
Abstract
Background
Respecting patients’ confidentiality is an ethical and legal responsibility for health professionals and the cornerstone of care excellence. This study aims to assess health professionals’ knowledge, attitudes, and associated factors towards patients’ confidentiality in a resource-limited setting.
Methods
Institutional based cross-sectional study was conducted among 423 health professionals. Stratified sampling methods were used to select the participants, and a structured self-administer questionnaire was used for data collection. The data was entered using Epi-data version 4.6 and analyzed using SPSS, version 25. Bi-variable and multivariable binary logistic regression analyses were used to measure the association between the dependent and independent variables. Odds ratio with 95% confidence intervals and P value was calculated to determine the strength of association and to evaluate statistical significance.
Result
Out of 410 participants, about 59.8% with [95% CI (54.8–68.8%)] and 49.5% with [95% CI (44.5–54.5%)] had good knowledge and favorable attitude towards patents confidentiality respectively. Being male (AOR = 1.63, 95% CI [1.03–2.59]), taking training on medical ethics (AOR = 1.73, 95% CI = [1.11–2.70]), facing ethical dilemmas (AOR = 3.07, 95% CI [1.07–8.79]) were significantly associated factors for health professional knowledge towards patients’ confidentiality. Likewise, taking training on medical ethics (AOR = 2.30, 95% CI [1.42–3.72]), having direct contact with the patients (AOR = 3.06, 95% CI [1.12–8.34]), visiting more patient (AOR = 4.38, 95% CI [2.46–7.80]), and facing ethical dilemma (AOR = 3.56, 95% CI [1.23–10.26]) were significant factors associated with attitude of health professionals towards patient confidentiality.
Conclusion
The findings of this study revealed that health professionals have a limited attitude towards patient confidentiality but have relatively good knowledge. Providing a continuing medical ethics training package for health workers before joining the hospital and in between the working time could be recommended to enhance health professionals’ knowledge and attitude towards patient confidentiality.
Similar content being viewed by others


Introduction
Confidentiality refers to the restriction of access to personal information from unauthorized persons and processes at authorized times and in an authorized manner [1, 2]. When we say patients have the right to confidentiality, it refers to keeping privileged communication secret and cannot be disclosed without the patient’s authorization [3, 4].
Health professionals have a legal obligation to handle patients' information privately and securely [5]. As a result, patients and professionals develop trust and a positive relationship. If such highly sensitive data is improperly disclosed, it could threaten patients' safety [6]. Hence confidentiality needs to be respected to protect patients’ well-being and maintain society’s trust in the physician–patient relationship. The issue of confidentiality has been recognized as a global concern. As a result, several internationally agreed on principles and guidelines for maintaining the sanctity of patients’ private lives during treatment. This law, known as Data Protection Act, was enacted in 1998 and was last revised in 2018 [7, 8]. The Data Protection Act was created to provide protection and set guidelines for handling personal data [7]. There is no comprehensive data protection law in Ethiopia that covers health data protection [9]. Ethiopia's only confidentiality-oriented policy is the healthcare administration law, which requires health practitioners to maintain confidentiality. This law mandates health providers to keep patients' health information confidential [10]. Furthermore, only a few research have looked into health professionals' awareness of ethical rules and data security and sharing laws in Ethiopia [9].
Confidentiality is the basis of the legal elements of health records and an ethical cornerstone of excellent care [11]. More importantly, the quality of information shared with healthcare experts is determined by their capacity to keep it private. Otherwise, the patient may withhold important information, lowering the quality of care offered.
Although information sharing is essential in an interdisciplinary health team, each professional should limit information disclosure to an unauthorized health professional to plan and carry out procedures in the patient's best interests [12]. The exchange of patient medical records and data with an unauthorized person continues to be a common occurrence in a variety of clinical settings [5]. Breaches of confidentiality in clinical practice due to negligence, indiscretion, or sometimes even maliciously jeopardize a duty inherent in the physician–patient relationship [8]. Breaches of confidentiality and sharing data with unauthorized parties may have the potential to harm the patients’ health [13]. Health care quality declines due to a loss of confidence in the professional-patient relationship [14]. Patients become hesitant to seek care and attend follow-up appointments due to their mistrust of health providers [7, 8].
Until recently, the standard curricula of Ethiopia's recent medical schools did not include a medical ethics course. Nevertheless, following proposals from the Ethiopian Medical Association and curriculum review committees, the medical ethics course was first established at Addis Ababa University's Faculty of Medicine in 2004 [15]. Despite the existence of a medical ethics course, patients' concern about maintaining their confidentiality has grown, and reports of unethical behavior by health professionals on patient confidentiality are familiar [15].
There are so many problems regarding patient medical record confidentiality and data sharing [16]. The loss of patient medical records due to handling by unauthorized staff without consent and transporting to another department is a big issue in Ethiopia. That can affect patients’ quality of care by consuming time, harming patient satisfaction, causing improper diagnosis, and making it difficult to get the previous history.
The significance of this research is that it addresses the rapidly growing trend of patient data sharing and confidentiality among health practitioners in developing countries taking Ethiopia as an example. There is limited evidence regarding health professional knowledge and attitude related to patients’ confidentiality in resources limited settings. Therefore, this study will fill evidence gaps on health professional knowledge, attitude, and associated factors related to patient confidentiality in Ethiopia. This study will provide policymakers with up-to-date information on health professionals' knowledge and attitude towards patient confidentiality. Aside from that, the outcomes of this study may aid legislators in developing plans to improve health professionals' knowledge and attitude toward patient confidentiality.
Method
Study design and setting
An Institutional based cross-sectional study was conducted among health professionals from August–September 2021. Gondar is a historical town situated in the northwestern part of Ethiopia, 772 km far from the capital Addis Ababa and 168 km from Bahir Dar [17]. The University of Gondar specialized hospital is one of the largest teaching hospitals in the Amhara region providing tertiary level care for more than seven million people in the northwest part of the country coming from Amhara, Tigray, and Benishangul Gumuz regions [18]. It has 960 health professionals distributed over 30 services units responsible for delivering healthcare services to an average of 800 patients per day.
Study subjects and eligibility criteria
All healthcare professionals working in the University of Gondar specialized hospital and those available during the study period were the sources and study population. The study excluded health professionals with less than six months of experience, those who had not been found in the hospital for various reasons, and those on yearly leave during the data collection period.
Sample size determination and sampling procedure
The sample size was calculated using the single population proportion formula, n = Z(α/2)2 pq/d2 [19]. We assumed: n = the required sample size, Z = the value of standard normal distribution corresponding to α/2, 1.96, p = proportion of health professionals who had good knowledge and attitude towards confidentiality, q = proportion of health professionals who had unfavorable knowledge and attitude towards confidentiality, and d = precision assumed as 0.05. To our knowledge, no study has been conducted in Ethiopia to determine the knowledge and attitude of health professionals towards patient confidentiality. Therefore, we assumed p (proportion of health professionals who had good knowledge and attitude towards confidentiality) to be 0.5. Hence, the required sample size was calculated to be 384. After adding a 10% non-response rate, 423 health care professionals were enrolled in the study.
Stratified with a simple random sampling method was used to select the 423 participants. Firstly, the sample was stratified based on their department. Then the selection was proportionally allocated in each stratum depending on the numbers of healthcare providers in each stratum or department to assess their knowledge, attitude, and associated factors related to patients' confidentiality. After allocating samples in each stratum proportionally, a computer-generated simple random sampling technique was employed to select the study subjects in each department (Fig. 1).

Sampling procedure and sample allocation in University of Gondar hospital
Study variables
The primary outcome variable of this study was knowledge and attitude towards patient confidentiality. The questionnaires used in this study were developed based on a review of related literature [20, 21]. Socio-demographic and work-related characteristics were used as independent variables in this study.
Operational definitions
Knowledge about patients' confidentiality was assessed using seven items with “yes” and “no” responses. Each correct answer was equal to one point, while each incorrect answer was equal to zero points, with a height possible score of 7 for the knowledge part. A mean of 7 questions regarding Knowledge towards patient confidentiality was calculated. And those above the mean score were categorized as ‘good’ knowledge, and those below were categorized as ‘poor’ knowledge [20].
Attitudes toward patient confidentiality were assessed by using 14 questions with a 5 point Likert scale from ‘strongly disagree’ (score 1) to ‘strongly agree’ (score 5) [20]. The final score in the attitude section ranges from 14 to 70. A mean of the 14 questions of attitude towards patient’s confidentiality was calculated. Those above the mean value were categorized as ‘favorable’ attitude, and those below the mean value were categorized as ‘unfavorable’ attitude [20].
Data collection tool and quality control
A self-administered, organized, and pre-tested questionnaire was created in English. The data collection process included two supervisors and ten data collectors. One-day training was given to the data collectors to eliminate ambiguities. A pre-test was conducted outside of the study area, in Gondar town health centers, with 10% of the study population. The validity and reliability of the data collection instrument were assessed using the pre-test results. The Cronbach alpha value for the attitude questions was 0.82, whereas the Cronbach alpha value for the knowledge questions was 0.76. These figures show that the questionnaire is highly reliable.
Data processing and analysis
The data entry was performed using Epi Data version 4.6 software packages and analyzed using Statistical Package for Social Sciences (SPSS) version 25. Descriptive statistics were computed to describe the socio-demographic variables and health professionals’ knowledge and attitudes about patient confidentiality and data sharing. Bi-variable and multivariable binary logistic regression analyses were done to measure the association between the dependent and independent variables. In the bi-variable regression analysis, variables with a p value of less than 0.2 were included in the multivariable regression analysis to assess their adjusted impacts on the dependent variables. Odds ratio with 95% confidence level and P value were calculated to ascertain the strength of association and to decide statistical significance. For all significantly associated variables, the cut-off value was p < 0.05. Before conducting the logistic regression model, assumptions of multi-collinearity were checked. The result revealed all the variance inflation factor (VIF) values less than three, which confirmed the absence of multi-collinearity.
Result
Description of participant’s socio-demographic and work-related characteristics
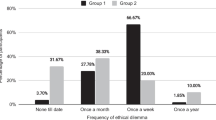
Of 423 participants, 410 responded to a questionnaire with a 96.9% response rate. The mean age of the participants was 28.12(SD ± 5.16) years which ranges from 21 to 50 years. The majority 271(66.1%) of the study participants were male and most of them 334 (81.5%) were orthodox religious followers. In terms of the educational level of the health professional, more than half 228 (55.6%) of participants have a BSc degree (Table 1). Of the total respondents, above three fourth 79.8% health professionals had below five years of work experience. A majority 47.8% of respondents were nurse professionals. Almost all 95.4% health professionals had direct contact with the patients and around 39% had visits above 40 patients per day. The results showed that about 5.9% of health professionals faced more than two ethical dilemmas daily while treating patients. In addition, 44.1% of the participants were taking training on medical ethics (Table 1).
Health professionals’ knowledge about patients’ confidentiality
Of the total participants, 59.8% with [95% CI (54.9–64.5%)] had good knowledge about confidentiality with a mean score of 3.91(SD ± 1.39) (out of a maximum of 7 points) (Fig. 2). From the knowledge questionnaire, most of the respondents 358(87.3%) were said ‘access to medical records should be governed by law’ and 183(44.6%) argued that non-medical information is also confidential. Furthermore, 291(71%) health professionals were aware that third-party insurance companies did not access patient examination results (such as insurance companies) without patient consent. However, only 115(28.0%) of participants knew that policies were not allowed to access medical records freely (Table 2).

Health professional knowledge and attitude related to patients’ confidentiality
Health professionals attitude towards patients’ confidentiality
Of the total participants, 49.5% with [95% CI (44.6–54.3%)] had a favorable attitude towards confidentiality with a mean score of 42.8(SD ± 8.90) (out of a maximum of 70 points) (Fig. 2). Table 3 illustrates that about 126(30.7%) of participants agreed that confidentiality affects the patient in any way, and 299(72.9%) believed they don’t allow non-medical personnel to enter the examination room while they are discussing with patients. Of all respondents, 220(53.7%) and 162(39.5%) participants use lock systems and computers to store patient information.
Factors associated with health professionals’ knowledge about patients’ confidentiality
Bi-variable and multivariable binary logistic regression analyses were done to measure the association between Health professionals’ knowledge towards patients’ confidentiality and independent variables. In bi-variable regression, Sex of participants, Age of the respondents, Work experience, Training on medical ethics, Numbers of the patient served, Direct contact with the patients, Numbers of ethical dilemmas faced, Income of participants were the candidates’ variables for health professionals’ knowledge towards confidentiality for the multivariable regression analysis (P < 0.2). With the multivariable regression model sex of respondents, training on medical ethics, number of ethical dilemmas faced were significantly associated factors for health professional knowledge towards patients’ confidentiality (Table 4). This means that being male was (AOR = 1.63, 95% CI [1.03–2.59]) times more likely to have good knowledge towards patient confidentiality as compared to females after controlling for other factors. Health professionals taking training on medical ethics were (AOR = 1.73, 95% CI = [1.11–2.70]) times more likely to have a good knowledge towards patients’ confidentiality as compared to their counterparts. Similarly, health professionals who faced more ethical dilemmas were (AOR = 3.07, 95% CI [1.07–8.79]) times more likely to have good knowledge than those who faced fewer ethical dilemmas.
Factors associated with health professionals’ attitude towards patients’ confidentiality
In both bi-variable and multivariable analysis training on medical ethics, direct contact with the patients, Numbers of patient visits, and numbers of ethical dilemmas faced were significant variables to the attitude of health professionals towards patient confidentiality (Table 5).
Health professionals taking on medical ethics were (AOR = 2.30, 95% CI [1.42–3.72]) times more likely to have a favorable attitude towards patient confidentiality when compared to those who didn’t take any pieces of training on medical ethics. Health professionals who had direct contact with the patients were (AOR = 3.06, 95% CI [1.12–8.34]) times more likely to have a favorable attitude towards patient confidentiality than those who didn’t have direct contact with the patients. Health professionals who visited more patients daily (more than 40 and 30–40) were approximately (AOR = 4.38, 95% CI [2.46–7.80]) and (AOR = 1.96, 95% CI [1.12–3.43]) times more likely to have a favorable attitude towards patients’ confidentiality when compared to those who visited less than 30 patients daily. Additionally, respondents who faced more ethical dilemmas were (AOR = 3.56, 95% CI [1.23–10.26]) times more likely to have a favorable attitude towards patients’ confidentiality than those who faced fewer ethical dilemmas.
Discussion
This study examines health professionals’ knowledge and attitude towards patient confidentiality and associated factors in Northwest Ethiopia.
This study revealed that around 59.8% of respondents had good knowledge related to patient confidentiality. The finding is in line with two studies conducted in Iran 56.6% [22], 63% [23]. However, the results of this study demonstrated that health professionals’ good knowledge towards patient confidentiality was lower than studies conducted in Spain 68% [24] and Tehran university medical school 65% [25]. The difference could be that health professionals working in high-resource countries are more informed about patients' privacy in their daily lives and recognize the relative benefit of patient confidentiality [26]. The other reasons for the disparity could be explained by the fact that approximately 75% of participants had less than 5 years of professional experience in the current study, and they were also considerably younger than in the Spanish study [24]. Furthermore, the participants in Spain were all physicians, who are supposed to have better clinical data management and specific training [24].
In this study, 49.5% of participants had a favorable attitude towards patient confidentiality. This finding is supported by the study conducted in northern Jordan 52.4% [20]. However, this finding is lower than the study conducted in Turkey (64.4%) physicians strongly agreed to protect patient confidentiality [27]. The possible reason could be that difference awareness among health professionals in different countries results in a good level of attitude.
The study also found factors associated with health professionals’ knowledge and attitude regarding patient confidentiality. The sex of respondents, training on medical ethics, and the number of ethical dilemmas faced was all significantly associated factors of health professional knowledge towards patients’ confidentiality. Likewise, training on medical ethics, direct contact with the patients, Numbers of patient visits, and numbers of ethical dilemmas faced were significant variables to the attitude of health professionals towards patient confidentiality.
Among the factors associated with knowledge, being males were more likely to have good knowledge towards patient confidentiality than females. This finding is consistent with study findings from Jordan [20, 21], Spain [24], and the United States [28]. This might be due to males were more access to information and technology and there is high information sharing between them [21]. Furthermore, the number of ethical dilemmas experienced and training on medical ethics were revealed to be predictive variables for both knowledge and attitude. Health professionals taking training on medical ethics were more likely to have a good knowledge and attitude related to patients’ confidentiality than those who had not taken the training. The greatest strategy to ensure adherence to confidentiality laws was to provide training on medical ethics, where health organizations would routinely update all health professionals on guidelines and strategies to prevent sensitive information disclosure [21, 29, 30]. Furthermore, the legislature's role is critical, not just in terms of legal norms to safeguard patient confidentiality, but also in terms of punishments when inappropriate behavior occurs [31]. And this finding is supported by a study conducted in Barbados [32], Vietnam [33]. Besides this, this study also found that health professionals who faced more ethical dilemmas were more likely to have good knowledge and attitude as compared to those who faced a less ethical dilemma. According to Hariharan et al. suggestions, health professionals may not report such problems to their seniors and try to solve them [32]. This may be the possible reasons for facing more ethical dilemma and trying to solve by themselves to have positive knowledge and attitude towards patient confidentiality.
In addition, direct contact with the patients and the number of patient visits were associated with a favorable attitude towards patient confidentiality. Respondents who have direct contact with the patients were more aware of confidentiality. This could be because the health of practitioners that deal with patients regularly are more familiar with confidentiality rules and strategies[22]. Besides this, health professionals who visit more patients per day were more likely to have a favorable attitude related to patient confidentiality. This might be because when health professionals serve more patients per day, they get a lot of challenges which helps to change their attitude to maintain the patient's information confidentially.
Conclusion
The findings of this study revealed that health professionals have a limited attitude towards patient confidentiality but have relatively good knowledge. The sex of respondents, training on medical ethics, and many ethical dilemmas faced were significantly associated factors of health professional knowledge towards patients’ confidentiality. Likewise, training on medical ethics, direct contact with the patients, Numbers of patient visits, and numbers of ethical dilemmas faced were significant variables to the attitude of health professionals towards patient confidentiality. Providing a continuing medical ethics training package for health workers before joining the hospital and in between the working time could be recommended to improve health professionals' knowledge and attitude towards patient confidentiality.
Strength and limitations
The findings from this study provide valuable information on health professionals' knowledge and attitude related to patients' confidentiality in resources limited countries. There are some limitations to this study. First, this study was an institution-based cross-sectional survey; only health professionals who came during the data collection period were interviewed.
Availability of data and materials
All the data generated or analyzed during this study are included in this published article and supplementary information [SPSS Data Knowledge and SPSS Data Attitude].
Abbreviations
- AOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- Epi-info:
-
Epidemiological information
- ICT:
-
Information communication technology
- SPSS:
-
Statistical package for social science
References
de Sousa Costa R, de Castro Ruivo I, editors. Preliminary remarks and practical insights on how the whistleblower protection directive adopts the GDPR principles. Annual Privacy Forum; 2020. Springer.
Štarchoň P, Pikulík T. GDPR principles in data protection encourage pseudonymization through most popular and full-personalized devices-mobile phones. Procedia Comput Sci. 2019;151:303–12.
Drogin EY. Confidentiality, privilege, and privacy. 2019.
Romeo C. Enciclopedia de Bioderecho y Bioética. Cuad Med Forense. 2012;18(3–4):144–5.
Beltran-Aroca CM, Girela-Lopez E, Collazo-Chao E, Montero-Pérez-Barquero M, Muñoz-Villanueva MC. Confidentiality breaches in clinical practice: what happens in hospitals? BMC Med Ethics. 2016;17(1):1–12.
Parsa M. Privacy and confidentiality in medical field and its various aspects. J Med Ethics Hist. 2009;4:1–14.
Spencer A, Patel S. Applying the data protection act 2018 and general data protection regulation principles in healthcare settings. Nurs Manag. 2019;26(1):34.
Act DP. Data protection act. London Station Off. 2018;5.
Yilma DKM. Privacy and personal data protection in Africa A rights-based survey of legislationin eight countries 2020 [cited 2021 January 23]. https://www.apc.org/sites/default/files/PrivacyDataProtectionAfrica_CountryReports.pdf.
Organization Wh. Policy - Food, Medicine and Health Care Administration and Control Council of Ministers Regulation (Regulation No. 299/2013) 2014 [cited 2022 January 23]. https://extranet.who.int/nutrition/gina/en/node/26274.
Adeleke I, Adekanye A, Adefemi S, Onawola K, Okuku A, Sheshi E, et al. Knowledge, attitude and practice of confidentiality of patients’ health records among health care professional at federal medical centre. Bida Niger J Med. 2011;20(2):228–35.
Cas G, Aji G. Analysis of the ethical aspects of professional confidentiality in dental practice. Br Dent J. 2008;205(5):257.
Blightman K, Griffiths S, Danbury C. Patient confidentiality: When can a breach be justified? Contin Educ Anaesth Critical Care Pain. 2014;14(2):52–6.
Bartlett YK, Coulson NS. An investigation into the empowerment effects of using online support groups and how this affects health professional/patient communication. Patient Educ Couns. 2011;83(1):113–9.
(EMA) EMA. medical ethics for doctorsin Ethiopia 2010 [cited 2022 January 23]. http://www.ethiopianorthopaedics-esot.org/index.php/ethics/send/4-ethics/8-ethics-code.
Ayalew NA. Duty of confidentiality in arbitration process in Ethiopia. Int J Soc Sci Econ Rev. 2019;1:92–100.
Wikipedia. Gondar 2020 [cited 2021 October 16]. https://en.wikipedia.org/wiki/Gondar.
Abdella NM, Tefera MA, Eredie AE, Landers TF, Malefia YD, Alene KA. Hand hygiene compliance and associated factors among health care providers in Gondar University Hospital, Gondar, North West Ethiopia. BMC Public Health. 2014;14(1):1–7.
Naing L, Winn T, Rusli B. Practical issues in calculating the sample size for prevalence studies. Arch Orofac Sci. 2006;1:9–14.
Karasneh R, Al-Mistarehi A-H, Al-Azzam S, Abuhammad S, Muflih SM, Hawamdeh S, et al. Physicians’ knowledge, perceptions, and attitudes related to patient confidentiality and data sharing. Int J General Med. 2021;14:721.
Abuhammad S, Alzoubi KH, Al-Azzam SI, Karasneh RA. Knowledge and practice of patients’ data sharing and confidentiality among nurses in Jordan. J Multidiscip Healthc. 2020;13:935.
Hosseini-Ghavam-Abad L, Asghari F, Bandehagh A, Najafipour S, Bigdeli S. Patient privacy: awareness and attitudes of Iran University of Medical Sciences medical students. Med J Islam Repub Iran. 2019;33:12.
Rangrazr F, Rabie R. Evaluation of patients’ rights in public hospitals in Kashan in 2002. J Kermanshah Uni Med Sci. 2005;1(9):62–71.
Beltran-Aroca CM, Labella F, Font-Ugalde P, Girela-Lopez E. Assessment of doctors’ knowledge and attitudes towards confidentiality in hospital care. Sci Eng Ethics. 2019;25(5):1531–48.
Sheikh-Taheri AK, BaratiMarnani KA. Knowledge of physicians, nurses and staff of medical records of the legal aspects of medical records in hospitals affiliated to Tehran University of Medical Sciences. Health Inf Manag. 2010;89(7):136–46.
Privacy_International. Medical privacy and security in developing countries and emergency situations 2012 [cited 2022 January 25]. https://privacyinternational.org/report/726/medical-privacy-and-security-developing-countries-and-emergency-situations.
Demirsoy N, Kirimlioglu N. Protection of privacy and confidentiality as a patient right: physicians’ and nurses’ viewpoints. Biomed Res. 2016;27(4):1437–48.
Wandrowski J, Schuster T, Strube W, Steger F. Medizinethische Kenntnisse und moralische Positionen von Ärztinnen und Ärzten aus Bayern. Dtsch Ärztebl. 2012;109(8):141–7.
Noor MM, Hassan WH. Wireless networks: developments, threats and countermeasures. Int J Dig Inf Wirel Commun (IJDIWC). 2013;3(1):125–40.
Nejad EM, Begjani J, Abotalebi G, Salari A, Ehsani SR. Nurses awareness of patients rights in a teaching hospital. J Med Ethics History Med. 2011;4:2.
Veerus P, Lexchin J, Hemminki E. Legislative regulation and ethical governance of medical research in different European Union countries. J Med Ethics. 2014;40(6):409–13.
Hariharan S, Jonnalagadda R, Walrond E, Moseley H. Knowledge, attitudes and practice of healthcare ethics and law among doctors and nurses in Barbados. BMC Med Ethics. 2006;7(1):1–9.
Khac Hai N, Lawpoolsri S, Jittamala P, Thi Thu Huong P, Kaewkungwal J. Practices in security and confidentiality of HIV/AIDS patients’ information: a national survey among staff at HIV outpatient clinics in Vietnam. PLoS ONE. 2017;12(11):e0188160.
Acknowledgements
We are very grateful to the University of Gondar, Institute of Public Health for providing this opportunity to conduct the research. Our acknowledgment also extends to the managing board of the University of Gondar specialized hospital for giving all the necessary information and support. We also forward our thanks to the study participants, data collectors, and supervisors.
Funding
Funding was not granted.
Author information
Authors and Affiliations
Contributions
MDT made significant contributions in conception, design, data collection supervision, data analysis, interpretation, and manuscript write-up. MSM & AFC have contributed extensively to revising the manuscript, analysis, and interpretation. AWS, DDH, MGL, TAE, ND, WZ, and TZ have drafted proposals, analyses, and interpretation. All authors have approved the final version of this manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We confirm that all procedures utilized in this study were conducted following the principles of the Helsinki Declaration. Ethical clearance and approval letters were secured from the Institutional Review Board (IRB) of the University of Gondar (Reference number H/I/D 656/9/21). Written consent was obtained from each health professional after telling the objective of the study. A supporting letter was also obtained from the University of Gondar hospital. During the data collection, the issue of confidentiality and privacy was assured by maintaining the anonymity of participants. Health professionals were voluntary, and participants could withdraw from the study at any time if they were not happy with the survey.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary SPSS data on Knowledge of Patient Confidentiality.
Additional file 2:
Supplementary SPSS data on attitude towards Patient Confidentiality.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tegegne, M.D., Melaku, M.S., Shimie, A.W. et al. Health professionals' knowledge and attitude towards patient confidentiality and associated factors in a resource-limited setting: a cross-sectional study. BMC Med Ethics 23, 26 (2022). https://doi.org/10.1186/s12910-022-00765-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12910-022-00765-0