
Abstract
Background
China faces a serious shortage of competent nurses who can address the healthcare needs of older people in an ageing society. Chinese higher education institutes face serious challenges when it comes to developing new curricula that are capable of educating sufficient numbers of competent gerontological nurses. Therefore, the aim of this research study was to identify and verify competencies for gerontological nurses in China that are needed to provide nursing care for the growing number of older people in all care settings. This study takes into account the possible opportunities that trends and developments may offer in the near future.
Methods
In this study, a two-phase research design was used. The first phase concerned needs analysis, including a situational analysis, a trend analysis and a competence analysis. This process resulted in a draft competence framework. The second phase addressed the verification of the competence framework through a two-round Delphi study with a panel of Chinese and European experts. This process led to the final competence framework.
Results
The final competence framework for gerontological nursing in China included six competencies divided into 13 essential and five relevant learning outcomes. The competencies are: ‘providing gerontological care’, ‘communication and collaboration’, ‘organization of gerontological nursing care’, ‘health promotion’, ‘evidence-based nursing and lifelong learning’ and ‘professional behaviour’.
Conclusion
The framework comprehensively covers the six core competencies that nurses who care for older people should possess. These competencies are well-embedded in a Chinese context. The framework therefore offers concrete, practical suggestions for the competencies and skills that nursing graduates will need to work in current and future professions related to gerontological nursing education and practice.
Similar content being viewed by others

Background
China faces a serious shortage of competent nurses who can address the healthcare needs of older people in an ageing society. According to the seventh population census of China’s National Bureau of Statistics, 264.02 million people in China are aged 60 or older, accounting for 18.70% of the country’s total population [1]. In contrast, there were 4.7 million registered nurses in China at the end of 2020, and the ratio of registered nurses per 1,000 people was 3.35 [2]. This is far below average international ratio, which is 8.8:1000 [3]. The Chinese government has offered various methods to increase the number of registered nurses and to meet the growing needs of older people. According to the National Health Commission of the People's Republic of China, increasing the number of registered nurses will require further efforts in healthcare education, healthcare organisations and healthcare infrastructure [4]. These changes are visible in the Healthy China 2030 Plan for the WHO [5] and in the country’s ongoing healthcare reform, which aims to increase training for medical professionals and to enhance investments in healthcare and care facilities for older people, especially in rural area [4]. Additionally, global cooperation and investments in new technologies are promoted to improve healthcare [4].
Gerontological care providers and educational institutes need to consider how to cope with the existing problems in the field of care for older people and how to address the development of gerontological nursing in China [6]. The Chinese nursing curriculum concerning gerontological nursing is quite traditional. From its inception, nursing education in China adopted the bio-medical model [7]. It focuses strongly on disease and theory, but it neglects prevention, health rehabilitation and practical skills [7, 8]. In general, graduates are neither motivated nor equipped with sufficient skills to work in the various healthcare environments that currently exist for older people [7]. Chinese higher education institutes (HEIs) face serious challenges when it comes to developing new curricula capable of educating sufficient numbers of competent gerontological nurses. Chinese nursing graduates need to acquire competencies to support healthy ageing today while also learning to understand the field’s future needs [7].
The GeNEdu project, which seeks to develop gerontological nursing education in China through multidisciplinary innovations, seeks to navigate the challenges in this field. In this Erasmus Capacity Building project, three Chinese HEIs work closely with three European HEIs. The main objective of the GeNEdu project is to renew nursing curricula by building the capacities of Chinese HEIs and by developing gerontological nursing education for future healthcare professionals to ensure that they can meet the needs of China’s ageing society [8]. Part of the project is the development of a competence framework for gerontological nurses in China. This framework is designed to guide the development of new educational programmes.
Competence frameworks typically are used to outline the characteristics of a competent workforce [9] and to serve as input for curriculum development [10]. In the field of healthcare, many competence frameworks exist, including several competence frameworks for gerontological nurses [11,12,13]. Most literature about gerontological nursing competences is based on research in western societies. China, in comparison to many other ageing societies, has distinctive national and cultural characteristics influencing gerontological nursing [8, 14]. Due to the cultural differences between China and Western countries that influence the perception of what gerontological care delivery entails, the need arose to develop a new competence framework as part of the GeNEdu-Erasmus project. Erasmus projects aim to bring expertise from European universities together with universities outside Europe, in order to learn from each other, conduct research together, and improve curricula [8]. GeNEdu’s competence framework for gerontological nursing will support the development of new curricula to meet the rising care needs of older people in China. Therefore, the aim of this research study was to identify and verify competencies for gerontological nurses in China.
Methods
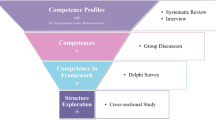
In this study, a two-phase research design was used. The first phase concerned the needs analysis, including a situational analysis, a trend analysis and a competence analysis. It resulted in a draft competence framework. The second phase concerned the verification of the competence framework through a two-round Delphi study with a panel of Chinese and European experts. It led to the final competence framework (Fig. 1).

Two-phase research design, including needs analysis and verification study
Needs analysis
The design of the needs analysis included three steps. Its goal was to identify the competencies that gerontological nurses in China need. The first step of the needs analysis was a situational analysis, which identified the needs in gerontological nursing practice and education in China on both a national and regional level. The second step was a trends analysis, which identified the international trends and developments in gerontological nursing. The third step was a competence analysis, which provided insight into existing competence descriptions for gerontological nurses.
Situational analysis
Performing a situational analysis identified the primary challenges, trends and developments in gerontological care and gerontological nursing in China. A DESTEP analysis approach was used to identify the demographic, economic, social, technological, ecological and political factors that are important to the future of gerontological care and gerontological nursing education [15, 16]. During a one-day workshop, participants from three Chinese partner universities systematically mapped their findings onto national and regional levels. After the workshop, the Chinese partner universities performed desk research to deepen the DESTEP analysis. They used scientific articles, online information, policy documents and other relevant material written in Chinese. An additional six Chinese experts in the field of gerontological nursing practice were also interviewed. The outcomes of these interviews were shared and discussed during online meetings. This created mutual understanding about the current status and future needs of gerontological nursing in China.
Trends analysis
A comprehensive review of scientific and grey literature was performed to identify the main international trends in gerontological nursing and gerontological nursing education.
A scientific literature search was performed simultaneously in two databases: CINAHL and MEDLINE. The keywords used were ‘gerontology or elderly or aging or geriatric’ and ‘nursing or nursing care or nursing education or nursing competence’. The search was limited to peer-reviewed, full-text articles published from 2016–2020. They all addressed gerontological education and the care of older people in various settings. Additionally, a grey literature search was performed to discover handbooks, policy documents, educational material and other relevant material in the English or Finnish languages. Two researchers analysed the literature and independently listed the main trends (MH, MV). Rigour was addressed by discussing the findings with project team until a consensus was reached about the main trends present in gerontological nursing.
Competence analysis
The competence analysis was conducted to provide an overview of the existing core areas and competencies for gerontological nursing. A search was performed for documents that included competence descriptions relevant to gerontological nurses. The eligible documents included policy documents, professional reports, scientific articles and educational materials published after 2010 in Chinese, English, Finnish and Dutch. Materials were included until saturation was reached and no new competencies appeared.
The project members used a structured checklist to extract the relevant data, including competence descriptions, from the documents. BD performed a mapping exercise using an Excel spreadsheet to organise the competencies according to the seven CanMEDS roles [17]. The choice for CanMEDS roles was made on the basis of a consensus decision, which showed that the CanMEDS role model was widely known and recognized in nursing education. It also shows significant similarities with the competence framework of the European Federation of Nurses (EFN) [18]. This framework also has a good degree of implementation in various European countries.
After several face-to-face and online meetings among project members, consensus was reached about which competencies and learning outcomes to include in the draft competence framework. The results of the situational analysis and trend analysis were used as references to reduce the likelihood that important information would be missing from the draft competence framework.
Verification
A Delphi panel with experts was consulted to verify the set of competencies for gerontological nurses in China. A Delphi study was chosen because this consensus-building tool has been applied in a variety of fields, including the development of competence frameworks [9, 19]. It is an appropriate method to use when experts are located at considerable geographic distances from each other, as was the case in this study. A Delphi study is predominantly qualitative in nature, but it also has a quantitative component whenever consensus is calculated [20].
The Delphi panel and procedure
A panel of experts was established by inviting 31 participants from China, Finland, Estonia and the Netherlands. Because the competencies should match the Chinese context, 75% of experts were selected from China. All experts were selected based on their authority and their high level of theoretical expertise in the field of gerontological nursing. Their professional backgrounds and settings included governmental organisations, long-term care facilities, community care providers and hospitals.
The Delphi study included two rounds of questionnaires concerning competencies and learning outcomes for gerontological nurses. The questionnaire for the first round was developed based on the results of the needs analysis. It included six competencies with a total of 21 learning outcomes. The questionnaire for the second round was composed based on the first round’s results. It included the competencies and learning outcomes that did not meet the consensus thresholds in the first round. Both questionnaires were translated from English to Chinese using the back-translation method [21]. The Chinese and English versions were distributed through Webropol.
Each participant received an individual link to the questionnaire via e-mail. They were all invited to rate the competencies and learning outcomes on a 3-point scale. For the first round, this scale included the following options: 1 (essential), 2 (useful but not essential) and 3 (not necessary) [22]. In addition, the questionnaire included open-ended questions to allow participants to provide additional comments. The 3-point scale in the second round included the following options: 1 (essential), 2 (very relevant) and 3 (relevant but not most important). No open-ended questions were included in the second round. Ratings were based on each participant’s personal opinions, and anonymity was guaranteed [23]. A reminder was sent after two weeks, and a second reminder was sent after four weeks.
Data analysis of the Delphi study
To analyse the first round’s ratings, content validity ratios (CVRs) were calculated. This is the appropriate technique to determine consensus among a panel of experts [22]. The CVR was determined as (ne—N/2)/(N/2), in which ne is the number of panellists who indicated ‘essential’ and N is the total number of panellists. In a panel consisting of 25–30 people, a content validity ratio of 0.37 is regarded as the minimum value to define consensus [22].
In the second round of the questionnaire, competencies and learning outcomes with a CVR lower than 0.37 and a percentage higher than 50% were presented for validation again. If the percentage was lower than 50%, it was considered to be nonessential, and it was removed from the competence framework after discussing the interpretation of the data with the project team. Open answers provided evidence for changes in the formulation of the competencies and learning outcomes.
Results
Needs analysis
Situational analysis
The situational analysis resulted in a summary of the specific characteristics that define the care of older people and the practice of gerontological nursing in China. Many older people live alone; these so-called "empty nesters" account for more than 54% of the country’s older population [24]. This group of people receives limited care and support – or none at all – from their family members. A large gap exists in the quality of life and poverty levels between the urban and rural populations. There are more women than men, and, especially in rural China, older women face great disadvantages in every aspect of life.
At present, gerontological nursing in China faces certain problems. These include a serious workforce shortage, the low payment of professional nurses in gerontological nursing and a lack of care institutions for older people. In addition, many nurses working in the gerontological care have lower education levels, and they may lack skills in technology or in other areas of contemporary nursing.
An important aspect of nursing practice is reflected in the Chinese cultural understanding of health and the use of traditional Chinese medicine (TCM) interventions to restore the overall balance, rather than simply treating the symptoms [25]. Experts agree that TCM should be integrated in future care as well because older people in China benefit from it. To obtain all-round development, nursing students should acquire basic theory, knowledge and skills of TCM [26].
Innovative models for gerontological care and the use of technology are needed to improve the quality of services for elderly people. China promotes new modes of nursing services, such as "smart elderly care" which is based on a sensor network system and information platform for elderly at home, communities and care organizations [27].
Trends analysis
The scientific database search located 117 scientific articles. After screening by title, abstract and full text, 14 scientific articles were included for analysis. In addition, 22 documents were selected from the grey literature search.
Content analysis revealed five trends in gerontological nursing. The first is an emphasis on person-centred care, which relates to the needs of older people and their families [28, 29]. Nurses should recognize individual and cultural factors and provide person-centred care in innovative ways. The second trend is a willingness to collaborate with and to account for the needs of family members and informal caregivers. Because family members often become part of the healthcare team, nurses require skills and knowledge to involve family caregivers accordingly [30,31,32]. The third trend in gerontological nursing is a focus on health promotion and healthy ageing via disease prevention and a healthy lifestyle [28, 33]. The fourth trend is support for independent living at home; many older people remain at home and use technological solutions in gerontology [34,35,36]. The fifth trend is multidisciplinary collaboration, which is important when a patient has multiple health or social issues. Complex, multifactorial interventions can significantly improve older adults’ ability to remain living at home and avoid residential care admission [37, 38].
It is possible to identify trends towards improved education programmes and the use thereof, particularly in settings such as home care, community care, long-term care and end-of-life care. Home care includes health maintenance, counselling and education to prevent illness; it also includes disease treatment, rehabilitation and palliative care [31]. Community nursing might be a cost-efficient way to decrease the burden of informal caregivers and primary care providers [39]. In long-term care settings, gerontological nurses ought to have the competence to recognize factors that contribute to a better quality of life for residents [31, 40, 41]. Additionally, nurses in these settings should emphasize their competence in pharmacotherapy [42]. For quality end-of-life care, a structured and evidence-based educational programme is recommended to nursing staff [30, 43]. End-of-life care provision must be possible in settings such as hospitals, homes or community and rehabilitation placements [44]. Nurses and health team members provide the medical, emotional and spiritual support needed in end-of-life care [34, 44]. Because HEIs educate the future workforce, it is important to incorporate these trends into nursing curricula.
Competence analysis and the draft competence framework
In total, 14 Chinese policy documents, 17 competence frameworks, 32 scientific articles and four educational materials were included in the competence analysis (see Table 1 an Appendix 1). The policy documents covered different fields of work for gerontological nurses in China. Competence descriptions in these policy documents focused primarily on competencies that belong to the expert or manager roles. The 17 competence frameworks included competencies covering all seven CanMEDS roles. Eight of the frameworks explicitly mentioned technology as part of the competencies. Additional competencies were retrieved from the scientific articles and the educational materials, which covered all seven CanMEDS roles.
Synthesis of the competence descriptions resulted in a draft competence framework of gerontological nursing. Its six competencies were: ‘providing gerontological care’, ‘communication and collaboration’, ‘nursing leadership and innovation’, ‘health promotion’, ‘evidence-based nursing and lifelong learning’ and ‘professional behaviour’. The six competencies were elaborated via 21 learning outcomes. For the purpose of the GeNeDU competence framework, competencies were defined as a dynamic combination of knowledge, skills, attitudes and values capable of being transferred to a certain context or real situation. Learning outcomes were defined as statements about what a learner is expected to know, understand and be able to demonstrate after the completion of learning [45].
Results verification phase
Participants’ characteristics
The first round included 29 participants, and the second round involved 26. The majority of them had more than 10 years of work experience and a nursing background. The majority were working at healthcare organizations when they answered the questionnaires (see Table 2). Both Delphi rounds identified the same background characteristics among participants.
Delphi study
After the first round of the Delphi study, a high level of consensus was found for the competencies ‘providing gerontological care’, ‘communication and collaboration’ and ‘professional behaviour’ (see Table 3). The experts agreed that these three competencies and the learning outcomes associated with them are essential for gerontological nurses in China. The CVR score for these three competencies was 0.93. The CVR scores for the corresponding learning outcomes varied from 0.45–0.86.
The competence ‘nursing leadership and innovation’ showed a CVR of 0.31. Analysing the ratings according to the level of the learning outcomes associated with this competence showed that the learning outcome ‘quality management’ was the only one that experts agreed to be essential. With a CVR of 0.31, the learning outcome ‘planning and organisation’ was close to the threshold value. The other learning outcomes – ‘leadership’, ‘policy development’ and ‘innovation and technology’ – showed CVR scores between -0.24 and 0.17. Although the competence ‘health promotion’ was rated as essential, there was no consensus about the three learning outcomes associated with this competence; they had CVR scores between -0.10 and 0.24. For the competence ‘evidence-based nursing’, only the learning outcome ‘evidence-based nursing and critical thinking’ was below the threshold for determining consensus; it had a CVR of 0.31. Because the CVR could not determine a consensus regarding the essentiality of the three competencies ‘nursing leadership and innovation’, ‘health promotion’ and ‘evidence-based nursing and lifelong learning’, these competences were reformulated and presented to the panel of experts in the second round of the Delphi study. The reformulation of these competencies and learning outcomes was based on the CVR scores and remarks that participants made.
Table 4 presents the second round’s scores. The competence ‘nursing leadership and innovation’ was reformulated towards ‘organisation of gerontological nursing care’, which resulted in higher ratings for its essentiality. The reformulated learning outcome ‘innovation and technology’ was still not considered to be essential, but it was rated very relevant. For the competence ‘health promotion’, the learning outcome ‘plan person-centred health promotion’ was rated essential. ‘Perform health promotion’ was rated below the CVR threshold for essentiality. Therefore, it was considered very relevant.
The competence ‘evidence-based nursing and lifelong learning’ shows a diffuse pattern. In the first round, this competence and two of the three associated learning outcomes were considered to be essential. Only the learning outcome ‘evidence-based nursing and critical thinking’ was below the consensus threshold. In the second round, there only seemed to be consensus that the learning outcome ‘lifelong learning and professional development’ was essential. The other learning outcomes were considered very relevant.
The Delphi study resulted in a verified final competence framework that showed the essential and relevant competencies and learning outcomes (see Table 5). The competence "providing gerontological care" and the corresponding learning outcomes describe care and planning of care on the level on one individual patient. The competence "organisation of gerontological care" and the corresponding learning outcomes concern the organisational level.
Discussion
The gerontological nursing competence framework for China includes six competencies and 18 learning outcomes. This framework comprehensively covers the core competencies that nurses who care for older people should possess. One strength of this comprehensive competence framework is its applicability to different care settings. The competence descriptions focus on the current and future needs of gerontological nursing.
We distinguished 13 essential and five relevant learning outcomes. The essential learning outcomes are all closely related to providing nursing care for patients and their family members. The learning outcomes that were rated as relevant are more supportive and more closely related to the organisation of care, innovation, personal development and professional development. Huizinga et al. (2016) explained that the more distant from patient activities a role is, the less frequently competencies are considered to be essential [46]. This includes competencies about social networks; research and innovation of care; legal, financial and organizational issues; professional ethics; and professional innovation [46]. Experts rated the learning outcome "Advocate for older people" as irrelevant for gerontological nurses in China, due to cultural and social values [14]. The competence framework targets vocational and bachelor levels. It includes the competencies related to organisation, leadership, research and innovation that are of foremost importance for bachelor-level students [18]. Although experts did not rate these competencies as essential, they should be part of gerontological education at a bachelor level.
The method used, in which Chinese gerontological nursing experts were involved in the needs analysis and the verification process, resulted in a competence framework that is well embedded in a Chinese context [14]. Although the competencies are specifically designed for gerontological nursing in China, the wording of the competencies and their associated learning outcomes is quite general. The GeNedu project used the results of the needs analysis to develop a handbook with more detailed descriptions of the required knowledge and assessment criteria for the learning outcomes that include specific cultural elements [8]. For example, the GeNEdu competence framework’s competencies and learning outcomes do not mention TCM, which is considered to be important for nursing practice in China. In the handbook TCM knowledge and skills are integrated in the competence "providing gerontological care" as part of holistic care. We recommend to take this into account during the curriculum development process, while specifying learning outcomes and developing educational content for the competencies associated with gerontological care.
The use of technology is becoming increasingly important for gerontological nurses. The competence framework’s learning outcome ‘innovation and technology’ shows this importance, but it is also embedded in all of the competencies. Further elaboration for educational purposes should include the key areas where digital technology is needed to provide high-quality, ethical patient care; social and communication skills; diagnoses and treatment; motivation and willingness to integrate digitalisation in a professional context; and collegial and organisational support for building positive experiences via digitalisation [47].
As most of the literature about gerontological nursing competences is based on research in western societies, our study focused on the transfer and application in Chinese culture. This is as far as we know the first study that compared and integrated information from different cultures in this way. In addition, the method we used may also be of interest to project leaders of similar curriculum development projects in other countries.
The Delphi method was suitable to reach consensus among the experts. Because of the extensive needs analysis, two rounds were sufficient [48]. One strong point of our approach is the feedback it provided to experts during the second round. It could be considered a limitation that we used a different scale during the second round of the Delphi study. On the other hand, this method provided deeper nuance in the competence set by distinguishing essential competencies from competencies that were relevant, but not essential.
Implications for practice
In China, this competence framework, which was developed through a process of international cooperation, will challenge Chinese institutions to meet international standards regarding the quality of nursing in higher education. The competence framework is available in Chinese and English. It will be a useful instrument for developing future gerontological nursing curricula in China. It offers concrete, practical suggestions about the competencies and skills that nursing graduates need for current and future gerontological nursing practice.
In general, the use of the competence framework will require a shift from theory-based to competence-based education. Training is recommended to help teachers develop competence-based education and to make learning outcomes specific, operable and comparative. Within the GeNEdu project, Chinese teachers who participated in such a training, developed successfully six modules for a gerontological nursing curriculum.
Since teaching and assessing learning outcomes is new to Chinese teachers, sustainable implementation of these modules will require training of all teachers. Additionally, the core competences for educators in gerontological nursing can help the Chinese institutes to develop these teacher trainings [49].
Conclusion
The gerontological nursing framework for China includes six competencies with 13 essential and five relevant learning outcomes. The competences are ‘providing gerontological care’, ‘communication and collaboration’, ‘organization of gerontological nursing care’, ‘health promotion’, ‘evidence-based nursing and lifelong learning’, and ‘professional behaviour’. The framework comprehensively covers the core competencies that nurses who care for older people should possess. These competencies are well embedded in a Chinese context.
Availability of data and materials
The datasets used and analysed during the present study are available from the corresponding authors upon reasonable request.
Abbreviations
- CVR:
-
Content validity ratio
- HEI:
-
Higher educational institute
- ICT:
-
Information and communication technology
- WHO:
-
World Health Organization
References
National Bureau of Statistics of China. Statistical data. Available at: http://www.stats.gov.cn/tjsj/sjjd/202105/t20210512_1817336.html. Accessed 5/12, 2021.
National Health Commission. Statistical Bulletin on health development in China 2020. Available at: https://www.med66.com/hushi/qita/lu2107159389.shtml[. Accessed 7/13, 2021.
OECD. Health at glance 2019: OECD indicators. Available at: https://www.oecd-ilibrary.org/sites/98e2d5de-en/index.html?itemId=/content/component/98e2d5de-en. Accessed 7/12, 2021.
National Health Commission of the People's Republic of China. The Twelfth Five-year plan for the development of China's ageing Career. Available at: http://www.nhc.gov.cn/lljks/zcwj2/201307/865bea09e8c2443390946eb8498e3635.shtml. Accessed 2/12, 2021.
WHO. Healthy China 2030 (from vision to action). Available at: https://www.who.int/teams/health-promotion/enhanced-wellbeing/ninth-global-conference/healthy-china. Accessed 7/13, 2021.
The State Council: Several Opinions on Accelerating the Development of the Elderly Service Industry (Document of State Council [2013] No. 35) [EB/OL]. 2013; Available at: http://www.moe.gov.cn/jyb_xxgk/moe_1777/moe_1778/201703/t20170308_298669.html.2017-2-28. Accessed May, 2021.
Wang CC, Whitehead L, Bayes S. Nursing education in China: Meeting the global demand for quality healthcare. International journal of nursing sciences. 2016;3(1):131–6.
JAMK. Developing Gerontological Nursing Education in China through Multidisciplinary Innovations / GeNEdu. 2019.
Batt AM, Tavares W, Williams B. The development of competency frameworks in healthcare professions: a scoping review. Adv Health Sci Educ. 2019;25(4):1–75.
Mulder M. Competence and the Alignment of Education and Work. Competence-Based Vocational and Professional Education: Springer; 2017. p. 229–51.
Traynor V, Inoue K, Crookes P. Literature review: understanding nursing competence in dementia care. J Clin Nurs. 2011;20(13–14):1948–60.
Mauk KL. Gerontological nursing: competencies for care. : Jones & Bartlett Publishers; 2010.
Britten N, Traynor V, Osmond T, Chenoweth L. Developing gerontological nursing competencies: An e-Delphi study. Australian Nursing and Midwifery Journal. 2018;25(7):42.
Chen Y. Chinese values, health and nursing. J Adv Nurs. 2001;36(2):270–3.
Leis M. Challenges for the Future of Learning Until 2030. 2010.
R De Vlieger. DESTEP analysis. 2012; Available at: https://www.calltheone.com/en/consultants/destep-analysis. Accessed 3/20, 2020.
Royal college of physicians and surgeons of Canada. CanMEDS, better physicians, better standards, better care. Available at: https://www.royalcollege.ca/rcsite/canmeds/canmeds-framework-e. Accessed 12/06, 2020.
European Union. The European Qualifications Framework. Available at: https://europa.eu/europass/en/european-qualifications-framework-eqf. Accessed 2/16, 2021.
Humphrey-Murto S, Varpio L, Wood TJ, Gonsalves C, Ufholz L, Mascioli K, et al. The use of the Delphi and other consensus group methods in medical education research: a review. Acad Med. 2017;92(10):1491–8.
Avella JR. Delphi panels: Research design, procedures, advantages, and challenges. Int J Dr Stud. 2016;11(1):305–21.
Brislin RW, Freimanis C. Back-translation. An Encyclopaedia of Translation: Chinese-English, English-Chinese 2001;22.
Lawshe CH. A quantitative approach to content validity. Person Psychol. 1975;28(4):563–75.
Linstone HA, Turoff M. The delphi method. : Addison-Wesley Reading, MA; 1975.
Liu LY, Zheng ZW, Rao KQ. Blue Book of Elderly Health-Annual Report on Elderly Health in China. : Social Sciences Academic Press; 2019.
Smith DR, Tang S. Nursing in China: Historical development, current issues and future challenges. Journal of Oita Nursing and Health Sciences. 2004;5(2):16–20.
Hao Y, Jiang J, Gu X. Traditional Chinese medicine and nursing care. Int J Nurs Sci. 2017;4(3):328–9.
Rural smart elderly care model: China’s development and challenges. 2020 5th International Conference on Universal Village (UV): IEEE; 2020.
Harris J. Geriatric Trends Facing Nursing with the Growing Aging. Critical Care Nursing Clinics. 2019;31(2):211–24.
Andrew N, Meeks S. Fulfilled preferences, perceived control, life satisfaction, and loneliness in elderly long-term care residents. Aging Ment Health. 2018;22(2):183–9.
Okumura-Hiroshige A, Fukahori H, Yoshioka S, Nishiyama M, Takamichi K, Kuwata M. Effect of an end-of-life gerontological nursing education programme on the attitudes and knowledge of clinical nurses: A non-randomised controlled trial. Int J Older People Nurs. 2020;15(3): e12309.
Rinnan E, André B, Drageset J, Garåsen H, Espnes GA, Haugan G. Joy of life in nursing homes: A qualitative study of what constitutes the essence of Joy of life in elderly individuals living in Norwegian nursing homes. Scand J Caring Sci. 2018;32(4):1468–76.
Ris I, Schnepp W, Mahrer IR. An integrative review on family caregivers’ involvement in care of home-dwelling elderly. Health Soc Care Community. 2019;27(3):e95–111.
Phurailatpam J, Clement I, Clement N. Trends, Issues and Practice in Geriatric Nursing Care. Research & Review. Journal of Geriatric Nursing and Health Sciences. 2019;1(2):1–9.
Mikkonen I, Sourtzi P, Turjamaa R, Äijö M, Ylinen E, Finnema EJ, et al. Trends and Developments in Health-Care and Social Services. Older People: Improving Health and Social Care: Springer; 2019. p. 103–138.
Technology to support aging in place. older adults’ perspectives. Healthcare: Multidisciplinary Digital Publishing Institute; 2019.
Panetta KG. 5 Trends Appear on the Gartner Hype Cycle for Emerging Technologies. Available at: https://www.gartner.com/smarterwithgartner/5-trends-appear-on-the-gartner-hype-cycle-for-emerging-technologies-2019/. Accessed 06/19, 2020.
Luker JA, Worley A, Stanley M, Uy J, Watt AM, Hillier SL. The evidence for services to avoid or delay residential aged care admission: a systematic review. BMC Geriatr. 2019;19(1):1–20.
Santini S, Tombolesi V, Baschiera B, Lamura G. Intergenerational programs involving adolescents, institutionalized elderly, and older volunteers: Results from a pilot research-action in Italy. BioMed research international 2018;2018.
Ljungbeck B, Forss KS. Advanced nurse practitioners in municipal healthcare as a way to meet the growing healthcare needs of the frail elderly: a qualitative interview study with managers, doctors and specialist nurses. BMC Nurs. 2017;16(1):1–9.
James I, Blomberg K, Kihlgren A. A meaningful daily life in nursing homes-a place of shelter and a space of freedom: a participatory appreciative action reflection study. BMC Nurs. 2014;13(1):1–13.
Haugan G. The relationship between nurse–patient interaction and meaning-in-life in cognitively intact nursing home patients. J Adv Nurs. 2014;70(1):107–20.
Johansson-Pajala R, Jorsäter Blomgren K, Bastholm-Rahmner P, Fastbom J, Martin L. Nurses in municipal care of the elderly act as pharmacovigilant intermediaries: a qualitative study of medication management. Scand J Prim Health Care. 2016;34(1):37–45.
Hum AY, Wu HY, Ali NB, Leong IY, Chin JJ, Lee AO, et al. The dignity in advanced dementia (diadem) study: developing an integrated geriatric palliative homecare program. Progress in Palliative Care. 2018;26(2):65–72.
Evans CJ, Ison L, ELLIS‐SMITH C, Nicholson C, Costa A, Oluyase AO, et al. Service delivery models to maximize quality of life for older people at the end of life: a rapid review. Milbank Q. 2019;97(1):113–75.
Wagenaar R. Competences and learning outcomes: a panacea for understanding the (new) role of Higher Education? Tuning Journal for Higher Education. 2014;1(2):279–302.
Huizenga P, Finnema E, Roodbol P. Learnt and perceived professional roles of a new type of nurse specialized in Gerontology and Geriatrics, a qualitative study. J Adv Nurs. 2016;72(7):1552–66.
Konttila J, Siira H, Kyngäs H, Lahtinen M, Elo S, Kääriäinen M, et al. Healthcare professionals’ competence in digitalisation: A systematic review. J Clin Nurs. 2019;28(5–6):745–61.
Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014;67(4):401–9.
Wyman JF, Abdallah L, Baker N, Bell C, Cartwright J, Greenberg SA, et al. Development of core competencies and a recognition program for gerontological nursing educators. J Prof Nurs. 2019;35(6):452–60.
Acknowledgements
Our thanks for their contribution go to all GeNEdu project members and the experts participating in the Delphi study, which was one part of the whole GeNEdu project.
Funding
GeNEdu project, abbreviated from “Developing Multidisciplinary Innovations in Gerontological Nursing Education in China”, is co-funded by the Erasmus + Programme of the European Union, specifically a project of Capacity Building in the field of Higher Education started from 15 November 2019. The project reference is 610060-EPP-1–2019-1-FI-EPPKA2-CBHE-JP.
The European Commission's support for the production of this publication does not constitute an endorsement of the contents, which reflect the views only of the authors, and the Commission cannot be held responsible for any use which may be made of the information contained therein.
Author information
Authors and Affiliations
Contributions
BLD, MP, MA and WP: initiation and design of the research. WW, YCu, YCh, JI, WJ, CF and YL: situational analysis. MH and MV: trend analysis. BD, MH, MV, WW, YCu, YCh JI, WJ, CF and CS: competence analysis. BD, MA, MH, YCu, YCh, WW, JI, CF and YL: development of the Delphi questionnaires and collection of data. BD, MH, MA, YCu, WW, JI, CF and YL: analysis of the Delphi study’s results. All authors: development and writing of the final competence framework. BD, MH, WW, MP and MA: writing the paper. WP: editorial revision of the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was given by the International GeNEdu Academic Advisory Board, chaired by Hanze University of Applied Sciences Groningen. Approval aimed to ensure safety, efficiency and all ethical considerations needed before the start of the research activities. Approval for the situational analysis was granted on 10-01-2020 under number GeNEdu-2.1.1a. Approval for the Delphi review was given on 11-12-2020 granted on under number GeNEdu-2.1.2a. Participants were invited and informed about the study purpose and methods by e-mail or personal contact. Informed consent was obtained from all participants. Participant anonymity was maintained throughout the study. All methods were carried out in accordance with relevant guidelines and regulations, as mentioned in Dutch Code of Conduct for Research Integrity 2018 (43) and World Medical Association Declaration of Helsinki (44).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Dijkman, B.L., Hirjaba, M., Wang, W. et al. Developing a competence framework for gerontological nursing in China: a two-phase research design including a needs analysis and verification study. BMC Nurs 21, 285 (2022). https://doi.org/10.1186/s12912-022-01074-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-022-01074-y