
Abstract
Background
The aging population and its associated health needs require specific nursing care. The aim of this study was to draw an epidemiological profile of Portuguese elderly adults attending in residential homes and day centers and to evaluate the association between the functioning and cognition of these older adults and their sociodemographic characteristics and presence of multimorbidity.
Methods
This was a cross-sectional study of 613 older adults. Functioning was assessed using the Elderly Nursing Core Set, and cognition was assessed using the Mini Mental State Examination. Descriptive and inferential analyses were performed.
Results
The mean age was 85.73 years; the majority of the participants were female (69.3 %), widowed (67.0 %) and over 85 years old (60.4 %). A total of 68.2 % of the sample presented multimorbidity. A total of 54.5 % had cognitive impairment, and the average functional profile was classified as “moderate difficulty”. Institutionalized older adults had more diseases than those who attended the day center. Women, those who were illiterate, those who were institutionalized and older adults who had diseases of the nervous system had a worse functional profile and greater cognitive impairment. Those with multimorbidity had a worse functional profile, and those without a spouse had greater cognitive impairment.
Conclusions
Given the functional and cognitive profile of older adults, it is necessary to adopt care practices focused on the rehabilitation/maintenance of self-care and affective relationships. This care must be provided by highly qualified professionals. Therefore, it is necessary to increase the ratio of nurses per older adult in these institutions.
Similar content being viewed by others


Background
Both physical and cognitive limitations can lead to a loss of independence in performing activities of daily living, making an individual dependent on others [1]. The functioning of older adults may be influenced by the sociodemographic, cultural and environmental context [2,3,4]. When limitations cannot be overcome with help from others, mechanical assistance or changes in the environment, the consequences can compromise the individual’s ability to perform activities of daily living and participate in society [5].
The decline in functioning, including cognitive function, and the prevalence of chronic diseases tend to worsen with age and is particularly evident starting at 80 years of age [6,7,8,9,10].
Cognitive decline is rarely evaluated, and such evaluation is especially important in individuals with multimorbidity because many people with cognitive decline also have limitations in performing activities of daily living, which hinder or prevent their self-management of diseases [11].
A recent study concluded that understanding the heterogeneity in chronic pathologies, functional limitations, geriatric syndromes and causes of death in people with cognitive impairment can contribute to adequate care management and resource allocation [11]. These factors must be considered in care management at institutions for older adults, such as in residential homes.
In Portugal, institutions for older adults comprise essentially three main modalities (day centers, home care services and residential homes). These institutions are the responsibility of the social security sector [12], which differs from other countries that have adopted the concept of “nursing homes” that provide 24-hour health care services [13]. In nursing homes, older adults with functional limitations, whether physical or mental, who require care and supervision are monitored by nurses. In Portugal, many residential homes offer nursing care for only a few hours a day, and the number of hours that care is provided is not guaranteed or regulated according to the needs of the people. The current legislation defines that only one nurse is required for every 20 to 40 residents, depending on the degree of dependence [14], and the method used to evaluate the degree of dependence has not been defined.
In view of these factors, we consider it necessary to identify the sociodemographic and pathological characteristics of older adults attending institutions for older adults in Portugal. In addition, it is essential to expand the scientific knowledge of the factors associated with functional and cognitive limitations and multimorbidity. Thus, this study had the following aims:
-
1.
To analyze the sociodemographic and pathological characteristics of older Portuguese adults attending in residential homes and day centers;
-
2.
To evaluate the association between the functioning and cognition of older adults and their sociodemographic and pathological characteristics.
Methods
Study design and participants
This was a cross-sectional, descriptive and correlational study of a quantitative nature.
The sample was composed of older adults attending 18 institutions from northern to southern Portugal. Nonprobabilistic convenience sampling was used for sample selection. All older adults from the selected institutions were considered for participation.
The sample was composed of 613 older adults who attended either a day center (n = 507) or a residential institution (n = 106). The inclusion criteria were as follows: being 65 years of age or older and having the ability to sign informed consent or having a legal representative to do so. Participants who were excluded consisted of those under the age of 65 and those who were unable to give informed consent, as the legal representative was not present at the time the data were collected.
Data collection instruments
In addition to the questionnaires administered, the following data were also collected: age, sex, marital status and education level. Information on diagnostic categories was also collected in the clinical process.
Mini Mental State Examination (MMSE)
The MMSE evaluates cognitive function and was developed by Folstein et al. (1975). The MMSE consists of six groups of questions that evaluate temporal and spatial orientation, recall, attention and calculation, repetition, language and constructive capacity [15]. Better scores indicate better cognitive ability[15]. The MMSE was adapted for the Portuguese population by Guerreiro and colleagues[16, 17].
Elderly Nursing Core Set (ENCS)
The ENCS was developed by Fonseca and collaborators, and it is used to assess the functioning of older adults[3]. The ENCS consists of 25 questions based on the International Classification of Functioning, Disability and Health (ICF) and is scored on a Likert scale from 1 to 5 points. The resulting scores yield a functional profile, as follows: (1) No disability: 0–4 %; (2) Mild disability: 5–24 %; (3) Moderate disability: 25–49 %; (4) Severe disability: 50–95 %; and (5) Complete disability: 96–100 %. The study that evaluated the psychometric characteristics of this tool showed a Cronbach’s alpha of 0.963[3]. The ENCS consists of four domains that are subdivided into various ICF codes: self-care, learning and mental functions, communication and social relationships[3]. The higher the score, the worse the functional profile of the individual[6].
Data collection procedures
After positive feedback from the ethics committee approval, permission to participate in the study was requested from the management of each of the institutions.
The researchers who collected the data received prior training on how to conduct the interviews. Data were collected between July 2019 and February 2020 at the institutions in the day center or residential home setting. Interviews were conducted to collect data from users and/or their family and/or health professionals at the institutions. Data on the total number of valid interviews were entered into the Multidimensional Integrated Assessment Platform for Elderly (MIAPe) platform[18]. The researchers recorded the responses on the MIAPE platform, assigning a code to each participant so that they would not be identified. The data were then exported from the platform to an Excel file and from there to SPSS so that they could be analyzed.
Ethical considerations
Authorization was obtained from the Ethics Committee for Scientific Research in the Areas of Human Health and Welfare of the University of Évora under reference number 19,013.
All methods were performed in accordance with the Declaration of Helsinki of 1964 and its subsequent amendments[19]. Participation in the study was explained to the participants, and informed consent was obtained from the participant or a legal representative if the participant was not able to provide it.
Data analysis
The data were analyzed using IBM SPSS Statistics version 24 for Windows. The sociodemographic variables were analyzed using descriptive statistics. The normality of the data was tested using the Kolmogorov-Smirnov test, and in the absence of a normal distribution, parametric tests were used given the sample size [20]. Thus, Pearson’s correlation was used to analyze the differences in age and the ENCS and MMSE scores. The independent t-test for independent samples was used to analyze differences in the ENCS or the MMSE scores, some sociodemographic characteristics and multimorbidity.
Results
Sample characteristics
The sample consisted of 613 older adults with a mean age of 85.73 years (± 6.890) and an age range from 65 to 100. Most were female (69.3 %), widowed (67.0 %) and over 85 years old (60.4 %). Regarding the nosological diagnosis, data could be obtained for only 572 participants, of whom 68.2 % had two or more diagnoses (multimorbidity) and only 0.5 % did not have any pathology (Table 1).
Regarding the functional and cognitive assessments, 54.5 % had cognitive impairment, and the sample as a whole had an average overall functional profile of “moderate disability” (2.34 (± 1.132)), with the worst results in the self-care domain, followed by the learning and mental function, communication and social relationship domains.
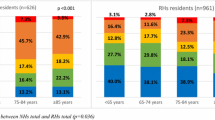
The most prevalent diagnostic category area was circulatory diseases, followed by diseases of the nervous system, including dementia; musculoskeletal system diseases; neoplasms; endocrine, nutritional and metabolic diseases; and mental and behavioral disorders (Table 2; Fig. 1).

Percentage of participants by diagnostic categories (n = 572)
Regarding the number of identified diagnostic categories, most of the sample (27.1 %) had two identified categories, and the maximum number of identified diagnostic categories was nine (Fig. 2).

Number of diagnostic categories (ICD11) identified per participant (n = 572)
Differences in functional and cognitive profiles, sociodemographic characteristics and multimorbidity
Pearson’s correlation was used to analyze the relationship between the participants’ age and average functional profile, and the higher the age, the worse the overall functional profile and the functional profile for all the ENCS domains, with a p < 0.05; the exception was the social relationship domain, for which no statistically significant differences were observed. The t-test revealed that participants with diseases of the nervous system presented worse results for the overall functional profile and in all ENCS domains, as well as on the MMSE (p < 0.001). Those with endocrine and/or metabolic diseases had worse results for the overall functional profile and in the domains of self-care and learning and mental functions (p < 0.05). There were no statistically significant differences for the other pathologies.
Pearson’s correlation for sociodemographic characteristics and the number of diseases was also analyzed, and the results indicated that older adults living in residential homes had more diseases than those who attended the day center (p < 0.05).
Table 3 shows the differences in the ENCS and MMSE scores according to the variables sex, marital status, education level, support level and multimorbidity.
Discussion
This study aimed to analyze the sociodemographic and pathological characteristics of elderly adults attending institutions for older adults and to evaluate the association between these variables and functioning and cognition.
The most notable finding was the high percentage of women in our sample (69.6 %). We know that women have greater longevity than men, a phenomenon known as the “feminization of aging” [21, 22]. However, in our sample, the number of women was more than twice the number of men, which is not consistent with data for women in the same age group living in Portugal (58.2 %). A study conducted in Portugal with older adults from the general population had a percentage of women of 52.9 % [23]. Another Portuguese study with 351 older people living at home had a percentage of women of 53.6 % [24]. These results indicate that a disproportionate number of women live in residential homes and day centers. In addition, women had a worse functional profile and more cognitive impairment than men, which indicates greater functional dependence. These data are in line with other international studies that indicate that women have higher rates of functional dependence [4, 25, 26] and cognitive deficits [26].
Regarding age, the older the age group was, the higher the proportion of the sample it comprised. Additionally, the mean age in this study (85.73 years) was higher than that in a Portuguese study conducted with older adults in the general population (80.16 years) [23]. This finding is to be expected given the need for increased care with increasing age and the need to resort to care services. Moreover, the mean age in this study was also higher than that in other international studies with older adults [27,28,29]. In fact, Portugal is the third oldest country in the European Union [30].
In relation to marital status, more than half of the participants were widowed, and only 17.8 % were married. The results indicate that married participants had better cognitive levels than unmarried participants. These data are in line with a recent longitudinal study conducted by the National Health and Aging Trends Study that concluded that unmarried older adults are particularly vulnerable to cognitive impairment, and marital status is a potentially important social protective factor [31]. Another study conducted in China with a sample of 2,498 older adults (> 55 years) concluded that being single or a widower was associated with higher cognitive impairments than being married, but only for men [32]. Another recent study concluded that social relationships can influence health and longevity, and their absence is a risk factor for premature death [33]. These data lead us to believe that the marital status of married individuals is a factor related to continuing to live at home. Thus, affective relationships should be given importance, and preventive measures to avoid cognitive impairment should be planned in advance and implemented when a spouse dies.
Most of the sample had attended school, but a significant percentage did not know how to read or write (31.8 %). Other studies with older adults showed similar data[34, 35]. Participants who had not attended school had a worse functional profile and more cognitive impairment than those who had attended school. Similar data were reported in a study of the Brazilian population in which illiterate individuals were the most dependent for instrumental activities of daily living [36]. Other studies concluded that a higher level of education is a predictor of better cognitive function [37, 38]. In addition, the higher an individual’s education level is, the better his or her physical and mental health [2, 39,40,41]. Considering these results, it is important to promote lifelong learning as a factor that contributes to healthy aging [42]. Thus, care models should focus on the promotion of literacy.
The participants who attended the day center and resided in their homes had better functional profiles and cognitive levels than those who resided in a residential center. These results are in line with those of other studies that indicate that functional dependence and cognitive impairment are predictive factors of institutionalization [43, 44]. In addition, factors such as living alone, not participating in recreational and social activities, not receiving visits from family and friends and a lack of social support are strong predictors of institutionalization in older adults [45]. Another important finding of our study is that the number of diseases was higher in the group of older adults living in residential centers. Multimorbidity may be another predictor of institutionalization, given its effect on the functional profile and, as a consequence, on the degree of dependence.
More than two-thirds of the sample had multimorbidity (68.2 %). Similar data were found in a study conducted in Scotland with older adults over 65 years of age in the general population [46]. Older adults with multimorbidity had a worse functional profile, and this finding was is in line with those of other studies with older adults [23, 47]. Participants with diseases of the nervous system, including dementias, had a worse functional profile and greater cognitive impairment and thus more dependence. These data are in line with those of other studies [48]. Scientific evidence shows that dementia is the main cause of disability in older adults [49]. Participants with endocrine, nutritional and metabolic diseases, including diabetes, had a worse functional profile. These results are in agreement with a study that indicated that Alzheimer’s disease and diabetes are among the diseases that contribute the most to disability [50].
Limitations
The limitations of the present study include the fact that it is a cross-sectional study that does not allow the establishment of a cause-effect relationship between the variables. Another limitation is the fact that multimorbidity was defined according to the medical diagnostic categories of the ICD-10 rather than the pathology itself. These limitations must be considered in the analysis of the results.
Conclusions
Understanding the factors that influence functional limitations, including cognitive limitations and multimorbidity, is an important step for the development of new care models for older adults in social support institutions. This study concluded that women, those who were illiterate, those who were institutionalized and older adults who had diseases of the nervous system had a worse functional profile and greater cognitive impairment. Those with multimorbidity had a worse functional profile, and those without a spouse had greater cognitive impairment.
Given the sociodemographic characteristics, functional and cognitive profiles and multimorbidity of older adults who attend institutions for older adults, it is necessary to adopt practices that focus on self-care. Considering the high multimorbidity and functional profile of older adults in these institutions, the social and health sectors must offer coordinated responses. In addition, care should be provided by health professionals qualified to provide assistance in self-care management, such as nurses, which is not the case in Portugal.
Therefore, it is necessary to develop new policies for implementing health promotion and disease prevention strategies in older adults in these institutions that promote active and healthy aging, as recommended by the WHO. Such efforts essentially involve the allocation of human resources in the area of health; the proper evaluation of functioning, including cognitive evaluation, on a regular basis to understand its evolution and to determine the effectiveness of care; and the adoption of care models focused on self-care management and the promotion of literacy and social relationships.
Participation in the study was explained to the participants, and informed consent was obtained from the participant or a legal representative if the participant was not able to provide it.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Harling G, Payne CF, Davies JI, et al. Impairment in activities of daily living, care receipt, and unmet needs in a middle-aged and older rural South African population: findings from the HAALSI study. J Aging Health. 2020;32(5–6):296–307. https://doi.org/10.1177/0898264318821220.
Abalo EM, Mensah CM, Agyemang-Duah W, et al. Geographical differences in perceived health status among older adults in Ghana: do gender and educational status matter? Gerontol Geriatr Med. 2018;4:233372141879666. https://doi.org/10.1177/2333721418796663.
Fonseca C, Lopes M, Mendes D, Parreira P, Mónico L, Marques C. Psychometric properties of the Elderly Nursing Core Set. In: José García-Alonso, César Fonseca, editors. Gerontechnology. IWoG 2018. Communications in computer and information science. Springer; 2019. p. 143–153. https://doi.org/10.1007/978-3-030-16028-9_13
Goes M, Lopes MJ, Oliveira H, Fonseca C, Marôco J. A nursing care intervention model for elderly people to ascertain general profiles of functionality and self care needs. Sci Rep. 2020;10(1). https://doi.org/10.1038/s41598-020-58596-1
World Health Organization. WHO | International Classification of Functioning, Disability and Health (ICF). Published 2015. http://www.who.int/classifications/icf/en/
Lopes MJ, Fonseca C. The construction of the Elderly Nursing Core Set. J Aging Inov. 2013;2(1):121–31.
Manini T. Development of physical disability in older adults. Curr Aging Sci. 2011;4(3):184–91.
Prados-Torres A, Poblador-Plou B, Calderón-Larrañaga A, et al. Multimorbidity patterns in primary care: Interactions among chronic diseases using factor analysis. PLoS One. 2012;7(2). https://doi.org/10.1371/journal.pone.0032190
Prazeres F, Santiago L. Prevalence of multimorbidity in the adult population attending primary care in Portugal: a cross-sectional study. BMJ Open. 2015;5(9):e009287. https://doi.org/10.1136/bmjopen-2015-009287.
Souza Freitas R, Fernandes MH, Da R, et al. Functional capacity and associated factors in the elderly: a population study. Acta Paul Enferm. 2012;25(6):933–99.
Schiltz NK, Warner DF, Sun J, et al. The influence of multimorbidity on leading causes of death in older adults with cognitive impairment. J Aging Health. 2019;31(6):1025–42. https://doi.org/10.1177/0898264317751946.
GEP/MTSSS. Carta Social - Rede de Serviços e Equipamentos - Relatório 2018. 2019.
National Institute on Aging. Long term care - how to choose a nursing home. Published 2017. https://www.nia.nih.gov/health/how-choose-nursing-home
Social M da solidariedade e da segurança. Portaria n.o 67/2012 de 21 de Março. Vol 1a Série. 2012. p. 1324–1329.
Folstein MF, Folstein SE, McHugh PR. Mini-mental state. J Psychiatr Res. 1975;12(3):189–98. https://doi.org/10.1016/0022-3956(75)90026-6.
Guerreiro M, Silva AP, Botelho MA, Leitão O, Castro-Caldas A, Garcia C. Adaptação à população portuguesa da tradução do Mini Mental State Examination (MMSE). Rev Port Neurol. 1994;1:9.
Guerreiro M. Contributo da neuropsicologia para o estudo das demências. Published online 1998.
Mendes DJM, Lopes MJ, García-Alonso JM, Santos J, Sousa LMM. Resilient software architecture platform for the individual care plan. In: Mendes D, Fonseca C, Lopes MJ, Garcia-Alonso J, Murillo JM, editors. Exploring the role of ICTs in healthy aging. 2020. p. 13–32. https://doi.org/10.4018/978-1-7998-1937-0.ch002
World Medical Association. World medical association declaration of Helsinki ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–4. https://doi.org/10.1001/jama.2013.281053.
Kwak SG, Kim JH. Central limit theorem: the cornerstone of modern statistics. Korean J Anesthesiol. 2017;70(2):144. https://doi.org/10.4097/kjae.2017.70.2.144.
World Health Organization. World health statistics 2019: monitoring health for the SDGs, sustainable development goals. World HealthOrganization. 2019. https://apps.who.int/iris/handle/10665/324835.
Davidson PM, DiGiacomo M, McGrath SJ. The Feminization of Aging: How Will This Impact on Health Outcomes and Services? Health Care Women Int. 2011;32(12):1031–1045. doi:https://doi.org/10.1080/07399332.2011.610539
Santiago LM, Prazeres F, Boto T, Maurício K, Rosendo I, Simões J. Multimorbidity daily life activities and socio-economic classification in the Central Portugal primary health care setting: an observational study. Fam Med Prim Care Rev. 2020;22(1):54–8. https://doi.org/10.5114/fmpcr.2020.92506.
Goes M, Lopes MJ, Marôco J, et al. The quality of life of older individuals following the world health organization assessment criteria. Geriatr. 2020;5(4):1–11. https://doi.org/10.3390/geriatrics5040102.
Safak ED, Kizilcay HD, Arguvanli S, et al. The relationship between daily living activities and cognitive function in the elderly: cross-sectional study. Yaşlılarda Günlük Yaşam Akt ve Bilişsel Fonksiyon İlişkisi Kesitsel Çalışma. 2019;11(1):30–5.
Campos ACV, e Ferreira EF, Vargas AMD. Determinantes do envelhecimento ativo segundo a qualidade de vida e gênero. Cien Saude Colet. 2015;20(7):2221–37. https://doi.org/10.1590/1413-81232015207.14072014.
Amadeus L, Nejc P, Danica Ž, Sebastjan B. Res Gerontol Nurs. 2017;10(6):260–6. https://doi.org/10.3928/19404921-20171013-03.
Muntinga ME, Jansen APD, Schellevis FG, Nijpels G. Expanding access to pain care for frail, older people in primary care: a cross-sectional study. BMC Nurs. 2016;15(1):26. https://doi.org/10.1186/s12912-016-0147-5.
Kelly ME, Duff H, Kelly S, et al. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: a systematic review. Syst Rev. 2017;6(1):259. https://doi.org/10.1186/s13643-017-0632-2.
Eurostat. Healthy life years statistics - statistics explained. Published 2020. https://ec.europa.eu/eurostat/statistics-explained/index.php/Healthy_life_years_statistics#Healthy_life_years_at_age_65
Liu H, Zhang Y, Burgard SA, Needham BL. Marital status and cognitive impairment in the United States: evidence from the National Health and Aging Trends Study. Ann Epidemiol. 2019;38:28-34.e2. https://doi.org/10.1016/j.annepidem.2019.08.007.
Feng L, Ng X-T, Yap P, et al. Marital status and cognitive impairment among community-dwelling Chinese older adults: the role of gender and social engagement. Dement Geriatr Cogn Dis Extra. 2014;4(3):375–84. https://doi.org/10.1159/000358584.
Holt-lunstad J. Why social relationships are important for physical health: a systems approach to understanding and modifying risk and protection. Published online 2018.
Lopes MJ, Escoval A, Pereira DG, Pereira CS, Carvalho C, Fonseca C. Evaluation of elderly persons’ functionality and care needs. Rev Lat Am Enfermagem. 2013;21(spe):52–60. https://doi.org/10.1590/S0104-11692013000700008.
Chang W-Y, Chen K-M, Chen M-C, Yang L-Y, Hsu H-F. Prevalence and demographic characteristics of high-need community-dwelling older adults in Taiwan. Health Soc Care Community. 2020;28(6):2382–9. https://doi.org/10.1111/hsc.13059.
Coutinho AT, de Vilela Q, Lima MBR, dede Silva MLLT. Social communication and functional independence of the elderly in a community assisted by the family health strategy. Rev CEFAC. 2018;20(3):363–73. https://doi.org/10.1590/1982-0216201820313417.
Rexroth DF, Tennstedt SL, Jones RN, et al. Relationship of demographic and health factors to cognition in older adults in the ACTIVE study. J Aging Health. 2013;25(8_suppl):128S-146S. https://doi.org/10.1177/0898264313498415.
Kujawski S, Kujawska A, Gajos M, et al. Cognitive functioning in older people. Results of the first wave of cognition of older people, education, recreational activities, nutrition, comorbidities, functional capacity studies (COPERNICUS). Front Aging Neurosci. 2018;10. https://doi.org/10.3389/fnagi.2018.00421
Cui S, Wang R, Lu L, Wang H, Zhang Y. Influence of education level on mental health and medical coping modes: a correlation analysis in the elderlies. Am J Nurs Sci. 2019;8(6):324. https://doi.org/10.11648/j.ajns.20190806.16.
Quach A, Levine ME, Tanaka T, et al. Epigenetic clock analysis of diet, exercise, education, and lifestyle factors. Aging (Albany NY). 2017;9(2):419–46. https://doi.org/10.18632/aging.101168.
Quinaz Romana G, Kislaya I, Salvador MR, Gonçalves SC, Nunes B, Dias C. Multimorbilidade em Portugal: Dados do Primeiro Inquérito Nacional de Saúde com Exame Físico. Acta Med Port. 2019;32(1):30–7. https://doi.org/10.20344/amp.11227.
UNECE Ministerial Conference on Ageing. 2017 LISBON MINISTERIAL DECLARATION “A Sustainable Society for All Ages: Realizing the potential of living longer.” Published online 2017. p. 7.
Mannucci PM, Nobili A, Mannucci PM, et al. Multimorbidity and polypharmacy in the elderly: lessons from REPOSI. Intern Emerg Med. 2014;9(7):723–34. https://doi.org/10.1007/s11739-014-1124-1.
Del Duca GF, Silva SG da, Thumé E, Santos IS, Hallal PC. Indicadores da institucionalização de idosos: estudo de casos e controles. Rev Saude Publica. 2012;46(1):147–153. https://doi.org/10.1590/S0034-89102012000100018
Oh A, Patel K, Boscardin WJ, et al. J Am Geriatr Soc. 2019;67(12):2622–7. https://doi.org/10.1111/jgs.16184.
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. https://doi.org/10.1016/S0140-6736(12)60240-2.
Peng X, Bao X, Xie Y, et al. The mediating effect of pain on the association between multimorbidity and disability and impaired physical performance among community-dwelling older adults in southern China. Aging Clin Exp Res. 2020;32(7):1327–34. https://doi.org/10.1007/s40520-019-01324-1.
Åkerborg Ö, Lang A, Wimo A, et al. Cost of dementia and its correlation with dependence. J Aging Health. 2016;28(8):1448–64. https://doi.org/10.1177/0898264315624899.
Lisko I, Kulmala J, Annetorp M, Ngandu T, Mangialasche F, Kivipelto M. How can dementia and disability be prevented in older adults: where are we today and where are we going? J Intern Med. Published online December 2020. https://doi.org/10.1111/joim.13227
DGS. IHME. Portugal: The Nation’s Health 1990–2016. An overview of the global burden of disease study 2016 results. 2018.
Acknowledgements
The authors thank all those who collaborated in the data collection; the multidisciplinary teams of the institutions involved; and, especially, all participants, because without them this study would not be possible.
Funding
This work was supported by the 4IE project (0045-4IE-4-P) funded by the Interreg V-A España-Portugal (POCTEP) 2014–2020 program.
Author information
Authors and Affiliations
Contributions
CJVF, LMGP and MJL conceived the present study within the scope of the 4IE project; analyzed and interpreted the data; and drafted the work. JGA developed the data collection platform. CJVF and MJL conceived the ENCS. LMGP contributed to the statistical analyses for all data. MJL and MCM were the senior guarantors who supervised the proposed methodology and critically revised the work for important intellectual content. All authors approved the final version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Authors’ information
CJVF has a PhD in nursing sciences. Their doctoral area is in the area of aging under the supervision of MJL, having both contributed to the construction of the ENCS. LMGP has an International PhD in nursing and health and a PhD in psychology, and her professional career focuses on the area of mental health and aging. MJL has a PhD in nursing sciences, and his professional career focuses on the area of mental health and aging; he has been the Coordinator for the NHS’s Reform in the Area of Integrated and Continuing Care. MCM has a PhD in psychology, and her professional career focuses on the area of surgical, medical and social representations in aging. JGA has a PhD in software engineering, and he has been researching in the area of gerontechnology.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Authorization was obtained from the Ethics Committee for Scientific Research in the Areas of Human Health and Welfare of the University of Évora under reference number 19013.
Consent for publication
Not applicable.
Competing interests
The authors report no conflicts of interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fonseca, C., de Pinho, L.G., Lopes, M.J. et al. The Elderly Nursing Core Set and the cognition of Portuguese older adults: a cross-sectional study. BMC Nurs 20, 108 (2021). https://doi.org/10.1186/s12912-021-00623-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-021-00623-1