
Abstract
Background
The use of complementary and alternative medicine (CAM) is common among cancer patients and it may reflect the individual and societal beliefs on cancer therapy. Our study aimed to evaluate the trends of CAM use among patients with cancer between 2006 and 2018.
Methods
We included 2 Cohorts of patients with cancer who were recruited for Cohort 1 between 2006 and 2008 and for Cohort 2 between 2016 and 2018. The study is a cross-sectional study obtaining demographic and clinical information and inquiring about the types of CAM used, the reasons to use them and the perceived benefits. We compared the changes in the patterns of CAM use and other variables between the two cohorts.
Results
A total of 1416 patients were included in the study, with 464 patients in Cohort 1 and 952 patients in Cohort 2. Patients in Cohort 2 used less CAM (78.9%) than Cohort 1 (96.8%). Cohort 1 was more likely to use CAM to treat cancer compared to Cohort 2 (84.4% vs. 73%, respectively, p < 0.0001,); while Cohort 2 used CAM for symptom management such as pain control and improving appetite among others. Disclosure of CAM use did not change significantly over time and remains low (31.6% in Cohort 1 and 35.7% for Cohort 2). However, physicians were more likely to express an opposing opinion against CAM use in Cohort 2 compared to Cohort 1 (48.7% vs. 19.1%, p < 0.001, respectively).
Conclusion
There is a significant change in CAM use among cancer patients over the decade, which reflects major societal and cultural changes in this population. Further studies and interventions are needed to improve the disclosure to physicians and to improve other aspects of care to these patients.
Similar content being viewed by others


Background
The use of complementary and alternative medicine (CAM) is common in different cultures and among healthy individuals as well as patients with various ailments, especially chronic diseases particularly cancer [1,2,3]. National Centre for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of various medical and health care systems, practices, and products that are not currently thought of as part of conventional medicine [4]. Pattern of CAM use differs according to the socioeconomic status, geography, various religious and spiritual backgrounds [4]. Patients with cancer are well known to use CAM for multiple reasons, driven by the seriousness and the life-threatening nature of the disease and the multiple complex medical psychosocial and emotional problems they are facing. Most cancer patients use alternative medicines as complementary means to help control symptoms. Smaller numbers of patients adopt alternative medicine treatments instead of mainstream therapy [5].
A recent systematic review of studies published between 2009 and 2018 reported about 51% of patients with cancer used CAM to treat the cancer, its complication or improve general health. Younger age, Female patients, higher education and income were characteristics associated with more use [6]. The reported prevalence of CAM use is higher than what reported in an earlier systematic review of studies conducted in 18 countries which also increase in the use over time and variation among countries with highest being in the US and lowest in Italy and Netherland [7].
It is critical to evaluate the CAM use in patients with cancer to understand their needs and help address them but also to prevent any harm form its use. The harms of CAM use may result from patients delaying or avoiding seeking proper cancer treatment leading to increase risk of cancer progression and reduce the chance of cure. On the other hands, CAM may interfere with treatment and reduce its efficacy leading to worse outcome. Furthermore, CAM may result in direct harm to the patients due to its toxicity or interaction with other medications leading to patients suffering in decline in quality of life [8,9,10]. In a large retrospective study of US National Cancer Database including 1,901,815 patients, the use of CAM was associated with refusal of conventional cancer treatment, and with a 2-fold greater risk of death compared with patients who had no complementary medicine use [11].
In Saudi Arabia, earlier studies reported the prevalent use of CAM among Saudi patients with cancer for different reasons varying from treatment and symptom relief to quality of life improvement. The reported CAM used by Saudi cancer patients includes dietary supplements and non-dietary supplement remedies [12]. Even though the use of CAM among cancer patients has some beneficial outcomes, it can lead to some potential risks such as interactions with chemotherapy drugs [13, 14].
These variations have been reported extensively in the past, however, data on trends and changes in CAM use overtime especially among our patients’ population do not exist. Therefore, we have conducted this study to compare CAM use among patients with cancer over 10 years.
Methods
Study design
A cross-sectional study included patients with cancer diagnosis served at the Oncology Department at King Abdulaziz Medical City of Ministry of National Guard Health Affairs, Riyadh, KSA. Ethical approvals for the studies were obtained from the Institutional Review Board at King Abdullah International Medical Research Center, Riyadh, Saudi Arabia. Participants consented before enrollment in the study.
Inclusion criteria
Inclusion criteria allowed enrollment of any patient with a diagnosis of malignancy who is willing to participate in the study and complete the questionnaire.
Tool description
The tool was a survey questionnaire written in a simple fashion and the research coordinator was available to help, in order to ensure that the majority of patients will be able to complete the survey without any difficulties. The questionnaire sought demographic information such as age, gender, education level and disease information such as type of cancer and stage. The type of CAM used, the reasons for use and perceived benefits were captured. Inquiries about diclosure of CAM use to physicians and the physician’s responses were also included.
Data collection
The study population included two cohorts, Cohort 1: patients enrolled between 2006 and 2008 and Cohort 2 patients enrolled between 2016 and 2018. Convenience sampling technique was used in both cohorts. Eligible patients attending the Oncology Clinics at our center were offered to participate in the study and those who consented were enrolled in the study and completed the survey. The findings of some these individual cohorts were published previously describing the tool used for the study and results of individual cohort [12, 15].
Data from both studies were transferred into (excel database), study participants were divided into 2 cohorts based on when the data was collected. Means and proportions of the study population were calculated for study participants, overall and in groups. To determine the patients’ perception characteristics changes associated with the time change, the two cohorts were compared using Chi-squared test or Fisher exact test for categorical factors and t Students’ t-test or Mann-Whitney U Test for continuous variables as appropriate. The level of significance was declared at α = 0.05. Statistical analysis was conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Patients’ characteristics
A total of 1416 patients were enrolled in the study in both cohorts; 464 patients in Cohort 1 and 952 patients in Cohort 2. Patients’ characteristics are detailed in Table 1.
There was no statistical difference between the two cohorts in terms of age, gender, or marital status. However, Cohort 2 included more patients with higher educational levels, higher unemployment, more solid tumors, and more patients who received radiation therapy and stem cell transplant. (Table 1) The increase in the use of stem cell transplant and radiation therapy in the second cohort can be explained by the establishment of these services at our institution at 2010 and 2015, respectively at our institution and patients did not have routine access to them prior to that and were referred to outside facilities.
Lifestyle changes and the use of complementary and alternative medicine
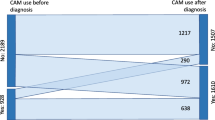
There were fewer patients doing exercise before and after the diagnosis of cancer, more patients who never smoke but fewer patients who quit smoking in Cohort 2 compared to Cohort 1. Furthermore, the use of CAM was significantly less in Cohort 2 (78.89%) compared to the Cohort 1 (96.8%) p < .0001. (Table 2).
More patients reported some CAM-related monthly cost in Cohort 2 compared to Chohort 1 (626 vs 234). However, the approximate cost of the alternative therapy per month was much higher in Cohort 1than Cohort 2 (952 vs 429 Saudi riyals per month, p < .0001. This translates to USD 254 vs USD 115. While this per person per month CAM-related cost, this may be a significant amount of a household income. To put into perspective, that figure may represent between 14 and 32% of a local lower-income household with a monthly income of 3000 Saudi Riyals. Reporting the use of CAM to health care staff (nurse or physician) remains low in both groups. Only 31.6% of Cohort 1 and 35.7% of Cohort 2 reported the use of CAM to their physicians, which is not significantly different (p 0.1513). More physicians opposed to the use of CAM in Cohort 2 (48.7%) compared to only 19.1% in Cohort 1, p < .0001. A similar percentage of patients (8%) delayed standard cancer treatment to try CAM. (Table 2) The low reporting rate to nurses compared to physician could be attributed to language barrier as most nurses are not Arabic speaking.
Reasons for the complementary and alternative medicine use
Patients in Cohort 2 were more likely to report using CAM to control pain, improve appetite, increase strength, enhance immunity, improve mood, and for religious and social beliefs. However, fewer patients in Cohort 2 (73%) used CAM as a treatment for cancer compared to (84.4%) in Cohort 1 p < .0001. (Table 3).
Trends in perceived benefits of complementary and alternative medicine
More patients in Cohort 2 perceived that CAM improved pain control, appetite, and cancer response compared to Cohort 1 in which more patients believed that CAM improved their general condition. More patients in the Cohort 2 believed that the improvement was due to the medical treatment not to CAM. (Table 4).
Trends in specific complementary and alternative medicine use
More patients used herbal mixture, Zamzam water (A holy water found only in Mecca, Saudi Arabia), camel milk, garlic, and multivitamins as well as other herbs and supplication in Cohort 2 compared to Cohort 1 and fewer people used black seeds (Nigella sativa). (Table 5).
There were no differences in the percentage of patients who practiced the Quran recitation in both cohorts.
Discussion
Our study revealed very interesting trends in CAM use by cancer patients as well as their perception about the benefits of CAM. Although the study revealed a reduction in the overall CAM use, there are very noticeable changes in the trend that are worth paying attention to. This trend of reduction in using CAM maybe due to more physician opposing the use of CAM as well as increased awareness of both of the public and the healthcare professionals of the potential harm of some of the CAM, due to interaction with the medications or the inherent side effects of CAM or avoiding getting treatment [16,17,18].
In a serial cross sectional study of 43,644 patients between 1999 and 2014, cancer patients were more likely to use botanical dietary supplements (BDS) compared to others and the overall trend for the whole group was stable, however, the use of BDS declined in certain subgroups such as elderly patients and those with low income and low educational level [19]. Another earlier study showed an increase in the use of CAM among patients with breast cancer [20].
The reason for using CAM to treat cancer decreased significantly with more confidence that the overall improvement in patients’ condition is due to the medical treatment. However, there was a trend to use CAM to manage symptoms such as pain, lack of appetite, fatigue and emotional and mood disturbance; which highlights the importance of the timely implementation of supportive care. The patients use these alternative therapies because they may feel that the usual medical care is not taking care of these symptoms. Interestingly, the impact of social factors and religious beliefs as reasons to use CAM was more apparent in Cohort 2 compared to the Cohort 1 [6, 21].
The perception of CAM benefits in controlling the pain and improving the appetite and contributing to the cancer response was apparent in the second cohort compared to the first. Cohort 1 patients perceived more improvement in their condition which was attributed to CAM, unlike Cohort 2 patients who were more likely to believe that the improvement was due to medical treatment and not to CAM. The trend to have less use of CAM in general and the less CAM use to treat cancer, in particular, may reflect the better education of the patients as well as the social and cultural changes in the society.
The trend in the specific types of CAM used showed that herbal mixture is being used more in the second cohort, however, alternative therapies of religious nature increased significantly such as the use of Zamzam water or water with Quran recited on it. The use of supplication increased significantly, while Quran recitation did not change. Black seeds consumption was less in the second cohort as well as olive oil. However, there was an increase in the use of multivitamins, garlic and camel milk. This reflects the continued impact of religious background on these practices because camel milk, Zamzam water and the water with the Quran recited on it are all of the religious backgrounds.
The use of herbal and plant products such as olive oil and black seeds originate from religious background and reported to be used by Muslim patients in different countries especially in Saudi Arabia. The use of these products may reach up to 68% of the patients. Olive oil can be ingested or used externally by rubbing it on the skin [22,23,24,25].
Zamzam water is a holy water that is found in the Holy city of Mecca and used based of the belief in its healing and spiritual properties and its ingestion was reported by authors from different countries [26,27,28].
The level of exercise before the illness or after the illness is much less in the second cohort. In addition, more people smoked in the second cohort with less likelihood to quit after diagnosis compared to the first cohort. There is a considerable number of patients delaying their cancer treatment to give a chance for the CAM to work. This may expose the patients to harm from disease progression or complication that deserves further investigation and implementation of remedial measures.
Interestingly, the majority of patients do not divulge to their physicians their use of CAM. In a systemic review of 21 studies, 20–90% of the patients did not disclose their use of CAM to the providers for many reasons, including lack of inquiry from physicians or anticipation of doctors disapproval among others [29]. Interestingly, in our study, more physicians seem to be opposing to CAM use with the second cohort. The low reporting rate highlights the need to educate the patients about the importance of disclosing to and encouraging the healthcare team to systematically inquire about the use of CAM in a very proactive way and not to count on the voluntary reports of the patient.
Although our study revealed significant change in the prevalence and pattern of CAM use over a decade; however, the reasons for these changes were not addressed in our study especially the impact of social media and the cultural transformation of the whole society. There are multiple factors, which might have contributed to these changes, such as the different levels of education and the type of cancer and treatment received. The fact that the second cohort are more educated with more solid malignancies and receiving more radiation therapy and stem cell transplant can not be ignored. However, these cannot be taken in isolation from the larger societal changes. Further studies are needed to investigate the reasons that prevented non-CAM users from doing so.
Conclusion
Although there was a reduction in its use, majority of patients still using some kind of CAM. The reasons for the use require further investigation as it may reflect gaps in the healthcare delivery which is not addressing all patients needs. Disclosure of CAM use for healthcare professionals remains a concern that need to be addressed systematically.
Availability of data and materials
Data and material are available.
Abbreviations
- CAM:
-
Complementary Alternative Medicine
- NCCAM:
-
National Centre for Complementary and Alternative Medicine
- BDS:
-
Botanical dietary supplements
References
Harris PE, Cooper KL, Relton C, Thomas KJ. Prevalence of complementary and alternative medicine (CAM) use by the general population: a systematic review and update. Int J Clin Pract. 2012;66(10):924–39. https://doi.org/10.1111/j.1742-1241.2012.02945.x.
Paul M, Davey B, Senf B, Stoll C, Münstedt K, Mücke R, et al. Patients with advanced cancer and their usage of complementary and alternative medicine. J Cancer Res Clin Oncol. 2013;139(9):1515–22. https://doi.org/10.1007/s00432-013-1460-y.
Kumar D, Goel NK, Pandey AK, Sarpal SS. Complementary and alternative medicine use among the cancer patients in northern India. South Asian J Cancer. 2016;5(1):8–11. https://doi.org/10.4103/2278-330X.179689.
Gupta D, Batra R, Mahajan S, Bhaskar DJ, Jain A, Shiju M, et al. Comparative evaluation of the complementary and alternative medicine therapy and conventional therapy use for musculoskeletal disorders management and its association with job satisfaction among dentists of West India. J Tradit Complement Med. 2014;4(4):263–7. https://doi.org/10.4103/2225-4110.126632.
Cassileth BR, Chapman CC. Alternative and complementary cancer therapies. Cancer Interdiscip Int J Am Cancer Soc. 1996;77(6):1026–34.
Keene MR, Heslop IM, Sabesan SS, Glass BD. Complementary and alternative medicine use in cancer: a systematic review. Complement Ther Clin Pract. 2019;35:33–47. https://doi.org/10.1016/j.ctcp.2019.01.004.
Horneber M, Bueschel G, Dennert G, Less D, Ritter E, Zwahlen M. How many cancer patients use complementary and alternative medicine: a systematic review and metaanalysis. Integr Cancer Ther. 2012;11(3):187–203. https://doi.org/10.1177/1534735411423920.
Drozdoff L, Klein E, Kalder M, Brambs C, Kiechle M, Paepke D. Potential interactions of biologically based complementary medicine in gynecological oncology. Integr Cancer Ther. 2019;18:153473541984639. https://doi.org/10.1177/1534735419846392.
Jermini M, Dubois J, Rodondi PY, Zaman K, Buclin T, Csajka C, et al. Complementary medicine use during cancer treatment and potential herb-drug interactions from a cross-sectional study in an academic Centre. Sci Rep. 2019;9(1):1–11. https://doi.org/10.1038/s41598-019-41532-3.
Firkins R, Eisfeld H, Keinki C, Buentzel J, Hochhaus A, Schmidt T, et al. The use of complementary and alternative medicine by patients in routine care and the risk of interactions. J Cancer Res Clin Oncol. 2018;144(3):551–7. https://doi.org/10.1007/s00432-018-2587-7.
Johnson SB, Park HS, Gross CP, Yu JB. Complementary medicine, refusal of conventional Cancer therapy, and survival among patients with curable cancers. JAMA Oncol. 2018;4(10):1375–81. https://doi.org/10.1001/jamaoncol.2018.2487.
Jazieh AR, Al Sudairy R, Abulkhair O, et al. Use of complementary and alternative medicine by patients with cancer in Saudi Arabia. J Altern Complement Med. 2012;18(11):1045–9. https://doi.org/10.1089/acm.2011.0266.
Loquai C, Dechent D, Garzarolli M, Kaatz M, Kaehler KC, Kurschat P, et al. Risk of interactions between complementary and alternative medicine and medication for comorbidities in patients with melanoma. Med Oncol. 2016;33(5):52. https://doi.org/10.1007/s12032-016-0764-6.
Sweet E, Dowd F, Zhou M, Standish LJ, Andersen MR. The use of complementary and alternative medicine supplements of potential concern during breast cancer chemotherapy. Evidence-Based Complement Altern Med. 2016;2016:1–8. https://doi.org/10.1155/2016/4382687.
Abuelgasim KA, Alsharhan Y, Alenzi T, Alhazzani A, Ali YZ, Jazieh AR. The use of complementary and alternative medicine by patients with cancer: a cross-sectional survey in Saudi Arabia. BMC Complement Altern Med. 2018;18(1):88. https://doi.org/10.1186/s12906-018-2150-8.
Chotipanich A, Sooksrisawat C, Jittiworapan B. Association between complementary and alternative medicine use and prolonged time to conventional treatment among Thai cancer patients in a tertiary-care hospital. PeerJ. 2019;7:e7159. https://doi.org/10.7717/peerj.7159.
Knecht K, Kinder D, Stockert A. Biologically-based complementary and alternative medicine (CAM) use in Cancer patients: the good, the bad, the misunderstood. Front Nutr. 2020;6:196. https://doi.org/10.3389/fnut.2019.00196.
Mohd Mujar NM, Dahlui M, Emran NA, et al. Complementary and alternative medicine (CAM) use and delays in presentation and diagnosis of breast cancer patients in public hospitals in Malaysia. Lafrenie RM, ed. PLoS One. 2017;12(4):e0176394. https://doi.org/10.1371/journal.pone.0176394.
Li C, Hansen RA, Chou C, Calderón AI, Qian J. Trends in botanical dietary supplement use among US adults by cancer status: the National Health and nutrition examination survey, 1999 to 2014. Cancer. 2018;124(6):1207–15. https://doi.org/10.1002/cncr.31183.
HS OF, Zick SM. Trends in complementary/alternative medicine use by breast cancer survivors: comparing survey data from 1998 and 2005. BMC Womens Health. 2007;7(1):1–7. https://doi.org/10.1186/1472-6874-7-4.
Sun Y, Wang R, Tang W, Li C, Huo N. Trends and factors of botanical dietary supplement use among US adults with COPD from 1999 to 2016. PLoS One. 2020;15(9 September). https://doi.org/10.1371/journal.pone.0239674.
Al Sudairy R, Al Omari A, Jarrar M, et al. Complementary and alternative medicine use among pediatric oncology patients in a tertiary care center, Riyadh, Saudi Arabia. J Clin Oncol. 2011;29(15_suppl):e20003. https://doi.org/10.1200/jco.2011.29.15_suppl.e20003.
Alrowais NA, Alyousefi NA. The prevalence extent of complementary and alternative medicine (CAM) use among Saudis. Saudi Pharm J. 2017;25(3):306–18. https://doi.org/10.1016/j.jsps.2016.09.009.
Akhu-Zaheya LM, Alkhasawneh EM. Complementary alternative medicine use among a sample of Muslim Jordanian oncology patients. Complement Ther Clin Pract. 2012;18(2):121–6. https://doi.org/10.1016/j.ctcp.2011.10.003.
Ahmad R, Ahmad N, Naqvi AA, Shehzad A, Al-Ghamdi MS. Role of traditional Islamic and Arabic plants in cancer therapy. J Tradit Complement Med. 2017;7(2):195–204. https://doi.org/10.1016/j.jtcme.2016.05.002.
Hamidah A, Rustam ZA, Tamil AM, Zarina LA, Zulkifli ZS, Jamal R. Prevalence and parental perceptions of complementary and alternative medicine use by children with cancer in a multi-ethnic southeast Asian population. Pediatr Blood Cancer. 2009;52(1):70–4. https://doi.org/10.1002/pbc.21798.
Mohieldin A, Eldali A, Aljubran A. Knowledge, perception, and attitudes of cancer patients towards cancer and cancer care: local perspective from Saudi Arabia. J Cancer Educ. 2017;32(2):314–9. https://doi.org/10.1007/s13187-015-0973-2.
Rahou BH, El RK, Hanchi Z, Ouasmani F, Benazzouz B, Mesfioui A. Self-reported use of complementary and alternative medicine among moroccan women with breast cancer. Cancer Oncol Res. 2017;5(1):1–9. https://doi.org/10.13189/cor.2017.050101.
Davis EL, Oh B, Butow PN, Mullan BA, Clarke S. Cancer patient disclosure and patient-doctor communication of complementary and alternative medicine use: a systematic review. Oncologist. 2012;17(11):1475–81. https://doi.org/10.1634/theoncologist.2012-0223.
Acknowledgements
NA
Funding
There is no funding for this study.
Author information
Authors and Affiliations
Contributions
ARJ: conceptualizing the idea, writing and reviewing the manuscript. KA: writing and reviewing the manuscript. MK: data management, writing and reviewing the manuscript. HA: statistical analysis, writing and reviewing the manuscript. OBD: reviewed the method and reviewing the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the International Review Board in King Abdullah International Medical Research Center with reference number RC16/165/R. Patients signed the consent forms prior to their participation in the study.
Consent for publication
Its not applicable in our institution since we have IRB approval.
Competing interests
There is no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jazieh, A.R., Abuelgasim, K.A., Ardah, H.I. et al. The trends of complementary alternative medicine use among cancer patients. BMC Complement Med Ther 21, 167 (2021). https://doi.org/10.1186/s12906-021-03338-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-021-03338-7