other health workers. Almost half (49.7%) of the respondents earned monthly salary of 100–150 dollar. More than half (58.6%) had positive belief in routine health information utilization. The majority (84.1%) gave no value to routine health information utilization, and 76.9% had no custom of routine health information utilization (Tables 1 and 2).
Organizational and technical factors
Of the total participants, 52, 57.6, 50.7 and 57% of had no culture of information utilization, had supervision on routine health information utilization (RHIU), had governance for RHIU and had good governance for RHIU. In addition, slightly higher than half (50.9 and 53.8%, respectively) used routine health data for planning, and received feedback on routine health information utilization. The majority (87.9% and 99.8%, respectively) of respondents received no training and no professional skill on RHIU. More than two-thirds (75% and 70.1%, respectively) had no professional knowledge about national indicators, and had no professional data analysis skills (Tables 3 and 4).
Routine health information system utilization
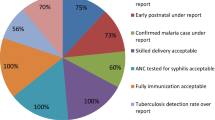
In this study, the majority (94%) of the respondents used routine health data for treating patients, 90.1% for disease prioritization, 85% for drug procurement, 89.6% for monitoring day to day health service activities, 92.6% for checking data quality, 86.7% for resource allocation, 89% for planning, 88% for department performance evaluation, 86.5% for evaluation of staff performance, 85% for selection of best experience within a health facility, 82.8% for sharing health data to other facilities and stakeholders, 87.8% for decision making, and 87.1% for community mobilization and discussion. Good routine health information system utilization was noted among 78.5% of the health care professionals. The proportion of good health information utilization was 84.9% at health centers and 64.1% at hospitals Table 5.
Factors associated with good routine health information system utilization
In the bivariable logistic regression analysis, sex, type of facility, standard indicator, data analysis skills, culture of information, supervision, governance, planning and position were factors associated with good routine health information utilization at a p-value of less than 0.2. Consequently, these variables were subjected to multivariable logistic regression analysis, and it was noted that sex, type of facility, standard indicators, data analysis skills and governance were significantly associated with good routine health information utilization at a p-value of 0.05.
In this study, the high odds of good routine health information system utilization were noted among male health care professionals [AOR = 2.91; 95% CI: 1.47, 3.27], types of facility [AOR = 3.57; 95% CI: 2.39,5.32], standard indicators [AOR = 3.28; 95% CI: 1.90,5.65],, data analysis skills [AOR = 1.91; 95% CI: 1.12,3.23], and good governance [AOR = 1.91; 95% CI: 1.12,3.23] (Table 6).
Discussion
The aim of this study was to identify factors associated with poor routine health information utilization of health care professionals at public health institutions. According to our findings, the magnitude of routine health information utilization of health care professionals was 78.5%. This finding is higher than that of a study conducted in North Gondar (22.5%) [22], Jimma (32.9%) [23], East Gojjam (45.8%) [24], Hadiya zone (69%) [25], west Amhara (38%) [29], and in Ethiopia (48%) [2]. This variation might be due to differences in study periods. Besides, recently the government has given a special emphasis to utilization of information for evidence based decision making and the improvement of health care professionals’ information using culture [8]. Similarly, the finding was higher than those of studies reported from outside Ethiopia, that is Uganda (59%) [20], South Africa (65%) [21]. This might be due to variations in study periods and the criteria for measuring routine health information use [15].
According to the multivariable logistic regression analysis, the higher odds of routine health information utilization were noted among health professionals who had good governance when compared to health care professionals who had poor governance. The finding was supported by those of other studies reported elsewhere [1]. This might be due to the fact that the presence of good governance at public health institutions encourages staff to use routine health information for evidence based decision by strengthening health information systems [2]. Routine health information utilization among male respondents was higher than among females. It was revealed that the odds of health information utilization among male health professionals were 2.9 times higher than among females. This might be due to the fact that the majority of respondents were male.
Among the reported significant organizational factors, higher odds of routine health information utilization were noted among health professional working at health centers compared with those working at hospitals. This finding was supported by that of a study conducted in East Gojjam zone [24]. This might be due to the attention given by the government to district health facilities in terms of supervision and regular feedback [28, 37].
In our work, the odds of routine health information utilization of health care professionals who had data processing skills were 1.9 times more likely compared to health care professionals who had no data processing skills. This might be due to the fact that data analysis skills are one of the inputs for utilizing routine health information. Thus, without turning data into information, it is difficult to utilize routine health information for evidence based decision making. This finding is supported by that of a study conducted in East Gojjam zone [24], that is, perhaps because data analysis skills are very important for turning data into information.
Furthermore, the odds of health information utilization among health care professionals who had standard indicators in their offices were3.28 times higher than those who no such indicators to utilize routine health data. This might be due to the presence of data sources (standard indicator) which provides utilization of information for evidence based decision making [1].
Conclusion
This study found that more than three fourths of the health care professionals at public health institutions in North Gondar had good routine health information utilization. Sex, standard indicators, good governance, and type of health facility had significant associations with routine health information utilization. Therefore, the standard indicators, and good governance at public health institutions are highly recommended. The study also suggested further investigations on the culture of health information utilization among health care providers where routine data are generated.
Abbreviations
- AOR:
-
Adjusted Odds Ratio
- CI:
-
Confidence Interval
- RHIS:
-
Routine Health Information System
- SPSS:
-
Statistical Package for Social Science
References
Aqil A, Lippeveld T, Hozumi D. PRISM framework: a paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy Plan. 2009;24(3):217–28.
WHO, Framework and Standards for Country Health Information Systems. 2012.
Framework, W. Standards for country health information systems/health metrics network. Geneva: World Health Organization; 2008.
AbouZahr C, Boerma T. Health information systems: the foundations of public health. Geneva: World Health Organization; 2014.
Singh A. Strengthening health systems to meet MDGs. Health Pol Plan. 2006;21(4):326–8.
Nisingizwe MP, et al. Toward utilization of data for program management and evaluation: quality assessment of five years of health management information system data in Rwanda. Glob Health Action. 2014;7(1):25829.
Mucee EM, Kaburi LW, Kinyamu RK. Routine Health Management Information Use in the Public Health Sector in Tharaka Nithi County, Kenya. Imperial J Interdisciplinary Res. 2016;2(3):660–672
Hotchkiss DR, et al. Evaluation of the performance of routine information system management (PRISM) framework: evidence from Uganda. BMC Health Serv Res. 2010;10(1):188.
Aqil A. PRISM case studies: strengthening and evaluating RHIS. Washington, D.C: MEASURE Evaluation, USAID; 2008.
Health Metrics, N. Assessing the National Health information systems. An assessment tool. Geneva: Health metrics network, World Health Organization; 2008.
Lærum H, Karlsen TH, Faxvaag A. Use of and attitudes to a hospital information system by medical secretaries, nurses and physicians deprived of the paper-based medical record: a case report. BMC Med Inform Decis Mak. 2004;4(1):18.
Organization, W.H. Everybody's business: strengthening health systems to improve health outcomes. WHO's Framework for Action. Geneva: WHO; 2007.
Organization., W.H. Strengthening Health Information Systems. Geneva: WHO; 2007. Retrieved february 10, 2014
Evaluation, M., Routine health information systems: a curriculum on basic concepts and practice - facilitators’ guide 2017.
Nutley T, Reynolds HW. Improving the use of health data for health system strengthening. Glob Health Action. 2013;6:20001.
Nutley T. Improving data use in decision making: an intervention to strengthen health systems. Chapel Hill: MEASURE Evaluation, Carolina Population Center, Carolina; 2012.
Federal Democratic Republic of Ethiopia, M.o.H., Health Sector Development Programme IV 2010/11–2014/15 https://www.medbox.org/et-policies-others/health-sector-development-programme-iv-201011-201415/preview?. Accessed 1 Sept 2018.
Tadesse K, Gebeyoh E, Tadesse G. Assessment of health management information system implementation in Ayder referral hospital, Mekelle, Ethiopia. Int J Intell Inf Syst. 2014;3(4):34.
Andualem M, Kebede G, Kumie A. Information needs and seeking behaviour among health professionals working at public hospital and health centres in Bahir Dar, Ethiopia. BMC Health Serv Res. 2013;13(1):534.
Gladwin J, Dixon R, Wilson T. Implementing a new health management information system in Uganda. Health Policy Plan. 2003;18(2):214–24.
Garrib A, et al. An evaluation of the district health information system in rural South Africa. SAMJ: S Afr Med J. 2008;98(7):549–52.
Andargie, G., Assessment of utilization of health information system at district level with particular emphasis to HIV/AIDS program in North Gondar zone Amhara national regional state. 2006, aau.
Abajebel S, Jira C, Beyene W. Utilization of health information system at district level in Jimma zone Oromia regional state, South West Ethiopia. Ethiop J Health Sci. 2011;21(3):65–76.
Shiferaw AM, et al. Routine health information system utilization and factors associated thereof among health workers at government health institutions in East Gojjam Zone, Northwest Ethiopia. BMC Med Inform Decis Mak. 2017;17(1):116.
Abera E, et al. Utilization of health management information system and associated factors in Hadiya zone health centers, Southern Ethiopia. Res Health Sci. 2016;1(2):98.
Yarinbab TE, Assefa MK. Utilization of HMIS Data and Its Determinants at Health Facilities in East Wollega Zone, Oromia Regional State, Ethiopia: A Health Facility Based Cross-Sectional Study. Med Health Sci. 2018;7(1)
Adane T, Tadesse T, Endazenaw G. Assessment on Utilization of Health Management Information System at Public Health Centers Addis Ababa City Administrative, Ethiopia. Internet Things Cloud Comput. 2017;5(1):7–18.
Belay, H., T. Azim, H. Kaddahun, Assessment of Health Management Information System (HMIS) Performance in SNNPR, Ethiopia. Measure Evaluation, 2013.
Asemahagn MA. Determinants of routine health information utilization at primary healthcare facilities in Western Amhara, Ethiopia. Cogent Med. 2017;4(1):1387971.
Shaikh BT, Hatcher J. Health seeking behaviour and health service utilization in Pakistan: challenging the policy makers. J Public Health. 2005;27(1):49–54.
Teklegiorgis K, et al. Factors associated with low level of health information utilization in resources limited setting, eastern Ethiopia. Inf Syst. 2014;3(6):69–75
Mucee EM, Kaburi W, Kinyamu RK. Routine Health Management Information Use in the Public Health Sector in Tharaka Nithi. Kenya: Interdisciplinary Research; 2016.
Gibson B. KAGARUK, Kimaro HC, Leonard G. MBOERA, Factors Affecting Utilization of Evidence Based Health Information System for Effective Supply Chain of Essential Medicine in Tanzania. Health Informatics in Developing Countries, 2013.
Asiimwe, A.K., Determinants of effective utilization of routine health information within private health facilities in. 2016.
Health, M.o. and F.D.R.o. Ethiopia, National Health Information System Road Map. 2012.
Health, E.F.M.o., Information Revolution Roadmap. 2016.
FMOH E, WHO, CSA, HMN. Assessment of the Ethiopian National Health Information System. Ethiop J health Sci; 2007.
Acknowledgments
The authors are indebted to the University of Gondar for the approval of the ethical clearance, North Gondar zone health departments and respective district health offices and Hospitals for giving us permission to collect the data in the health facilities. The authors also forward its gratitude to health care professionals, data collectors and supervisors who participated in the study.
Availability of data and materials
Data will be available upon request from the corresponding author.
Author information
Authors and Affiliations
Contributions
ED conceived of the study, coordinate data collection. ED, SAW, and AMS performed statistical analysis and drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was obtained from the Ethical Review Board of the University of Gondar. A letter of permission was obtained from North Gondar zonal health department. After the objective of the study was explained, verbal consent was obtained from each participant. Moreover, privacy and confidentiality of information was strictly guaranteed by all data collectors and investigators. The information retrieved was used only for the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Questionnaire to assess routine health information utilization and associated factors in north Gondar, northwest Ethiopia. (DOCX 36 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Dagnew, E., Woreta, S.A. & Shiferaw, A.M. Routine health information utilization and associated factors among health care professionals working at public health institution in North Gondar, Northwest Ethiopia. BMC Health Serv Res 18, 685 (2018). https://doi.org/10.1186/s12913-018-3498-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-018-3498-7