
Abstract
Background
The Thai traditional herbal formula–Mathurameha, consisting of 26 medicinal plants, has been used as an alternative and complementary medicine for diabetes treatment in Wangnamyen Hospital, Thailand. To provide scientific evidences on the efficacy and safety of this herbal formula, in vivo hypoglycaemic activity, effect on serum biochemical profiles and acute toxicity were investigated.
Methods
Experimental type 2 diabetes was induced in male Sprague-Dawley rats by intraperitoneal injection of nicotinamide 15 min prior to intravenous injection of streptozotocin. The most effective extract from the oral glucose tolerant test (OGTT) was administered daily via the oral route to diabetic rats for 2 weeks. Two-hour postprandial plasma glucose (2h–PPG) levels were measured on days 0, 7, and 14. Biochemical data were measured at the end of daily oral administration experiment.
Results
Aqueous extract of the herbal formula was the most potent extract for improving glucose tolerance of streptozotocin-nicotinamide-induced diabetic rats after single oral administration. After 2 weeks of daily oral administration, the aqueous extract showed a dose-dependent glucose lowering effect. At doses of 12.5, 25, and 50 mg/kg, the 2h–PPG level of diabetic rats decreased by 3.32%, 15.78%, and 17.94%, respectively. Most of the biochemical profiles of diabetic rats were improved, including the total cholesterol (TC), alkaline phosphatase (ALP), total protein, albumin, globulin, creatinine, and uric acid levels. The significantly increased triglyceride (TG) level observed in treated diabetic rats indicated a lack of a beneficial effect of the extract on lipid homeostasis. Nevertheless, there were no signs or symptoms of acute toxicity observed after oral administration of aqueous extract (5 g/kg) to both male and female rats.
Conclusions
The results revealed that the herbal formula aqueous extract has hypoglycaemic activity, beneficial effects on biochemical profiles and a lack of acute toxicity. This study confirms the efficacy and safety of the Mathurameha herbal formula used for treating type 2 diabetes mellitus.
Similar content being viewed by others

Background
Diabetes mellitus (DM), a chronic metabolic disorder that is characterized by hyperglycaemia, continues to be a major health problem with that has seen a great increase in worldwide incidence due to behaviour and lifestyle changes [1]. In Thailand, there has been a rising trend in the hospitalization rate for patients with diabetes over the last decade, from 380.8 in 2003 to 1081.2 per 100,000 persons in 2013 [2]. Due to high cost of medical care and required treatments with long-term healing, diabetes is considered to be an economic burden and national public health problem that is of great concern [3]. According to the failure of conventional hypoglycaemic drugs to satisfactorily maintain normal glucose levels and some serious side effects [4,5,6], significant interest in alternative and complementary medicine, especially herbal preparations, has been maintained [7, 8].
Mathurameha, a Thai traditional herbal formula established by Nirund Pongsoiphet and Foundation for the promotion of Thai Traditional Medicine Formula, has long been used by Ayuravedic (Chevagakomarapat) school to treat diabetes mellitus for more than 30 years. In recent years, it has been used as a complementary treatment for type 2 diabetes mellitus in Wangnamyen Community Hospital, Sa kaeo province [9]. The oral dosage form (350 mg capsule) of this herbal formula contains dried powder of 26 medicinal herb combinations (Table 1 ).
From previous studies, in vivo hypoglycaemic effects of 12 component herbs have been reported [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32], and 8 component herbs have been studied for their hypoglycaemic actions, including α-glucosidase inhibitory activity [30, 31, 33,34,35,36,37,38], inhibition of glucose absorption [17], stimulation of insulin secretion from pancreatic β-cells [17, 24, 29, 39], stimulation of glucose uptake to fat and muscle cells [18, 40,41,42,43,44], normalization of hepatic glucose output and glycogen synthesis [19, 43]. Twelve active hypoglycaemic compounds have been identified — these include andrographolide from Andrographis paniculata (Burm.f.) Nees [30, 45]; corosolic acid [36] and lagerstroemin [41, 42] from Lagerstroemia speciosa (L.) Pers; salacinol and kotalanol from Salacia chinensis (L.) [31]; gallic acid from Terminalia bellirica (Gaertn.) Roxb. [21]; chebulanin, chebulagic acid and chebulinic acid from Terminalia chebula Retz. [34]; and borapetoside C [35, 43] and borapetol B [39] from Tinospora crispa (L.) Hook.f. & Thomson. Therefore, the hypoglycaemic effects as well as the mechanism of actions of this anti-diabetic herbal formula are worth investigating.
Because of the high oral solid dosage form of this formula (5 capsules twice daily) as well as the unappreciable taste of the decoction, development of a preparation based on traditional knowledge might be helpful to reduce the administration dose [46]. Therefore, a comparison between the hypoglycaemic effects of the dried powder and extracts of the whole formula is needed to confirm the efficacy of the extract and to examine the most suitable extraction method. Although this herbal formula has already been used in diabetic patients without any sign or symptom of toxicity [9], the toxicity study of the whole formula extract remains necessary to ensure its safety for further usage.
The aims of this study are to observe the in vivo hypoglycaemic activity, effects on biochemical profiles as well as acute toxicity of the whole formula extracts to provide scientific evidence of its efficacy and safety, which might be useful for the further development of this herbal drug as well as for treating diabetes patients with fewer undesirable side effects.
Methods
Chemicals
Nicotinamide, o-dianisidine, PGO enzyme and streptozotocin (STZ) were purchased from Sigma Chemical Co. (St Louis, MO, USA); Glibenclamide tablets (Daonil) were purchased from Aventis Pharma Ltd. (Bangkok, Thailand). All other chemicals and reagents were of analytical grade.
Plant materials
Commercial crude drug specimens of 26 single herbs were sampled from dried plant materials, which were used in Wangnamyen Hospital from February 2012 to November 2013. All of the drug specimens were deposited at the Department of Pharmaceutical Botany, Faculty of Pharmacy, Mahidol University (Crude drug’s no. are shown in Table 1). The commercial crude drug specimens of each herb were verified their scientific names by comparing the microscopic characteristics and thin-layer chromatographic fingerprints to the authentic crude drug specimens.
Authentic crude drug specimens of 17 herbs were collected from different locations in Thailand. All of the authentic specimens were identified according to the standard botanical literature and compared with specimens of the herbarium collection at the Forest Herbarium (BKF), Department of National Parks, Wildlife and Plant Conservation. Then, they were deposited at Mahidol University Herbarium (PBM), Department of Pharmaceutical Botany, Faculty of Pharmacy, Mahidol University. The authentic specimens of 7 herbs were collected from Queen Sirikit Botanic Garden (QSBG) under the regulations for accessing biological resources, while the other 2 authenticated crude drugs were gifts from from Assoc. Prof. Weena Jiratchariyakul. The voucher numbers of all of the authentic specimens are shown in Table 1.
Derris reticulata and Homalomena aromatica reproductive parts were not collected. As a result, they were identified by comparing the characteristics of their vegetative parts with the standard botanical literature as well as an organoleptic examination compared with a Thai traditional medicine textbook [47]. The crude drug, Samo thet, was considered to be a member of Terminalia genus according to its fruit characteristics [48].
Extractions
Crude drugs of 26 single herbs were mixed and ground together. The whole formula powder was then separately extracted by 3 different solvents — 80% ethanol, 50% ethanol, or water. Ethanolic extracts were achieved by percolation; the miscella was dried by a rotary evaporator. The percentage yield of 80% ethanol and 50% ethanol extracts were 24.57% and 28.12% dry weight, respectively. Aqueous extract was derived from a decoction of the powdered mixture (1 kg) by soaking with water for 30 min and then boiling at 100 °C for 30 min. The decoction was filtered through gauze and dried by a spray dryer, yielding 14.73% dry weight. All extracts were kept in closed containers at 4 °C until use.
Animal maintenance
Sprague-Dawley rats (105 male and 5 female rats), weighting 120–150 g, were purchased from the National Laboratory Animal Centre (NLAC), Mahidol University, Thailand. They were housed in an air conditioned room (22–25 °C) and subjected to a 12-h light/dark cycle for at least 1 week prior to the experiment. The animals were given free access to a pellet diet and water ad libitum. The animal protocol was approved by the Animal Care and Used Committee, Faculty of Pharmacy, Mahidol University, Thailand (PYT008/2555).
Induction of experimental diabetes
Experimental type 2 diabetes was induced in rats using the method in Masiello et al. [49], with a slight modification. Overnight fasted male rats were intraperitoneally injected with 80 mg/kg nicotinamide 15 min before a single intravenous injection of 65 mg/kg streptozotocin (STZ). The urine glucose levels were checked weekly with a urine glucose strip. Three weeks after induction, the 6-h fasting plasma glucose (FPG) levels were examined, and the rats that had a FPG level greater than 160 mg/dL were used in further experiments.
In vivo hypoglycaemic experiments
Effect on oral glucose tolerance of normal and diabetic rats
The dosages of all of the extracts (mg/kg by weight) used in this study were calculated from the percent yield of extractions equivalent to 350 mg of the dry powdered mixture. All of the extracts and glibenclamide were dissolved in distilled water. The ethanolic extracts were then sonicated for 15 min. The dry powdered mixture was suspended in distilled water with vigorous stirring and was immediately given to the rats.
Overnight fasted normal male rats were randomly divided into 6 experimental groups with 5 rats per group. The oral glucose tolerant test (OGTT) was performed according to Peungvicha et al. [50]. Blood samples of all rats were collected by drawing from the tail vein, and each group was immediately given oral treatments (assigned as −30 min) as follows:
Group 1: distilled water (negative control).
Group 2: glibenclamide, 5 mg/kg.
Group 3: 80% ethanol extract, 87.5 mg/kg.
Group 4: 50% ethanol extract, 98 mg/kg.
Group 5: aqueous extract, 50 mg/kg.
Group 6: powdered mixture suspension, 350 mg/kg.
Thirty minutes later (assigned as 0 min), blood samples were collected and glucose (1.25 g/kg b.w.) was immediately given to all rats by oral administration. After glucose loading, blood samples were collected every 30 min until 150 min. The plasma glucose level of each time point was examined by the glucose oxidase method.
Diabetic rats were fasted 6 h prior to the experiment and were randomly divided into 6 experimental groups (5 rats per group), which were then treated with the same treatment as normal rats. The OGTT experiment was performed with the same protocol as that explained above. The most effective extract was selected for further experiments.
Effects on the postprandial plasma glucose levels
STZ-nicotinamide-induced diabetic rats were randomly divided into 8 experimental groups, with 5 rats per group. Each group was daily orally given with distilled water, glibenclamide, various doses of aqueous extract or powdered mixture suspension for 2 weeks as follows:
Group 1: distilled water (diabetic control).
Group 2: glibenclamide, 5 mg/kg b.w.
Group 3–5: aqueous extract, 12.5, 25, and 50 mg/kg.
Group 6–8: powdered mixture suspension, 87.5, 175, and 350 mg/kg.
Two-hour postprandial plasma glucose (2h–PPG) levels were determined on days 0 (the day before oral administration started), 7, and 14. Blood samples were collected from the tail vein after 2 h of fasting and were examined for the plasma glucose level by the glucose oxidase method. The rats were weighted on days 0, 7 and 14 to adjust the treatment doses [18].
Effect on the serum biochemical profiles of diabetic rats
At the end of the 2-week daily oral administration and postprandial plasma glucose experiment, each rat was euthanized prior to blood sample drawing from the heart. The blood samples were centrifuged at 5000 rpm for 10 min; then, blood serum was separated. All serum samples were kept at −20 °C until further examinations. Diabetic rats that were orally given distilled water served as the ‘diabetic control’ group, while normal rats that received oral administration of distilled water served as the ‘normal control’ group.
The biochemical profiles, including alanine transferase (ALT), aspartate transferase (AST), alkaline phosphatase (ALP), total protein, albumin, globulin, blood urea nitrogen (BUN), creatinine, uric acid, total cholesterol (TC) and triglycerides (TG), were measured by National Laboratory Animal Centre (NLAC), Mahidol University, Thailand.
Acute toxicity
The aqueous extract and powdered mixture suspension that dissolved in distilled water was orally administered to male and female rats (n = 5 in each sex) at a dose of 5 g/kg. The animals were observed at least once during the first 30 min and periodically during the first 24 h following a standard behavioural, neurologic, and autonomic animal profile. Afterwards, they were observed daily for a total of 14 days for any indication of illness or death. Food and water were provided ad libitum.
Statistical analysis
The distribution of data was analysed by Komogorov-Smirnof’s normality test. The datasets with a normal distribution were then analysed by one-way ANOVA and/or Student’s t-test. The datasets with an abnormal distribution were analysed by the Mann-Whitney test. A p-value less than 0.01 and/or 0.05 indicated a significantly difference.
Results
Effects on the oral glucose tolerance of normal and diabetic rats
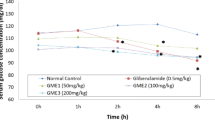
The effects of the whole formula powder and extracts on the oral glucose tolerance of normal rats are shown in Fig. 1a. The plasma glucose level of all of the extract treated groups was not different from that of the control group while the glibenclamide-treated group showed a significant decrease in plasma glucose levels at 90–150 min after glucose administration. In diabetic rats, whole formula powder and extracts improved their glucose tolerance, as shown in Fig. 1b.

Effects of the whole formula powder and extracts on oral glucose tolerance of a normal rats and b diabetic rats (N = 5); *Significant different from control group (p < 0.05; Student’s t-test); Data were expressed as mean ± S.E
Both ethanolic extracts (80% and 50% ethanol extracts) and powdered mixture suspensions showed a similar potency in lowering the plasma glucose levels. Aqueous extract significantly lowered the plasma glucose levels of treated rats at 60–120 min after glucose administration, as well as after glibenclamide administration, compared to the control group. Therefore, aqueous extract was selected for further experiments [51].
Effects on the postprandial plasma glucose levels
After 1-week of daily oral administration, diabetic rats treated with 50 mg/kg aqueous extract showed a significant decrease in the 2-hour postprandial plasma glucose (2h–PPG) level of 19.96%, while the other doses had no effects on the 2 h–PPG levels. After 2 weeks, aqueous extract at doses of 12.5, 25 and 50 mg/kg decreased the 2h–PPG levels of diabetic rats in a dose-dependent manner by 3.32%, 15.78% and 17.94%, respectively [51]. However, the effects of equivalent doses of the powdered mixture suspension did not correspond to aqueous extract due to the lack of a dose-dependent pattern.
After a significant increase in the 2h–PPG level by 31.97% in the first week, 350 mg/kg powdered mixture suspension slightly decreased the 2h–PPG levels of rats after 2-weeks of administration. At a dose of 175 mg/kg, the 2h–PPG levels of diabetic rats were not changed in the first week; instead, they were slightly increased in the second week. The two-hour PPG levels of diabetic rats treated with 87.5 mg/kg powdered mixture suspension were slightly increased in the first week, but they were significant decreased by 10.26% in the second week (Fig. 2).

Effect of herbal formula aqueous extract and powder on 2-h postprandial plasma glucose (2h–PPG) levels of STZ-induced diabetic rats (N = 5); *Significant different from control group of each week; #Significant different from glibenclamide group of each week (p < 0.05; Mann-Whitney); Data were expressed as mean ± S.E.
Effects on the serum biochemical profile of diabetic rats
The results from serum biochemical profiles determinations are shown in Table 2. Data were expressed as the mean ± S.D. of each group.
Effects on lipid profiles
Aqueous extract at a dose of 25 mg/kg significantly decreased the total cholesterol (TC) level of diabetic rats (15.8%), while 50 mg/kg of the extract slightly decreased the TC level (7.05%) compared to the diabetic control. The whole formula powder had no effect on the TC level of diabetic rats. Both aqueous extract and the whole formula powder increased the triglycerides levels of diabetic rats compared to normal controls.
Effects on the liver function
Aqueous extract at doses of 12.5 and 25 mg/kg significantly lowered the serum level of alkaline phosphatase (ALP) (46.7% and 41.8%, respectively), while 50 mg/kg slightly, but not significantly, lowered the level (29.0%) of diabetic rats compared with the diabetic control group. The serum levels of alanine transferase (ALT) and aspartate transferase (AST) in the diabetic control group were not significantly different from those of the normal control group. However, aqueous extract at a dose of 25 mg/kg significantly decreased the ALT level and slightly decreased the AST levels of diabetic rats. Aqueous extract at a dose of 12.5 mg/kg and the powdered mixture suspension at a dose of 175 mg/kg significantly increased the total protein and albumin and slightly increased the globulin levels of diabetic rats compared to diabetic controls.
Effects on the renal function
The serum levels of blood urea nitrogen (BUN), creatinine, and uric acid of diabetic rats were significantly higher than those of the normal control group. The herbal formula had no effect on the BUN level of treated diabetic rats. By contrast, the serum creatinine and uric acid levels of diabetic rats treated with both aqueous extract and powdered mixture suspension significantly decreased to normal levels.
Acute toxicity
Aqueous extract and powdered mixture suspension, at a dose of 5 g/kg, when given to male and female rats, showed no effect on their behavioural, neurologic, and autonomic profiles during the 24 h observation periods. No mortality was observed for up to 14 days of monitoring. The value of the lethal dose at 50% of the extract in rats was estimated to be more than 5 g/kg.
Discussion
In this study, diabetes in rats was induced by a streptozotocin-nicotinamide injection. Streptozotocin (STZ) has toxic effects on pancreatic β-cells based on its potent alkylating properties, which are related to cell death induction. STZ generates reactive oxygen species and acts as a nitric oxide donor, which contributes to DNA fragmentation and caused other changes that resulted in the destruction of pancreatic islet cells [52, 53]. The administration of suitable dosages of nicotinamide partially protects β-cells from the cytotoxic effect of STZ. Therefore, the diabetes syndrome induced in this experiment appears to be closer to human type 2 diabetes in that it demonstrated a significant response to glucose and sensitivity to sulfonylureas, a class of hypoglycaemic drug [49]. These drugs, including glibenclamide, stimulate insulin secretion from pancreatic β-cells by closing the ATP-dependent potassium channel (KATP) [54].
The oral glucose tolerance test (OGTT), which examines changes in the plasma glucose levels in response to oral glucose administration, has long been used clinically for diabetes mellitus diagnosis and in research to evaluate the effectiveness of hypoglycaemic agents [17]. In the present study, the OGTT was employed in a single dose administration experiment to determine the plasma glucose lowering effects of the Mathurameha herbal formula and its extracts at the same equivalent dose of 350 mg/kg in both normal and diabetic rats.
In normal rats, the plasma glucose levels of all of the treated groups and the untreated control group at every time point after glucose administration were the same. This indicates that the herbal formula did not alter blood glucose regulation in normoglycaemic conditions. However, the hypoglycaemic effects of the herbal formula were observed in diabetic rats. A single dose of aqueous extract (50 mg/kg) exhibited outstanding plasma glucose lowering effects in diabetic rats (Fig. 1 ). The results suggested that the major components that possessed hypoglycaemic activity of this herbal formula could be polar compounds, which are soluble in water. Daily oral administration of various doses of aqueous extract to diabetic rats revealed that a dose of 50 mg/kg exhibited the most potent glucose lowering effect and lowered 2-hour postprandial plasma glucose (2h–PPG) level after a 1-week administration, and this effect remained after 2-week administration. While the powdered mixture suspension showed a non-dose dependent glucose lowering effect, aqueous extract exhibited this effect in a dose-dependent manner after 2 weeks (Fig. 2 ), possibly because of the difference in the intestinal absorption of actively hypoglycaemic components. In the powdered mixture suspension, the active components that are covered by plant cell wall lead to low consistency in intestinal absorption. By contrast, the active components in aqueous extract are more available for absorption, resulting in high consistency in intestinal absorption. Aqueous extract is preferred for developing an herbal drug formulation for diabetes treatment.
Furthermore, previous reports showed that aqueous extract of medicinal plants, including Abutilon indicum [17, 28], Derris reticulata [20], Lagerstroemia speciosa [16, 55], Orthosiphon aristatus [29], Solanum trilobatum [14], Terminalia chebula [23], and Tinospora crispa [24], which are the components of this herbal formula, have in vivo hypoglycaemic effects. It has been reported that Lagerstroemia speciosa contains polar active compounds, including ellagitannins, such as lagerstroemin and ellagic acid derivatives, which could stimulate glucose uptake into 3T3-L1 adipocytes [40,41,42]. Ellagitanins from Terminalia chebula including chebulanin, chebulagic acid, and chebulinic acid, have been reported to have inhibitory effects against α-glucosidase [34]. Boropetoside C, which was isolated from Tinospora crispa, also showed α-glucosidase inhibitory effects [35], increased glucose utilization in peripheral tissues, and reduced hepatic gluconeogenesis [43]. Therefore, it is suggested that these compounds might contribute to the hypoglycaemic effects of this herbal formula aqueous extract.
In this study, an increase in the serum level of total cholesterol (TC) triglycerides (TG) was observed in diabetic rats. The elevation of the TC and TG levels in circulation could be due to the increase in cholesterogenesis, fatty acid uptake, and deposit as triglycerides in the liver [56, 57]. The altered TC levels were significantly restored to normal values by aqueous extract (25 mg/kg) treatment (Table 2 ). The extract might have hypocholesterolomic effects with clearance elevation and reduction of endogenous cholesterol production [57, 58]. However, an increase in the serum TG level was observed in diabetic rats that were treated with extract (Table 2 ). This indicates that the formula failed to reduce TG production and could not control mobilization of triglycerides from the liver to circulation [59].
Liver enzymes, including AST, ALT, and ALP, in circulation that were investigated in this study are indicators of hepatic damage as they are released into the bloodstream after cell membrane damage reflecting hepatocellular necrosis [57, 60, 61]. However, the serum AST and ALT levels of the diabetic rats used in this study were not significantly different from those of the normal control group (Table 2 ). This might be due to the protection of nicotinamide against the hepatotoxic effects of STZ [62, 63]. Moreover, the significant decrease in the ALT levels in the 25 mg/kg aqueous extract treated group might be from the gluconeogenesis inhibitory effects of the extract [64]. Nevertheless, the serum ALP levels of the diabetic control group were significantly increased, indicating leakage from liver damage. A decline in the serum ALP levels was observed in the diabetic groups that were treated with aqueous extract (12.5 and 25 mg/kg) (Table 2 ). This revealed that the extract could reduce the leakage of liver enzymes into the bloodstream.
The decline of plasma proteins in diabetes, albumin and globulin, which are mainly synthesized by the liver, might be from the augmentation of protein catabolism or microproteinuria, indicators of diabetic nephropathy [64]. This study demonstrated that the serum total protein, albumin, and globulin levels of diabetic rats were significantly lower than those of the normal control group. The significant increase in these serum proteins was observed in diabetic groups that were treated with the 12.5 mg/kg aqueous extract (Table 2 ). These results are in agreement with decreasing the serum ALP levels by aqueous extract, indicating the protective effects of herbal formulas against liver damage that are associated with hyperglycaemia. Considering the evidence implicating diabetes mellitus in hepatic dysfunction, this hepatoprotective effect may be due to the hypoglycaemic effects of the whole formula aqueous extract investigated in this study [65].
Diabetic hyperglycaemia induces elevation of serum blood urea nitrogen (BUN), creatinine, and uric acid, which are considered to be significant markers of renal dysfunction [66, 67]. A significant increase in the serum BUN, creatinine and uric acid levels was observed in diabetic rats compared to the normal control group. Aqueous extract could not restore the altered BUN levels in diabetic rats (Table 2 ). This might indicate that the extract could not reduce the accumulation of urea nitrogen that occurred due to the enhanced breakdown of both liver and plasma proteins and that it did not play a role in protein metabolism [68]. Additionally, the treatment with all doses of aqueous extract significantly reduced the serum creatinine and uric acid levels of diabetic rats to normal levels (Table 2 ). This indicates improvement of the kidney excretion ability of creatinine, a byproduct of the breakdown of creatine and phosphocreatine, which are energy storage compounds in muscle, as well as uric acid, an end product of purine metabolism [68]. The normalization of the serum creatinine and uric acid levels indicates the role of this herbal formula in renal function improvement [67].
Overall, the results suggested that the aqueous extract is a good candidate for diabetes treatment because no undesirable effects on liver and kidney functions were observed, as it could be generated by long-term treatment with anti-diabetic agents. Although, the most potent dose of aqueous extract in regard to hypoglycaemic activity was 50 mg/kg, lower doses (12.5 and 25 mg/kg) exhibited more beneficial effects on the lipid profiles and liver and kidney functions. Therefore, 25 mg/kg was considered to be the most suitable dose because it has both potent hypoglycaemic activity and biochemical profile improvement effects in diabetic rats. Therefore, this dose should be used in the experimental design of further pharmaceutical, pharmacological and clinical studies on this herbal formula.
Aqueous extract did not exhibit acute toxicity to either sex of normal rats. Its LD50 was estimated to be higher than 5 g/kg. This result agreed with those of previous studies that reported the aqueous extracts of Abutilon indicum [17, 69], Acanthus ebracteatus [70], Harrisonia perforata [71], Imperata cylindrica [13], and Terminalia chebula [72] showed no acute toxicity in animals.
Conclusion
The plasma glucose lowering effect in both single and daily repeated oral administration of whole formula aqueous extract observed in STZ-nicotinamide-induced diabetic rats revealed its potent hypoglycaemic activity. Overall, the results suggested that aqueous extract is a good candidate for diabetes treatment due to the lack of observed undesirable effects on liver and kidney functions. The extract was not only unaltered, it improved most biochemical profiles, including total cholesterol, alkaline phosphatase, total proteins, albumin, globulin, creatinine, and uric acid. It was considered to have hypocholesterolomic, hepatoprotective, and renoprotective effects during diabetic hyperglycaemia. However, the elevation of serum triglycerides levels of diabetic rats treated with aqueous extract should be considered. Aqueous extract has no acute toxicity on male and female rats at a dose of 5 g/kg.
This study confirms the efficacy and safety of the Mathurameha herbal formula treating type 2 diabetes mellitus. The revealed hypoglycaemic activity, beneficial effects to biochemical profiles and non-acute toxicity of the entire formula aqueous extract provided valuable insight for next-steps research of this herbal formula. Further investigations on the in vitro hypoglycaemic actions of the whole formula aqueous extract and chemical compounds responsible for its effect should be performed to clarify the mechanisms and active compounds.
Abbreviations
- 2h–PPG:
-
2-h postprandial plasma glucose
- ALP:
-
Alkaline phosphatase
- ALT:
-
Alanine transferase
- AST:
-
Aspartate transferase
- BUN:
-
Blood urea nitrogen
- FPG:
-
Fasting plasma glucose
- OGTT:
-
Oral glucose tolerant test
- PGO:
-
Peroxidase-glucose oxidase
- STZ:
-
S treptozotocin
- TC:
-
T otal cholesterol
- TG:
-
Triglyceride
References
Zimmet P, Alberti KGMM, Shaw J. Global and societal implications of the diabetes epidemic. Nature. 2001;414:782–7.
Strategic Management and Service Plan Group. NCD Annual Report. Bangkok, Thailand: Bureau of Non Communicable Disease (NCD), Department of Disease Control, Ministry of Public Health; 2014.
Chatterjee S, Riewpaiboon A, Piyauthakit P, Riewpaiboon W, Boupaijit K, Panpuwong N, et al. Cost of diabetes and its complications in Thailand: a complete picture of economic burden. Heal Soc Care Community. 2011;19:289–98.
Groop LC, Pelkonen R, Koskimies S, Bottazzo GF, Doniach D. Secondary failure to treatment with oral antidiabetic agents in non-insulin-dependent diabetes. Diabetes Care. 1986;9:129–33.
Harrigan RA, Nathan MS, Beattie P. Oral agents for the treatment of type 2 diabetes mellitus: pharmacology, toxicity, and treatment. Annu Emerg Med. 2001;38:68–78.
Jager J, de Kooy A, Lehert P, Wulffele’ MG, van der Kolk J, Bets D, et al. Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: randomised placebo controlled trial. BMJ. 2010;340:1–7.
Moolasarn S, Sripa S, Kuessirikiet V, Sutawee K, Huasary J, Chaisila C. Usage of and cost of complementary/alternative medicine in diabetic patients. J Med Assoc Thail. 2005;88:1630–7.
Pumthong G, Nathason A, Tuseewan M, Pinthong P, Klangprapun S, Thepsuriyanon D, et al. Complementary and alternative medicines for diabetes mellitus management in ASEAN countries. Complement Ther Med. 2015;23:617–25. doi:10.1016/j.ctim.2015.01.016S0965-2299(15)00067-9. [pii]
Permphol P. Efficacy and safety of Mathurameha (Nirund Pongsoiphet and foundation for the promotion of Thai traditional medicine formula) for type 2 diabetes mellitus treatment: Thammasat University; 2015.
Adisakwattana S, Pudhom K, Yibchok-anun S. Influence of the methanolic extract from Abutilon indicum leaves in normal and streptozotocin-induced diabetic rats. African J Biotechnol. 2009;8:2011–5.
Ahmad M, Razak A, Akowuah GA, Asmawi Z, Zhari I. HPLC profile and antihyperglycemic effect of ethanol extracts of Andrographis paniculata in normal and streptozotocin-induced diabetic rats. J Nat Med. 2007;61:422–9.
Anulakanapakorn K, Pancharoen O, Bansiddhi J. Hypoclycemic effect of Tinospora crispa (Linn.) Mier ex Hook f. & Thoms (Menispermaceae) in rats. Bull Dep Med Sci. 1999;41:231–43.
Chunlaratthanaphorn S, Lertprasertsuke N, Srisawat U, Thuppia A, Ngamjariyawat A, Suwanlikhid N, et al. Acute and subchronic toxicity study of the water extract from root of Imperata cylindrica (Linn.) Raeusch. In rats. Songklanakarin J Sci Technol. 2007;29(Suppl. 1):141–55.
Doss A, Palaniswamy M, Angayarkanni J, Dhanabalan R. Antidiabetic activity of water extract of Solanum trilobatum (Linn.) in alloxan-induced diabetes in rats. African J Biotechnol. 2009;8:5562–4.
Fukunaga T, Miura T, Furuta K, Kato A. Hypoglycemic effect of the rhizomes of Smilax glabra in normal and diabetic mice. Biol Pharm Bull. 1997;20:44–6.
Kakuda T, Sakane I, Takihara T, Ozaki Y, Takeuchi H, Kuroyanagi M. Hypoglycemic effect of extracts from Lagerstroemia speciosa L. leaves in genetically diabetic KK-AY mice. Biosci Biotechnol Biochem. 1996;60:204–8.
Krisanapun C, Peungvicha P, Temsiririrkkul R, Wongkrajang Y. Aqueous extract of Abutilon indicum Sweet inhibits glucose absorption and stimulates insulin secretion in rodents. Nutr Res. 2009;29:579–87.
Krisanapun C, Lee S-H, Peungvicha P, Temsiririrkkul R, Baek SJ. Antidiabetic activities of Abutilon indicum (L.) Sweet are mediated by enhancement of adipocyte differentiation and activation of the GLUT1 promoter. Evidence-Based Complement Altern Med. 2011.
Kumar GPS, Arulselvan P, Kumar DS, S.P. Subramanian. Anti-diabetic activity of fruits of Terminalia chebula on streptozotocin induced diabetic rats. J Heal Sci. 2006;52:283–91.
Kumkrai P, Kamonwannasit S, Chudapongse N. Cytoprotective and anti-diabetic effects of Derris reticulata aqueous extract. J Physiol Biochem. 2014;70:675–84.
Latha RCR, Daisy P. Insulin-secretagogue, antihyperlipidemic and other protective effects of gallic acid isolated from Terminalia bellerica Roxb. In streptozotocin-induced diabetic rats. Chem Biol Interact. 2011;189:112–8.
Mohamed EAH, Mohamed AJ, Asmawi MZ, Sadikun A, Yam MF. Antihyperglycemic effect of Orthosiphon Stamineus Benth leaves extract and its bioassay-guided fractions. Molecules. 2011;16:3787–801.
Murali YK, Chandra R, Murthy PS. Antihyperglycemic effect of water extract of dry fruits of Terminalia chebula in experimental diabetes mellitus. Indian J Clin Biochem. 2004;19:202–4.
Noor H, Hammonds P, Sutton R, Ashcroft SJH. The hypoglycaemic and insulinotropic activity of Tinospora crispa: studies with human and rat islets and HIT-T15 B cells. Diabetologia. 1989;32:354–9.
Rahmat A, Baharudin BR, Baker MFA. Effects of Andrographis paniculata crude extract in normal and alloxan induced hyperglycemic rats. J Biol Sceinces. 2006;6:92–5.
Raut NA, Gaikwad NJ. Antidiabetic activity of hydro-ethanolic extract of Cyperus rotundus in alloxan induced diabetes in rats. Fitoterapia. 2006;77:585–8.
Sabu MC, Kuttan R. Antidiabetic and antioxidant activity of Terminalia belerica. Roxb Indian J Exp Biol. 2009;47:270–5.
Seetharam YN. Chalageria G, Setty SR, Bheemachar. Hypoglycemic activity of Abutilon indicum leaf extracts in rats. Fitoterapia. 2002;73:156–9.
Sriplang K, Adisakwattana S, Rungsipipat A, Yibchok-anun S. Effects of Orthosiphon stamineus aqueous extract on plasma glucose concentration and lipid profile in normal and streptozotocin-induced diabetic rats. J Ethnopharmacol. 2007;109:510–4.
Subramanian R, Asmawi MZ, Sadikun A. In vitro α-glucosidase and α-amylase enzyme inhibitory effects of Andrographis paniculata extract and andrographolide. Acta Biochim Pol. 2008;55:391–8.
Yoshikawa M, Pongpiriyadacha Y, Kishi A, Kageura T, Wang T, Morikawa T, et al. Biological activities of Salacia chinensis originating in Thailand: the quality evaluation guided by a-glucosidase inhibitory activity. Pharm Soc Japan. 2003;123:871–80.
Zhang X-F, Tan BK-H. Antihyperglyceamic and anti-oxidant properties of Andrographis paniculata in normal and diabetic rats. Clin Exp Pharmacol Physiol. 2000;27:358–63.
Adisakwattana S, Jiphimai P, Prutanapajai P, Chanathong B, Sapwarobol S, Ariyapitipan T. Evaluation of α-glucosidase, α-amylase and protein glycation inhibitory activities of edible plants. Int J Food Sci Nutr. 2010;61:295–305.
Gao H, Huang YN, Xu PY, Kawabata J. Inhibitory effect on a-glucosidase by the fruits of Terminalia chebula Retz. Food Chem. 2007;105:628–34.
Hamid HA, Liu M, Karim MR. α-Glucosidase and α-amylase inhibitory constituents of Tinospora crispa: isolation andchemical profile confirmation by ultra-highperformance liquid chromatography-quadrupoletime-of-flight/mass spectrometry. J Funct Foods. 2015;16:74–80.
Hou W, Li Y, Zhang Q, Wei X, Peng A, Chen L, et al. Triterpene acids isolated from Lagerstroemia speciosa leaves as α-glucosidase inhibitors. Phyther Res. 2009;23:614–8.
Kumkrai P, Weeranantanapan O, Chudapongse N. Antioxidant, α-glucosidase inhibitory activity andsub-chronic toxicity of Derris reticulata extract:its antidiabetic potential. BMC Complement Altern Med. 2015;15
Mohamed EA, Siddiqui MJ, Ang LF, Sadikun A, Chan SH, Tan SC, et al. Potent alpha-glucosidase and alpha-amylase inhibitory activities of standardized 50% ethanolic extracts and sinensetin from Orthosiphon stamineus Benth as anti-diabetic mechanism. BMC Complement Altern Med. 2012;12:176. doi:10.1186/1472-6882-12-1761472-6882-12-176. [pii]
Lokman FE, Gu HF, Mohamud WNW, Yusoff MM, Chia KL, Östenson C-G. Antidiabetic effect of oral borapetol B compound, isolated from the plant Tinospora crispa, by stimulating insulin release. Evidence-Based Complement Altern Med. 2013;2013:1–7.
Bai N, He KAN, Roller M, Zheng B, Chen X, Shao Z, et al. Active compounds from Lagerstroemia speciosa, insulin-like glucose uptake-stimulatory/inhibitory and adipocyte differentiation-inhibitory activities in 3T3-L1 cells. J Agric Food Chem. 2008;56:11668–74.
Hattori K, Sukenobu N, Sasaki T, Takasuga S, Hayashi T, Kasai R, et al. Activation of insulin receptors by lagerstroemin. J Pharmacol Sci. 2003;93:69–73.
Hayashi T, Maruyama H, Kasai R, Hattori K, Takasuga S, Hazeki O, et al. Ellagitannins from Lagerstroemia speciosa as activators of glucose transport in fat cells. Planta Med. 2002;68:173–5.
Lam SH, Ruan CT, Hsieh PH, Su MJ, Lee SS. Hypoglycemic diterpenoids from Tinospora crispa. J Nat Prod 75. 2012;75:153–9.
Noipha K, Purintrapiban J, Herunsalee A, Ratanachaiyavong S. In vitro glucose uptake activity of Tinospora crispa in skeletal muscle cells. Asian Biomed. 2008;2:415–20.
Yu BC, Hung CR, Chen WC, Cheng JT. Antihyperglycemic effects of andrographolide in streptozotocin-induced diabetic rats. Planta Med. 2003;69:1075–9.
Bone K, Mills S. Dosage and dosage forms in herbal medicine. In: Principles and Practice of Phytotherapy (Second Edition). Saint Louis: Churchill Livingstone; 2013. p. 121–33. doi:http://dx.doi.org/10.1016/B978-0-443-06992-5.00006-2.
Department for Development of Thai Traditional and Alternative Medicine. Monographs of Selected Thai Materia Medica. 2008;1.
Steenis CGGJ van. Flora Malesiana 1950;4:548–584.
Masiello P, Broca C, Gross R, Roye M, Manteghetti M, Hillaire-Buys D, et al. Experimental NIDDM: development of a new model in adult rats administered streptozotocin and nicotinamide. Diabetes. 1998;47:224–9. doi:10.2337/diabetes.47.2.224.
Peungvicha P, Thirawarapan SS, Temsiririrkkul R, Watanabe H, Prasain JK, Kadota S. Hypoglycemic effect of the water extract of Piper Sarmentosum in rats. J Ethnopharmacol. 1998;60:27–32.
Chayarop K, Temsiririrkkul R, Peungvicha P, Wongkrajang Y, Chuakul W, Rojsanga P. Anti-diabetic activity and acute toxicity of Thai traditional herbal formula, Mathura Meha aqueous extract. Planta Med. 2014;80(16):P2B102.
Elsner M, Guldbakke B, Tiedge M, Munday R, Lenzen S. Relative importance of transport and alkylation for pancreatic beta-cell toxicity of streptozotocin. Diabetologia. 2000;43:1528–33.
Szkudelski T. The mechanism of alloxan and streptozotocin action in β-cells of the rat pancreas. Physiol Res. 2001;50:537–46.
Lorenzati B, Zucco C, Miglietta S, Lamberti F, Bruno G. Oral hypoglycemic drugs: pathophysiological basis of their mechanism of action. Pharmaceuticals. 2010;3:3005–20.
Thuppia A, Rabintossaporn P, Saenthaweesuk S, Ingkaninan K, Sireeratawong S. The hypoglycemic effect of water extract from leaves of Lagerstroemia speciosa L. in streptozotocin-induced diabetic rats. Songklanakarin J Sci Technol. 2009;31:133–7.
Babu PS, Srinivasan K. Hypolipidemic action of curcumin, the active principle of tumeric (Curcuma longa) in streptozotocin induced diabetic rats. Mol Cell Biochem. 1997;166:169–75.
Rajasekaran S, Ravi K, Sivagnanam K, Subramanian S. Beneficial effects of Aloe vera leaf gel extract on lipid profile status in rats with streptozotocin diabetes. Clin Exp Pharmacol Physiol. 2006;33:232–7.
Sachdewa A, Khemani LD. Effect of Hibiscus rosa sinensis Linn. Ethanol flower extract on blood glucose and lipid profile in streptozotocin induced diabetes in rats. J Ethnopharmacol. 2003;89:61–6.
Ahmed I, Lakhani MS, Gillett M, John A, Raza H. Hypotriglyceridemic and hypocholesterolemic effects of anti-diabetic Momordica charantia (karela) fruit extract in streptozotocin-induced diabetic rats. Diabetes Res Clin Pract. 2001;51:155–61.
Elgazar AF, Rezq AA, Bukhari HM. Anti-hyperglycemic effect of saffron extract in alloxan-induced diabetic rats. Eur J Biol Sci. 2013;5:14–22.
Menon N, Sparks J, Omoruyi F. Hypoglycemic and hypocholesterolemic activities of the aqueous preparation of Kalanchoe pinnata leaves in streptozotocin-induced diabetic rats. Asian Pac J Trop Biomed. 2015;5:3–9.
Kroger H, Hauschild A, Ohde M, Bache K, Voigt WP, Thefeldt W, et al. Nicotinamide and methionine reduce the liver toxic effect of methotrexate. Gen Pharmacol. 1999;33:203–6.
Schein PS, Loftus S. Streptozotocin: depression of mouse liver pyridine nucleotides. Cancer Res. 1968;28:1501–6.
Rao PV, Madhavi K, Naidu MD, Gan SH. Rhinacanthus nasutus improves the levels of liver carbohydrate, protein, glycogen, and liver markers in streptozotocin-induced diabetic rats. Evidence-Based Complement Altern Med. 2013;2013:1–7.
Erejuwa OO, Sulaiman SA, Wahab MS, Sirajudeen KNS, Salleh MS, Gurtu S. Hepatoprotective effect of tualang honey supplementation in streptozotocin-induced diabetic rats. Int J Appl Res Nat Prod. 2012;4:37–41.
El-Demerdash FM, Yousef MI, El-Naga NIA. Biochemical study on the hypoglycemic effects of onion and garlic in alloxan-induced diabetic rats. Food Chem Toxicol. 2005;43:57–63.
Saeed MK, Deng Y, Dai R. Attenuation of biochemical parameters in streptozotocin-induced diabetic rats by oral administration of extracts and fractions of Cephalotaxus sinensis. J Clin Biochem Nutr. 2008;42:21–8.
Palsamy P, Subramanian S. Resveratrol, a natural phytoalexin, normalizes hyperglycemia in streptozotocin-nicotinamide induced experimental diabetic rats. Biomed Pharmacother. 2008;62:598–605.
Porchezhiana E, Ansari SH. Hepatoprotective activity of Abutilon indicum on experimental liver damage in rats. Phytomedicine. 2005;12:62–4.
Yahaufai J, Siripong P, Limpanasithikul W. Immunomodulatory effect of Acanthus Ebracteatus Vahl. Aqueous extract on macrophage function. Thai Cancer J. 2010;30:55–67.
Sireeratawong S, Lertprasertsuke N, Srisawat U, Thuppia A, Ngamjariyawat A, Suwanlikhid N, et al. Acute and subchronic toxicity study of the water extract from Harrisonia perforata Merr. In rats. Songklanakarin J Sci Technol. 2009;31:63–71.
Panunto W, Jaijoy K, Lerdvuthisopon N, Lertprasertsuke N, Jiruntanat N, Soonthornchareonnon N, et al. Acute and chronic toxicity studies of the water extract from dried fruits of Terminalia chebula Rezt. In rats. Int J Appl Res Nat Prod. 2010;3:36–43.
Acknowledgements
Authors would like to thank the Office of Thai Traditional Medical Knowledge Fund, Department for Development of Thai Traditional and Alternative Medicine, Ministry of Public Health, Thailand and The Thailand Research Fund and Faculty of Pharmacy, Mahidol University (IRG5780007) for the financially support.
Funding
1. Office of Thai Traditional Medical Knowledge Fund, Department for Development of Thai Traditional and Alternative Medicine, Ministry of Public Health, Thailand – financially supports all materials used in this study.
2. The Thailand Research Fund and Faculty of Pharmacy, Mahidol University (IRG5780007) – financially supports the publication charge.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
KC and RT designed the study. KC performed all experiments as well as analysed the data, and drafted the manuscript. PP was a major contributor in analysis and interpretation of data from in vivo hypoglycaemic experiments. RT and PR designed the chemical extraction procedures. YW was contributed to the acute toxicity study, and the interpretation of a biochemical data. WC identified all plant authentic specimens. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
The animal protocol was approved by the Animal Care and Used Committee, Faculty of Pharmacy, Mahidol University, Thailand (PYT008/2555).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chayarop, K., Peungvicha, P., Temsiririrkkul, R. et al. Hypoglycaemic activity of Mathurameha, a Thai traditional herbal formula aqueous extract, and its effect on biochemical profiles of streptozotocin-nicotinamide-induced diabetic rats. BMC Complement Altern Med 17, 343 (2017). https://doi.org/10.1186/s12906-017-1851-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-017-1851-8