
Abstract
Background
Hypertension is a public health concern for many countries. The World Health Organization has established a global objective to reduce the prevalence of non-communicable diseases, including hypertension, which is associated with cardiovascular disease. Remote nursing interventions can potentially lessen the burden on the healthcare system and promote a healthier population. This systematic review aims to synthesize available evidence on the effectiveness of nursing-led telehealth interventions in reducing blood pressure in hypertensive patients.
Methods
A systematic review was conducted. The search was performed from May to June 2021, in the databases: PubMed, Scopus, Cochrane Library, Web of Science, CINAHL, and ProQuest within 2010–2021 in English, Spanish and Portuguese. Randomized controlled trials and Quasi-experimental studies were considered. This systematic review followed the criteria of the Cochrane Handbook for Systematic Reviews of Interventions, with the support of the PRISMA guidelines and registered in PROSPERO. For critical analysis, the tools of the Joanna Briggs Institute were used.
Results
Of the 942 articles found, six controlled clinical trials and one quasi-experimental study were selected. Different nurse-led interventions (telehealth devices, remote video consultation, calls and email alerts) have demonstrated a significant decrease in blood pressure (especially systolic blood pressure) in the intervention groups. Nurse-led interventions also effect hypertension awareness, self-efficacy, and self-control. Positive effects on lowering cholesterol, consumption of fruits and vegetables, physical activity and adherence to medication were also described.
Conclusion
Nurse-led interventions delivered remotely have a positive effect in lowering the blood pressure of patients with hypertension. Further research is required to support strategies that will deliver the best continuous, quality, and cost-effective nursing care.
Similar content being viewed by others


Introduction
In 2019, 17.9 million people died from cardiovascular diseases (CVDs) which represents 32% of all global deaths [1]. Hypertension is one of the most important risk factors in the development of CVD [2] and currently, 30% of the world’s population, or approximately one billion people are affected by hypertension [3]. Given hypertension’s relationship to CVD, the World Health Organization (WHO) (2021) established a goal to reduce hypertension by 25% by 2025 [1].
Worldwide, the prevalence of hypertension is higher in low- and middle-income countries, due to the presence of more risk factors associated with diet (consumption of saturated fat and salt) and lifestyle (smoking, sedentary behavior) [2]. The prevalence of complications from hypertension is also greater in low- and middle-income countries, where 50% of mortality from cardiovascular causes occurs between 30 and 69 years, 10 years earlier than in higher-income countries [4]. This problem is especially important in countries that have a rural or dispersed population or those with small numbers of health care providers [5].
Background
Hypertension, defined as systolic blood pressure (BP) of 130 mmHg or above or diastolic BP of 80 mmHg or above is the main risk factor for CVDs [6], including coronary heart disease, stroke, chronic kidney disease [7], heart failure, arrhythmia, and dementia. Healthy diet (normal salt consumption, low saturated and trans-fat consumption, a high intake of fruits and vegetables), physical activity, and normal weight decrease the risk of developing hypertension. Lifestyle change is a main component in decreasing blood pressure and the related cardiovascular risk [8].
The COVID-19 pandemic has increased barriers of face-to-face interactions between patients and healthcare providers, particularly in primary health settings. To continue to provide care for patients, nurses have begun incorporating different strategies to care for their patients, such as telehealth interventions to monitor and support patients with chronic conditions like hypertension [9, 10].
The concept of telehealth has been in use for more than 30 years, but it was not given a definition by WHO until 2007. The WHO defines telehealth as the deliberate use of communication technologies by healthcare professionals for the diagnosis, treatment and prevention of diseases, as well as the research and continuing education of patients, families and communities where distance between the user(s) and health professionals is a critical factor. According to Mann et al. [11] and Omboni et al. [12], telehealth (also called telemedicine) can be defined as the use of electronic resources to provide efficient and high-quality healthcare. It includes the diagnosis and treatment of patients, as well as the enhancement of patient monitoring techniques such as checking vital signs or reporting symptoms, all with telecommunications technology like smartphones and computers [1, 13]. With the telehealth model, patients do not have to leave their homes to receive a diagnosis or testing results. Telehealth delivery is practiced in all settings and requires the support of different healthcare professionals. The nurse has a vital role in much of this delivery.
The COVID-19 pandemic, declared as such by WHO in March 2020, increased the use of telemedicine to treat patients in many countries [14,15,16]. Telehealth made it possible to provide diverse care services for patients with chronic diseases. These remote services were fundamental during the pandemic, alleviating the shortage of medical resources and reducing the risk of infection in hospitals and medical centers [17]. In regard to hypertensive patients, telehealth is presented as an opportunity for routine care and continuation of treatment at home even beyond the pandemic [13]. The increased demands for telehealth during the COVID-19 pandemic show the need to prepare nurses to support telehealth and to take the lead in its integration within the healthcare system.
Nursing-led interventions are based on a care delivery model that incorporates assessment, evaluation, education, counseling, treatment and other procedures using a comprehensive nurse-patient (family) approach, with the nursing professional working independently or in interdisciplinary teams [18].
Multiple systematic reviews completed in the last decade have investigated the impact of nursing-led interventions in patients with hypertension, with the incorporation of new roles such as advanced nursing practice [6, 19,20,21]. Jointly with advanced nursing practices, nursing-led clinical practices emerge, with interventions that, in addition to counseling and education for patient self-management, incorporate the diagnosis and prescription of medications [19]. Patients express a greater satisfaction and adherence to treatment when guided by nursing-led interventions [21], especially compared to medical management alone [22]. A decrease in cardiovascular adverse events and mortality have also been reported with the use of nursing-led interventions [20], where continuity of care has shown a reduction of hospitalizations and readmissions [21]. Since the onset of the COVID-19 pandemic, improvements in remote monitoring of BP coordinated by nurses compared to usual care have been reported [6]. Additionally, the global costs associated with hypertension mortality have increased exponentially in recent years [23]; self-monitoring of BP has been reported as a cost-effective measure to reduce arterial hypertension morbidity and mortality indicators [24].
This systematic review will synthesize recent evidence of the effectiveness of nursing-led telehealth interventions on hypertensive patients to reduce their high blood pressure, actively exploring the potential of telemedicine to solve the current and future health problems.
Review
Aims
This study will explore the effectiveness of nurse-led telehealth interventions in adult patients with hypertension. Randomized controlled trials (RCTs) and quasi-experimental studies that explored the effectiveness or impact of telehealth nursing-led interventions on high blood pressure were included in this review. Secondary outcomes of the review included adherence to the antihypertensive therapy and healthy lifestyle behaviors such as smoking, drinking, exercise, and sleep hours.
Design
A systematic review was performed according to the protocol and extraction form in the Cochrane Handbook for Systematic Reviews of Interventions, version 6.0. [25] The review protocol was registered in PROSPERO (ID: CRD42021262081) and the PRISMA statement was followed to guide this review [26]. Our initial research question was, are nursing-led telehealth interventions effective in lowering blood pressure in hypertensive patients?
Search methods
The literature search was conducted on PubMed, Scopus, Cochrane Library, Web of Science, CINAHL, and ProQuest from May to July 2021, using the following keywords: Search (Nursing Interventions) AND (Telehealth)) AND (high blood pressure) Filters: Clinical Trial, Randomized Controlled Trial, from 2010 to 2021 Languages English, Spanish and Portuguese.
Reference lists of publications were searched for potentially relevant articles. Grey literature and thesis were also included. The authors consulted a medical librarian in order to help expand the search as noted in Additional file 1: Appendix 1.
Inclusion criteria and study selection
To identify all eligible studies, this review considered the following study designs, populations, interventions, and outcome(s):
-
Study design: Randomized Controlled trials and quasi-experimental studies.
-
Population: Hypertensive adult patients, with or without other comorbidities like diabetes, obesity, and dyslipidemia.
-
Interventions: All types of telehealth or phone technologies conducted by nurses, including M-health, telehealth, telemonitoring, virtual interventions, e-coaching, panel monitoring.
-
Outcomes: The primary outcome was change in blood pressure, systolic (mmHg) and diastolic pressure (mmHg) or mean arterial pressure (mmHg).
Exclusion criteria
Review articles, letters to the editor, book chapters, protocols, and prospective observational designs were excluded. Articles on telehealth interventions done by professionals other than nursing were not considered.
Search outcomes
According to the inclusion and exclusion criteria, three authors (MK, PE, and VJ) each independently extracted data to check and compare against each other’s work. Microsoft excel (version 16.0) was used to collate the extracted data.
A standardized data extraction form was used to extract data from each study, which included the following criteria: author’s names, country, participants, sample size, intervention/control groups, follow-up period, measurement tools, and results. Rayyan software was used to manage and organize the articles used in this review.
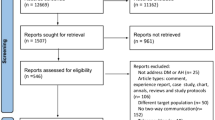
Nine hundred and forty-two articles were identified with the search strategy. (Fig. 1) In the first stage, duplicate articles and those that did not agree with the objective of the study were excluded based on reading the abstract and title. Of the 24 articles that remained, 16 were excluded because nurses were not involved in the intervention. One article was excluded because it did not describe a nursing-led intervention. Therefore, 7 articles were included in this review.

PRISMA article selection flowchart
Quality appraisal and data extraction
Quality assessment was based on the use of the critical analysis tools of the Joanna Briggs Institute [27]. These tools were selected because each checklist contained an explanation of how to respond appropriately to each item. This tool has also been well evaluated compared with others and is appropriate to use in nursing research [28].
In this review, we used different tools to evaluate controlled clinical trials and quasi-experimental studies (Additional file 2: Appendix 2). These tools consisted of 13 and 9 points, respectively. Each question on the list was answered with “yes,” “no” or “unclear.“ When using the critical analysis tools, we used 2 criteria to decide to include the studies thereby ensuring quality. First, the studies needed to meet at least 60% of the criteria outlined by Chan et al [29] for controlled clinical trials. Second, they also had to meet the following criteria from the tool:
-
“Was true randomization used for assignment of participants to treatment groups?”
-
“Were treatment groups similar at the baseline?”
-
“Were outcome assessors blind to treatment assignment?”
-
“Were outcomes measured in the same way for treatment groups?”
The authors required the use these criteria as mandatory elements in order to accept the study for inclusion because they are critical for identifying the risk of bias [25].
Two independent reviewers performed the critical evaluations. In the event of a disagreement between evaluators, a third evaluator was asked to review the study. Following this critical analysis, the studies were included in this review (Fig. 1).
Synthesis
The data from the included studies information was transferred into an excel table with the items: authors, the aim of the study, population, design, duration, intervention, outcomes, and findings. Although the population and outcomes of the studies were comparable, there was great heterogeneity within the interventions performed, which is why it was impossible to conduct a meta-analysis. Therefore, results are presented in narrative form.
Results
Through the search strategy, 942 articles were identified. After applying the inclusion and exclusion criteria, 7 articles were included in the final analysis. Figure 1 summarizes the search, identification and selection process of the articles included in this review. The results of the critical evaluation of these 7 studies are summarized in Additional file 3: Appendix 3. Of the 7 studies included in the systematic review, 6 were RCTs and 1 was a quasi-experimental study. A total of 2102 participants completed the studies, and their data were included in the analysis. Age of patients ranged from 54 to 77 years old. The number of female participants was slightly larger than male, and the races included were primarily White, Hispanic and African American. Educational level, familiar arrangements and Body Mass Index (BMI) were reported in all of the studies.
Sample sizes of some of the included studies were calculated using power analysis [6, 30], while the others didn’t mention how they were calculated [31,32,33,34,35]. Wakefield et al. [31] and Bosworth et al. [30] used a random number generator to select participants, in the other 5 studies sampling was done with purpose [6, 32,33,34,35]. Four studies used a randomization process to allocate participants into different groups [6, 31,32,33]. Brennan [32] used a blind recruitment process, as a blind allocating process was used in 3 studies [33,34,35].
All 7 studies (Table 1) included 1 control group and a different number of intervention groups. Some of them had 1 group [6, 32, 33], some 2 [31, 34], and others 3 groups of participants [30, 35]. While the majority of the studies included single set type of intervention, 2 studies involved mixing intervention content [30, 35]. One study used different levels of monitoring and educational content with all the participants [31], and every study included one control group that received normal care. In terms of follow-up, two studies had a follow-up time of 2 months [6, 35], three studies a 6-month follow-up period [32, 33], one a 12 month follow up [31] and two 18-months follow up [30, 34].
In terms of intervention, one offered home telehealth devices to improve blood pressure, while a nurse manager reviewed daily data from a blood pressure monitoring device and responses of participants to decide if a closer follow-up, information, reinforcement or referral to health care provider was needed using inbound–outbound remote video consultation [31]. Cicolini el al. [33] and Hebert et al. [34] offered a one-time educational program about using the home BP monitor, strategies to improve medication adherence and healthy lifestyle done by a nurse care manager, plus phone calls, and email alerts to reinforce the information and do a follow-up of participants. Brennan et al. [32] did monthly telephone follow ups of about 15 to 20 min to reinforce hypertension knowledge, medication adherence and support lifestyle changes such as smoking cessation, regular exercise, and healthy diet. Kim [35] and Bosworth et al. [30] used long message service and phone-based health coaching to provide evidence-based recommendations regarding hypertension related behaviors. Kim [35] used an 8-week coaching program and monthly long-distance message, while Bosworth et al. [30] used a behavioral management program of 11 weeks with reinforcing messages, e-mails and calls. Choi’s et al. [6] intervention consisted of a remote consultation twice a week for 8 weeks done by licensed and trained nurses.
Some of the studies’ interventions used algorithms based on guidelines about disease management, lifestyle modification, and treatment, to provide educational content [30,31,32,33,34]. The only one reporting a theoretical framework for the intervention was Kim [35] using Cox’s Interaction Model of Client Health Behavior to develop phone-based health coaching. Only one study did not provide a clear description to support their intervention [6].
Concerning the professional nurses participating in the 7 studies, some were nurses [30], registered nurses [34] with some with previous experience in delivering home telehealth and nursing care management [31, 33], while others were trained licensed nurses [6]. The disease management nurses received training in cardiac care and cultural care competency before the study [32], and registered nurses were required to complete over 40 h of training in phone-based health coaching [35]. Herbert et al. [34] used a trained nurse for the intervention arm without providing details in terms of the type of training or education that was delivered. None of the studies described if the intervention nurses had any postgraduate education such as a BSN, MSN or doctoral degree.
Nurse-led interventions included educational interventions [6, 30, 32,33,34], such as training the patient to measure blood pressure [6, 30, 32,33,34], performing patients remote consultation, undertaking video conferences with the participants [30], taking responsibility for phone calls and email [31,32,33,34,35] doing long message service and delivering phone health coaching to participants [35] or using a software application to deliver educational scripts and algorithms [30]. In Herbert et al. [34] study, nurses contacted patient’s clinicians to address medications problems and arrange any prescription changes.
Effects of interventions on patients’ blood pressure
The Wakefield et al. [31] study compared two remote monitoring intensity levels and usual care in hypertensive patients with type 2 diabetes being treated in primary care. The high-intensity group received a set of messages based on a disease management algorithm programmed into an electronic device focusing on diet, exercise, smoking cessation, foot care, advice for sick days, medications, weight management, preventive care, and behavior modification and lifestyle showed significant improvement (p = 0.001) on the blood pressure compared with the low intensity group (not set of messages or algorithm) and the usual care group. The Choi et al. [6] study compared remote video consultation and blood pressure monitoring vs. only blood pressure monitoring. The difference in resulting systolic BP between the control and experimental groups was statistically significant, although the difference in diastolic BP was not statistically significant. The strategy used in the study by Cicolini et al. [33] consisted of an educational program for both groups and was added to the experimental group weekly email alerts and phone calls from a nurse care manager. Systolic and diastolic blood pressure significantly decreased in both groups (all p < 0.01) but in the intervened group, obesity, low fruit consumption, total cholesterol and uncontrolled arterial pressure decreased more significantly.
A study conducted by Kim [35] reviewed the efficacy of telephone messages on patients’ blood pressure. Phone-based health-coaching with long message service was effective in decreasing systolic BP as compared to long message service only (p < 0.05). In another study, the systolic BP adjusted mean of the intervention group was significantly lower than of the control group (123.6 vs. 126.7, P.0.03) post-intervention, nevertheless, there was no statistically significant difference in diastolic BP between the groups at the end of the intervention [32].
All patients of the intervention arm (3 groups) of Bosworth et al. [30] study used telemedicine and home BP monitoring compared to the usual care group. The improvement in BP control to usual care at 12 months was statically significant in the first group that received behavioral management by nurses with 12.8% (95% CI, 1.6–24.1%; P = 0.03) and also on the medication management group with the physician and the nurse working together with 12.5% (95% CI, 1.3–23.6%; P = 0.03). Differences on BP with the third intervention (combination of intervention 1 and 2) and usual care were not statistically significant.
Herbert et al. [34] divided participants into three groups, the first involved BP monitoring and registered nurse counseling and telephone follow up for 9 months, the second only received the BP monitor, and the third group received usual care. The statistically significant changes on BP from intervention groups to usual care were only at 9 months. On the first intervention was − 7.0 mm Hg (Confidence Interval [CI], -13.4 to − 0.6) and in the second was + 1.1 mm Hg (95% CI, -5.5 to 7.8).
Effects of intervention on patient adherence to medication and healthy lifestyle
Adherence to medication was assessed using one question of the Morisky Medication Adherence Scale [36], and improved over time for both groups, although there was no significant difference among them [33]. In the Wakefield et al. [31] study, adherence to the antihypertensive therapy was measured using two scales and reported no significant differences between the 3 groups. Medication adherence in Kim study [35] was measured using a scale developed by Morisky et al. [36] and the results showed significant differences between the 4 groups. An adjusted version of Healthy Lifestyles and Lifestyle Behavior tool were used in the Choi et al. [6] study, and the results indicated that the only significant difference found was in sleep patterns and hobbies. Physical activity was evaluated through a questionnaire previously validated by the authors and was compared between the intervention and control group showing a statistically significantly greater improvement in BMI, alcohol consumption, cigarette smoking, fruit consumption, and physical activity on the intervention arm of the study [33].
Discussion
The purpose of this systematic review was to explore the effectiveness of nursing-led telehealth interventions on adult patients with high blood pressure. This systematic review indicates that different nurse-led interventions (telehealth devices, remote video consultation, calls and email alerts) demonstrated a significant decrease in blood pressure (especially systolic blood pressure) in intervention groups. Nurse-led interventions also effect hypertension awareness, self-efficacy, and self-control. Positive outcomes related to lowering cholesterol, improving consumption of fruits and vegetables, increased physical activity and adherence to medication were also described.
The findings of the systematic review included different populations, all of them reported interventions guided, managed, and performed by nurses. These results are consistent with a systematic review completed in 2021 which reported that nurse-led interventions provided coordinated interventions that support continuity of care for people with chronic disease [18].
The interventions included in this systematic review were effective primarily in achieving changes in blood pressure and as well as improving patients’ knowledge acquisition related to a healthy lifestyle [30, 32, 33, 35]. When reviewing the content of these interventions, common elements were noted such as the quest for medication adherence and the focus on education in healthy lifestyles habits like food consumption, frequent exercise, smoking cessation, etc. The sources of information delivered to patients through the interventions in this systematic review have also been reported in other studies [32, 37, 38] and were based on nationwide guidelines and evidence regarding a healthy lifestyle and blood pressure management.
The technologies used in the present study included electronic devices to measure blood pressure and telehealth devices to enable data transmission. Some of the studies used personalized messages, videoconferencing and videos with information for patient education, however, the majority used emails and telephone calls to provide efficient and high-quality healthcare. Findings from two systematics reviews that studied the use of mobile applications and multiple media (SMS, email and telephone call) to take care of chronic conditions reported different level of outcomes effectiveness [39, 40] and disparities in the quality of the evidence provided [39].
The results of this systematic review have shown that intensity, defined as the frequency of interactions with the participants or in the amount of material delivered to some groups, resulted in differences in blood pressure results. Interactions with participants during the study showed significant variability among the 7 studies and within the studies. For example, one study sent text messages more than once a day depending of the of the BP results [31], others offered remote videoconferencing consultation twice a week [6], one receive email alerts with a reminder of the compliance with heathy lifestyle and occasional phone calls [33] one had monthly telephone interactions with a specific attention to the cultural aspects of care while improving their hypertension knowledge [32] or nursing health coaching for 30 min once a week [35]. Bosworth’s study [30] used 3 types of alert messages triggered by readings of high BP and those messages included elements of a behavioral management intervention. Herbert et al. [34] used regular telephone follow-up (frequency not reported) to reinforce messages on adherence to medication and healthy lifestyles. Findings from a recent systematic review support the findings of the present study reporting improvements in hypertension self-management behavior and medication adherence using interventions that combined tailored messages, interactive communication, and multifaceted functions [41].
Follow-up time in this systematic review ranged from 6 months to one year and nurses were responsible of sending emails or completing phone calls to patients requesting information regarding BP and/or answering questionnaires. All studies reported a loss of participants during the follow-up which may have influenced the results. Perhaps therapeutic relationship building and communication between nurses and their patients on the telehealth context needs different patterns of interaction to build empathy and rapport to facilitate the continuity of care.
Findings of this systematic review specified the nurse’s background and preparation for each study. Four of the studies reported including experienced nurses in the field of chronic disease management [6, 30, 31, 33], one included a nurse manager [34], two studies highlighted the need to have the nurses go through a special course on cultural competency [32] and formal training on telephone health coaching [35] prior to participating in the study. Other studies have reported that Registered Nurses (RN) have the undergraduate preparation to promote healthy lifestyles, prevent the development of disease and deliver care and follow-up to different health conditions on community heath setting [42, 43], never the less, telehealth content and experiences among different levels of nursing education appeared to remain low [44].
Implications for nursing
Health services recognize that interventions developed and performed by nurses support hypertensive patients in controlling their disease and preventing complications, especially in primary care and developing countries. Telehealth has been gaining ground recently as an effective and efficient strategy to deliver health care, especially in remote geographic areas, with an insufficient number of health professionals and a lack of specialized care. The COVID-19 pandemic limited nurse-patient interactions in the health center context and forced the exploration of new strategies that would allow continuity of care, especially in patients with chronic diseases such as hypertension. It is in this context that telehealth is emerging with great force. The results of this systematic review will provide a foundation from which to build standardizing successful nurse-led interventions for patients with hypertension, using the technological resources already available in their healthcare centers including computers, telephones, and smart phones to send e-mails, messages and/or telephone calls. It is hoped that some lessons learned from the COVID-19 pandemic will be transformed into a quality and safe care for all, reaching all who need it, regardless of where they are.
Limitations
There were some limitations to this review. Given the small number of articles found searching the 6 databases, it is possible that the search terms may not have covered all possible terms, though we searched for studies in English, Spanish and Portuguese. As the nurse-led interventions were heterogeneous, especially regarding the type of online resources used, intensity of intervention and follow-up, it was difficult to quantify their benefits and compare one intervention to another. Therefore, most of the results were presented in a narrative summary. Additionally, the effects of the nursing-led interventions delivered remotely might depend upon the nature of the content delivered and the online resources used. The patient’s cultural and educational backgrounds, state of the disease and its complications, and baseline blood pressure level measurements may have influenced the assessment accuracy of nurse -led interventions.
This analysis was limited to a population of adult hypertensive outpatients, and nurse-led interventions may not be able to be generalized to other patients with chronic conditions. More research may be needed to establish a consistent online nurse-led intervention program for patients with hypertension and to test the effectiveness of using different telehealth resources.
Conclusion
Although nurse -led interventions for the management and control of high blood pressure in primary care are effective, it is important to resolve whether they continue to be effective when using technological resources to deliver this care remotely. With the tools used, the selected studies were of high quality, however, the small number of subjects who were evaluated does not allow for generalization of the results.
After searching the scientific literature from the last 10 years, in multiple databases and different languages, and after critically reviewing all relevant studies, this systematic review analyzed only 7 studies to evaluate the effectiveness of nurse -led interventions in controlling high blood pressure in patients diagnosed with hypertension. This study describes the best evidence for making informed decisions regarding the strategies that will deliver the best continuous, quality, and cost-effective nursing care.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
References
World Health Organization. Cardiovascular diseases (CVDs). 2021. Available at: https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds.
Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore-Mensah Y, Elkind MSV, Evenson KR, Eze-Nliam C, Ferguson JF, Generoso G, Ho JE, Kalani R, Khan SS, Kissela BM, Knutson KL, Levine DA, Lewis TT, Liu J, Loop MS, Ma J, Mussolino ME, Navaneethan SD, Perak AM, Poudel R, Rezk-Hanna M, Roth GA, Schroeder EB, Shah SH, Thacker EL, VanWagner LB, Virani SS, Voecks JH, Wang NY, Yaffe K, Martin SS. Heart Disease and Stroke Statistics-2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153–639. https://doi.org/10.1161/CIR.0000000000001052. Epub 2022 Jan 26. Erratum in: Circulation. 2022 Sep 6;146(10):e141. PMID: 35078371.
World Hypertension Day. PAHO/WHO | Pan American Health Organization. 2020. Available from: https://www.paho.org/en/campaigns/world-hypertension-day-2020. Cited 2022 Nov 17.
Gheorghe A, Griffiths U, Murphy A, et al. The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review. BMC Public Health. 2018;18:975. https://doi.org/10.1186/s12889-018-5806-x.
Li X, Li T, Chen J, Xie Y, An X, Lv Y, et al. A wechat-based self-management intervention for community middle-aged and elderly adults with hypertension in Guangzhou, China: a cluster-randomized controlled trial. Int J Environ Res Public Health. 2019;16:4058. https://doi.org/10.3390/ijerph16214058.
Choi H, Kim J. Effectiveness of telemedicine: videoconferencing for low-income elderly with hypertension. Telemed J E Health. 2014;20(12):1156–64. https://doi.org/10.1089/tmj.2014.0031.
Tam TSC, Wu MHY, Masson SC, Tsang MP, Stabler SN, Kinkade A, Tung A, Tejani AM. Eplerenone for hypertension. Cochrane Database Syst Rev 2017. (2):CD008996. https://doi.org/10.1002/14651858.CD008996.pub2. Accessed 30 Jul 202.
Ozemek C, Tiwari S, Sabbahi A, Carbone S, Lavie CJ. Impact of therapeutic lifestyle changes in resistant hypertension. Prog Cardiovasc Dis. 2020;63(1):4–9. https://doi.org/10.1016/j.pcad.2019.11.012. Epub 2019 Nov 20. PMID: 31756356; PMCID: PMC7257910.
Dwinger S, Rezvani F, Kriston L, Herbarth L, Härter M, Dirmaier J. Effects of telephone-based health coaching on patient-reported outcomes and health behavior change: a randomized controlled trial. PLoS One. 2020;15(9):e0236861 https://doi.org/10.1371/journal.pone.0236861PMID: 32960886; PMCID: PMC7508388.
Joo JY. Nurse-led telehealth interventions during COVID-19: a scoping review. Comput Inform Nurs. 2022. https://doi.org/10.1097/CIN.0000000000000962. Epub ahead of print. PMID: 36067472.
Mann DM, Chen J, Chunara R, Testa PA, Nov O. COVID-19 transforms health care through telemedicine: evidence from the field. J Am Med Inform Assoc. 2020;27(7):1132–5. https://doi.org/10.1093/jamia/ocaa072.
Omboni S, Caserini M, Coronetti C, Telemedicine. Hypertension Management: Technologies, Applications and clinical evidence. High Blood Press Cardiovasc Prev. 2016;23(3):187–96. https://doi.org/10.1007/s40292-016-0143-6.
Perry AF, Federico F, Huebner J. Telemedicine. Ensuring safe, equitable, person-centered virtual care. IHI White Paper. Boston: Institute for Healthcare Improvement; 2021. www.ihi.org. Accessed 9 Nov 2021.
Itani R, Khojah HMJ, Jaffal F, et al. Provision of pharmaceutical care to suspected high-risk COVID-19 patients through telehealth: a nationwide simulated patient study. BMC Health Serv Res. 2021;21:997. https://doi.org/10.1186/s12913-021-07014-x.
Giorgino F, Bhana S, Czupryniak L, Dagdelen S, Galstyan GR, Janež A, Lalić N, Nouri N, Rahelić D, Stoian AP, Raz I. Management of patients with diabetes and obesity in the COVID-19 era: experiences and learnings from South and East Europe, the Middle East, and Africa. Diabetes Res Clin Pract. 2021;172:108617 Epub 2020 Dec 10. PMID: 33310175; PMCID: PMC7728417.
Caetano R, Silva AB, Guedes ACCM, Paiva CCN, Ribeiro GDR, Santos DL, Silva RMD. Challenges and opportunities for telehealth during the COVID-19 pandemic: ideas on spaces and initiatives in the brazilian context. Cad Saude Publica. 2020;36(5):e00088920. https://doi.org/10.1590/0102-311x00088920. Epub 2020 Jun 1. PMID: 32490913English, Portuguese.
Wang H, Yuan X, Wang J, Sun C, Wang G. Telemedicine maybe an effective solution for management of chronic disease during the COVID-19 epidemic. Prim Health Care Res Dev. 2021;22:e48. https://doi.org/10.1017/S1463423621000517.
Wong ST, Watson DE, Young E, Mooney D. Supply and distribution of primary healthcare registered nurses in British Columbia. Healthc Policy. 2009;5 Spec no(Spec No):91–104 PMID: 21037906; PMCID: PMC2906209.
Clark CE, Smith LF, Taylor RS, Campbell JL. Nurse led interventions to improve control of blood pressure in people with hypertension: systematic review and meta-analysis. BMJ. 2010;23:c3995. https://doi.org/10.1136/bmj.c3995. PMID: 20732968; PMCID: PMC2926309.
Al-Mallah MH, Farah I, Al-Madani W, Bdeir B, Al Habib S, Bigelow ML, Murad MH, Ferwana M. The impact of nurse-led clinics on the mortality and morbidity of patients with cardiovascular diseases: a systematic review and meta-analysis. J Cardiovasc Nurs. 2016;31(1):89–95. https://doi.org/10.1097/JCN.0000000000000224. PMID: 25658181.
Davis KM, Eckert MC, Hutchinson A, Harmon J, Sharplin G, Shakib S, Caughey GE. Effectiveness of nurse-led services for people with chronic disease in achieving an outcome of continuity of care at the primary-secondary healthcare interface: a quantitative systematic review. Int J Nurs Stud. 2021;121:103986. https://doi.org/10.1016/j.ijnurstu.2021.103986. Epub 2021 May 27. PMID: 34242979.
Martínez-González NA, Djalali S, Tandjung R, Huber-Geismann F, Markun S, Wensing M, Rosemann T. Substitution of physicians by nurses in primary care: a systematic review and meta-analysis. BMC Health Serv Res. 2014;14:214. https://doi.org/10.1186/1472-6963-14-214. PMID: 24884763; PMCID: PMC406538.
Forouzanfar MH, Liu P, Roth GA, Ng M, Biryukov S, Marczak L, et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990–2015. JAMA. 2017;317(2):165–82. https://doi.org/10.1001/jama.2016.19043. Erratum in: JAMA. 2017 Feb 14;317(6):648. PMID: 28097354.
Monahan M, Jowett S, Nickless A, Franssen M, Grant S, Greenfield S, Hobbs FDR, Hodgkinson J, Mant J, McManus RJ. Cost-effectiveness of telemonitoring and self-monitoring of blood pressure for Antihypertensive Titration in Primary Care (TASMINH4). Hypertension. 2019;73(6):1231–9. https://doi.org/10.1161/HYPERTENSIONAHA.118.12415. PMID: 31067190; PMCID: PMC6510405.
Higgins JPT, et al editors. Cochrane handbook for systematic reviews of interventions version 6.0 (updated in July 2019). London: Cochrane; 2019. Available at: www.training.cochrane.org/handbook. Accessed 30 Jul 2021.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Lockwood C, Porrit K, Munn Z, Rittenmeyer L, Salmond S, Bjerrum M, Loveday H, Carrier J, Stannard D. Chapter 2: Systematic reviews of qualitative evidence. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. JBI; 2020. Available from: https://doi.org/10.46658/JBIMES-20-03https://synthesismanual.jbi.global.
Munn Z, editor. JBI manual for evidence synthesis. JBI; 2020. https://doi.org/10.46658/JBIMES-20-03https://synthesismanual.jbi.global.
Chan ST, Khong PCB, Wang W. Psychological responses, coping and supporting needs of healthcare professionals as second victims. Int Nurs Rev. 2017;64(2):242–62. https://doi.org/10.1111/inr.12317. Epub 2016 Sep 28. PMID: 27679402.
Bosworth HB, Powers BJ, Olsen MK, McCant F, Grubber J, Smith V, Gentry PW, Rose C, Van Houtven C, Wang V, Goldstein MK, Oddone EZ. Home blood pressure management and improved blood pressure control: results from a randomized controlled trial. Arch Intern Med. 2011;171(13):1173–80. https://doi.org/10.1001/archinternmed.2011.276. PMID: 21747013.
Wakefield BJ, Holman JE, Ray A, Scherubel M, Adams MR, Hillis SL, Rosenthal GE. Effectiveness of home telehealth in comorbid diabetes and hypertension: a randomized, controlled trial. Telemed J E Health. 2011;17(4):254–61. https://doi.org/10.1089/tmj.2010.0176.
Brennan T, Spettell C, Villagra V, Ofili E, McMahill-Walraven C, Lowy EJ, et al. Disease management to promote blood pressure control among African Americans. Popul Health Manag. 2010;13(2):65–72. https://doi.org/10.1089/pop.2009.0019.
Cicolini G, Simonetti V, Comparcini D, Celiberti I, Di Nicola M, Capasso LM, Flacco ME, Bucci M, Mezzetti A, Manzoli L. Efficacy of a nurse-led email reminder program for cardiovascular prevention risk reduction in hypertensive patients: a randomized controlled trial. Int J Nurs Stud. 2014;51(6):833–43. https://doi.org/10.1016/j.ijnurstu.2013.10.010.
Hebert PL, Sisk JE, Tuzzio L, Casabianca JM, Pogue VA, Wang JJ, Chen Y, Cowles C, McLaughlin MA. Nurse-led disease management for hypertension control in a diverse urban community: a randomized trial. J Gen Intern Med. 2012;27(6):630–9. https://doi.org/10.1007/s11606-011-1924-1. Epub 2011 Dec 6. PMID: 22143452; PMCID: PMC3358388.
Kim M. Effects of customized long-message service and phone-based Health-Coaching on Elderly People with Hypertension. Iran J Public Health. 2019;48(4):655–63 PMID: 31110975; PMCID: PMC6500537.
Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. https://doi.org/10.1097/00005650-198601000-00007. PMID: 3945130.
Zabler B, Tsai PY, Fendrich M, Cho Y, Taani MH, Schiffman R. Effect of a nurse case management intervention for hypertension self-management in low-income African Americans. Contemp Clin Trials. 2018;71:199–204. https://doi.org/10.1016/j.cct.2018.06.011.
Cui X, Zhou X, Ma LL, Sun TW, Bishop L, Gardiner FW, Wang L. A nurse-led structured education program improves self-management skills and reduces hospital readmissions in patients with chronic heart failure: a randomized and controlled trial in China. Rural Remote Health. 2019;19(2):5270. https://doi.org/10.22605/RRH5270.
Alessa T, Abdi S, Hawley MS, de Witte L. Mobile apps to support the self-management of hypertension: systematic review of effectiveness, usability, and user satisfaction. JMIR Mhealth Uhealth. 2018;6(7). https://doi.org/10.2196/10723.
Ma Y, Cheng HY, Cheng L, Sit JWH. The effectiveness of electronic health interventions on blood pressure control, self-care behavioral outcomes and psychosocial well-being in patients with hypertension: a systematic review and meta-analysis. Int J Nurs Stud. 2019;92:27–46. https://doi.org/10.1016/j.ijnurstu.2018.11.007.
Li R, Liang N, Bu F, Hesketh T. The effectiveness of self-management of hypertension in adults using Mobile Health: systematic review and Meta-analysis. JMIR Mhealth Uhealth. 2020;8(3):e17776. https://doi.org/10.2196/17776.
Garner SL, George CE, Young P, Hitchcock J, Koch H, Green G, Mahid Z, Norman G. Effectiveness of an mHealth application to improve hypertension health literacy in India. Int Nurs Rev. 2020;67(4):476–83. https://doi.org/10.1111/inr.12616.
Choi W-S, Kim N-S, Kim A-Y, Woo H-S. Nurse-coordinated blood pressure telemonitoring for urban hypertensive patients: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18:6892. https://doi.org/10.3390/ijerph18136892.
Eickhoff DO, Guido-Sanz F, Anderson M. Telehealth across nursing education: findings from a national study. J Prof Nurs. 2022;42:308–14. https://doi.org/10.1016/j.profnurs.2022.07.013.
Acknowledgements
Not applicable.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Study design: PE, MK, VJ, AH. Literature search: PE, MK, VJ. Quality assessment: PE, MK, VJ. Analysis and interpretation: PE, MK. Manuscript writing: PE, MK, VJ, AH. Critical revisions for important intellectual content: PE, MK, VJ. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
no ethical approval was required for this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix 1.
Search strategy.
Additional file 2: Appendix 2.
Critical appraisal tools.
Additional file 3: Appendix 3:
Critical appraisal results for included studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kappes, M., Espinoza, P., Jara, V. et al. Nurse-led telehealth intervention effectiveness on reducing hypertension: a systematic review. BMC Nurs 22, 19 (2023). https://doi.org/10.1186/s12912-022-01170-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-022-01170-z