
Abstract
Background
Owing to different social background factor in Yunnan-Myanmar Chinese border region, stressful working environment may lead to extra psychological burden among nurse staff in China. However, the prevalence of workplace violence and its effect on psychological characteristics among nurse staff are still unclear. This study aims to explore the effect of workplace violence against psychological health among nurse staff from Yunnan-Myanmar Chinese border region.
Methods
A cross-sectional survey was conducted among 18 local governmental hospitals in Dehong districts. Participants were 1,774 nurses. Psychosocial characteristics were screened by sleep quality, the 9-item Patient Health Questionnaire for depressive symptoms, the generalized anxiety disorder-7 for anxiety symptoms, the Connor Davidson Resilience Scale – 10 item for resilience, the multidimensional scale of perceived social support for social support, the Chinese version of Work place Violence Scale for workplace violence. Propensity score matching and multivariate linear regression were applied to analyze the data.
Results
The nurse staff with workplace violence have a higher risk of bad sleep quality (b = -0.883, 95%CI = [-1.171, -0.595]), anxiety symptoms (b = 2.531, 95%CI = [2.031, 3.031]) and depressive symptoms (b = 3.227, 95%CI = [2.635, 3.819]), loneliness (b = 0.683, 95%CI = [0.503, 0.863]), perceived cognitive deficits (b = 1.629, 95%CI = [1.131, 2.127]), poor resilience (b = -2.012, 95%CI = [-2.963, -1.061]), and poor social support (b = -5.659, 95%CI = [-7.307, -4.011]).
Conclusions
Preventing workplace violence can improve mental health outcomes significantly among nurse staff, including loneliness, perceived cognitive deficits, anxiety symptoms, depressive symptoms, sleep quality, resilience and social support.
Similar content being viewed by others


Introduction
Workplace violence (WPV) is widely recognized as a significant issue in negative medical work environments worldwide [1], and nurse staff are often the primary victims. Nurse staff members are known to be at high risk of WPV [2]. A meta included 136 international studies, related to Asian, European, etc., present that 36.4% of nurse staff experienced physically assaulted, and 67.2% reported have been nonphysical assaults [3]. During the normalized COVID-19 epidemic prevention and control of China, nurse staff members have been particularly vulnerable to workplace violence due to heavy workloads and stressful work environments [4], which can significantly impact their psychosocial characteristics.
Workplace violence can cause a range of health problems among nurse staff members. Theoretical evidence suggests that exposure to violence can weaken personal stress regulation, leading to negative mental reactions such as sadness, anger, and fear [5, 6]. Previous studies have also found that nurse staff members who are exposed to workplace violence are more likely to experience symptoms of anxiety and depression [7]. A meta-analysis has shown that exposure to workplace violence is associated with various sleep problems [8, 9]. In China, several studies have reported that a significant number of medical staff members experience symptoms of anxiety, depression, and burnout, among other psychological problems [10,11,12]. Such psychological problems may have both short-term and long-term effects on the mental health of nurse staff members [13]. In light of these findings, it is crucial to assess and attend to the mental health needs of nurse staff members who have experienced workplace violence, providing timely and effective psychological assistance services.
Workplace violence can have varying prevalence and impact on the mental health of nurse staff members in different regions of China, particularly those with multi-ethnic and multi-neighboring settings. However, research in these areas remains limited, especially in Chinese border regions with diverse ethnic groups. Therefore, our study aims to contribute to the existing literature by investigating the effects of workplace violence on the mental health outcomes of nurse staff members in the Yunnan-Myanmar Chinese border region, where unique challenges related to healthcare worker safety and well-being may arise. In addition, previous studies have primarily used linear or logistic regression models to explore the associations between different variables. However, by comparison with randomized controlled trials (RCTs), these models may only control for confounding factors to a limited extent. In recent research, propensity score matching (PSM) analysis has been proposed as an alternative method to address such issues [14, 15]. PSM involves dividing samples into treatment and control groups and using propensity scores to match their baseline socio-demographic variables [16]. This approach ultimately excludes unmatched samples and includes matched samples for final analysis. While previous studies have utilized regression analyses to examine the relationship between workplace violence and mental health outcomes, few studies have employed propensity score matching as a method of analysis.
Previous studies have primarily focused on the impact of workplace violence on mental health outcomes such as PTSD, depression, anxiety, and burnout among healthcare workers. However, there is still limited research on the impact of workplace violence on other mental health outcomes, such as loneliness and perceived cognitive deficits, which are important indicators of psychological well-being. This study aims to address this gap by examining the impact of workplace violence on psychosomatic outcomes, including loneliness, perceived cognitive deficits, anxiety symptoms, depressive symptoms, sleep quality, resilience, and social support among nurse staffs from the Yunnan-Myanmar Chinese border region. To investigate the potential differences in the effects of workplace violence on mental health outcomes, this study employs a combination of Propensity Score Matching (PSM) and regression analysis. Unlike prior research that has relied solely on regression analysis, the PSM method is used to obtain matched data, which is subsequently analyzed using regression analysis to examine the relationships between variables. To summarize, this study aims to examine the impact of workplace violence on mental health outcomes among nurse staffs from the Yunnan-Myanmar Chinese border region, by applying the PSM method. Specifically, this study aims to compare the effectiveness of PSM methods in matching confounders and the differences in outcomes between pre-matching and post-matching methods.
Methods
Participants and procedure
A cross-sectional study was conducted in Dehong districts, Yunnan province from July 11 to July 26, 2022. Nurse staff comes from all 18 local governmental hospitals in Dehong districts, were recruited to participate in this study. Dehong is an ethnic border district located in the southwest of China, with a population of approximately 1.32 million people as of the end of 2021 [17]. It shares a 503.8-kilometer-long border with Myanmar on its north, west, and south sides [18]. The convenience sampling method was applied to recruit the participants, who completed our questionnaires using Wenjuanxing software, the largest online questionnaire software in China. Trained researchers fully explained the purpose of the study to each participant, and the questionnaire link was distributed by the nursing department of each governmental hospital. The survey was anonymous, and participants were asked to complete the questionnaire independently. They could contact the researchers if they had any questions about the survey and were informed of their right to withdraw at any time. Most participants took approximately 7 min to complete the questionnaire. Ultimately, a total of 1965 nurse staff members were invited to participate, and 1774 completed the survey, resulting in a response rate of 90.3%. The Ethics Committee of Dehong People’s Hospital in China approved the study (Ethics Approval Number: DYLL-KY032).
Inclusion criteria and sample size
Participants met the following inclusion criteria and then have been included in this study: (1) work at the 18 local governmental hospitals; (2) able to understand the content of questionnaire; (3) agreed to participants and provided informed consent; (4) were not mental illness, (5) were not student nurse. The cross-sectional survey formula was applied to calculate the sampling as follows:
Z1−α/2 is the statistical value for significance testing, where α = 0.05 and its value is 1.96. p is the prevalence rate of psychological health problems, where q = 1-p, and d is the allowable error, where d = 0.2p. According to previous studies, the prevalence rate of psychological health problems among nurses were ranging from 6.2 to 36.9% [19]. In this study, the minimum value of 6.2% was used for calculations, which translates to a minimum of 1706 subjects considering a non-response rate of 10%.
Measures
Socio-demographic variables
Basic socio-demographic characteristics such as age, sex, ethnic, marital status, residence, education level, only children, monthly income, and work experiences were collected. In addition, we recorded their weight and height, and used these measurements to calculate their BMI score (BMI = Weight [kg] /Height2 [m]). The BMI group was classified into four groups: Underweight (< 18.5), Normal (18.5 ~ 24.9), Overweight (25.0 ~ 29.9), and Obese (> 30.0).
Workplace violence
Workplace violence were assessed by the Chinese version of Work place Violence Scale (WVS) [20], which consists of five-dimension items with physical assault (PA), emotional abuse (EA), threats (T), verbal sexual harassment (VSH), sexual abuse (SA) (e.g., In the past year, have you encountered the physical assault violence from patients or patients’ relatives? Including pushing, biting, beating, spitting). Each item was scored on a scale from 0 to 3 (0 = never, 1 = one time, 2 = two or three times, 3 = more than three times). The total score for the scale was calculated by summing each item and then dividing participants into two categories: those who had experienced workplace violence (score from 1 to 15) and those who had not (score of 0). This scale has been confirmed good reliability and validity in China [21]. The Cronbach’s α = 0.76 in this study.
Loneliness
Loneliness was assessed using the Three-Item Loneliness Scale [22], which is a 3-point Likert scale consisting of three items that ask participants to rate how often they feel they lack companionship. Response options include “hardly ever,“ “some of the time,“ and “often.“ The total score for the scale is calculated by summing each item, resulting in a score range of 3 to 9. Higher scores indicate a greater level of loneliness. The Cronbach’s α = 0.83 in this study.
Sleep quality
Sleep quality was assessed by the single-item sleep quality scale (SQS) [23]. Participants were asked to rate their overall sleep quality during the past seven days on an 11-point scale ranging from 0 (terrible) to 10 (excellent), with higher scores indicating better sleep quality. The SQS is a single-item questionnaire that has been found to have appropriate measurement characteristics for evaluating sleep quality, compared to longer questionnaires such as the Morning Questionnaire-Insomnia and Pittsburgh Sleep Quality Index (PSQI) [23]. The instrument has been reported to have a good reliability and validity, and it has been used in various published studies [24, 25], including research conducted in China [26, 27].
Perceived cognitive deficits
Perceived cognitive deficits were assessed using the Perceived Deficits Questionnaire (PDQ-5) [28]. This questionnaire consists of five questions related to attention, concentration and planning, organization, retrospective memory, and prospective memory. Participants were asked to rate their level of agreement with each item on a scale ranging from “never” (scored 0) to “always” (scored 4). The total score for the questionnaire is calculated by summing each item, with higher scores indicating more severe perceived cognitive deficits. The Cronbach’s α = 0.85 in this study.
Anxiety symptoms
The generalized anxiety disorder-7 (GAD-7) [29] was used to measure anxiety symptoms in this study. This scale consists of seven items that ask participants to rate how often they have experienced specific symptoms of anxiety in the past two weeks, on a 4-point scale ranging from “not at all” to “nearly every day.“ The total score for the scale ranges from 0 to 21, with higher scores indicating more severe anxiety symptoms. The Chinese version of GAD-7 have been confirmed good validity and reliability [30]. The Cronbach’s α = 0.93 in this study.
Depressive symptoms
Depressive symptoms were assessed using the 9-item Patient Health Questionnaire (PHQ-9) [31]. This scale consists of nine items that ask participants how often they have experienced specific symptoms of depression in the past two weeks, on a 4-point Likert scale ranging from “not at all” to “nearly every day.“ Scores for each item range from 0 to 3, depending on the response. The total score for the scale ranges from 0 to 27, with higher scores indicating more severe depressive symptoms. The Chinese version of PHQ-9 have shown good validity and reliability in China [32, 33]. And the Cronbach’s α = 0.91 in this study.
Resilience
Resilience was assessed using the Connor-Davidson Resilience Scale-10 item (CD-RISC-10) [34]. This scale consists of ten items that ask participants to rate the extent to which they agree with specific statements about their ability to cope with adversity, on a 5-point scale ranging from “never true” to “always true.“ Scores for each item range from 0 to 4, depending on the response. The total score for the scale is calculated by summing the scores for each item, with higher scores indicating stronger resilience levels. The CD-RISC-10 has been found to have good validity and reliability in China [35]. And the Cronbach’s α = 0.94 in this study.
Social support
Social support was assessed by the multidimensional scale of perceived social support (MSPSS) [36]. It is containing 12 items with response on seven-point Likert scale, ranged from 1 (strongly disagree) to 7 (strongly agree). The sum score were calculated by adding each item, with higher scores indicting higher level of social support. The Chinese version of this scale have been used in Chinese population [37]. And the Cronbach’s α = 0.96 in this study.
Statistical analysis
Descriptive analysis
Qualitative data were presented as numbers and percentages (N/%), while quantitative data were presented as mean ± standard deviation (SD). The chi-square test and t-test were used to assess differences in basic sociodemographic variables between participants who experienced workplace violence and those who did not.
PSM analysis
In order to control confounding covariates, propensity score (PS) is a statistic that calculates the conditional probability of being assigned to a specific treatment, given a set of observed covariates [38], which can be used to decrease the impact of selection bias. We used PSM analysis to match baseline socio-demographic characteristics, including age, sex, ethnic, marital status, residence, education level, only children, monthly income and BMI. In this study, nurse with workplace violence as experiment group, and non-workplace violence nurse as control group, and Nearest neighborhood matching were used to matched baseline socio-demographic variables (caliper = 0.05), with a ratio of 1 (case) :1(control).
Multivariate liner regression
Multivariate liner regression model was used to assess the effect of workplace violence on mental health outcomes before matching and after matching. All multivariate liner regression model also controlled basic socio-demographic covariates.
R version 3.6.2 were used to performed PSM analysis and other statistical analysis were conducted by SPSS version 22.0. P value were set at 0.05 in this study (two-tails). The Cronbach’s alpha coefficient (Cronbach’s α) was calculated to confirm the reliability of the questionnaires in this study. The Cronbach’s α ranges from 0 to 1, with higher values indicating greater internal consistency. Generally, a Cronbach’s α value of 0.70 or higher is considered acceptable for most research purposes [39, 40].
Results
A total of 1,774 nurses were included in the statistical analysis, of whom 559 (31.5%) reported experiencing workplace violence in the past year. Table 1 presents the baseline sociodemographic characteristics and mental health outcomes of the participants. The majority of nurses were female (93.9%), of Han ethnicity (71.9%), married (67.6%), had a normal body mass index (64.0%), were only children (84.0%), lived in rural areas (60.4%), and had a monthly income of 3001–5000 RMB (44.1%). The average age of the nurses was 32.00 years old (SD = 7.99), and most had 5–9 years of nursing experience (33.4%). With regard to mental health outcomes, the mean scores for loneliness, sleep quality, perceived cognitive deficits, anxiety symptoms, depressive symptoms, resilience, and social support were 2.26 (SD = 1.55), 6.33 (SD = 2.44), 7.12 (SD = 4.27), 6.29 (SD = 4.32), 7.42 (SD = 5.13), 21.85 (SD = 8.28), and 62.60 (SD = 14.02), respectively.
In the propensity scores matching analysis, nurses who did not experience workplace violence were designated as the control group, while those who did were considered the treatment group. Figure 1 displays the distributions of propensity scores between unmatched samples and matched samples. In details, the total sample have been dropped from 1774 to 1082 (N non-workplace violence = 541, N workplace violence = 541), with a total of 692 unmatched cases excluded. The absolute standardized mean difference of basic socio-demographic characteristics is down from 0.230 to 0.002 before matching and after matching, indicting post-matched samples present a well covariate balance (See Figure 2). In addition, the result of Chi-square test and T test of basic socio-demographic characteristics separated by workplace violence before and after matching also have confirmed that the PSM analysis was performed well (Chi-square/T value and P value were decreased) (See Table 2).
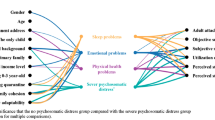
Figure 3 exhibited the link between workplace violence and mental health outcomes with Pre-matching and Post-matching among nurse staff. In Pre-matching analysis, after controlling socio-demographic covariates, multivariate liner regression models revealed that nurse staffs with workplace violence have a higher risk of loneliness (b = 0.723, 95%CI = [0.570, 0.876]), poor perceived cognitive deficits (b = 1.786, 95%CI = [1.365, 2.207]), anxiety symptoms (b = 2.503, 95%CI = [2.082, 2.924]) and depressive symptoms (b = 3.194, 95%CI = [2.700, 3.688]). And workplace violence can negatively affect good sleep quality (b = -0.880, 95%CI = [-1.123, -0.637]), resilience (b = -2.340, 95%CI = [-3.159, -1.521]) and social support (b = -5.966, 95%CI = [-7.344, -4.588]). In Post-matching analysis, all covariates were matched well, and the result of multivariate liner regression show different with Pre-matching results. In details, the nurse staff with workplace violence was associated with sleep quality (b = -0.883, 95%CI = [-1.171, -0.595]), anxiety symptoms (b = 2.531, 95%CI = [2.031, 3.031]) and depressive symptoms (b = 3.227, 95%CI = [2.635, 3.819]), with higher beta value of liner regression models. Other mental health outcomes were also associated workplace violence significantly, with lower beta value of liner regression models including loneliness (b = 0.683, 95%CI = [0.503, 0.863]), perceived cognitive deficits (b = 1.629, 95%CI = [1.131, 2.127]), resilience (b = -2.012, 95%CI = [-2.963, -1.061]), and social support (b = -5.659, 95%CI = [-7.307, -4.011]).
Discussion
In this study, we revealed that the adverse impact of workplace violence on psychosomatic outcomes and PSM analysis methods of control confounding factors show effectively. Results showed that workplace violence was significantly associated with higher levels of loneliness, sleep quality, perceived cognitive deficits, anxiety symptoms, depressive symptoms, reduced resilience, and decreased social support among nurses. Hospital administrators should take effective measures to prevent workplace violence and mitigate the mental stress associated with it, in order to avoid psychosomatic problems. In addition, this study is also the first to report the prevalence of workplace violence among nurse staff in the Yunnan-Myanmar Chinese border region. The rate of workplace violence was 31.5% in the past 12 months among nurse staff in this study. Several previous studies shown the different rate of workplace violence depending on the study design, timeframe, location, and other factors [41,42,43]. A meta-analysis shown that the rate of workplace violence was 62.4% for the whole of life among health work provider in China [44]. Lu’s study also revealed that 84.2% of frontline psychiatric nurses was experienced workplace violence [44]. However, the prevalence of workplace violence was 18.5% among health work provider [45]. Direct comparison cannot be done due to not locate any previous research in Yunnan-Myanmar Chinese border region. So, our findings highlight the need for targeted interventions to address workplace violence and its impact on the mental health of healthcare workers in the Yunnan-Myanmar Chinese border region.
Our results also revealed that workplace violence increased the likelihood of anxiety symptoms, depression symptoms, bad sleep quality, and it also decreased the level of resilience and social support among nurse staff, which consist of previous studies [46,47,48,49]. A cross-sectional study surveyed in China have shown that workplace violence plays a negative effect on nurse staff’s mental health and well-being [46]. A review contains 16 international researches revealed that nurse staff exposed to workplace violence can have a higher risk of poor quality of life welling-being, life satisfaction, depressive symptoms, occupational stress [47]. Furthermore, a survey carried out among healthcare professionals in China revealed that workplace violence could greatly diminish their perceived social support, ultimately resulting in mental health issues [50]. Similarly, another study conducted on Chinese nurses and general practitioners highlighted that experiencing workplace violence can decrease their resilience levels, ultimately causing symptoms of depression [51]. Conservation of resources theory have elaborated that the individual of resources are limited [52], and workplace violence can increase the discomfort of nurse staff, which further increased nurse staff’s resource consumption. And the new resources such as self-esteem, social support and resilience were hard to obtain for high exposure of nurse staff to workplace violence [48, 49]. Thus, poor mental health outcomes can be raised with the consumption of resource, and future study can examine more mental health outcomes and the relationship between workplace violence and them to provide related strategies to tackle workplace violence. Moreover, it is important to mention that the linear regression analysis conducted post-matching demonstrated a higher effect coefficient for workplace violence on anxiety and depressive symptoms compared to the pre-matching analysis, while the effect coefficient for workplace violence on resilience and social support was lower. This difference in regression coefficients may be attributed to the confounding factors such as age and sex that were controlled in the Propensity Score Matching (PSM) analysis. The accurate linear coefficients were displayed, especially when the actual impact of workplace violence on resilience, social support, anxiety, and depressive symptoms with covariates were perfectly balanced.
Consistent with previous research findings [8, 53, 54], our study found a positive association between workplace violence and poor sleep quality. A review of 119,361 participants across 15 countries demonstrated that experiencing physical, verbal, or sexual violence in the workplace was a predictor of sleep problems [8]. Similarly, a cross-sectional study of 550 nurses and nursing assistants revealed a significant association between workplace violence and headaches and poor sleep quality. Those exposed to physical abuse at work had over twice the risk of developing headaches and poor sleep quality [53]. Psychological stress after experiencing workplace violence may be a contributing factor leading to sleep disturbance and health issues [55]. Moreover, gender of the nurse staff was found to be related to impaired sleep quality [56]. However, gender was considered a covariate in this study to balance the relationship between workplace violence and sleep quality after post-matching. Consequently, the significant linear regression coefficient in pre-matching and post-matching indicated that the effect of workplace violence on sleep problems was underestimated.
Our findings on the relationship between workplace violence and loneliness also worth a mention. The results revealed that nurse staff with workplace violence were found to report to higher level loneliness. In line with prior findings, the general population have shown a strong association between loneliness and bullying or abuse [57, 58]. In the stage of normalized COVID-19 pandemic prevention and control, nurse staff exposed to negative interpersonal events can induce the sense of social alienation, and lead to the avoidance of social situation [59]. If the social situation were not altered, and this tough social situation could cause the feeling of loneliness among nurse staff. Previous studies have reported varying levels of loneliness among nurses of different genders[60]. Therefore, in this study, the age was controlled as a covariate to balance the relation between workplace violence and loneliness after post-matching. The significant linear regression coefficient in pre-matching and post-matching indicated that the effect of workplace violence on loneliness was overestimated.
In agreement with previous studies, poor perceived cognitive deficits was associated with workplace violence in this study. In shobhit’s research surveyed in India, the violent older adult tends to be of lower cognitive ability than non-violent older adults [61]. Similarly, Priscilla’s study revealed that the children with intimate partner violence have a lower cognitive ability score within a year, while it is not significantly within 10 years [62]. Lower cognitive ability are unfavorable factors of satisfaction nursing and safety nursing among nurse staff, which may further increase the possibility of workplace violence. To the best understating of present studies, the mechanism of cognitive ability and violence are still unclear. However, Priscilla and his colleges assume that the violence events can affect chronic biological stress, and in turn response to subsequent cognitive development. Future studies maybe test and verify it by experimental program. Furthermore, the inconsistent results obtained before and after matching indicated that the propensity score matching method is more robust in testing the effects of WPV compared to the simple regression method.
Consistent with aims, our findings also proved that PSM analysis is an important instrument to control covariate characteristics. By performed PSM analysis, the baseline socio-demographic characteristics were more comparable between workplace violence and non-workplace violence nurse staff. And it further leading to the distinguish coefficient of pre-matching and post-matching on multiple liner regression model, with higher/lower beta value of liner regression models. To achieve effectiveness, PSM analysis may be a functional approach to meet the exacting statistical requirements in further research.
Workplace violence has adverse effects on the well-being of nurses, highlighting the importance of taking steps to prevent it. The healthcare system in China has implemented a “safe hospital” policy that utilizes social media to promote positive images of nurses and raise awareness of their contributions [63]. Hospitals have also collaborated with public security departments to establish warning and defense systems to address workplace violence. Such strategies hold promises for effectively reducing instances of workplace violence against healthcare workers, including nurses [63, 64]. Additionally, our study suggests that hospitals should further take measures to enhance their aftermath management for nurses who have experienced workplace violence. Effectively strategies aim to improving work environment and accessibility of psychological counseling may be beneficial for decreasing the frequency of workplace violence and improving these nurse staffs’ psychological health. For example, nursing managers can conduct comprehensive measures to improve staff-patient relationship, such as creating a good nurse atmosphere, strength the accessibility of psychological counseling.
This study has some limitations that should be acknowledged. Firstly, as the data was collected using a cross-sectional design, it is difficult to establish causal relationships between variables. Future longitudinal studies should be conducted to further verify the validity of the findings. Secondly, although we employed PSM analysis to control for potentially confounding demographic variables, other confounding factors (such as nursing department and night shift schedules) may still exist. Future studies could build upon these findings by conducting a more in-depth analysis that includes these additional factors. Thirdly, our sample only includes participants from Dehong districts in Yunnan province, and as such, the representativeness of the results may not extend to nursing staff throughout China. Finally, participant information was derived from self-reporting, which may have introduced self-reporting bias due to participants concealing certain information.
Conclusion
This study offers novel insights into the prevalence of workplace violence (31.5%) among nurse staff from Yunnan-Myanmar Chinese border region. Our findings also highlight the effectiveness of Propensity Score Matching as a statistical tool for controlling the impact of confounding factors and achieving more precise results. As such, future research could benefit from utilizing this approach to enhance precision even further. Furthermore, the data we have gathered presents a strong association between nurse staff exposed to workplace violence and experiences of loneliness, perceived cognitive deficits, anxiety symptoms, depressive symptoms, poor sleep quality, poor resilience, and lack of social support. These results emphasize the urgent need to implement preventative measures to address this pressing issue in the workplace.

The distribution of propensity score before and after PSM analysis

The absolute standardized mean difference before and after PSM analysis

The effect of workplace violence on mental health outcomes before and after PSM analysis
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.`.
Abbreviations
- WPV:
-
Workplace violence
- RCTs:
-
Randomized controlled trials
- PSM:
-
propensity score matching analysis
- GAD-7:
-
The generalized anxiety disorder-7
- CDRISC-10:
-
The Connor Davidson Resilience Scale – 10 item
- PHQ-9:
-
the 9-item Patient Health Questionnaire
References
Hahn S, Müller M, Hantikainen V, Kok G, Dassen T, Halfens RJ. Risk factors associated with patient and visitor violence in general hospitals: results of a multiple regression analysis. Int J Nurs Stud. 2013;50(3):374–85. https://doi.org/10.1016/j.ijnurstu.2012.09.018.
Lu L, Lok KI, Zhang L, Hu A, Ungvari GS, Bressington DT, Cheung T, An FR, Xiang YT. Prevalence of verbal and physical workplace violence against nurses in psychiatric hospitals in China. Arch Psychiatr Nurs. 2019;33(5):68–72. https://doi.org/10.1016/j.apnu.2019.07.002.
Spector PE, Zhou ZE, Che XX. Nurse exposure to physical and nonphysical violence, bullying, and sexual harassment: a quantitative review. Int J Nurs Stud. 2014;51(1):72–84. https://doi.org/10.1016/j.ijnurstu.2013.01.010.
Hersi NSALAHALSSAL. Depression among physicians and other medical employees involved in the COVID-19 outbreak: a cross-sectional study. Medicine. 2021;100(15):e25290. https://doi.org/10.1097/md.0000000000025290.
Portoghese I, Galletta M, Leiter MP, Cocco P, D’Aloja E, Campagna M. Fear of future violence at work and job burnout: a diary study on the role of psychological violence and job control. Burnout Res. 2017;7:36–46.
Szczygiel DD, Mikolajczak M. Emotional Intelligence Buffers the Effects of Negative Emotions on Job Burnout in Nursing. 2018.
Cheung T, Yip P. Workplace violence towards nurses in Hong Kong: prevalence and correlates. BMC Public Health 2017, 17(196).
Magnavita N, Di Stasio E, Capitanelli I, Lops EA, Chirico F, Garbarino S. Sleep problems and Workplace Violence: a systematic review and Meta-analysis. Front NeuroSci. 2019;13:997. https://doi.org/10.3389/fnins.2019.00997.
Nielsen MB, Harris A, Pallesen S, Einarsen SV. Workplace bullying and sleep - A systematic review and meta-analysis of the research literature. Sleep Med Rev. 2020;51:101289. https://doi.org/10.1016/j.smrv.2020.101289.
Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, Wu J, Du H, Chen T, Li R, et al. Exposed to Coronavirus Disease 2019. JAMA Netw open. 2020;3(3):e203976. https://doi.org/10.1001/jamanetworkopen.2020.3976. Factors Associated With Mental Health Outcomes Among Health Care Workers.
Li D, Wang Y, Yu H, Duan Z, Peng K, Wang N, Zhou Q, Hu X, Fang K, Wilson A, et al. Occupational Burnout among Frontline Health Professionals in a high-risk area during the COVID-19 outbreak: a structural equation Model. Front Psychiatry. 2021;12:575005. https://doi.org/10.3389/fpsyt.2021.575005.
Rodriguez RM, Montoy JCC, Hoth KF, Talan DA, Harland KK, Eyck PT, Mower W, Krishnadasan A, Santibanez S, Mohr N. Symptoms of anxiety, Burnout, and PTSD and the Mitigation Effect of Serologic Testing in Emergency Department Personnel during the COVID-19 pandemic. Ann Emerg Med. 2021;78(1):35–43. https://doi.org/10.1016/j.annemergmed.2021.01.028.
Maunder RG, Lancee WJ, Balderson KE, Bennett JP, Borgundvaag B, Evans S, Fernandes CM, Goldbloom DS, Gupta M, Hunter JJ, et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg Infect Dis. 2006;12(12):1924–32. https://doi.org/10.3201/eid1212.060584.
Badhiwala JH, Karmur BS, Wilson JR. Propensity score matching: a powerful Tool for analyzing Observational Nonrandomized Data. Clin spine Surg. 2021;34(1):22–4. https://doi.org/10.1097/bsd.0000000000001055.
Schober P, Vetter TR. Propensity score matching in Observational Research. Anesth Analg. 2020;130(6):1616–7. https://doi.org/10.1213/ane.0000000000004770.
Liang J, Hu Z, Zhan C, Wang Q. Using propensity score matching to Balance the baseline characteristics. J Thorac oncology: official publication Int Association Study Lung Cancer. 2021;16(6):e45–6. https://doi.org/10.1016/j.jtho.2020.11.030.
Statistical Communiqué of Dehong Dai and Jingpo Autonomous Prefecture on the National Economic. and Social Development in 2021 [https://tjgb.hongheiku.com/djs/31259.html].
Ye S. Dehong Border Anti-Epidemic: guarding the Country door for my Motherland. Today’s Nationalities (Chinese). 2022;1:39–41.
Kang L, Ma S, Chen M, Yang J, Wang Y, Li R, Yao L, Bai H, Cai Z, Xiang Yang B, et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: a cross-sectional study. Brain Behav Immun. 2020;87:11–7. https://doi.org/10.1016/j.bbi.2020.03.028.
Wang PX, Wang MZ, Hu GX, Wang ZM. [Study on the relationship between workplace violence and work ability among health care professionals in Shangqiu City]. Wei sheng yan jiu = Journal of hygiene research. 2006;35(4):472–4.
Tian Y, Yue Y, Wang J, Luo T, Li Y, Zhou J. Workplace violence against hospital healthcare workers in China: a national WeChat-based survey. BMC Public Health. 2020;20(1):582. https://doi.org/10.1186/s12889-020-08708-3.
Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two Population-Based Studies. Res aging. 2004;26(6):655–72. https://doi.org/10.1177/0164027504268574.
Snyder E, Cai B, DeMuro C, Morrison MF, Ball W. A new single-item Sleep Quality Scale: results of psychometric evaluation in patients with chronic primary insomnia and depression. J Clin sleep medicine: JCSM : official publication Am Acad Sleep Med. 2018;14(11):1849–57. https://doi.org/10.5664/jcsm.7478.
Gupta B, Sharma V, Kumar N, Mahajan A. Anxiety and sleep disturbances among Health Care Workers during the COVID-19 pandemic in India: cross-sectional online survey. JMIR public health and surveillance. 2020;6(4):e24206. https://doi.org/10.2196/24206.
Dereli M, Kahraman T. Validity and reliability of the turkish version of single-item Sleep Quality Scale in healthy adults. Sleep Med. 2021;88:197–203. https://doi.org/10.1016/j.sleep.2021.10.032.
Pan Y, Xin M, Zhang C, Dong W, Fang Y, Wu W, Li M, Pang J, Zheng Z, Wang Z, et al. Associations of Mental Health and Personal Preventive measure compliance with exposure to COVID-19 Information during Work Resumption following the COVID-19 outbreak in China: cross-sectional survey study. J Med Internet Res. 2020;22(10):e22596. https://doi.org/10.2196/22596.
Fu L, Fang Y, Luo D, Wang B, Xiao X, Hu Y, Ju N, Zheng W, Xu H, Yang X, et al. Pre-hospital, in-hospital and post-hospital factors associated with sleep quality among COVID-19 survivors 6 months after hospital discharge: cross-sectional survey in five cities in China. BJPsych open. 2021;7(6):e191. https://doi.org/10.1192/bjo.2021.1008.
Moscovici M, Wnuk S, Okrainec A, Hawa R, Sockalingam S. Psychosocial predictors of cognition in bariatric surgery. Psychosomatics. 2019;60(2):164–71. https://doi.org/10.1016/j.psym.2018.06.010.
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7. https://doi.org/10.1001/archinte.166.10.1092.
Labrague LJ, De Los Santos JAA. COVID-19 anxiety among front-line nurses: predictive role of organisational support, personal resilience and social support. J Nurs Adm Manag. 2020;28(7):1653–61. https://doi.org/10.1111/jonm.13121.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x.
Tu ZH, He JW, Zhou N. Sleep quality and mood symptoms in conscripted frontline nurse in Wuhan, China during COVID-19 outbreak: a cross-sectional study. Medicine. 2020;99(26):e20769. https://doi.org/10.1097/md.0000000000020769.
Huo L, Zhou Y, Li S, Ning Y, Zeng L, Liu Z, Qian W, Yang J, Zhou X, Liu T, et al. Burnout and its relationship with depressive symptoms in Medical Staff during the COVID-19 epidemic in China. Front Psychol. 2021;12:616369. https://doi.org/10.3389/fpsyg.2021.616369.
Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-davidson Resilience Scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–28. https://doi.org/10.1002/jts.20271.
Ye ZJ, Qiu HZ, Li PF, Chen P, Liang MZ, Liu ML, Yu YL, Wang SN, Quan XMJEJoON. Validation and application of the chinese version of the 10-item Connor-Davidson Resilience Scale (CD-RISC-10) among parents of children with cancer diagnosis. 2017, 27:36–44.
Cheng ST, Chan AJP, Differences I. The multidimensional scale of perceived social support: dimensionality and age and gender differences in adolescents. 2004, 37(7):1359–69.
Ding C, Chen X, Wang W, Yu B, Yang H, Li X, Deng S, Yan H, Li S. Sexual minority stigma, sexual orientation concealment, Social Support and depressive symptoms among men who have sex with men in China: a moderated mediation modeling analysis. AIDS Behav. 2020;24(1):8–17. https://doi.org/10.1007/s10461-019-02713-3.
Morgan CJ. Reducing bias using propensity score matching. J nuclear cardiology: official publication Am Soc Nuclear Cardiol. 2018;25(2):404–6. https://doi.org/10.1007/s12350-017-1012-y.
Dasrilsyah RA, Ng BK, Atan IK, Khong SY, Nusee Z, Lim PS. Validation of the malay version of the p-QOL questionnaire. Int Urogynecol J. 2021;32(12):3163–7. https://doi.org/10.1007/s00192-020-04362-w.
Korrel M, Lof S, Alseidi AA, Asbun HJ, Boggi U, Hogg ME, Jang JY, Nakamura M, Besselink MG, Abu Hilal M. Framework for Training in minimally invasive pancreatic surgery: an International Delphi Consensus Study. J Am Coll Surg. 2022;235(3):383–90. https://doi.org/10.1097/xcs.0000000000000278.
Phillips JP, Workplace Violence against Health Care Workers in the United States. N Engl J Med. 2016;374(17):1661–9. https://doi.org/10.1056/NEJMra1501998.
Shi L, Li G, Hao J, Wang W, Chen W, Liu S, Yu Z, Shi Y, Ma Y, Fan L, et al. Psychological depletion in physicians and nurses exposed to workplace violence: a cross-sectional study using propensity score analysis. Int J Nurs Stud. 2020;103:103493. https://doi.org/10.1016/j.ijnurstu.2019.103493.
Babiarczyk B, Turbiarz A, Tomagová M, Zeleníková R, Önler E, Sancho Cantus D. Reporting of workplace violence towards nurses in 5 european countries - a cross-sectional study. Int J Occup Med Environ Health. 2020;33(3):325–38. https://doi.org/10.13075/ijomeh.1896.01475.
Lu L, Dong M, Wang SB, Zhang L, Ng CH, Ungvari GS, Li J, Xiang YT. Prevalence of Workplace Violence Against Health-Care Professionals in China: a comprehensive Meta-analysis of observational surveys. Trauma violence & abuse. 2020;21(3):498–509. https://doi.org/10.1177/1524838018774429.
Yang Y, Li Y, An Y, Zhao YJ, Zhang L, Cheung T, Hall BJ, Ungvari GS, An FR, Xiang YT. Workplace violence against chinese Frontline Clinicians during the COVID-19 pandemic and its Associations with demographic and clinical characteristics and quality of life: a structural equation modeling investigation. Front Psychiatry. 2021;12:649989. https://doi.org/10.3389/fpsyt.2021.649989.
Han X, Jiang F, Shen L, Liu Y, Liu T, Liu H, Wang P, Yang Z, Tang YL, Zhu J. Workplace Violence, Workforce Stability, and well-being in China’s Psychiatric Hospitals. Am J Prev Med. 2022;62(4):e265–73. https://doi.org/10.1016/j.amepre.2021.09.013.
Newman C, Roche M, Elliott D. Exposure to workplace trauma for forensic mental health nurses: a scoping review. Int J Nurs Stud. 2021;117:103897. https://doi.org/10.1016/j.ijnurstu.2021.103897.
Zhao S, Xie F, Wang J, Shi Y, Zhang S, Han X, Sun Z, Shi L, Li Z, Mu H, et al. Prevalence of Workplace Violence against Chinese Nurses and its Association with Mental Health: a cross-sectional survey. Arch Psychiatr Nurs. 2018;32(2):242–7. https://doi.org/10.1016/j.apnu.2017.11.009.
Faghihi M, Farshad A, Abhari MB, Azadi N, Mansourian M. The components of workplace violence against nurses from the perspective of women working in a hospital in Tehran: a qualitative study. BMC Womens Health. 2021;21(1):209. https://doi.org/10.1186/s12905-021-01342-0.
Yang Y, Wang P, Kelifa MO, Wang B, Liu M, Lu L, Wang W. How workplace violence correlates turnover intention among chinese health care workers in COVID-19 context: the mediating role of perceived social support and mental health. J Nurs Adm Manag. 2022;30(6):1407–14. https://doi.org/10.1111/jonm.13325.
Tong C, Cui C, Li Y, Wang L. The Effect of Workplace Violence on depressive symptoms and the Mediating Role of Psychological Capital in Chinese Township General Practitioners and Nurses: a cross-sectional study. Psychiatry Invest. 2019;16(12):896–903. https://doi.org/10.30773/pi.2019.0095.
Hobfoll SE. Conservation of resource caravans and engaged settings. J Occup Organizational Psychol. 2011;84(1):116–22.
Magnavita N, Mele L, Meraglia I, Merella M, Vacca ME, Cerrina A, Gabriele M, Labella M, Soro MT, Ursino S, et al. The impact of Workplace violence on headache and sleep problems in nurses. Int J Environ Res Public Health. 2022;19(20). https://doi.org/10.3390/ijerph192013423.
El-Zoghby SM, Ibrahim ME, Zaghloul NM, Shehata SA, Farghaly RM. Impact of workplace violence on anxiety and sleep disturbances among egyptian medical residents: a cross-sectional study. Hum Resour health. 2022;20(1):84. https://doi.org/10.1186/s12960-022-00786-1.
Sun T, Gao L, Li F, Shi Y, Xie F, Wang J, Wang S, Zhang S, Liu W, Duan X, et al. Workplace violence, psychological stress, sleep quality and subjective health in chinese doctors: a large cross-sectional study. BMJ open. 2017;7(12):e017182. https://doi.org/10.1136/bmjopen-2017-017182.
Giorgi F, Mattei A, Notarnicola I, Petrucci C, Lancia L. Can sleep quality and burnout affect the job performance of shift-work nurses? A hospital cross-sectional study. J Adv Nurs. 2018;74(3):698–708. https://doi.org/10.1111/jan.13484.
Hawker DS, Boulton MJ. Twenty years’ research on peer victimization and psychosocial maladjustment: a meta-analytic review of cross-sectional studies. J Child Psychol Psychiatry Allied Discip. 2000;41(4):441–55.
Brunes A, M BH, Heir T. Loneliness among adults with visual impairment: prevalence, associated factors, and relationship to life satisfaction. Health Qual Life Outcomes. 2019;17(1):24. https://doi.org/10.1186/s12955-019-1096-y.
Qualter P, Vanhalst J, Harris R, Van Roekel E, Lodder G, Bangee M, Maes M, Verhagen M. Loneliness across the life span. Perspect Psychol science: J Association Psychol Sci. 2015;10(2):250–64. https://doi.org/10.1177/1745691615568999.
Drageset J, Kirkevold M, Espehaug B. Loneliness and social support among nursing home residents without cognitive impairment: a questionnaire survey. Int J Nurs Stud. 2011;48(5):611–9. https://doi.org/10.1016/j.ijnurstu.2010.09.008.
Srivastava S, Muhammad T. Violence and associated health outcomes among older adults in India: a gendered perspective. SSM - population health. 2020;12:100702. https://doi.org/10.1016/j.ssmph.2020.100702.
Savopoulos P, Brown S, Anderson PJ, Gartland D, Bryant C, Giallo R. Intimate partner violence during infancy and cognitive outcomes in middle childhood: results from an australian community-based mother and child cohort study. Child Dev. 2022;93(4):e396–e411. https://doi.org/10.1111/cdev.13736.
Liu J, Zheng J, Liu K, Liu X, Wu Y, Wang J, You L. Workplace violence against nurses, job satisfaction, burnout, and patient safety in chinese hospitals. Nurs Outlook. 2019;67(5):558–66. https://doi.org/10.1016/j.outlook.2019.04.006.
Li M, Shu Q, Huang H, Bo W, Wang L, Wu H. Associations of occupational stress, workplace violence, and organizational support on chronic fatigue syndrome among nurses. J Adv Nurs. 2020;76(5):1151–61. https://doi.org/10.1111/jan.14312.
Acknowledgements
We would like to thank all nurses who generously shared their time to participate in this survey.
Funding
No.
Author information
Authors and Affiliations
Contributions
CM D, LD L, ZZ D analyzed the data and wrote manuscript; ZZ D and CM D revised the manuscript; GZ L, XH L, LLX, and ZZ D edited the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Participants provided written informed consent, and the Ethics Committee of Dehong people’s hospital in China (Number: DYLL-KY032) approved this study. And all methods were performed in accordance with t Declaration of Helsinki.
Consent for publication
No applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ding, C., Li, L., Li, G. et al. Impact of workplace violence against psychological health among nurse staff from Yunnan-Myanmar Chinese border region: propensity score matching analysis. BMC Nurs 22, 242 (2023). https://doi.org/10.1186/s12912-023-01402-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-023-01402-w