
Abstract
Background
Antibiotic resistance is a major health threat. Inappropriate antibiotic use has been shown to be an important determinant of the emergence of antibiotic resistance. Decision support systems for antimicrobial management can support clinicians to optimize antibiotic prescription.
Objective
The aim of this systematic review is to identify factors influencing the implementation of decision support systems for antibiotic prescription in hospitals.
Methods
A systematic search of factors impeding or facilitating successful implementation of decision support systems for antibiotic prescription was performed in January 2022 in the databases PubMed, Web of Science and The Cochrane Library. Only studies were included which comprised decision support systems in hospitals for prescribing antibiotic therapy, published in English with a qualitative, quantitative or mixed-methods study design and between 2011 and 2021. Factors influencing the implementation were identified through text analysis by two reviewers.
Results
A total of 14 publications were identified matching the inclusion criteria. The majority of factors relate to technological and organizational aspects of decision support system implementation. Some factors include the integration of the decision support systems into existing systems, system design, consideration of potential end-users as well as training and support for end-users. In addition, user-related factors, like user attitude towards the system, computer literacy and prior experience with the system seem to be important for successful implementation of decision support systems for antibiotic prescription in hospitals.
Conclusion
The results indicate a broad spectrum of factors of decision support system implementation for antibiotic prescription and contributes to the literature by identifying important organizational as well as user-related factors. Wider organizational dimensions as well as the interaction between user and technology appear important for supporting implementation.
Similar content being viewed by others

Background
The rise of antibiotic resistance is widely acknowledged to be an increasing threat to global public health. Worldwide 700.000 people die because of antibiotic-resistant infections [1]. The development of antibiotic resistance is mainly promoted by inadequate antibiotic prescribing practices by physicians, such as antibiotic intake in viral infections, incorrect dosing and incorrect dosing cycles [2, 3]. This results in treatment problems such as prolonged hospital stays or a reduced quality of life, which can be challenging for the affected persons as well as for the whole society [4].
Providing antibiotic therapy indicates constant decision making, which requires responsibility and conscientiousness, because it can have a significant impact on patients´ health [5]. Due to the complexity of medical information, decisions are often made under uncertainty as well as with limited previous knowledge and under great time pressure [6]. In addition, medical decisions don’t base solely on medical factors, but also on the manifold organizational processes of the hospital as an institution with a high degree of division of labor [7, 8].
Information technology has become increasingly prevalent in all industries, especially in healthcare. The development of a wide variety of information systems employed to aid clinicians in decision-making [9]. One such system is called decision support systems (DSSs). These are defined as software systems that are used to facilitate decision-making for clinicians by preparing data and making it available to users in a structured and selective manner, in order to support the clinical decision [10]. Classically, DSSs use knowledge systems that rely on if–then rules. Increasingly, machine-learning techniques are used, where large data sets are used to learn from further events and so recognize certain patterns. Both methods are based on artificial intelligence that are often combined in applications [11].
Many studies demonstrate that DSSs can potentially offer considerable support for many aspects of the appropriate use of antibiotics [12] and advantages for reducing toxic drug levels and medication errors as well as costs [13, 14]. While evidence on the technological characteristics of DSSs or the effectiveness on clinical outcomes are widespread [15,16,17], there is a need of evidence that provides insights into wider social and organizational aspects that needed to accompany successful implementation [18, 19]. Although there are diverse approaches explaining the adoption of DSSs, relevant studies often describe the effects of a DSS on level of disease management without addressing the importance of matching user-related characteristics, the technology being implemented and the organizational circumstances all together [20, 21]. The aim of this systematic review is to identify facilitating and impeding factors of DSS implementation for antibiotic prescription in hospitals at the levels of technology, organization as well as user and by use of a sociotechnical framework.
Methods
The search, systematization and analysis of literature follows the recommendations of the PRISMA statement [22].
Search strategy
An extensive search of literature was performed in the databases PubMed, The Cochrane Library and Web of Science from May 2021 to January 2022. A search syntax was developed based on relevant search terms. Various search techniques as well as different operators and combinations (AND, OR, *) were used when entering the search terms (Additional file 1: Table S1). Additionally, the reference lists of the identified studies have been searched for further relevant references.
Eligibility of studies
In a first step, publications were screened for title and abstract according to inclusion and exclusion criteria individually by the first (PT) and second author (JH). The inclusion criteria comprised (1) DSSs for prescribing antibiotic therapy, (2) DSSs used in hospitals for clinical practice, (3) studies in English with a qualitative, quantitative or mixed-methods study design, (4) published between 2011 and 2021 and (5) examining DSS implementation factors. Exclusion criteria were (1) studies analyzing the technological development of DSSs without practical relevance and (2) DSSs in outpatient care. Studies that seemed to meet the inclusion criteria were selected for a full text review. Second, the full papers of the resulting set of publications was retrieved and reviewed, again by the first (PT) and second author (JH). Any disagreement about the inclusion of a publication between the two reviewers was resolved thorough discussion and, if required, the third author (CD) was consulted.
Data extraction
The articles were extracted using standardized table formats with the following parameters:
-
Authors and publication year
-
Country
-
Funding of the study
-
Study design
-
Sample size
-
Targeted group
-
Characteristics of the DSS
-
Methodological quality
Despite diverse approaches explaining the implementation of DSSs, the interface between technology-organization-user has been insufficiently considered. To describe and categorize the identified implementation factors, the Human-Organization-Technology-fit-model (HOT-fit model) of Yusof et al. [23] was chosen as a theoretical framework in this paper (Fig. 1).

Human–Organization–Technology-fit framework [23]
It focuses the fit between the three domains technology, human and organization and maps their relationships and possible interactions, as well. The three domains comprise subdomains, so that the factors can be mapped onto seven interrelated dimensions: System use and user satisfaction in the human domain, structure and environment in the organizational domain and system quality, information quality and service quality in the technological domain. The framework is completed with the dimension net benefits, which comprises the potential negative and positive impacts on individual, organizational or societal level. All these dimensions influence each other in a temporal and causal way. This model has been developed and validated for the implementation and evaluation of innovations in organizations, especially in hospitals [24, 25]. On this basis, not only the static user and system attributes but also dynamic organizational processes that can influence the implementation process will be elaborated. The implementation factors were identified thematically by the first and second author by textual analysis of the included publications. The factors were individually mapped to the HOT-fit dimensions, as described in Table 1. Furthermore, each factor was categorized as either impeding (for example reported on in a publication as hindering or obstructing implementation of DSSs) or facilitating (for example reported on in a publication as positively influencing DSSs implementation). A narrative synthesis was further performed to summarize the evidence on factors most often and less reported respectively.
Quality assessment
A critical evaluation of the methodological study quality was performed using the Mixed Methods Appraisal Tool (MMAT) version 2011 [26]. This scoring system is specially developed to concomitantly appraise the methodological quality of qualitative, quantitative and mixed methods studies. The scoring system contains specific quality criteria, which are assessed, if applicable or not. An overall quality score is than calculated as percentage. Publications were scored after the inclusion process by first and second author individually. Disagreement were resolved by consensus. For a better overview and in line with the calculation of the overall score, the quality of the included studies was classified into categories based on the percentages achieved (Table 2).
Results
Study selection
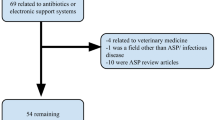
In total, 975 publications were identified through the databases The Cochrane Library, PubMed and Web of Science (Fig. 2). Duplicates were sorted out and appropriate studies were included in a second screening. 14 publications met the inclusion criteria and were included in the qualitative analysis.

PRISMA flow diagram of literature search and selection process [22]
Study characteristics
A total of five publications were identified from Australia [27,28,29,30,31], two studies from the Netherlands [32, 33] and two publications from Singapore [34, 35]. In addition, one study was conducted in Malaysia [36], one in Sweden [37], one in the United States [38] and in Portugal [39]. One study was conducted concomitantly in France and Switzerland [40]. Most studies (n = 6) used a combination of qualitative and quantitative methods [29, 30, 32, 34, 35, 37] or only qualitative methods (n = 5) [28, 33, 38,39,40]. Three studies used quantitative methods [27, 31, 36].
In the majority of publications (n = 11) the DSS was fully embedded in existing systems, such as the electronic health record [27,28,29,30,31, 33,34,35,36, 39, 40]. In two publications, the DSS was designed as a standalone system that operated independently from existing technical structure [32, 37]. In one study, the DSS characteristics are not described [38]. The quality assessment of the included studies resulted in an average quality score of 75% (range 50–100%). Thereby, all studies fulfilled at least 50% of the MMAT criteria and had at least a moderate quality level. An overview of the quality assessment of included publications (Additional file 2: Table S2) as well as the study characteristics can be found in Additional file 3: Table S3.
Barriers and facilitators of DSS implementation
A total of 61 factors were identified (Tables 3, 4). Of these, 25 factors could be assigned to the technology-related domain, 15 factors to the organizational domain and eleven factors to the user-related domain. Ten factors included the net benefits of DSSs.
Within the technology domain, with 76% the majority of factors refers to system quality (n = 19/25) and with approx. 24% to information quality (n = 6/25). No factor could be assigned to the area of service quality. The compatibility of the DSS with already existing systems [27, 32, 34, 35, 37, 39] and the flexibility of the system [32, 33, 36, 37] are recognized as facilitating for successful implementation. In contrast, the incompatibility of the DSS with existing systems and the resulting double documentation [38, 39] as well as a complicated access to the DSS [29, 39] are described as impeding.
About 87% of the organizational factors (n = 13/15) can be assigned to structural conditions and about 13% to the organizational environment (n = 2/15). With 57% the majority of publications (n = 8/14) examines factors related to participation and the integration of potential user groups in the planning, development and implementation phases as facilitating for implementation [27,28,29, 31, 32, 36, 38, 39]. Moreover, the attitude of senior physicians in particular is crucial, so that a negative attitude can have a negatively impact on the implementation of DSSs in practice [28, 30, 38]. On the other hand, insufficient technical equipment or workstations represent impeding aspects [27, 28].
In the human domain, about 91% (n = 10/11) of the factors relate to system use and only two factors to user satisfaction (about 9%). In this context, a positive attitude towards technologies is positively associated with the use of the technology [28, 34, 37, 38] while a negative attitude imped successful implementation [27, 36]. Moreover, prior experience with DSSs is positively associated with successful implementation [32, 38], while insufficient familiarity with DSSs leads to less acceptance and not successful implementation [27, 28, 33, 40]. Additionally, a lack of satisfaction impedes the successful implementation of DSSs [27, 30].
Apart from these three domains, twelve publications examine positive and negative effects of DSS implementation [27, 28, 30,31,32, 34,35,36,37,38,39,40]. The factors predominantly relate to the impact of DSSs on workflow [27, 28, 30, 32, 34, 35, 37,38,39,40], perceptions of professional autonomy [27, 28, 31, 32, 36, 40] and time constraints [27, 28, 32, 38, 40].
Discussion
Main findings
In undertaking this review, we have provided an overall picture of the current evidence surrounding existing factors to promote the implementation of DSSs for antibiotic prescription in hospitals. Multiple factors could be identified that might affect the success or failure of DSS implementation. According to the HOT-fit framework, the majority of factors could be assigned to the domain of technology and organization.
Clearly, a successful DSS is dependent on the completeness and accuracy of the evidence base used to support it and the technical design of the system modalities. However, DSS is not just about technical content or technical design; DSSs involve workflow. DSSs are as much an organizational as a technical intervention, and organizational, professional and other challenges to implementing DSSs may be as daunting as the technical challenges [41]. The findings of this review show that intraorganizational standards or rules might not be compatible with the implementation of new technologies like DSSs and that members of the organization first have to be convinced from potential advantages of DSSs. Adopting a new technology is often about getting out of comfort zone and laying hands on to new things that require some extra effort, which can be challenging both for organizations as well as the individuals being a part of the organization [41].
Thus, factors concerning the potential impact of implementing DSSs, such as the time required or integration into existing workflow are assessed as fundamental to the implementation process. A disrupted workflow can lead to increased cognitive effort, more time required to prescribe and less time face-to-face with patients [42]. How to integrate DSSs with clinicians´ workflow, however, remains a challenge, in part because there are no current standards for clinical workflow. With regard to organizational factors, this review points out that it is crucial to pay attention to the social context i.e. the hospital setting when designing and implementing DSSs. This requires the need for developing strategies that consider the organizational structures and the specific roles of potential target groups in this social context. In addition, the success of DSSs is determined by the policies, norms and culture of the organization in which they are being used [43]. In fact, special attention should be paid to the integration and implementation of DSSs in hospitals, as well as their adoption and utilization by clinicians. Co-design including clinicians and system developers may be key for success and allow to study the interaction between health professionals and DSSs and promote the implementation in clinical practice [44]. To enable DSSs to improve clinical workflow, the use of user-centered design principles and techniques during the initial design phase seem crucial. In particular, determining needs rather than user desires is an important consideration.
This work can be taken forward as a basis for designing and integrating DSSs for antibiotic prescription in a hospital setting, since central components of such interventions need to build on the existing literature, as identified in this work and on existing guidance surrounding the development and evaluation of complex interventions [45]. Ideally, future work should consist of multicenter randomized controlled trials. Embedding qualitative evaluation would ensure that end-user perspectives are considered properly. Given the complex effects of DSSs and variety of settings in which they are used, randomized controlled trials may not be feasible, in which case quasi-experimental studies may be considered. In this context, paying attention to both social and technical dimensions of change as well as drawing on longitudinal qualitative designs for integration user perspective is central for going forward [46].
In relation to systems design there are various options that can help to promote the appropriate use of antibiotics. These include the availability of large volumes of electronic data, which allows the provision of reliable recommendations and so increases the trustworthiness of the DSS. Moreover, an easy access to the DSS and understandable provision of relevant data are crucial. As described in the most of the publications [27, 32, 34, 35, 37, 39] embedding DSS in existing technical structures, like electronic health records or hospital information systems can yield synergistic effects in improving implementation process, as additional effort to learn to operate with the new technical infrastructure is minimized [42, 47, 48].
In any case, appropriate organizational and social components will need to play an essential part. For this reason, it is important to identify stakeholders that support implementation and a multidisciplinary team to achieve realization, distribution and continuation. The literature synthesis also showed that training with the new system and the availability of educational material are important contributors to successful implementation [49]. In light of these findings, clinicians should receive enhanced and hands-on training prior to implementation to familiarize them as much as possible with the system before it is actually implemented in daily practice [48].
Sociotechnically guided work can also help to ensure the improvement in clinicians’ performance regarding antibiotic prescription effectively. Here, examination the interaction of technical features and user interfaces as well as organizational aspects such as training will be crucial. User perspectives and needs are equally important factors in DSS implementation, which are closely related to the requirement to involve potential user groups early in the development process. For the successful development and implementation of new technical systems it is also essential that various stakeholders are able to integrate their different knowledge and perspectives in this process. By involving relevant target groups, a positive attitude towards advantages and the benefits of DSSs can arise [47].
As highlighted in this review, DSS facilitates decision-making and thus reduces the burden on clinicians. However, when used regularly, the degree of reliance or trust on DSS can also generate a form of dependency. Additionally, the user’s ability to act may be limited, when the system fails [41]. Also, the risk of “deskilling” clinicians who use DSSs and the importance of minimizing the perceived threats to professional autonomy are commonly cited in previous reviews [42, 50,51,52], as well as in this review. In this context, trust is an important success factor, so that traceability and transparency should be created when using DSSs. Trust is a social construction that originates from interpersonal relationships [53]. Due to its relationship-based nature, it has been argued that trust is multifaceted and that the formation of trusting beliefs involves conjunctive underlying reasons [54]. Prior research suggests that trust can be attributed to a variety of causes, such as dispositional, calculative, institutional and knowledge-based reasons [53]. A DSS, that informs users about how and why it performs in a certain way, enables users to better understand its recommendations [55]. It should provide the necessary knowledge and guidance for them to make informed choices when prescribing antibiotics. Additionally, institution-based trust is crucial for trust formation. It is associated with societal structures, that represent institutional safeguards, on which the members of the institution can rely on. Structural assurance is an assessment of trust based on contextual conditions, e.g., regulations, involvement and legal guidelines [53]. Moreover, trust in technologies influences persons´ use of technology and their perception of the advantages provided by these technologies [55]. Users´ expectation about DSS design and performance can influence trust in DSS due to an interactive reason. Understanding trust formation in DSS will assist researchers and practitioners in identifying the design that augments users´ trust and supporting their professional abilities concurrently, which will consequently increase the acceptance of DSSs. Future research is therefore recommended on DSS design that can enhance users´ trust in DSSs for antibiotic prescription.
The likely difficulty for any future work in this area is the complexity of DSSs. These are likely to consist of multiple components accompanied by organizational characteristics. This justifies the high importance of future research integrating the user perspective. Embedded qualitative designs can help to facilitate insights into which components are potentially transferable between settings for antibiotic prescribing. Such work is also needed to gain deeper insights into the impact on time and reservations amongst users as well as other reasons as to why DSS implementation for antibiotic prescription is not successful [56].
Strength and limitations
The mixed method synthesis approach, which has been used to identify factors for DSS implementation has several strength. First, due to the large variety in the methods used in research, combining the results of quantitative, qualitative and mixed methods studies was well suited for this review. The multilevel approach chosen for this review was expedient, since different types of factors, which are important for DSS implementation for antibiotic prescription in hospitals, were considered. We, however, considered publications published in the last decade, so that only studies on current generation of DSSs were included. Third, we applied a systematic approach for data extraction with two independent researcher assessing the inclusion criteria per publication, extracting implementation factors and mapping these to the dimensions of the HOT-fit framework. However, several of the identified factors- impeding as well as facilitating- are not unique to DSSs for antibiotic prescribing. Nevertheless, findings from this review also highlight factors that are specific to antibiotic prescription in hospitals and should be considered. For instance, guidance and recommendations for antibiotic treatment require in most cases more detailed information about patient history, previous antibiotic exposure, local resistance patterns and proper examination of microbiological test results. The provision of flexible and comprehensible recommendations appears to be an important factor to increase the uptake of DSSs like highlighted in this review. Indeed, several studies have reported a correlation between DSS adoption and their impact on antibiotic prescription [57, 58], which highlights the need to assess not only the effects of DSSs on antibiotic prescription but also their implementation process. In order to optimize DSS implementation for antibiotic prescription, current gaps in implementation and evaluation should be addressed, which comprises, inter alia, user satisfaction and the impact on clinicians´ attitude in line with specific organizational characteristics. In fact, this review might be considered as a basis for further research of DSS implementation in the field of antibiotic prescribing in hospitals.
The interpretation of the results of this review and their representativeness requires the consideration of some methodological limitations. Despite the intensive efforts, it is possible that not all relevant studies have been identified as some may not be available in the public domain, and others may be published outside the peer-reviewed academic literature. Furthermore, the MMAT has been used to assess the methodological quality of the studies. One advantage of this assessment tool is the easy applicability, since criteria are assessed, which are only dichotomously differentiated. However, this leads to the major disadvantage that only a rough differentiation of the quality assessment of the included studies can be made. Final limitation of this review is that the HOT-fit framework was considered useful; the mapping of factors to the HOT-fit framework was a subjective undertaking of two independent researchers. Some factors proved to be difficult to map to one specific evaluation measure of a certain dimension, because these evaluation measures were sometimes not clearly defined or ambiguous. Additionally, the mapping does not reflect the level of interaction between the various factors and their relative importance. Importantly, the findings may not necessarily indicate the significance of a particular issue. Rather, the relative weight of these factors should be determined in developing and implementing DSSs. Nevertheless, the consideration of the HOT-fit framework was expedient to systemize implementation factors and to highlight the importance of paying attention to technical components and the users as well as the surrounding environment for the implementation process all together [59]. Furthermore, by using sociotechnical frameworks during the development and implementation phase of DSSs, possible impeding or facilitating factors can be identified in an early stage and so appropriate strategies can be defined to increase the success of DSS implementation for antibiotic prescription in hospitals.
Conclusion
There is yet inconclusive evidence about the factors influencing the implementation of DSSs for antibiotics prescription in hospitals. The wide range of identified impeding and facilitating factors contribute to the understanding of the implementation process and suggest that there is no “one size fits all approach”. In future, there is a clear need to pay closer attention to social as well as human components and with a broader organizational focus when developing and implementing DSSs for antibiotic prescription in hospitals.
Abbreviations
- DSS:
-
Decision support system
- HOT-fit-model:
-
Human–Organization–Technology-fit-model
- MMAT:
-
Mixed Methods Appraisal Tool
References
Taylor A, Littmann J, Holzscheiter A, Voss M, Wieler L, Eckmanns T. Sustainable development levers are key in global response to antimicrobial resistance. Lancet. 2019. https://doi.org/10.1016/S0140-6736(19)32555-3.
Kern WV. Rationale Antibiotikaverordnung in der Humanmedizin. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2018. https://doi.org/10.1007/s00103-018-2727-x.
Sauskojus H, Wagner-Ahlfs C, Razum O. Antibiotikaresistenz: In welchen Handlungsfeldern muss mehr getan werden? Gesundheitswesen. 2019. https://doi.org/10.1055/s-0042-123847.
Wieler LH, Broich K. Antibiotikaresistenzen: Große Herausforderungen erfordern komplexe Lösungen. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2018. https://doi.org/10.1007/s00103-018-2732-0.
Hausmann D, Zulian C, Battegay E, Zimmerli L. Tracing the decision-making process of physicians with a Decision Process Matrix. BMC Med Inform Decis Mak. 2016. https://doi.org/10.1186/s12911-016-0369-1.
Faller H, Meng K, Neuderth S, Richard M. Urteilsbildung und Entscheidung. In: Faller H, Lang H, editors. Medizinische Psychologie und Soziologie. Berlin: Springer; 2019. p. 265–74.
Vogd W, Feißt M, Molzberger K, Ostermann A, Slotta J. Entscheidungsfindung im Krankenhausmanagement. Wiesbaden: Springer Fachmedien; 2018. https://doi.org/10.1007/978-3-658-17001-1.
Weber J. Alle entscheidenden Konzepte, Steuerungssysteme und Instrumente für Managerund Controller. Weinheim: Wiley; 2005.
Gluchowski P, Gabriel R, Dittmar C. Management support systeme und business intelligence. Berlin: Springer; 2008. https://doi.org/10.1007/978-3-540-68269-1.
Haefeli WE, Seidling HM. Elektronische Entscheidungsunterstützung zur Annäherung an eine sichere Arzneimitteltherapie. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2018. https://doi.org/10.1007/s00103-017-2685-8.
Börm P. Leitlinienbasierter Clinical decision support—Anforderungen an evidenzbasierte Entscheidungsunterstützungssysteme. OP-JOURNAL. 2021. https://doi.org/10.1055/a-1284-3193.
Rawson TM, Moore LSP, Hernandez B, et al. A systematic review of clinical decision support systems for antimicrobial management: Are we failing to investigate these interventions appropriately? Clin Microbiol Infect. 2017;23(8):524–32. https://doi.org/10.1016/j.cmi.2017.02.028.
Main C, Moxham T, Wyatt JC, Kay J, Anderson R, Stein K. Computerised decisionsupport systems in order communication for diagnostic, screening or monitoring test ordering: systematic reviews of the effects and cost-effectiveness of systems. Health Technol Assess. 2010. https://doi.org/10.3310/hta14480.
Rothman B, Leonard JC, Vigoda MM. Future of electronic health records: implicationsfor decision support. Mt Sinai J Med. 2012. https://doi.org/10.1002/msj.21351.
Rittmann B, Stevens MP. Clinical decision support systems and their role in antibiotic stewardship: a systematic review. Curr Infect Dis Rep. 2019. https://doi.org/10.1007/s11908-019-0683-8.
Curtis CE, Al Bahar F, Marriott JF. The effectiveness of computerised decision support on antibiotic use in hospitals: a systematic review. PLoS ONE. 2017. https://doi.org/10.1371/journal.pone.0183062.
Baysari MT, Lehnbom EC, Li L, Hargreaves A, Day RO, Westbrook JI. The effectiveness of information technology to improve antimicrobial prescribing in hospitals: a systematic review and meta-analysis. Int J Med Inform. 2016. https://doi.org/10.1016/j.ijmedinf.2016.04.008.
Van Dort BA, Penm J, Ritchie A, Baysari MT. The impact of digital interventions on antimicribial stewardship in hospitals: a qualitative synthesis of systematic reviews. J Antimicrob Chemother. 2022. https://doi.org/10.1093/jac/dkac112.
Nabovati E, Jeddi FR, Farrahi R, Anvari S. Information technology interventions to improve antibiotic prescribing for patients with acute respiratory infection: a systematic review. Clin Microbiol Infect. 2021. https://doi.org/10.1016/j.cmi.2021.03.030.
Carracedo-Martinez E, Gonzalez-Gonzalez C, Teixeira-Rodrigues A, Prego Dominguez J, Takkouche B, Herdeiro MT, et al. Computerized clinical decision support systems and antibiotic prescribing: a systematic review and meta-analysis. Clin Ther. 2019. https://doi.org/10.1016/j.clinthera.2019.01.018.
Neugebauer M, Ebert M, Vogelmann R. A clinical decision support system improves antibiotic therapy for upper urinary tract infection in a randomized single-blinded study. BMC Health Serv Res. 2020. https://doi.org/10.1186/s12913-020-5045-6.
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MW, et al. Cochranehandbook for systematic reviews of interventions. Chichester West Sussex: Wiley; 2019.
Yusof MM, Papazafeiropoulou A, Paul RJ, Stergioulas LK. Investigating evaluation frameworks for health information systems. Int J Med Inform. 2008. https://doi.org/10.1016/j.ijmedinf.2007.08.004.
Erlirianto LM, Ali AHN, Herdiyanti A. The implementation of the human, organization, and technology-fit (HOT–Fit) framework to evaluate the electronic medical record (EMR) system in a hospital. Procedia Comput Sci. 2015. https://doi.org/10.1016/j.procs.2015.12.166.
Puspita SC, Supriyantoro H. Analysis of hospital information system implementation using the human–organization–technology (HOT) fit method: a case study hospital in Indonesia. Eur J Bus Manag Res. 2020. https://doi.org/10.24018/ejbmr.2020.5.6.592.
Souto RQ, Khanassov V, Hong QN, Bush PL, Vedel I, Pluye P. Systematic mixed studies reviews: updating results on the reliability and efficiency of the Mixed Methods Appraisal Tool. Int J Nurs Stud. 2015. https://doi.org/10.1016/j.ijnurstu.2014.08.010.
Zaidi STR, Marriott JL. Barriers and facilitators to adoption of a web-based antibiotic decision support system. South Med Rev. 2021;5(2):42–50.
Zaidi STR, Thursky KA. Using formative evaluation to improve uptake of a web-based tool to support antimicrobial stewardship. J Clin Pharm Ther. 2013. https://doi.org/10.1111/jcpt.12093.
Diasinos N, Baysari M, Kumar S, Day RO. Does the availability of therapeutic drugmonitoring, computerised dose recommendation and prescribing decision support services promote compliance with national gentamicin prescribing guidelines? Intern Med J. 2015. https://doi.org/10.1111/imj.12627.
Baysari MT, Del Gigante J, Moran M, Sandaradura I, Li L, Richardson KL, et al. Redesign of computerized decision support to improve antimicrobial prescribing. A controlled before and-after study. Appl Clin Inform. 2017. https://doi.org/10.4338/ACI2017040069.
Chavada R, Walker HN, Tong D, Murray A. Changes in antimicrobial prescribing behavior after the introduction of the antimicrobial stewardship program: a pre- and postintervention survey. Infect Dis Rep. 2017. https://doi.org/10.4081/idr.2017.7268.
Beerlage-de Jong N, Wentzel J, Hendrix R, van Gemert-Pijnen L. The value ofparticipatory development to support antimicrobial stewardship with a clinical decisionsupport system. Am J Infect Control. 2017. https://doi.org/10.1016/j.ajic.2016.12.001.
Akhloufi H, Verhaegh SJC, Jaspers MWM, Melles DC, van der Sijs H, Verbon A. Ausability study to improve a clinical decision support system for the prescription of antibioticdrugs. PLoS ONE. 2019. https://doi.org/10.1371/journal.pone.0223073.
Chow A, Lye DCB, Arah OA. Psychosocial determinants of physicians’ acceptance of recommendations by antibiotic computerised decision support systems: a mixed methods study. Int J Antimicrob Agents. 2015. https://doi.org/10.1016/j.ijantimicag.2014.10.009.
Chow AL, Ang A, Chow CZ, Ng TM, Teng C, Ling LM, et al. Implementation hurdles ofan interactive, integrated, point-of-care computerised decision support system for hospitalantibiotic prescription. Int J Antimicrob Agents. 2016. https://doi.org/10.1016/j.ijantimicag.2015.12.006.
Esmaeilzadeh P, Sambasivan M, Kumar N, Nezakati H. Adoption of clinical decision support systems in a developing country: Antecedents and outcomes of physician’s threat to perceived professional autonomy. Int J Med Inform. 2015. https://doi.org/10.1016/j.ijmedinf.2015.03.007.
Forsman J, Anani N, Eghdam A, Falkenhav M, Koch S. Integrated information visualization to support decision making for use of antibiotics in intensive care: design and usability evaluation. Inform Health Soc Care. 2013. https://doi.org/10.3109/17538157.2013.812649.
Giuliano CA, Binienda J, Kale-Pradhan PB, Fakih MG. “I never would have caught that before”: pharmacist perceptions of using clinical decision support for antimicrobial stewardship in the United States. Qual Health Res. 2018. https://doi.org/10.1177/1049732317750863.
Simões AS, Maia MR, Gregório J, Couto I, Asfeldt AM, Simonsen GS, et al. Participatory implementation of an antibiotic stewardship programme supported by an innovative surveillance and clinical decision-support system. J Hosp Infect. 2018. https://doi.org/10.1016/j.jhin.2018.07.034.
Catho G, Centemero NS, Catho H, Ranzani A, Balmelli C, Landelle C, et al. Factors determining the adherence to antimicrobial guidelines and the adoption of computerized decision support systems by physicians: a qualitative study in three European hospitals. Int J Med Inform. 2020. https://doi.org/10.1016/j.ijmedinf.2020.104233.
Eichner J, Das M. Challenges and barriers to clinical decision support (CDS) design and implementation experienced in the agency for healthcare research and quality CDS demonstrations. Agency Healthc Res Qual. 2010.
Devaraj S, Sharma SK, Fausto DJ, Viernes S, Kharrazi H. Barriers and facilitators to clinical decision support systems adoption: a systematic review. J Bus Adm Res. 2014. https://doi.org/10.5430/jbar.v3n2p36.
Karsh B-T. Clinical practice improvement and redesign: how change in workflow can be supported by clinical decision support. Agency Healthc Res Qual. 2009.
Greenhalgh T, Wherton J, Papoutsi C, et al. Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Med Internet Res. 2017. https://doi.org/10.2196/jmir.8775.
Campbell M, et al. Framework for design and evaluation of complex interventions to improve health. BMJ. 2000. https://doi.org/10.1136/bmj.321.7262.694.
Berg M. Patient care information systems and health care work: a sociotechnical approach. Int J Med Inform. 1999. https://doi.org/10.1016/s1386-5056(99)00011-8.
Liberati EG, Ruggiero F, Galuppo L, Gorli M, González-Lorenzo M, Maraldi M, et al. Whathinders the uptake of computerized decision support systems in hospitals? A qualitativestudy and framework for implementation. Implement Sci. 2017. https://doi.org/10.1186/s13012-017-0644-2.
Jenders RA. Advances in clinical decision support: highlights of practice and the literature 2015–2016. Yearb Med Inform. 2017. https://doi.org/10.15265/IY-2017-012.
Silhavy P, Silhavy R, Prokopova Z. Patients’ perspective of the design of provider patients electronic communication services. Int J Environ Res Public Health. 2014. https://doi.org/10.3390/ijerph110606231.
Van Dort BA, Zheng WY, Baysari MT. Prescriber perceptions of medication-related computerized decision support systems in hospitals: a synthesis of qualitative research. Int J Med Inform. 2019. https://doi.org/10.1016/j.ijmedinf.2019.06.024.
Sutton RT, Pincock D, Baumgart DC, Sadowski DC, Fedorak RN, Kroeker KI. An overview of clinical decision support systems: benefits, risks, and strategies for success. NPJ Digit Med. 2020. https://doi.org/10.1038/s41746-020-0221-y.
Trivedi MH, Daly EJ, Kern JK, Grannemann BD, Sunderajan P, Claassen CA. Barriers to implementation of a computerized decision support system for depression: an observational report on lessons learned in “real world” clinical settings. BMC Med Inform Decis Mak. 2009. https://doi.org/10.1186/1472-6947-9-6.
McKnight DH, Cummings LL, Chervany NL. Initial trust formation in new organizational relationships. Acad Manag Rev. 1998.
Hewstone M. Causal attribution: from cognitive processes to collective beliefs.1989.
Bussone A, Stumpf S, O’Sullivan D. The role of explanations on trust and reliance in clinical decision support systems. Int Conf Healthc Inform. 2015. https://doi.org/10.1109/ICHI.2015.26.
Kesselheim AS, et al. Clinical decision support systems could be modified to reduce ‘alert fatigue’ while still minimizing the risk of litigation. Health Aff. 2011. https://doi.org/10.1377/hlthaff.2010.1111.
Richardson S, Mishuris R, O’Connell A, Feldstein D, Hess R, Smith P, McCullagh L, McGinn T, Mann D. “Think aloud” and “Near live” usability testing of two complex clinical decision support tools. Int J Med Inform. 2017. https://doi.org/10.1016/j.ijmedinf.2017.06.003.
Khadem TM, Ergen HJ, Salata HJ, Andrzejewski C, McCreary EK, Massih RCA, Bariola JR. Impact of clinical decision support system implementation at a community hospital with an existing tele-antimicrobial stewardship program. 2022. https://doi.org/10.1093/ofid/ofac235.
Patel VL, Kannampallil TG. Human factors and health information technology: current challenges and future directions. Yearb Med Inform. 2014. https://doi.org/10.15265/IY-2014-0005.
Acknowledgements
Not applicable.
Funding
This Project was financially supported by a Grant of the Federal Ministry of Health. The Federal Ministry of Health played no role in the planning and conceptualization of the manuscript did not participate in the writing of the manuscript and played no role in the decision to submit the manuscript. We acknowledge support for the publication costs from the Open Access Publication Fund of the University of Siegen. Open Access funding enabled and organized by Projekt DEAL. No other funding was provided.
Author information
Authors and Affiliations
Contributions
Conceptualization and literature search, PT and JH; data analysis, PT and JH; writing—original draft preparation, PT; writing—review and editing PT, JH and CD. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interest
The authors declare that there are no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Table S1.
Search strategy.
Additional file 2. Table S2.
Appraisal of the methodological quality.
Additional file 3. Table S3.
Study characteristics.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tokgöz, P., Hafner, J. & Dockweiler, C. Factors influencing the implementation of decision support systems for antibiotic prescription in hospitals: a systematic review. BMC Med Inform Decis Mak 23, 27 (2023). https://doi.org/10.1186/s12911-023-02124-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12911-023-02124-4