
Abstract
Background
Traditional and complementary medicine (T&CM) is commonly used in South Asian countries such as Nepal. There are various causes and contributing factors for patients with cancer to consider using T&CM. However, little is known about the use of T&CM among the cancer population in this region.
Methods
The study followed a cross-sectional design using a structured survey questionnaire. Survey participants were recruited from two National hospitals in Kathmandu, Nepal. The survey instrument comprised 30 questions, including variables on demographics, use of T&CM, and perceived level of disease severity, and cancer treatment. Chi-square test and logistic regression were used for data analysis using SPSS ver. 23.0.
Results
Of 908 participants, 31.6% used one or more modalities of T&CM after a cancer diagnosis. The most commonly used T&CM was Ayurveda (46.5%), followed by yoga (32.4%). About 46% of T&CM users discussed their use with their doctors. The main source of information on T&CM was their family members and relatives (55.7%). Cancer type (head and neck cancer OR: 2.30, CI: 1.23–4.29; abdominal cancer OR: 2.69, CI: 1.47–4.95; lung cancer OR: 5.88, CI: 2.69–12.89), cancer stage (Stage I OR: 1.92¸CI: 1.14–3.25; Stage II OR: 1.76, CI: 1.06–2.94), and the patients’ self-rated disease severity (high perceived severity OR: 1.50, CI: 1.05–2.16) were strong predictors of T&CM use.
Conclusion
This study underlined that despite the widespread use of T&CM among cancer patients in Nepal, most patients obtained information on T&CM from informal sources and did not disclose their use to physicians. To ensure the safe use of T&CM modalities, physicians should integrate questions on T&CM use into routine patient assessments in order to facilitate active communication and improve the quality of care.
Similar content being viewed by others

Background
Cancer is still a life-threatening disease for all populations and can pose a greater challenge in resource-limited countries, where cancer diagnosis and treatment are delayed due to the inadequate availability of medical services [1]. Despite global efforts to improve cancer patients’ accessibility to conventional medicine [2, 3], traditional medicine has been generally considered an available and affordable medical resource in less developed countries, such as Nepal [4,5,6]. Traditional and complementary medicine (T&CM) is an umbrella term that refers to a set of healthcare practices provided outside of the dominant medical system and forms of indigenous medicine such as Ayurveda medicine [7].
The use of T&CM is common in various cultural settings [7], and its use among the cancer patients has increased over the past decades [4, 8, 9]. Since the early 1980s, multiple studies examined patterns or predictors of T&CM utilization among cancer patients [9,10,11]. The average prevalence of T&CM use in cancer patients has doubled from 25.0% before the 1990s [8] to 51.0% after the 2010s [9]. The increasing trends in T&CM use seem to reflect unmet needs that are commonly identified among cancer patients, associated with their physical and psychological symptoms and quality of life [12]. Given the potential risk of concurrent use with anti-cancer treatment and complementary therapies, identifying the predictors of traditional and complementary medicine (T&CM) use among cancer patients is a significant public health concern [13, 14].
According to the complementary and alternative medicine (CAM) healthcare model [15], individuals perceiving high severity of illness are generally more likely to pursue all kinds of health care services under their beliefs. Patients experiencing more severe symptoms or poor prognoses were more likely to use non-conventional medicine to improve their health [16,17,18]. However, no previous literature has identified differences in T&CM modalities used by cancer patients depending on the perceived level of disease severity.
Nepal, located in the Hindu Kush Himalayan (HKH) region, has a long history of traditional medicines use, which have been passed down through generations in a community-based belief system [19, 20]. More than half of patients with chronic conditions in Nepal (55.7%) used non-conventional therapies, especially Ayurveda. Furthermore, patients aged 40 or above, with higher education levels, higher family income, residing in cities, and with chronic problems were more likely to rely on self-care approaches [21]. However, no studies have focused on the T&CM use by Nepalese cancer patients. Therefore, this study aims to investigate the prevalence, patterns, and predictors of T&CM used by patients with cancer in Nepal, particularly the differences in the use of T&CM modalities based on the patients’ perceived severity of the disease. This study also explores the doctor-patient communication on T&CM use.
Methods
Study design
A cross-sectional study was conducted to assess the T&CM use among cancer patients in Nepal.
Study setting and participants
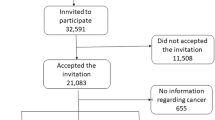
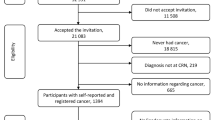
The study was conducted at Bhaktapur Cancer Hospital (BCH) and Tribhuvan University Teaching Hospital (TUTH). TUTH is the largest tertiary hospital and provides care in all major specialties to 700 inpatients and more than 2000 outpatients per day. BCH is the only specialized cancer hospital in Kathmandu (the capital city), providing almost 425 outpatient services, including radiation and daycare, emergency care with 110 inpatient services per day. These two hospitals cover almost half of the cancer care services of the nation. Patients in the oncology wards and visiting outpatient clinics during the data collection period were invited to participate in the study. Eligible participants were diagnosed with cancer at the time of the interview, 18 years of age or older, and understood questions in Nepali or English. Exclusion criteria were newly diagnosed cancer patients because cancer diagnosis could not have influenced the patient’s use of T&CM, and the patients who expressed refusal to participate in the survey or had difficulty responding to the survey.
Study size
The required sample size was calculated using the confidence interval-based sample size determination formula: n = Z2α/2*pq/d2, where n is the required sample size, α = 1-CL, Zα/2 is 1.96, which corresponds to the confidence interval of 95%, d is the margin of error set on 0.035, p is expected proportion based on an average prevalence of T&CM use in South Asian countries (p = 0.56) [22,23,24,25,26], and q is the proportion of people not using T&CM (1-p). The calculated sample size was 771, and the total sample size was 930 considering a 20% non-response rate.
Data collection
The data was collected by two trained nurses through face-to-face interviews using a structured questionnaire from December 2018 and August 2019. All participation was voluntary, and Institutional Review Board (IRB) approved informed consent was obtained before the survey. If the respondents could not read the self- administered questionnaire, a written/signed informed consent were obtained from legal guardian for study participation. A total of 930 cancer patients were invited to participate in the study, and after excluding the incomplete responses, 908 responses were included in the final analysis (a response rate of 97.6%).
Survey instrument
The questionnaire was first developed in the English language based on previous studies investigating T&CM use among cancer patients [23, 27,28,29,30], and the content validity of the questionnaire was tested by four experts (two researchers who previously conducted similar studies in Korea and two research advisors from TUTH Research Center, Nepal). A Nepalese researcher then translated the questionnaire into the Nepali language, and it was converted back into English to verify its accuracy. Lastly, the pilot test was performed with 20 participants to improve its clarity and evaluate the reliability of the modified questionnaire.
The final version of the questionnaire consisted of four sections with 36 items, including multiple-choice and open-ended questions. The first section included 11 questions on the medical characteristics of participants, such as cancer types, stage of cancer, type of conventional treatment, and health behaviors obtained from the medical records. The second section contained Likert-type scales to assess the patient’s current health status, including general health condition (1 = poor, 5 = excellent), and the level of disease severity and perceived discomfort due to conventional cancer treatment (1 = not at all severe, 10 = extremely severe). The third section includes eleven questions regarding T&CM use, which contain the patterns of T&CM use, the reason for T&CM use, the perceived effectiveness of T&CM, side effects of T&CM, the sources of information about T&CM, and the disclosure of T&CM use to physicians. T&CM modalities were categorized into three different groups based on their type (i.e., natural products such as herbal products, honey, vitamins, and minerals; mind and body practices such as yoga, meditation, massage, prayers, and spiritual process; and the complementary approaches such as Ayurveda and traditional healers). Furthermore, the last section consists of ten questions on the socio-economic characteristics of respondents (gender, age, educational level, employment status, perceived-economic status, area of residence, religion, ethnicity, marital status, housing type, and family structure).
Statistical analysis
The collected data were summarized using Statistical Package for Social Sciences (SPSS) version 23.0. Pearson’s Chi-square test was used to identify associations between T&CM use and variables; gender, age groups (≤49, 50–59, ≥60), levels of education (no formal education, basic education and above), place of residence (city, municipality, village), employment (housewife, employed), economic status (enough, barely enough, inadequate), types of cancer (hematologic cancer, urogenital cancer, women’s cancer (ovary/breast), head and neck cancer, abdominal cancer, and lung cancer), and received conventional treatments (surgery, radiotherapy, chemotherapy, and others). Items measured on a 10-point scale were categorized into two groups based on the average response value: self-perceived disease severity (average response: 6.11; low-perceived disease severity: 1–6; high-perceived disease severity: 7–10) and level of discomfort due to conventional cancer treatments (average response: 2.79; low-level of discomfort: 1–3; high-level of discomfort: 4–10). Lastly, multivariate logistic regression analysis was conducted to determine potential predictors of T&CM use among cancer patients. The significant factors from the previous chi-square test (age, education, residential area, employment status, type of cancer, cancer stage, type of conventional cancer treatment (CCT), self-rated disease severity, perceived discomfort in CCT were included in the regression analysis. In addition, only the data of 784 respondents with specific cancer type (i.e., non-metastatic cancer) was included in the regression analysis because cancer type, which is one of the significant factors from the chi-square analysis, only includes the data of patients with localized cancer.
Ethical clearance
The study was performed in compliance with the Declaration of Helsinki. The Institutional Review Board on Human Subjects Research and Ethics Committees at Hanyang University (HYI-18-164-2) and Institutional Review Committee at Tribhuvan University (437 (6–11) E2 /075/76) approved the study.
Results
Sociodemographic and clinical characteristics of study participants
The sociodemographic and clinical characteristics of the respondents are shown in Table 1. The mean age of the respondents was 53.7 ± 15.6 years (range 18–92), and the ratio of males and females was similar. The majority were respondents without a spouse (69.3%), employed (56.4%), without any formal education (78.3%), and lived outside the city (82.5%). The most frequent types of cancer were abdominal cancer (22.8%), followed by head and neck cancer (20.3%), and hematologic cancer (18.3%).
Use of T&CM
Overall, 31.6% (n = 287) of participants used at least one type of T&CM (Table 1). Significant differences between T&CM users and non-users were found in age (p = 0.005), education level (p = 0.002), employment status (p < 0.001), and residential area (p = 0.001). In addition, we found that the type of cancer (p < 0.001), cancer stage (p < 0.001), type of treatment such as surgery (p = 0.025) and radiotherapy (p = 0.001) were associated with T&CM use. The respondents rated their self-perceived severity and the discomfort level due to conventional cancer treatment as 6.11 ± 2.08 and 2.79 ± 1.04, respectively, which were significantly higher among T&CM users (p < 0.001). As Fig. 1 presents, there were significant differences in T&CM use among the different cancer diagnostic groups of the respondents (p < 0.001). The highest prevalence of T&CM use was observed among lung cancer patients (62.3%), followed by abdominal cancer patients (38.2%), and the patients with head and neck cancer (36.4%).

Frequency of T&CM use by cancer diagnostic group
T&CM modalities
The most common types of CAM, reportedly used by respondents, were Ayurveda (46.5%), yoga (32.4%), herbal products (30.9%), meditation (28.9%), and honey (23.4%). Table 2 shows the T&CM modalities used by respondents based on the self-rating of disease severity. Among natural products, herbal product use was the highest (30.9%), followed by honey (23.4%). Consumption of honey (p < 0.001) and ginger (p < 0.001) was significantly greater in the group with a higher rating of disease severity. For mind and body practices, yoga, meditation, and praying was most common among respondents (32.4, 28.9, 12.5%, respectively), and it was also found that yoga (p < 0.001) and meditation (p < 0.001) were significantly higher in the group with the greater perception of disease severity. Among other complementary health approaches, consumption of Ayurveda was the most prevalent (46.5%), followed by traditional healers (18.4%).
Source of information on T&CM
As presented in Table 3, the main source of information on T&CM as reported by the cancer patients was their family members and relatives (55.7%), followed by friends (27.2%), and billboard advertisements/magazines/TV/radio (7.1%). Only, 6.3% of respondents obtained T&CM information from T&CM providers.
Reasons for T&CM use and non-disclosure of T&CM use to physicians
The most frequently stated reasons for T&CM use were due to patients’ desire to do everything possible to fight the disease (54.7%), to relieve symptoms (49.1%), to improve the general condition (48.1%), and to improve immune function (39.7%). Among non-users, the primary reason was insufficient information on the efficacy of T&CM (34.5%), followed by satisfaction with conventional medicine (30.6%). Of the 287 participants that used T&CM, 46.1% disclosed their physician of T&CM use. The most reported reason for non-disclosure of T&CM use was the doctors not asking about the use (51.7%), followed by the fear of doctors discouraging T&CM use (22.6%), and the concern over the doctor not understanding their use (14.2%) (Table 3).
Predictors of T&CM use
The results from multivariate logistic regression analysis are shown in Table 4, and it revealed that patients with lung cancer were 5.88 times more likely to use T&CM than patients with hematologic cancer (CI: 2.69–12.89, p < 0.001). In addition, suffering from abdominal cancer (OR: 2.69, CI: 1.47–4.95) or head and neck cancer (OR: 2.30, CI: 1.23–4.29), early-stages of cancer (Stage I OR: 1.92¸CI: 1.14–3.25; Stage II OR: 1.76, CI: 1.06–2.94), and having higher perceived disease severity (OR: 1.50, CI: 1.05–2.16) were positively associated with the utilization of T&CM.
Discussion
To our knowledge, this is the first study to explore the prevalence and patterns of T&CM use among cancer patients in Nepal. The overall prevalence of T&CM use among Nepali cancer patients was 31.6%, and among the cancer groups, the prevalence of T&CM ranged from 13.3% (hematologic cancer) to 62.3% (lung cancer). The finding was in accordance with a previous study [4], a systematic review of T&CM use in cancer patients in low-income and lower-middle-income countries.
The use of T&CM was associated with various factors such as education, residence, cancer stage, and perceived disease severity, which are in line with the previous studies such as a higher level of education [27, 29, 31, 32], residing outside the urban [6], the early stage of cancer [18], and the higher perceived disease severity [18]. Interestingly, the prevalence rates of T&CM use were different based on cancer types and stages. Despite suggestions from the literature that T&CM use is significantly higher in the group with advanced diseases and recurrent diseases [33], some studies showed that the tumor stage is not associated with the use of alternative therapies [28, 34]. Moreover, the present study showed that patients with advanced cancer stage were less likely to use T&CM. These results suggest that cancer stages affecting the use of T&CM are varied. These variations between studies may be explained by various causes such as the attitude of oncologists, cultural and religious beliefs, the cost of conventional treatment, and the questionnaire used to collect the data [35].
It was also interesting to see the prevalence of T&CM use in Nepal, where a wide range of modalities such as Ayurveda, spiritual healers (Dhami-Jhankri), and self-treatment with medicinal plants, have been officially established as a part of traditional medical systems [6]. The results showed that the prevalence of T&CM use is similar to a previous study in Germany (29.0%) [36], Turkey (33.8%) [28], South Korea (37.5%) [37] and India (38.7%) [22]. However, the prevalence of T&CM use in Nepal was lower than those reported in Mongolia (47.9%) [27], and Italy (48.9%) [29]. The potential reasons for variations between the results are the heterogeneity of study designs, such as differences in definitions of T&CM [11, 13, 29], or in sampling strategies that cause selection bias [11, 38]. Another possible explanation may be that cancer patients from resource-limited countries, such as Nepal [39], may not attend cancer treatment facilities [4].
As a part of T&CM, Ayurveda is commonly used in South Asian countries, such as Nepal and India. This is not unexpected, as many patients seek traditional medicine in Nepal and India [7]. Congruent with the results reported in India [25], nearly half of cancer patients using T&CM have taken Ayurveda. In addition, our results showed that the patients with a higher perceived level of disease severity are more likely to practice yoga/meditation and consume honey, ginger and tulsi than the group with lower perceived severity. An interesting key finding was that patients who perceived cancer as serious are more likely to use T&CM. Therefore, we further analyzed how respondents used different T&CM modalities based on their perceived level of disease severity. Unlike general preference, cancer patients with higher self-rated severity were more likely to use yoga, meditation, honey, ginger, and tulsi than the group with lower self-rated severity. The high popularity of natural products can be attributed to the patients’ belief that those modalities are safe [22, 40, 41]. However, natural products are not completely natural and safe in all cases [42]. For example, ginger, which is one of the most widely cultivated herbs in Nepal, is known to be effective for managing chemotherapy-induced nausea [43]; yet, when co-dosed with aprepitant, it is found to aggravate nausea [44, 45]. Therefore, caution should be taken when it is taken concurrently with conventional medicine. Furthermore, the popularity of natural honey consumption among cancer patients suggests that although the health benefits of honey on cancer are well documented [46], further research is required to examine its potential role in alleviating cancer-related symptoms.
Our findings are consistent with previous studies conducted in developing countries [9, 47], which showed that the most commonly reported reasons for cancer patients’ use of T&CM are due to its curative and holistic effects, beliefs in T&CM, and dissatisfaction with conventional medicine [27, 41]. Thus, patients’ perception of T&CM as a cure for cancer [24, 44] is associated with a delay in seeking appropriate cancer treatment, especially in less developed countries with limited health resources [24, 48]. Moreover, a previous study reported the risk of interactions between T&CM and conventional medicine, which may have serious clinical consequences [36]. Therefore, clinicians should be aware of and make patients aware of the potential interactions in developing countries.
Considering the prevalence of T&CM use among cancer patients [13, 27] and T&CM’s potential interactions with conventional medicines [49], physician-patient communication on T&CM use is important. However, T&CM use is rarely discussed with conventional health care providers, and the communication on T&CM use is most likely to be initiated by the patient [50]. Moreover, including this study, patients’ disclosure rates to their physicians were still considerably low, ranging from 40 to 50% [13]. The reason for not disclosing their use to physicians primarily depends on how the patient perceives their physician’s attitude, such as oncologists’ indifference (lack of inquiry) and opposition (fear of physician’s disapproval) towards T&CM [13, 51, 52]. Additionally, the physicians may feel inadequacy in their skills and knowledge to counsel patients on T&CM use [53]. Thus, the physicians should consider patients’ cluster differences in disclosure, their attitude towards T&CM use, and gain cancer patients’ confidence in delivering healthcare services [54].
Similar results have been reported in India [25], where the common source of T&CM information was family and friends. On the other hand, the Western study showed that the media is the primary source of information followed by family and friends [29], whereas a low proportion of cancer patients obtain information on T&CM use from healthcare professionals [27, 55]. Moreover, oncology patients are more likely to continue using T&CM in the hospital setting even though they are uncertain about the efficacy and effectiveness of the non-conventional medicine use [56]. This can be a significant concern for the patients whose use was neither supported by the scientific evidence nor gained the approval from the healthcare professionals [9]. Furthermore, healthcare professionals’ lack of knowledge on T&CM may result in them responding negatively to patients’ use and queries regarding T&CM [57, 58].
As for the information regarding T&CM, the primary sources were informal sources like family, friends, or other patients. The proportion of nonprofessional group in our findings (82.9%) was higher than Indonesia (70.9%) [55], India (67.9%) [59], as well as Australia (77.0%) [60], the United States (60.0%) [61]. While medical personnel accounts for a significant proportion as the source of information in the United States (17.8%) and Australia (39.0%), but in Asia, it is meager like our result (0.7%) or Indonesia (7.3%) [55]. It can be explained by reflecting socio-cultural traditions, which the tradition of “family” in South-East Asia is strong and economic influences [62].
Oncology patients are likely to continue to use T&CM, notwithstanding the lack of scientific knowledge of T&CM or the disapproval from their health professionals [9]. Even though many cancer patients use T&CM, they might not be convinced that their choice is appropriate [56]. Therefore, considering potential issues related to the interaction between T&CM and conventional treatment, it is important to encourage two-way communication between health professionals and patients.
This study shows value in light of the following limitations and strengths. First, as we only evaluated patients who attended hospital settings, which would exclude patients who make do without conventional cancer treatment are not well represented in this study, it might reduce generalizability. Second, in terms of methodology, it is also possible that the use of the face-to-face interview could have influenced the participant’s response, or there may be a recall bias for experience (e.g., discrepancies between what the patient used and remembered as T&CM). Despite these limitations, our findings call for further studies in other Hindu Kush Himalayan countries.
Conclusions
The finding of this study highlights that T&CM is widely used among cancer patients in Nepal. Despite the wide popularity of T&CM use among cancer patients, a lack of consultation and disclosure of T&CM use to healthcare providers suggests a need to raise awareness on the importance of open communication between the patients and the healthcare professionals.
Most commonly used T&CM among Nepali cancer patients include Ayurveda medicine, yoga, and herb/herbal products. The present study also demonstrates the association between T&CM use and the self-rated severity of cancer conditions. Significant differences were found in the preferred T&CM modalities between the group with a higher rating of the perceived disease severity and the group with a lower rating of the perceived severity. Moreover, T&CM users’ primary sources of information are their family members, relatives, and friends, and nearly half of the patients do not inform their physicians of their T&CM use. Given the danger of potential interactions between cancer and T&CM therapies, as well as the limited amount of research in this area that has been conducted to date, it is necessary to systematically evaluate the effectiveness, education, and safety of the use of T&CM. Furthermore, health care providers should stay up to date on the evidence of T&CM use in cancer and investigate the possible effects of T&CM on patients’ prognoses.
Availability of data and materials
The datasets generated and/or analysed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- T&CM:
-
Traditional and complementary medicine
- CCT:
-
Conventional cancer treatment
- IRB:
-
Institutional Review Board
- HKH:
-
Hindu Kush Himalayan
References
Ginsburg O, Bray F, Coleman MP, et al. The global burden of women’s cancers: a grand challenge in global health. Lancet. 2017;389(10071):847–60.
World Health Organization. WHO report on cancer: setting priorities, investing wisely and providing care for all. Geneva: World Health Organization; 2020.
Saud B, Adhikari S, Awasthi M. Cancer burden in Nepal: a call for action. MOJ Proteomics Bioinform. 2018;7(5):278–9.
Hill J, Mills C, Li Q, Smith JS. Prevalence of traditional, complementary, and alternative medicine use by cancer patients in low income and lower-middle income countries. Glob Public Health. 2019;14(3):418–30.
Patwardhan B. Traditional Medicine: A Novel Approach for Available, Accessible and Affordable Health Care. A paper submitted for Regional consultation on Development of Traditional Medicine in the South-East Asia Region. Korea: World Health Organization; 2005.
Thorsen RS, Pouliot M. Traditional medicine for the rich and knowledgeable: challenging assumptions about treatment-seeking behaviour in rural and peri-urban Nepal. Health Policy Plan. 2015;31(3):314–24.
World Health Organization. WHO global report on traditional and complementary medicine 2019: World Health Organization; 2019.
Horneber M, Bueschel G, Dennert G, Less D, Ritter E, Zwahlen M. How many cancer patients use complementary and alternative medicine: a systematic review and metaanalysis. Integr Cancer Ther. 2012;11(3):187–203.
Keene MR, Heslop IM, Sabesan SS, Glass BD. Complementary and alternative medicine use in cancer: a systematic review. Complement Ther Clin Pract. 2019;35:33–47.
Copeland DR, Silberberg Y, Pfefferbaum B. Attitudes and practices of families of children in treatment for cancer. A cross-cultural study. Am J Pediatr Hematol/Oncol. 1983;5(1):65–71.
Ernst E, Cassileth BR. The prevalence of complementary/alternative medicine in cancer: a systematic review. Cancer. 1998;83(4):777–82.
Wang T, Molassiotis A, Chung BPM, Tan JYJBpc. Unmet care needs of advanced cancer patients and their informal caregivers: a systematic review. BMC Palliat Care. 2018;17(1):96.
Davis EL, Oh B, Butow PN, Mullan BA, Clarke S. Cancer patient disclosure and patient-doctor communication of complementary and alternative medicine use: a systematic review. Oncologist. 2012;17(11):1475.
Jones E, Nissen L, McCarthy A, Steadman K, Windsor C. Exploring the use of complementary and alternative medicine in Cancer patients. Integr Cancer Ther. 2019;18:1534735419846986.
Fouladbakhsh JM, Stommel M. Using the Behavioural Model for Complementary and Alternative Medicine: The CAM Healthcare Model. J Complement Integr Med. 2007;4:1–19.
Hwang JH, Kim WY, Ahmed M, Sj C, Jw K, Han DW. The use of complementary and alternative medicine by Korean breast cancer women: is it associated with severity of symptoms? Evid Based Complement Alternat Med. 2015;2015:182475.
Lövgren M, Wilde-Larsson B, Hök J, Leveälahti H, Tishelman CJEJoON. Push or pull? Relationships between lung cancer patients’ perceptions of quality of care and use of complementary and alternative medicine. Eur J Oncol Nurs. 2011;15(4):311–7.
Fouladbakhsh JM, Stommel M, Given BA, Given CW. Predictors of use of complementary and alternative therapies among patients with cancer. Oncol Nurs Forum. 2005;32(6):1115–22.
Tali BA, Khuroo AA, Nawchoo IA, Ganie AH. Prioritizing conservation of medicinal flora in the Himalayan biodiversity hotspot: an integrated ecological and socioeconomic approach. Environ Conserv. 2019;46(2):147–54.
Gewali MB, Awale S. Aspects of traditional medicine in Nepal. Japan: Institute of Natural Medicine University of Toyama; 2008.
Kadayat TM, Bist G, Parajuli A, Karki R, Kaundinnyayana A, Dhami N. Patterns and perception of complementary and alternative medicine use by patients in western Nepal. J Public Health. 2012;20(3):297–303.
Kumar D, Goel NK, Pandey AK, Sarpal SS. Complementary and alternative medicine use among the cancer patients in northern India. South Asian J Cancer. 2016;5(1):8.
Broom A, Wijewardena K, Sibbritt D, Adams J, Nayar K. The use of traditional, complementary and alternative medicine in Sri Lankan cancer care: results from a survey of 500 cancer patients. Public Health. 2010;124(4):232–7.
Chaturvedi P, Chaturvedi U, Sanyal B. Alternative medicine and cancer patients in less developed countries. Lancet Oncol. 2002;3(1):10.
Gupta M, Shafiq N, Kumari S, Pandhi P. Patterns and perceptions of complementary and alternative medicine (CAM) among leukaemia patients visiting haematology clinic of a north Indian tertiary care hospital. Pharmacoepidemiol Drug Saf. 2002;11(8):671–6.
Malik IA, Khan NA, Khan W. Use of unconventional methods of therapy by cancer patients in Pakistan. Eur J Epidemiol. 2000;16(2):155–60.
Oyunchimeg B, Hwang JH, Ahmed M, Choi S, Han D. Complementary and alternative medicine use among patients with cancer in Mongolia: a national hospital survey. BMC Complement Altern Med. 2017;17(1):58.
Üstündag S, Zencirci AD. Complementary and alternative medicine use among cancer patients and determination of affecting factors: a questionnaire study. Holist Nurs Pract. 2015;29(6):357–69.
Berretta M, Della Pepa C, Tralongo P, Fulvi A, Martellotta F, Lleshi A, et al. Use of complementary and alternative medicine (CAM) in cancer patients: an Italian multicenter survey. Oncotarget. 2017;8(15):24401.
Algier LA, Hanoglu Z, Ozden G, Kara F. The use of complementary and alternative (non-conventional) medicine in cancer patients in Turkey. Eur J Oncol Nurs. 2005;9(2):138–46.
Zulkipli AF, Islam T, Mohd Taib NA, Dahlui M, Bhoo-Pathy N, Al-Sadat N, et al. Use of complementary and alternative medicine among newly diagnosed breast Cancer patients in Malaysia: an early report from the MyBCC study. Integr Cancer Ther. 2018;17(2):312–21.
Chow WH, Chang P, Lee SC, Wong A, Shen HM, Verkooijen HM. Complementary and alternative medicine among Singapore cancer patients. Ann Acad Med Singap. 2010;39(2):129–35.
Johnson SB, Park HS, Gross CP, Yu JB. Complementary medicine, refusal of conventional Cancer therapy, and survival among patients with curable cancers. JAMA Oncol. 2018;4(10):1375–81.
Armstrong T, Cohen MZ, Hess KR, Manning R, Lee EL, Tamayo G, et al. Complementary and alternative medicine use and quality of life in patients with primary brain tumors. J Pain Symptom Manag. 2006;32(2):148–54.
Puataweepong P, Sutheechet N, Ratanamongkol P. A survey of complementary and alternative medicine use in cancer patients treated with radiotherapy in Thailand. Evid Based Complement Alternat Med. 2012;2012:670408. https://doi.org/10.1155/2012/670408. Epub 2012 Feb 23.
Firkins R, Eisfeld H, Keinki C, Buentzel J, Hochhaus A, Schmidt T, et al. The use of complementary and alternative medicine by patients in routine care and the risk of interactions. J Cancer Res Clin Oncol. 2018;144(3):551–7.
Kwon JH, Lee S-C, Lee MA, Kim YJ, Kang JH, Kim JY, et al. Behaviors and attitudes toward the use of complementary and alternative medicine among Korean cancer patients. Cancer Res Treat. 2019;51(3):851.
Verhoef MJ, Balneaves LG, Boon HS, Vroegindewey A. Reasons for and characteristics associated with complementary and alternative medicine use among adult cancer patients: a systematic review. Integr Cancer Ther. 2005;4(4):274–86.
Gyawali B, Sharma S, Shilpakar R, Dulal S, Pariyar J, Booth CM, et al. Overview of delivery of cancer care in Nepal: current status and future priorities. JCO Glob Oncol. 2020;6:1211–7.
Kafle G, Bhattarai I, Shrestha AK, Siwakoti M. Why do patients choose to consume Ayurvedic medicines in Nepal? An exploratory study. Int J Ayurvedic Med. 2018;9(4):250–7.
Buckner C, Lafrenie R, Dénommée J, Caswell J, Want D. Complementary and alternative medicine use in patients before and after a cancer diagnosis. Curr Oncol. 2018;25(4):e275.
National Cancer Institute: Complementary and alternative medicine. https://www.cancer.gov/about-cancer/treatment/cam. Accessed 26 June 2020.
Arslan M, Ozdemir L. Oral intake of ginger for chemotherapy-induced nausea and vomiting among women with breast cancer. Clin J Oncol Nurs. 2015;19(5):E92–7.
Greenlee H, Balneaves LG, Carlson LE, Cohen M, Deng G, Hershman D, et al. Clinical practice guidelines on the use of integrative therapies as supportive care in patients treated for breast cancer. JNCI Monogr. 2014;2014(50):346–58.
Zick SM, Ruffin MT, Lee J, Normolle DP, Siden R, Alrawi S, et al. Phase II trial of encapsulated ginger as a treatment for chemotherapy-induced nausea and vomiting. Support Care Cancer. 2009;17(5):563–72.
Othman NH. Does honey have the characteristics of natural cancer vaccine? J Tradit Complement Med. 2012;2(4):276–83.
Truant TL, Porcino AJ, Ross B, Wong M, Hilario C. Complementary and alternative medicine (CAM) use in advanced cancer: a systematic review. Support Oncol. 2013;11(3):105–13.
Mwaka AD, Mangi SP, Okuku FM. Use of traditional and complementary medicines by cancer patients at a national cancer referral facility in a low-income country. Eur J Cancer Care. 2019;28(6):e13158.
Ziemann J, Lendeckel A, Müller S, Horneber M, Ritter CA. Herb-drug interactions: a novel algorithm-assisted information system for pharmacokinetic drug interactions with herbal supplements in cancer treatment. Eur J Clin Pharmacol. 2019;75(9):1237–48.
Roberts CS, Baker F, Hann D, Runfola J, Witt C, McDonald J, et al. Patient-physician communication regarding use of complementary therapies during cancer treatment. J Psychosoc Oncol. 2006;23(4):35–60.
Chang KH, Brodie R, Choong MA, Sweeney KJ, Kerin MJ. Complementary and alternative medicine use in oncology: a questionnaire survey of patients and health care professionals. BMC Cancer. 2011;11(1):196.
Tasaki K, Maskarinec G, Shumay DM, Tatsumura Y, Kakai H. Communication between physicians and cancer patients about complementary and alternative medicine: exploring patients' perspectives. Psychooncology. 2002;11(3):212–20.
Milden SP, Stokols D. Physicians' attitudes and practices regarding complementary and alternative medicine. Behav Med. 2004;30(2):73–84.
Kelak JA, Cheah WL, Safii R. Patient’s Decision to Disclose the Use of Traditional and Complementary Medicine to Medical Doctor: A Descriptive Phenomenology Study. Evid Based Complement Alternat Med. 2018;2018:4735234. https://doi.org/10.1155/2018/4735234.
Almasdy D, Eptiyeni E, Khamri D, Kurniasih N. Use of complementary and alternative medicine (CAM) among breast Cancer patients in a public Hospital in Padang, Indonesia. J Young Pharm. 2018;10(2):S145.
Humpel N, Jones SC. Gaining insight into the what, why and where of complementary and alternative medicine use by cancer patients and survivors. Eur J Cancer Care. 2006;15(4):362–8.
Lua PL. The role of complementary indigenous Malay therapies: perspectives from palliative care patients. J J Complement. 2011;8(1):1–25.
Shorofi SA, Arbon P. Nurses’ knowledge, attitudes, and professional use of complementary and alternative medicine (CAM): a survey at five metropolitan hospitals in Adelaide. Complement Ther Clin Pract. 2010;16(4):229–34.
Pandey L, Pasricha R, Joseph D, Ahuja R, Yanthan Y, Garg PK, et al. Use of complementary and alternative medicine among patients with cancer in a sub-Himalayan state in India: an exploratory study. J Ayurveda Integr Med. 2021;12(1):126–30.
Gillett J, Ientile C, Hiscock J, Plank A, Martin JM. Complementary and alternative medicine use in radiotherapy: what are patients using? J Altern Complement Med. 2012;18(11):1014–20.
Bismark RS, Chen H, Dy GK, Gage-Bouchard EA, Mahoney MC. Complementary and alternative medicine use among patients with thoracic malignancies. Support Care Cancer. 2014;22(7):1857–66.
World Health Organization. Family as centre of health development: Report of the regional meeting, Bangkok, Thailand, 18-20 March 2013. No. SEA-HSD-363. WHO Regional Office for South-East Asia, 2013.
Acknowledgments
The authors would like to express their sincere gratitude to all the participants for their cooperation and willingness to share their experience.
Funding
Research support was provided by a university-funded research program for the publication of an international academic paper at Hanyang University Seoul, Korea (grants number: 201800000001066).
Author information
Authors and Affiliations
Contributions
SJ, SK, and DW were responsible for the study concept and design. DW, SJ, HB, and JH analyzed the data and drafted the manuscript. SJ, SK, HB, DI and DW contributed to the designing of data collection tools and data collection. SJ, SK, HB, JH, DI and DW critically reviewed the manuscript and contributed intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was granted by the Institutional Review Board on Human Subjects Research and Ethics Committees, Hanyang University (HYI-18-164-2). Additional formal permission was approved by Institutional Review Committee at Tribhuvan University (437(6–11) E2 /075/76). Enrollment of the respondents was voluntary, and written informed consent was obtained from all the participants.
Consent for publication
Not applicable.
Competing interests
The authors have no conflicts of interest to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Choi, S.J., Kunwor, S.K., Im, H.B. et al. Traditional and complementary medicine use among cancer patients in Nepal: a cross-sectional survey. BMC Complement Med Ther 22, 70 (2022). https://doi.org/10.1186/s12906-022-03555-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-022-03555-8