
Abstract
Background
Telemedicine includes the delivery of health-care services and sharing of health information across distances. Past research has found that telemedicine can play a role in enhancing complementary, alternative, and integrative medicine (CAIM) while allowing the maintenance of cultural values and ancestral knowledge. This scoping review synthesized evidence regarding the use of telemedicine in the context of CAIM.
Methods
Following Arksey and O’Malley’s scoping review framework, CINAHL, PsycINFO, MEDLINE, EMBASE and AMED databases were searched systematically. The CADTH website was also searched for grey literature. Eligible articles included a CAIM practice or therapy offered through telemedicine, with no restrictions placed on the type of telemedicine technology used. Inductive thematic analysis was conducted to synthesise common themes among the included studies.
Results
Sixty-two articles were included in this synthesis. The following themes emerged: 1) the practitioner view of CAIM delivered through telemedicine, 2) the patient view of CAIM delivered through telemedicine, and 3) the technological impacts of telemedicine delivery of CAIM.
Conclusions
Studies have shown that telemedicine delivery of CAIM is feasible, acceptable, and results in positive health outcomes. Some barriers remain such as the presence of chronic illness and morbidity, inability to form strong patient-provider relationships relative to face-to-face approaches, and technological difficulties. Future intervention research should focus on reducing such barriers, as well as explore which patient population would realize the greatest benefit from CAIM delivered via telemedicine, and the impact of interventions on providers and caregivers.
Similar content being viewed by others


Background
Telemedicine is used today as an umbrella term encompassing the delivery of health-care services and the exchange of health-care information across distances, with the help of a wide variety of technology [1, 2]. The word telemedicine has been supplemented by terms such as telehealth, online health, and more recently, e-Health [1]. It is widely recognized that there is no single, definitive definition of telemedicine [3]. However, the World Health Organization describes telemedicine as: “the delivery of healthcare services by healthcare professionals over a distance involving the exchange of information related to diagnosis, treatment and prevention of diseases and injuries, research and evaluation, and for continuing the education of healthcare providers, all with the goal of advancing health and the healthcare system” [4].
While technology continues to advance, infrastructure and legal barriers remain within the field of telemedicine [5]. Despite these barriers, the implementation of telemedicine measures remains promising with the potential to significantly reduce healthcare expenditures, especially in rural or remote areas such as Northern Canada where the cost of healthcare prevails [6]. Past research has found that telemedicine can also play a role in enhancing complementary, alternative, and integrative medicine (CAIM), allowing the maintenance of cultural values and ancestral knowledge [7]. However, more research is warranted to understand the use and impacts of telemedicine for CAIM.
CAIM is typically described as therapies used together (complementary), in replacement (alternative) of conventional Western medicine, or as the combining of both conventional and unconventional therapies in a coordinated way (integrative) [8, 9]. CAIMs encompass a broad range of approaches that commonly include natural products (e.g., vitamins, herbs, probiotics), mind and body practices (e.g., yoga), and traditional forms of medicine (e.g., traditional Chinese medicine) [9]. The use of telemedicine for the delivery of CAIM holds unique potential to increase access to CAIM practices for those living in remote areas or with accessibility challenges. Greater accessibility to CAIMs through telemedicine may potentially improve clinical outcomes, decrease patient healthcare utilisation, and enhance patient satisfaction with mental health and chronic disease management [10, 11]. The continued use of CAIM in treatment plans, and the growing use of telemedicine as an avenue to extend healthcare, particularly for remote and rural communities, justifies the need to investigate how telemedicine is used in the context of CAIM. Thus, the purpose of this scoping review is to understand the breadth of the literature regarding telemedicine used in the context of CAIM, to inform future areas of investigation and practice.
Methods
This review was conducted to understand how telemedicine is used in the context of CAIM. Arksey and O’Malley’s five-stage scoping review framework [12] was utilised and also supplemented with additional scoping review guides [13,14,15]. The five steps were as follows: 1) identify the research question, 2) identify the relevant studies, 3) select relevant studies, 4) chart data, and 5) collate, summarise, and report the results.
Step 1: Identify the research question
The research question for this scoping review was as follows: “How is telemedicine used in the context of CAIM?” For the purposes of this review, telemedicine was defined based on recent, well-cited review articles, as the application of any online or digital service such as Facebook live groups, Twitter, phone, mobile application, and websites, to enhance health-care management [16,17,18]. CAIM was defined using the operational definition provided by the Cochrane Complementary Medicine group, which included a list of therapies that were classified as complementary, alternative, or integrative medicines [19, 20]. All CAIMs discussed met the Cochrane Complementary Medicine group’s definition. In this review, all included studies contained at least one type of telemedicine being used for at least one type of CAIM.
Step 2: Finding relevant studies
A preliminary scan of the literature indicated that academic literature on this subject area was sparse. We devised a systematic search strategy as shown in Table 1. CINAHL, PsycINFO, MEDLINE, EMBASE and AMED databases were searched on October 12, 2020. The CADTH website was used to search for grey literature, and was also searched on the same day [21]. Primary research articles were considered, and relevant reviews were used to source additional eligible primary research articles.
Step 3: Selecting the studies
Records were included if they mentioned CAIM and telemedicine, with no restrictions placed on the type of telemedicine strategy. Records were excluded if they were 1) non-academic or non-scholarly sources (e.g., websites, blogs, news articles), 2) found outside of bibliographic database searches (e.g., unpublished theses and dissertations), or 3) conference abstracts. Only articles published in English were included. Three authors (NN, AM, CH) first pilot-screened titles and abstracts independently and in duplicate, and then met to verify the appropriateness of the inclusion criteria. Next, the three authors completed independent screening of articles for eligibility by title and abstract, and full text. Disagreements were resolved with discussion with the senior author (JYN) and in the case that consensus was not reached, eligibility was determined based on majority vote.
Step 4: Charting the data
Articles that met inclusion criteria were critically reviewed using Arksey and O’Malley’s descriptive-analytical narrative method [12]. The following information was extracted by three authors (NN, AM, CH): title, author, year, country, study setting, study design, population type and sample size, type of CAIM used, type of telemedicine used, primary and secondary outcomes and how they were measured, main findings, challenges encountered, and conclusions. Authors then met to resolve any data discrepancies. Later, four authors (AQS, NR, RCS, ZK) reviewed the data extraction as a quality measure.
Step 5: Collating, summarising and reporting results
Charted data was summarized in table format, and thematic and descriptive data was analysed (NN, AM, CH). A thematic analysis was conducted to present a narrative related to the research question and highlight knowledge gaps in the current literature (AQS, NR, RCS, ZK). Themes were discussed in consultation with NN and JYN, who have prior experience in conducting thematic analyses.
Results
Search results
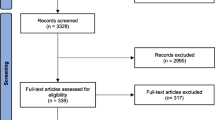
Searches identified a total of 1797 records, of which 1602 were unique. A total of 1402 titles and abstracts were eliminated, leaving 200 full-text articles to be considered. Of these, 138 were ineligible for the following reasons: did not include a CAIM (n = 58) or did not include telemedicine (n = 15), review (n = 44), research protocol (n = 9), conference abstract (n = 5), case study (n = 5), commentary (n = 1), or letter to editor (n = 1), leaving a total of 62 eligible studies which are included in this scoping review. A breakdown of study filtration through the inclusion exclusion process can be found in Fig. 1.

PRISMA diagram displaying the search strategy and selection process [22]
Eligible article characteristics
Eligible articles were published from 1999 to 2020, and originated from the United States (n = 34), Italy (n = 4), the United Kingdom (n = 3), South Korea (n = 3), Canada (n = 2), China (n = 2), Norway (n = 2), Taiwan (n = 2), Australia (n = 2), France (n = 1), Germany (n = 2), Iceland (n = 1), Israel (n = 1), and Switzerland (n = 1). One article included participants from both the US and the UK [23], and another study included collaboration between Austria and China [24]. Of the 62 articles included, all were primary research articles focused on, development of a telemedicine technology or processes for CAIM (n = 11), analysis of the data collected by a telemedicine technology for CAIM (n = 26) and/or, analysis of usability, acceptability, or feasibility of existing telemedicine software (n = 25). The characteristics of all eligible articles can be found in Tables 2, 3, and 4.
CAIM characteristics
Of the 62 articles included, the distribution of CAIMs discussed were as follows: mindfulness training (n = 11), mind–body exercise (n = 7), yoga (n = 7), biofeedback (n = 4), music therapy (n = 4), spiritual care (n = 4), dance therapy (n = 3), cannabis (n = 3), chiropractic manipulation (n = 2), guided imagery (n = 2), hypnosis (n = 2), ketogenic diet (n = 2), acupuncture (n = 1), auricular acupressure (n = 1), Chinese medicine (n = 1), exercise (n = 1), qigong (n = 1), herbal medicine (n = 1), meditation (n = 1), Mediterranean diet (n = 1), play-based therapy (n = 1), and vitamin B weight loss (n = 1).
Telemedicine characteristics
Of the 62 articles included, the telemedicine tools used were as follows: videoconferencing (n = 16), mobile application (n = 7), web- or mobile-based application (n = 2), videos (n = 10), websites (n = 7), telephone (n = 7), database/cloud system (n = 1), telemedicine centre (n = 1), teleconference (n = 1), telephone and video (n = 1), e-mail (n = 1), remote tele-biofeedback (n = 1), social media platform (n = 1), telephone and portable electromyograph (n = 1), videos and chat group (n = 1), text messaging (n = 1), telephone and videoconferencing (n = 1), telephone and mp3 audio (n = 1), and website and videoconferencing (n = 1).
Findings from thematic analysis
In total, three main themes emerged from our analysis and are described below.
Theme 1: Practitioner view of CAIM telemedicine
Feasibility of CAIM telemedicine interventions
Overall, practitioners found it feasible to deliver traditionally in-person CAIM interventions through a telemedicine approach (n = 26) [24, 25, 27, 31,32,33,34,35, 38,39,40, 42, 43, 51, 52, 54, 55, 58,59,60, 63, 68, 69, 71, 72, 74, 76, 80, 83, 85]. Sufficient technology exists to meet the delivery needs of a great number of heterogeneous CAIM interventions. For example, Skype as a videoconferencing platform could be effectively used for hypnotherapy [42], but also for mind–body therapy [80]. Other technologies such as telephones, internet websites, smartphone applications, virtual-reality technology, and even specialized cloud platforms were successfully tailored to the goals of particular CAIM interventions and targeted towards a diverse range of patient populations including older adults [27]. Practitioners found it feasible to implement physical activities such as dance and yoga virtually [25, 59, 68], but also found it was possible to administer more complex CAIM interventions such as hypnosis therapy, or the virtual management and treatment of patients with COVID-19 [51, 71].
The feasibility of the intervention itself was comparable, and in some cases, superior to in-person delivery. One study found that interest in participation and feasibility of a Skype mind–body therapy was superior compared to an in-person pilot test of the same intervention [43], while another study found increased scheduling flexibility and subsequently, greater participation in the telemedicine intervention compared to in-person care delivery [80]. Telemedicine approaches to CAIM were also more inclusive for participants who would usually have been unable to participate due to cost barriers, or travel difficulties such as urinary incontinence [42].
High acceptability and satisfaction of CAIM telemedicine interventions
Practitioners readily accepted and reported favourable attitudes towards telemedicine approaches to CAIM (n = 21) [23, 39, 41, 45, 46, 50,51,52,53,54,55,56,57, 61, 63,64,65,66, 68, 70, 73]. Practitioners did not have major concerns regarding ease of use, appeal to target population, or efficacy of telemedicine CAIM interventions. This held true across the various populations included in this review. For example, clinicians in a cannabis reduction intervention did not have concerns about confidentiality, or application of mobile device technology [70]. Another telephone-adapted delivery format for a mindfulness-based stress reduction was perceived by practitioners as “very positive” [63]. In a dance-therapy session for older adults, student nurse leaders expressed high interest and enjoyment in intervention delivery among study participants [52]. Moreover, practitioners involved with a study by Green et al. [39] found that telehealth enabled continuity of care with patients and was therefore a “valuable” tool.
A common view was that telemedicine is valuable to improve the efficiency of medical resource use, through reducing wait times for patients [51], improving hospital-bed shortage problems [51], and reducing the workload burden of healthcare staff [45, 46, 50, 73]. Practitioners were also satisfied with the potential to lower healthcare delivery costs [46, 55, 57, 63, 66, 73], in one case by up to 75% [63]. Practitioners believed telemedicine delivery of CAIM had a high potential for wider scalability in the healthcare system [63, 64, 66, 73]. Although, some studies expressed barriers such as a lack of a tailored approach to goal setting in an internet-based workplace intervention promoting a Mediterranean diet [61], and poor software and hardware usability of an electromyographic audio biofeedback program for telerehabilitation [65].
Health and well-being improvements
Practitioners found that CAIM interventions delivered using telemedicine resulted in health and well-being improvements across a variety of patient populations, comparable to improvements observed in in-person delivery modes (n = 35) [23, 24, 27,28,29, 31, 33, 36,37,38, 40, 41, 43, 45, 47,48,49,50, 55, 58, 64, 66,67,68,69, 72, 74,75,76,77,78, 80,81,82, 84]. This applied not only to physical patient health [77], but also to quality of life [76], mental [31, 40, 43, 75] and spiritual [64] health, and aspects of personality such as self-concept and self-esteem [64]. The improvement in health was observed across all age groups, from children and adolescents [64], to older adults [67]. Moreover, the improvements to health manifested across a diverse range of patient groups, including veterans, cancer patients, and individuals with chronic illness. Many of these changes were clinically meaningful, having positively impacted the course of the illness or resulted in visible improvements from the perspective of both patients and clinicians [64, 66, 67]. Positive health changes often persisted longitudinally at various follow-up periods, indicating that telemedicine interventions can produce persistent health benefits [28, 43, 48,49,50, 57, 58, 62, 64, 68, 74, 75, 80, 81]. In some cases, health benefits did not remain at follow-up [29], or longitudinal assessment was not reported.
Theme 2: Patient view of CAIM telemedicine
The patient-practitioner relationship
Patients felt it was challenging to form meaningful connections with CAIM practitioners employing telemedicine alternatives (n = 10) [23, 25, 26, 32, 33, 44, 47, 52, 71, 78, 79]. Study participants reported a lack of understanding of the role of the practitioner, difficulty following along with remote-based interventions, and lack of sufficient feedback on their performance from practitioners. For example, participants involved in yoga interventions through video-conferencing technologies identified challenges such as having to continuously “readjust screens,” difficulty “learning and doing poses simultaneously,” a lack of instructor feedback in real-time, and an inability to “bond” with the instructor [25, 47, 78]. In telephone-based coaching interventions, participants seemed to be unclear of the role of coaches, and found it “difficult to develop a relationship with or trust a stranger on the phone” [26, 44]. Furthermore, according to participants, CAIM interventionists may misinterpret their needs particularly when employing audio-visual or phone-based telemedicine technology [25, 26, 29, 41, 47, 67, 71, 78, 85], for reasons such as being unable to perceive “subtle expressions” of interest, emotion, or physical comfort [25], or as a consequence of ineffective communication between practitioners and participants through digital platforms [47, 78].
The impact of existing chronic health conditions and morbidities on intervention outcomes
Complex or chronic conditions, as well as multimorbidity, was found to negatively impact participation, patient safety, or retention of patients in CAIM interventions delivered through telemedicine (n = 12) [23, 25, 32,33,34, 37, 43, 47, 52, 55, 63, 69]. In particular, the presence of these types of health conditions were associated with various functional and mobility limitations such as breathing problems and fatigue, which served as a barrier to participation [23, 47, 63]. For example, some individuals with cancer found it difficult to participate in virtual yoga training due to “[cancer] treatment-related fatigue,” and cancer-related overwhelmingness and forgetfulness [25]. Individuals with chronic pain found that their condition interfered with their ability to attend virtual mindfulness-based classes as part of an intervention [37]. However, this issue was acknowledged and the program was lengthened to suit their needs [37]. Other studies noted that attrition was often due to deteriorating health, or health-related responsibilities (e.g., surgery) [33, 43, 55, 63].
The benefit of telemedicine delivery of CAIM for traditionally underserved populations
Participants most frequently cited CAIM interventions administered through a telemedicine approach as an accessible alternative to in-person care, that leads to improved health outcomes without any salient consequences (n = 21) [25, 27, 28, 30, 32, 37,38,39, 42, 45,46,47, 51, 55, 57, 63, 69,70,71, 74, 76]. Virtual care delivery appeared to expand access to care particularly for rural populations [74], or those with chronic health conditions that prevented them from travelling long distances. Many of the included studies also engaged populations that are often neglected such as racial or ethnic minorities [26, 60], or women veterans [74]. Evaluations and feedback were overwhelmingly positive and in support of these health interventions, noting improved accessibility in receiving CAIM in the comfort of their own homes [32, 43]. Previously identified barriers to participation such as high travel costs [28, 32, 42, 45, 63], inability to travel [28, 42, 63, 69], time conflicts [28, 30, 63], and reluctance to participate in a group or associate with other frail individuals [27], among others, were overcome.
Theme 3: The technological impacts of CAIM via telemedicine
Overall, technological issues did not appear to impede the success of CAIM delivered via telemedicine. However, some participants did believe that technological difficulties were a hindrance. Broadly, issues included degradation of audio and visual quality, limited access to the necessary devices, complex user interface in applications, and troubles with downloading CAIM intervention content, which are all necessary components in successful telecommunication delivery of CAIM (n = 14) [23, 25,26,27, 29, 30, 32, 33, 42, 43, 46, 47, 54, 72]. For example, an unstable internet connection, especially in rural areas, made it difficult to attend or follow along during CAIM sessions [23, 72]. Even when participants did connect to the telemedicine platform being used, freezing of the video stream or inconsistent audio made it difficult to engage and maximally benefit from the intervention [23, 32, 54]. Consequently, some participants believed the technological difficulties prevented them from gaining the “full benefit of the teacher’s feedback and interaction” [33]. In some cases, the technological difficulty meant that the therapeutic session had to be rescheduled [32]. Other types of technological barriers included font and video screen sizes in a mobile app study [30]. In contrast, practitioners did not generally find that technological difficulties were a significant barrier to the feasibility of intervention delivery, reporting that issues were infrequent [29, 32, 63, 74], and quickly and easily resolved when they did occur [25].
Discussion
The purpose of this review was to synthesize the literature on telemedicine utilised in the context of CAIM. To our knowledge, this is the first study to explore this field using a systematic search of peer-reviewed and grey literature to inform practice and future areas of research. Overall, CAIM interventions offered through telemedicine approaches are comparable to face-to-face interventions across dimensions of feasibility, clinical efficacy, and patient and provider satisfaction. The presence of complex or chronic health conditions such as cancer, as well as technological difficulties were reported as barriers to patient participation and satisfaction.
The results of our study reveal that telemedicine strategies to deliver CAIM are diverse, including videoconferencing, telephone, mobile applications, email, and cloud platforms. There is also great heterogeneity in the target populations of these interventions. This aligns with previous findings that telemedicine approaches can be effective for populations with diverse physical, mental, and emotional health-care needs [86,87,88].
Both practitioners and patients overwhelmingly found that telemedicine delivery of CAIM was feasible and acceptable. Practitioners perceived telemedicine as a valuable, cost-effective tool with potential for wider scalability [31, 43, 47, 55]. Furthermore, statistically significant, and clinically meaningful improvements in health outcomes were noted by both patients and practitioners. This reflects evidence telemedicine is found to comparable to face-to-face care in terms of feasibility and clinical-effectiveness [85, 89,90,91,92]. Practitioners also cite time savings after implementing telemedicine, due to a reduction in “downtime and inefficiencies” [93]. For many families, telemedicine delivery reduced cost and transportation barriers, increasing access to care. A recent review indicates that telemedicine advancements have improved access to care for a wide range of clinical conditions, and has addressed geographical barriers to care, although social barriers still lack attention [94].
Both patients and providers appear to be highly satisfied with telemedicine delivery of CAIM, citing that technical difficulties that arose in the intervention delivery were quickly and easily resolved. However, more patients noted technological difficulties that interfered with their participation and satisfaction with the intervention relative to providers delivering the intervention. This is in contrast to the literature where patients typically report high satisfaction with telemedicine approaches [95, 96]. One aspect of technological difficulties included a lack of access to the internet or telecommunication devices. This necessitates education to guide patients that may be unfamiliar about the use of various internet and mobile technologies (e.g., videoconferencing platforms, mobile applications), and its benefits in promoting health and well-being [97]. Patients in areas with unstable internet connections such as rural and remote regions also faced additional barriers to participation in telemedicine delivery of CAIM interventions [97, 98]. This may require government action to enhance internet network bandwidth and deploy advanced generations of network technologies to provide the necessary support as telemedicine continues to expand [97]. On the other hand, provider satisfaction with telemedicine has been studied less frequently as there was a lack of evidence found in this review. This is despite provider perspectives being crucial to the expansion of telemedicine [96].
An important barrier identified by patients is that it was more difficult to establish valuable, meaningful connections with care providers virtually compared to face-to-face. Sharing difficult diagnoses and end-of-life conversations are examples of situations where it is challenging to facilitate via telemedicine, and the telemedicine approach cannot replace human connections formed with a face-to-face conversation [99]. This underscores the importance of ensuring that medical practitioners delivering care using telemedicine modes consider the limitations of these approaches. Both patients and providers reflecting on using telemedicine for chronic disease management recommended that the initial patient-provider interaction should be face-to-face, and that patients should see the same provider at follow-up visits [100].
It is also important to consider that participants with chronic health conditions such as cardiovascular disease, cancer, or diabetes may experience condition-specific barriers such as “chemo fatigue,” [25] or functional limitations [101]. Older adults with chronic illness may face additional challenges relating to frailty, vision and hearing loss, and cognitive limitations that have relevance in non-face-to-face interventions [102]. Moreover, elderly patients may not be able to handle large volumes of online information and some older adults may become anxious or annoyed when adding technology to their regular routine [102]. This is supported by past studies, which identified that special populations such as older adults, patients with disabilities (e.g., vision or hearing difficulties), limited mobility, and/or racial and ethnic minorities may face additional barriers in telemedicine delivery of care [97, 98]. Accordingly, training both care providers and patients is paramount for effective delivery of CAIM via telemedicine [97].
Implications and future directions
Telemedicine models of care have been used for many years, particularly in the United States, but its use has expanded globally during the COVID-19 pandemic [103]. The reviewed literature highlights the potential to deliver CAIM via telemedicine. This study has generated several areas for future research on CAIM delivered using telemedicine.
Further research is required to identify groups that would realize the greatest impact from telemedicine delivery of CAIM. For patients with chronic conditions such as diabetes or cancer, or for older adults, it is important to consider physical or cognitive limitations that may be barriers to successful completion of these interventions. There is also a need to investigate the impact of a more personalized or tailored approach for these high-needs groups with existing illnesses and morbidities [104].
CAIM interventions delivered via telemedicine would benefit from a more holistic evaluation beyond biomedical outcomes. Currently there is a lack of reporting in the literature on how CAIM therapies delivered via telemedicine compare to face-to-face approaches with respect to provider and staff burden, and the experiences of family and friend caregivers [102]. There is also a lack of incorporation of social determinants of health such as socioeconomic status, and race in telemedicine interventions. Evidence indicates that social determinants affect access to telemedicine for groups already suffering from inequities in healthcare access [105]. Accordingly, future telemedicine policy and research should go beyond technological dimensions, and consider social determinants of health [106]. Further, assessment of outcomes at longer follow-up periods is needed to determine whether telemedicine delivery of CAIM is capable of producing sustainable effects [43, 49, 81].
Finally, future work at the intersection of CAIM and telemedicine should identify and evaluate the (in)appropriate use of telemedicine across various CAIM practices. In line with this, more work is needed to examine the facilitators and barriers that providers face in employing telemedicine delivery of CAIM.
Strengths and limitations
Strengths of this study include adherence to Arksey and O’Malley’s five-stage scoping review framework [12], and the use of a comprehensive systematic search strategy across several bibliographic databases to identify eligible articles. Interpretation of the findings was strengthened by the fact that three authors independently screened, and a total of seven authors extracted, and summarised the findings. There are some limitations to this scoping review. By including studies only written in English, we could be missing important international work. This is especially relevant because CAIM may be practiced more frequently in non-English speaking regions of the world, such as traditional Chinese medicine in China.
Another limitation is that despite the use of a comprehensive search strategy, CAIM is an umbrella term encompassing a broad range of practices and as such, it is possible that not all CAIM therapies were captured in the search. Finally, records outside of those found via bibliographic database searches (e.g., unpublished theses and dissertations) were considered outside of the scope of this review, although we acknowledge that this may have contributed to some relevant literature being missed.
Conclusions
The present scoping review explored the breadth of the literature on telemedicine used in the context of CAIM. Three main themes were identified: 1) the practitioner view of CAIM telemedicine, 2) the patient view of CAIM telemedicine, and 3) the technological impacts of CAIM telemedicine. These themes highlight the feasibility, acceptability, and satisfaction of CAIM delivered via telemedicine from both a practitioner and patient point of view. Telemedicine approaches increase access to CAIM, and there is high potential for scalability. Patient barriers include chronic illness and morbidities, low technical proficiency, and an inability to form meaningful connections with care providers. Further research is required to mitigate barriers to telemedicine uptake and increase the knowledge of clinicians on topics of CAIM and telemedicine. We recognize that this may take the form of changes to training, management techniques, and health-care policies.
Availability of data and materials
All relevant data are included in this manuscript.
Abbreviations
- CADTH:
-
Canadian Agency for Drugs and Technologies in Health
- CAIM:
-
Complementary, alternative, and integrative medicine
References
Wootton R. Recent advances: Telemedicine. BMJ. 2001;323(7312):557–60. https://doi.org/10.1136/bmj.323.7312.557.
Craig J, Patterson V. Introduction to the practice of telemedicine. J Telemed Telecare. 2005;11(1):3–9. https://doi.org/10.1177/1357633X0501100102.
Sood S, Mbarika V, Jugoo S, Dookhy R, Doarn CR, Prakash N, et al. What is telemedicine? A collection of 104 peer-reviewed perspectives and theoretical underpinnings. Telemed J E Health. 2007;13(5):573–90. https://doi.org/10.1089/tmj.2006.0073.
WHO. A Health Telematics Policy in support of WHO’s Health-for-All Strategy for Global Helath Development. 1998.
Serper M, Volk ML. Current and Future Applications of Telemedicine to Optimize the Delivery of Care in Chronic Liver Disease. Clin Gastroenterol Hepatol. 2018;16(2):157–61 e8. https://doi.org/10.1016/j.cgh.2017.10.004.
Jong M, Mendez I, Jong R. Enhancing access to care in northern rural communities via telehealth. Int J Circumpolar Health. 2019;78(2):1554174. https://doi.org/10.1080/22423982.2018.1554174.
Kamsu-Foguem B, Foguem C. Could telemedicine enhance traditional medicine practices? European Research in Telemedicine/La Recherche Européenne en Télémédecine. 2014;3(3):117–23. https://doi.org/10.1016/j.eurtel.2014.08.001.
Ng JY, Boon HS, Thompson AK, Whitehead CR. Making sense of “alternative”, “complementary”, “unconventional” and “integrative” medicine: exploring the terms and meanings through a textual analysis. BMC Complement Altern Med. 2016;16:134. https://doi.org/10.1186/s12906-016-1111-3.
National Center for Complementary and Integrative Health. Complementary, alternative, or integrative health: what’s in a name?. 2022. https://www.nccih.nih.gov/health/complementary-alternative-or-integrative-health-whats-in-a-name.
Niles BL, Klunk-Gillis J, Ryngala DJ, Silberbogen AK, Paysnick A, Wolf EJ. Comparing mindfulness and psychoeducation treatments for combat-related PTSD using a telehealth approach. Psychol Trauma Theory Res Pract Policy. 2012;4(5):538–47. https://doi.org/10.1037/a0026161.
Der-Martirosian C, Shin M, Upham ML, Douglas JH, Zeliadt SB, Taylor SL. Telehealth Complementary and Integrative Health Therapies During COVID-19 at the U.S. Department of Veterans Affairs. Telemed J E Health. 2022. https://doi.org/10.1089/tmj.2022.0209.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. https://doi.org/10.1080/1364557032000119616.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69. https://doi.org/10.1186/1748-5908-5-69.
Daudt HM, van Mossel C, Scott SJ. Enhancing the scoping study methodology: a large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med Res Methodol. 2013;13:48. https://doi.org/10.1186/1471-2288-13-48.
Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–26. https://doi.org/10.11124/JBIES-20-00167.
Anthony JB. Implications of telehealth and digital care solutions during COVID-19 pandemic: a qualitative literature review. Inform Health Soc Care. 2021;46(1):68–83. https://doi.org/10.1080/17538157.2020.1839467.
Crilly P, Kayyali R. A Systematic Review of Randomized Controlled Trials of Telehealth and Digital Technology Use by Community Pharmacists to Improve Public Health. Pharmacy (Basel). 2020;8(3). https://doi.org/10.3390/pharmacy8030137.
Baker J, Stanley A. Telemedicine Technology: a Review of Services, Equipment, and Other Aspects. Curr Allergy Asthma Rep. 2018;18(11):60. https://doi.org/10.1007/s11882-018-0814-6.
Ng JY, Dhawan T, Dogadova E, Taghi-Zada Z, Vacca A, Wieland LS, et al. Operational definition of complementary, alternative, and integrative medicine derived from a systematic search. BMC Complement Med Ther. 2022;22(1):104. https://doi.org/10.1186/s12906-022-03556-7.
Medicine CC. Operational Definition of Complementary, Alternative, and Integrative Medicine: The Cochrane Collaboration 2022 [https://cam.cochrane.org/operational-definition-complementary-medicine.
Canadian Agency for Drugs and Technologies in Health. Grey Matters: A Practical Tool for Searching Health-Related Grey Literature. Ottawa, ON: CADTH; 2018.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. https://doi.org/10.1016/j.ijsu.2021.105906.
Selman L, McDermott K, Donesky D, Citron T, Howie-Esquivel J. Appropriateness and acceptability of a Tele-Yoga intervention for people with heart failure and chronic obstructive pulmonary disease: qualitative findings from a controlled pilot study. BMC Complement Altern Med. 2015;15:21. https://doi.org/10.1186/s12906-015-0540-8.
Wang L, Valentini J, Sugimoto K, Cheng W, Cheng G, Geng H, et al. Biomedical Teleacupuncture between China and Austria Using Heart Rate Variability, Part 1: Poststroke Patients. Evid Based Complement Alternat Med. 2011;2011:782489. https://doi.org/10.1155/2011/782489.
Addington EL, Sohl SJ, Tooze JA, Danhauer SC. Convenient and Live Movement (CALM) for women undergoing breast cancer treatment: Challenges and recommendations for internet-based yoga research. Complement Ther Med. 2018;37:77–9. https://doi.org/10.1016/j.ctim.2018.02.001.
Armin JS, Nair U, Giacobbi P, Povis G, Barraza Y, Gordon JS. Developing a Guided Imagery Telephone-Based Tobacco Cessation Program for a Randomized Controlled Trial. Tob Use Insights. 2020;13:1179173X20949267. https://doi.org/10.1177/1179173X20949267.
Berman RL, Iris MA, Bode R, Drengenberg C. The effectiveness of an online mind-body intervention for older adults with chronic pain. J Pain. 2009;10(1):68–79. https://doi.org/10.1016/j.jpain.2008.07.006.
Bombardier CH, Ehde DM, Gibbons LE, Wadhwani R, Sullivan MD, Rosenberg DE, et al. Telephone-based physical activity counseling for major depression in people with multiple sclerosis. J Consult Clin Psychol. 2013;81(1):89–99. https://doi.org/10.1037/a0031242.
Cavalera C, Rovaris M, Mendozzi L, Pugnetti L, Garegnani M, Castelnuovo G, et al. Online meditation training for people with multiple sclerosis: A randomized controlled trial. Mult Scler. 2019;25(4):610–7. https://doi.org/10.1177/1352458518761187.
Cheung DST, Or CKL, So MKP, Tiwari A. Usability Testing of a Smartphone Application for Delivering Qigong Training. J Med Syst. 2018;42(10):191. https://doi.org/10.1007/s10916-018-1048-9.
Davis JM, Manley AR, Goldberg SB, Stankevitz KA, Smith SS. Mindfulness training for smokers via web-based video instruction with phone support: a prospective observational study. BMC Complement Altern Med. 2015;15:95. https://doi.org/10.1186/s12906-015-0618-3.
Dimitropoulos A, Zyga O, Russ S. Evaluating the Feasibility of a Play-Based Telehealth Intervention Program for Children with Prader-Willi Syndrome. J Autism Dev Disord. 2017;47(9):2814–25. https://doi.org/10.1007/s10803-017-3196-z.
Donesky D, Selman L, McDermott K, Citron T, Howie-Esquivel J. Evaluation of the Feasibility of a Home-Based TeleYoga Intervention in Participants with Both Chronic Obstructive Pulmonary Disease and Heart Failure. J Altern Complement Med. 2017;23(9):713–21. https://doi.org/10.1089/acm.2015.0279.
Ezenwa MO, Yao Y, Engeland CG, Molokie RE, Wang ZJ, Suarez ML, et al. A randomized controlled pilot study feasibility of a tablet-based guided audio-visual relaxation intervention for reducing stress and pain in adults with sickle cell disease. J Adv Nurs. 2016;72(6):1452–63. https://doi.org/10.1111/jan.12895.
Ferraris C, Guglielmetti M, Tamagni E, Trentani C, De Giorgis V, Pasca L, et al. Use of Remote Monitoring by E-mail for Long-Term Management of the Classic Ketogenic Diet. Nutrients. 2020;12(6). https://doi.org/10.3390/nu12061833.
Freeman LW, White R, Ratcliff CG, Sutton S, Stewart M, Palmer JL, et al. A randomized trial comparing live and telemedicine deliveries of an imagery-based behavioral intervention for breast cancer survivors: reducing symptoms and barriers to care. Psychooncology. 2015;24(8):910–8. https://doi.org/10.1002/pon.3656.
Gardner-Nix J, Barbati J, Grummitt J, Pukal S, Raponi NR. Exploring the Effectiveness of a Mindfulness-Based Chronic Pain Management Course Delivered Simultaneously to On-Site and Off-Site Patients Using Telemedicine. Mindfulness. 2014;5:223–31.
Golebowicz M, Levanon Y, Palti R, Ratzon NZ. Efficacy of a telerehabilitation intervention programme using biofeedback among computer operators. Ergonomics. 2015;58(5):791–802. https://doi.org/10.1080/00140139.2014.982210.
Green BN, Pence TV, Kwan L, Rokicki-Parashar J. Rapid Deployment of Chiropractic Telehealth at 2 Worksite Health Centers in Response to the COVID-19 Pandemic: Observations from the Field. J Manipulative Physiol Ther. 2020;43(5):404 e1- e10. https://doi.org/10.1016/j.jmpt.2020.05.008.
Guetin S, Brun L, Deniaud M, Clerc JM, Thayer JF, Koenig J. Smartphone-based Music Listening to Reduce Pain and Anxiety Before Coronarography: A Focus on Sex Differences. Altern Ther Health Med. 2016;22(4):60–3.
Hansen MM. A feasibility pilot study on the use of complementary therapies delivered via mobile technologies on Icelandic surgical patients’ reports of anxiety, pain, and self-efficacy in healing. BMC Complement Altern Med. 2015;15:92. https://doi.org/10.1186/s12906-015-0613-8.
Hasan SS, Pearson JS, Morris J, Whorwell PJ. SKYPE HYPNOTHERAPY FOR IRRITABLE BOWEL SYNDROME: Effectiveness and Comparison with Face-to-Face Treatment. Int J Clin Exp Hypn. 2019;67(1):69–80. https://doi.org/10.1080/00207144.2019.1553766.
Hernandez R, Burrows B, Wilund K, Cohn M, Xu S, Moskowitz JT. Feasibility of an Internet-based positive psychological intervention for hemodialysis patients with symptoms of depression. Soc Work Health Care. 2018;57(10):864–79. https://doi.org/10.1080/00981389.2018.1523268.
Horneber M, van Ackeren G, Fischer F, Kappauf H, Birkmann J. Addressing Unmet Information Needs: Results of a Clinician-Led Consultation Service About Complementary and Alternative Medicine for Cancer Patients and Their Relatives. Integr Cancer Ther. 2018;17(4):1172–82. https://doi.org/10.1177/1534735418808597.
Houweling TA, Braga AV, Hausheer T, Vogelsang M, Peterson C, Humphreys BK. First-contact care with a medical vs chiropractic provider after consultation with a swiss telemedicine provider: comparison of outcomes, patient satisfaction, and health care costs in spinal, hip, and shoulder pain patients. J Manipulative Physiol Ther. 2015;38(7):477–83. https://doi.org/10.1016/j.jmpt.2015.06.015.
Hu NZ, Lee CY, Hou MC, Chen YL. A cloud system for mobile medical services of traditional Chinese medicine. J Med Syst. 2013;37(6):9978. https://doi.org/10.1007/s10916-013-9978-8.
Huberty JL, Matthews J, Leiferman J, Cacciatore J. Experiences of women who participated in a beta-test for an online-streamed yoga intervention after a stillbirth. Int J Yoga Therap. 2017;27(1):59–68. https://doi.org/10.17761/1531-2054-27.1.59.
Hucker A, McCabe MP. An online, mindfulness-based, cognitive-behavioral therapy for female sexual difficulties: impact on relationship functioning. J Sex Marital Ther. 2014;40(6):561–76. https://doi.org/10.1080/0092623X.2013.796578.
Kahn JR, Collinge W, Soltysik R. Post-9/11 Veterans and Their Partners Improve Mental Health Outcomes with a Self-directed Mobile and Web-based Wellness Training Program: A Randomized Controlled Trial. J Med Internet Res. 2016;18(9):e255. https://doi.org/10.2196/jmir.5800.
Kemper KJ, Rao N, Gascon G, Mahan JD. Online Training in Mind-Body Therapies: Different Doses, Long-term Outcomes. J Evid Based Complementary Altern Med. 2017;22(4):696–702. https://doi.org/10.1177/2156587217701857.
Kim DS, Chu H, Min BK, Moon Y, Park S, Kim K, et al. Telemedicine Center of Korean Medicine for treating patients with COVID-19: a retrospective analysis. Integr Med Res. 2020;9(3):100492. https://doi.org/10.1016/j.imr.2020.100492.
Krampe J, Rubbelke C, Reeves N, Sullivan M, Whitten M. Building Evidence: Fuze Versus Skype for Dance-Based Therapy With Older Adults and Nursing Students. Comput Inform Nurs. 2016;34(6):241–4. https://doi.org/10.1097/CIN.0000000000000257.
Krampe J, Musterman K. Shall we skype dance? Connecting nursing students with older adults via skype for dance-based therapy. Comput Inform Nurs. 2013;31(4):151–4. https://doi.org/10.1097/NXN.0b013e31828e2faf.
Krout RE, Baker FA, Muhlberger R. Designing, piloting, and evaluating an on-line collaborative songwriting environment and protocol using Skype telecommunication technology: perceptions of music therapy student participants. Music Ther Perspect. 2010;28(1):79–85.
Kubo A, Kurtovich E, McGinnis M, Aghaee S, Altschuler A, Quesenberry C Jr, et al. A Randomized Controlled Trial of mHealth Mindfulness Intervention for Cancer Patients and Informal Cancer Caregivers: A Feasibility Study Within an Integrated Health Care Delivery System. Integr Cancer Ther. 2019;18:1534735419850634. https://doi.org/10.1177/1534735419850634.
Kwon CY, Kwak HY, Kim JW. Using Mind-Body Modalities via Telemedicine during the COVID-19 Crisis: Cases in the Republic of Korea. Int J Environ Res Public Health. 2020;17(12). https://doi.org/10.3390/ijerph17124477.
Lee D, Lee WJ, Choi SH, Jang JH, Kang DH. Long-term beneficial effects of an online mind-body training program on stress and psychological outcomes in female healthcare providers: A non-randomized controlled study. Medicine (Baltimore). 2020;99(32):e21027. https://doi.org/10.1097/MD.0000000000021027.
Lester E, DiStefano S, Mace R, Macklin E, Plotkin S, Vranceanu AM. Virtual mind-body treatment for geographically diverse youth with neurofibromatosis: A pilot randomized controlled trial. Gen Hosp Psychiatry. 2020;62:72–8. https://doi.org/10.1016/j.genhosppsych.2019.12.001.
Mussman KB. A mixed-methods feasibility study on the provision of a brief online yoga intervention as e-health for improving stress management: Perceived stress, stage of change for stress management, and self-efficacy for stress management and engagement in yoga (Doctoral dissertation, Teachers College, Columbia University). 2016. https://www.proquest.com/docview/1799599787.
Ondersma SJ, Beatty JR, Puder KS, Janisse J, Svikis DS. Feasibility and Acceptability of e-Screening and Brief Intervention and Tailored Text Messaging for Marijuana Use in Pregnancy. J Womens Health (Larchmt). 2019;28(9):1295–301. https://doi.org/10.1089/jwh.2018.7169.
Papadaki A, Thanasoulias A, Pound R, Sebire SJ, Jago R. Employees' Expectations of Internet-Based, Workplace Interventions Promoting the Mediterranean Diet: A Qualitative Study. J Nutr Educ Behav. 2016;48(10):706–15 e1. https://doi.org/10.1016/j.jneb.2016.08.003.
Petersen CL, Callahan MF, McCarthy DO, Hughes RG, White-Traut R, Bansal NK. An Online Educational Program Improves Pediatric Oncology Nurses’ Knowledge, Attitudes, and Spiritual Care Competence. J Pediatr Oncol Nurs. 2017;34(2):130–9. https://doi.org/10.1177/1043454216646542.
Reilly-Spong M, Reibel D, Pearson T, Koppa P, Gross CR. Telephone-adapted mindfulness-based stress reduction (tMBSR) for patients awaiting kidney transplantation: Trial design, rationale and feasibility. Contemp Clin Trials. 2015;42:169–84. https://doi.org/10.1016/j.cct.2015.03.013.
Rickhi B, Kania-Richmond A, Moritz S, Cohen J, Paccagnan P, Dennis C, et al. Evaluation of a spirituality informed e-mental health tool as an intervention for major depressive disorder in adolescents and young adults - a randomized controlled pilot trial. BMC Complement Altern Med. 2015;15:450. https://doi.org/10.1186/s12906-015-0968-x.
Rogante M, Silvestri S, Grigioni M, Zampolini M. Electromyographic audio biofeedback for telerehabilitation in hospital. J Telemed Telecare. 2010;16(4):204–6. https://doi.org/10.1258/jtt.2010.004012.
Rosmarin DH, Pargament KI, Pirutinsky S, Mahoney A. A randomized controlled evaluation of a spiritually integrated treatment for subclinical anxiety in the Jewish community, delivered via the Internet. J Anxiety Disord. 2010;24(7):799–808. https://doi.org/10.1016/j.janxdis.2010.05.014.
Rybarczyk B, DeMarco G, DeLaCruz M, Lapidos S. Comparing mind-body wellness interventions for older adults with chronic illness: classroom versus home instruction. Behav Med. 1999;24(4):181–90. https://doi.org/10.1080/08964289.1999.11879274.
Sarah S, Wolfgang MB, Claudia P. Effect of telerehabilitation on long-term adherence to yoga as an antihypertensive lifestyle intervention: Results of a randomized controlled trial. Complement Ther Clin Pract. 2019;35:148–53. https://doi.org/10.1016/j.ctcp.2019.02.001.
Seidler KJ, Duncan RP, McNeely ME, Hackney ME, Earhart GM. Feasibility and preliminary efficacy of a telerehabilitation approach to group adapted tango instruction for people with Parkinson disease. J Telemed Telecare. 2017;23(8):740–6. https://doi.org/10.1177/1357633X16668092.
Shrier LA, Rhoads AM, Fredette ME, Burke PJ. “Counselor in Your Pocket”: Youth and Provider Perspectives on a Mobile Motivational Intervention for Marijuana Use. Subst Use Misuse. 2014;49(1–2):134–44. https://doi.org/10.3109/10826084.2013.824470.
Simpson S, Morrow E, Jones M, Ferguson J, Brebner E. Video-hypnosis–the provision of specialized therapy via videoconferencing. J Telemed Telecare. 2002;8(Suppl 2):78–9. https://doi.org/10.1177/1357633X020080S236.
Singh NN, Chan J, Karazsia BT, McPherson CL, Jackman MM. Tele-health training of teachers to teach a mindfulness-based procedure for self-management of aggressive behavior to students with intellectual and developmental disabilities. International Journal of Developmental Disabilities. 2017;63(4):195–203. https://doi.org/10.1080/20473869.2016.1277841.
Stubberud A, Tronvik E, Olsen A, Gravdahl G, Linde M. Biofeedback Treatment App for Pediatric Migraine: Development and Usability Study. Headache. 2020;60(5):889–901. https://doi.org/10.1111/head.13772.
Tan G, Teo I, Srivastava D, Smith D, Smith SL, Williams W, et al. Improving access to care for women veterans suffering from chronic pain and depression associated with trauma. Pain Med. 2013;14(7):1010–20. https://doi.org/10.1111/pme.12131.
Thompson NJ, Patel AH, Selwa LM, Stoll SC, Begley CE, Johnson EK, et al. Expanding the efficacy of Project UPLIFT: Distance delivery of mindfulness-based depression prevention to people with epilepsy. J Consult Clin Psychol. 2015;83(2):304–13. https://doi.org/10.1037/a0038404.
Tkatch R, Bazarko D, Musich S, Wu L, MacLeod S, Keown K, et al. A Pilot Online Mindfulness Intervention to Decrease Caregiver Burden and Improve Psychological Well-Being. J Evid Based Complementary Altern Med. 2017;22(4):736–43. https://doi.org/10.1177/2156587217737204.
Tucker LA, Cook AJ, Nokes NR, Adams TB. Telephone-based diet and exercise coaching and a weight-loss supplement result in weight and fat loss in 120 men and women. Am J Health Promot. 2008;23(2):121–9. https://doi.org/10.4278/ajhp.07051646.
Uebelacker L, Dufour SC, Dinerman JG, Walsh SL, Hearing C, Gillette LT, et al. Examining the Feasibility and Acceptability of an Online Yoga Class for Mood Disorders: A MoodNetwork Study. J Psychiatr Pract. 2018;24(1):60–7. https://doi.org/10.1097/PRA.0000000000000286.
Vederhus JK, Rorendal M, Bjelland C, Skar AKS, Kristensen O. Can a Smartphone App for Cannabis Cessation Gain a Broader User Group than Traditional Treatment Services? Subst Abuse. 2020;14:1178221820902237. https://doi.org/10.1177/1178221820902237.
Vranceanu AM, Riklin E, Merker VL, Macklin EA, Park ER, Plotkin SR. Mind-body therapy via videoconferencing in patients with neurofibromatosis: An RCT. Neurology. 2016;87(8):806–14. https://doi.org/10.1212/WNL.0000000000003005.
Wang Q, Chair SY, Wong EM, Li X. The Effects of Music Intervention on Sleep Quality in Community-Dwelling Elderly. J Altern Complement Med. 2016;22(7):576–84. https://doi.org/10.1089/acm.2015.0304.
Yeh ML, Hung YL, Chen HH, Lin JG, Wang YJ. Auricular acupressure combined with an internet-based intervention or alone for primary dysmenorrhea: a control study. Evid Based Complement Alternat Med. 2013;2013:316212. https://doi.org/10.1155/2013/316212.
Zini EM, Tagliabue A, Trentani C, Ferraris C, Boninsegna R, Quaglini S, et al. An mHealth Application for Educating and Monitoring Patients Treated with a Ketogenic Diet Regimen. Stud Health Technol Inform. 2018;247:481–5.
Zwart LM, Palmer SL, Strawn BD, Milliron JT, Brown WS. The impact of lay pastoral telecare on the spiritual well-being of church attenders. J Pastoral Care. 2000;54(1):63–73. https://doi.org/10.1177/002234090005400108.
In: Joy JE, Penhoet EE, Petitti DB, editors. Saving Women's Lives: Strategies for Improving Breast Cancer Detection and Diagnosis. The National Academies Collection: Reports funded by National Institutes of Health. Washington (DC)2005. https://doi.org/10.17226/11016.
Beheshti L, Kalankesh LR, Doshmangir L, Farahbakhsh M. Telehealth in Primary Health Care: A Scoping Review of the Literature. Perspect Health Inf Manag. 2022;19(1):1n.
Morland LA, Wells SY, Glassman LH, Greene CJ, Hoffman JE, Rosen CS. Advances in PTSD Treatment Delivery: Review of Findings and Clinical Considerations for the Use of Telehealth Interventions for PTSD. Current Treatment Options in Psychiatry. 2020;7(3):221–41. https://doi.org/10.1007/s40501-020-00215-x.
Sutherland R, Trembath D, Roberts J. Telehealth and autism: A systematic search and review of the literature. Int J Speech Lang Pathol. 2018;20(3):324–36. https://doi.org/10.1080/17549507.2018.1465123.
King SC, Richner KA, Tuliao AP, Kennedy JL, McChargue DE. A comparison between telehealth and face-to-face delivery of a brief alcohol intervention for college students. Subst Abus. 2020;41(4):501–9. https://doi.org/10.1080/08897077.2019.1675116.
Laver K, Liu E, Clemson L, Davies O, Gray L, Gitlin LN, et al. Does Telehealth Delivery of a Dyadic Dementia Care Program Provide a Noninferior Alternative to Face-To-Face Delivery of the Same Program? A Randomized. Controlled Trial Am J Geriatr Psychiatry. 2020;28(6):673–82. https://doi.org/10.1016/j.jagp.2020.02.009.
Whitley A, Yahia N. Efficacy of Clinic-Based Telehealth vs. Face-to-Face Interventions for Obesity Treatment in Children and Adolescents in the United States and Canada: A Systematic Review. Child Obes. 2021;17(5):299–310. https://doi.org/10.1089/chi.2020.0347.
Eze ND, Mateus C, Cravo Oliveira Hashiguchi T. Telemedicine in the OECD: An umbrella review of clinical and cost-effectiveness, patient experience and implementation. PLoS One. 2020;15(8):e0237585. https://doi.org/10.1371/journal.pone.0237585.
Mills EC, Savage E, Lieder J, Chiu ES. Telemedicine and the COVID-19 Pandemic: Are We Ready to Go Live? Adv Skin Wound Care. 2020;33(8):410–7. https://doi.org/10.1097/01.ASW.0000669916.01793.93.
Barbosa W, Zhou K, Waddell E, Myers T, Dorsey ER. Improving Access to Care: Telemedicine Across Medical Domains. Annu Rev Public Health. 2021;42(1):463–81. https://doi.org/10.1146/annurev-publhealth-090519-093711.
Harkey LC, Jung SM, Newton ER, Patterson A. Patient Satisfaction with Telehealth in Rural Settings: A Systematic Review. Int J Telerehabil. 2020;12(2):53–64. https://doi.org/10.5195/ijt.2020.6303.
Nguyen M, Waller M, Pandya A, Portnoy J. A Review of Patient and Provider Satisfaction with Telemedicine. Curr Allergy Asthma Rep. 2020;20(11):72. https://doi.org/10.1007/s11882-020-00969-7.
Ftouni R, AlJardali B, Hamdanieh M, Ftouni L, Salem N. Challenges of Telemedicine during the COVID-19 pandemic: a systematic review. BMC Med Inform Decis Mak. 2022;22(1):207. https://doi.org/10.1186/s12911-022-01952-0.
Brunton C, Arensberg MB, Drawert S, Badaracco C, Everett W, McCauley SM. Perspectives of Registered Dietitian Nutritionists on Adoption of Telehealth for Nutrition Care during the COVID-19 Pandemic. Healthcare. 2021;9(2):235.
Fix OK, Serper M. Telemedicine and Telehepatology During the COVID-19 Pandemic. Clin Liver Dis (Hoboken). 2020;15(5):187–90. https://doi.org/10.1002/cld.971.
Hiratsuka V, Delafield R, Starks H, Ambrose AJ, Mau MM. Patient and provider perspectives on using telemedicine for chronic disease management among Native Hawaiian and Alaska Native people. Int J Circumpolar Health. 2013;72(1):21401. https://doi.org/10.3402/ijch.v72i0.21401.
Cnossen IC, van Uden-Kraan CF, Rinkel RN, Aalders IJ, de Goede CJ, de Bree R, et al. Multimodal guided self-help exercise program to prevent speech, swallowing, and shoulder problems among head and neck cancer patients: a feasibility study. J Med Internet Res. 2014;16(3):e74. https://doi.org/10.2196/jmir.2990.
Foster MV, Sethares KA. Facilitators and barriers to the adoption of telehealth in older adults: an integrative review. Comput Inform Nurs. 2014;32(11):523–33; quiz 34–5. https://doi.org/10.1097/CIN.0000000000000105.
Wosik J, Fudim M, Cameron B, Gellad ZF, Cho A, Phinney D, et al. Telehealth transformation: COVID-19 and the rise of virtual care. J Am Med Inform Assoc. 2020;27(6):957–62. https://doi.org/10.1093/jamia/ocaa067.
Freed J, Lowe C, Flodgren G, Binks R, Doughty K, Kolsi J. Telemedicine: Is it really worth it? A perspective from evidence and experience. J Innov Health Inform. 2018;25(1):14–8. https://doi.org/10.14236/jhi.v25i1.957.
Romain Carmelle V, Trinidad S, Kotagal M. The Effect of Social Determinants of Health on Telemedicine Access During the COVID-19 Pandemic. Pediatr Ann. 2022;51(8):e311–5. https://doi.org/10.3928/19382359-20220606-04.
Saigi-Rubió F, Jiménez-Zarco A, Torrent-Sellens J. Determinants of the intention to use telemedicine: evidence from primary care physicians. Int J Technol Assess Health Care. 2016;32(1–2):29–36. https://doi.org/10.1017/S0266462316000015.
Acknowledgements
None.
Funding
JYN was awarded a Research Scholarship and an Entrance Scholarship from the Department of Health Research Methods, Evidence and Impact, Faculty of Health Sciences at McMaster University.
Author information
Authors and Affiliations
Contributions
AQS: collected and analysed data, co-drafted the manuscript, and gave final approval of the version to be published. NN: collected and analysed data, co-drafted the manuscript, and gave final approval of the version to be published. RCS: collected and analysed data, critically revised the manuscript, and gave final approval of the version to be published. CH: collected and analysed data, critically revised the manuscript, and gave final approval of the version to be published. ZK: collected and analysed data, critically revised the manuscript, and gave final approval of the version to be published. AM: collected and analysed data, critically revised the manuscript, and gave final approval of the version to be published. NR: collected and analysed data, critically revised the manuscript, and gave final approval of the version to be published. JYN: designed and conceptualized the study, collected and analysed data, critically revised the manuscript, and gave final approval of the version to be published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study involved a systematic review of peer-reviewed literature only; it did not require ethics approval or consent to participate.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shah, A.Q., Noronha, N., Chin-See, R. et al. The use and effects of telemedicine on complementary, alternative, and integrative medicine practices: a scoping review. BMC Complement Med Ther 23, 275 (2023). https://doi.org/10.1186/s12906-023-04100-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-023-04100-x