
Abstract
Background
Probiotics have rarely been studied in young healthy infants from low-income countries. This phase I study investigated the safety and acceptability of two probiotics in Bangladesh.
Methods
Healthy infants aged four to twelve weeks from urban slums in Bangladesh were randomized to one of three different intervention dosing arms (daily, weekly, biweekly – once every two weeks) of Lactobacillus reuteri DSM 17938 and Bifidobacterium longum subspecies infantis 35624 over one month or to a fourth arm that received no probiotics. All subjects were followed for two additional months. Reported gastrointestinal and respiratory symptoms as well as breastfeeding rates, hospitalizations, differential withdrawals, and caretakers’ perception of probiotic use were compared among arms.
Results
In total, 160 infants were randomized (40 to each arm) with 137 (Daily n = 35, Weekly n = 35, Biweekly n = 35, Control n = 32) followed up for a median of twelve weeks; 113 completed the study. Illness and breastfeeding rates were similar across all arms. Ten hospitalizations unrelated to probiotic use occurred. Forty eight percent of the caretakers of infants in intervention arms believed that probiotics improved their baby’s health.
Conclusions
These two commonly used probiotics appeared safe and well-accepted by Bangladeshi families.
Trial registration
ClinicalTrials.gov NCT01899378. Registered July 10, 2013.
Similar content being viewed by others

Background
Probiotics are living microbial organisms that when administered in adequate amounts confer health benefits to the host [1]. Although a number of probiotic strains have been shown to be safe and to improve health by a variety of mechanisms [2, 3], few studies have assessed probiotics in healthy young infants in low-income countries. Gut microbiota of children in low-income countries differ from those in wealthier nations [4]. Gastrointestinal pathogens and diarrheal disease are more common in children in low-income countries, as is environmental enteropathy, a condition of increased intestinal permeability and decreased nutrient absorption [5]. We and others speculate that probiotics could modify gut microbiota, enhance gut immunity, and decrease gastrointestinal disease risk, especially if administered early in life [6]. Furthermore, probiotics administered early in life may have the greatest potential to achieve long-term colonization and immunologic benefits, before infants have begun to receive complementary foods and their microbiota shift to a more mature assemblage. However, it is possible that probiotics may induce adverse events in young infants with dysbiosis, reduced intestinal integrity, and decreased immunity [7, 8]. Therefore, determining safety in this infant population is crucial.
The choice of probiotics in this study was based on a literature review and strong safety data in infants. Lactobacillus reuteri DSM 17938 (parent strain L. reuteri ATCC 55730) [9] has been safely used in infants [10] and adults in the US and Europe [11] and recently in adults in the Peruvian Amazon [12] and has been reported to prevent or reduce diarrhea and gastrointestinal and respiratory infections [13–15], reduce pathogen colonization and alter microbiota composition [16, 17], reduce infant colic and crying time [18–20], suppress Helicobacter pylori and gastric symptoms [21], relieve constipation [22], control reflux and abdominal pain [23], and improve infant weight gain [24]. Bifidobacterium longum subspecies infantis is commonly found in both breast milk [25] and healthy infant stools [4] and is generally recognized as safe [26].
With the ultimate goal of evaluating the efficacy of probiotics to improve health in children in Bangladesh, the objectives of this report are to assess the safety and acceptability of three different regimens of Lactobacillus reuteri DSM 17938 and Bifidobacterium longum subspecies infantis 35624 given over one month to very young healthy infants.
Methods
Study population
Infants were recruited from three vaccination clinics near the International Center for Diarrheal Disease Research, Bangladesh (ICDDR,B) in Dhaka between October 2013 and April 2014. Inclusion criteria were: a) four to twelve weeks of age; b) no birth defects, history of hospitalization, or ongoing acute or chronic illness; c) no current antibiotic or probiotic use; d) weight within three standard deviations of the norm; and e) local residence for next four months. To select for infants who were more likely to be affected by environmental enteropathy, gastrointestinal infections, malnutrition, and stunting, children from lower socioeconomic status communities from households that shared a kitchen, water source, latrine, or courtyard with at least one other household were recruited. No restrictions on the diet of participating infants were made during the study. Parents or guardians provided written informed consent. The study was approved by the institutional review boards at both ICCDR,B (Protocol ID 13022) and Stanford University (Protocol ID 25487) and was registered on ClinicalTrials.gov (NCT01899378).
For the primary outcome of this study, proportion of days with symptoms, to detect a difference in change of 0.15 between the two groups with a sigma of 0.18 and an alpha of 0.05 and greater than 80 % power, 25 infants were needed per group. Twenty five infants in each group would allow detection of almost a two-fold difference (74 % vs. 35 %) between arms with 80 % power for dichotomous variables such as breastfeeding rates. Because the study population was transient, high levels of drop-out and loss to follow-up were expected. A similar study in this population had a 38 % drop-out rate; therefore 40 infants were enrolled per arm in order achieve a final sample size of at least 25 infants per arm [27].
Study design
The study design was multi-arm parallel where infants were randomized in equal numbers to one of four arms – a control arm (observation only) or to one of three intervention arms of L. reuteri DSM 17938 (108 colony forming units (CFU)) and B. longum subspecies infantis 35624 (109 CFU): daily dosing (29 doses overall), weekly dosing (five doses), or every two week dosing (three doses). Block randomization using a computerized random number generator and block sizes of twenty was used to account for seasonal differences. The primary researcher generated the sequence and the field research officer in charge of coordinating enrollment was blinded to block sizes. Enrollment was conducted by multiple field team members simultaneously. After screening and obtaining consent for an infant, the field team member contacted the field research officer for the next enrollment identification number to be assigned. Post-intervention follow-up occurred for two months (Fig. 1). Data collection ended in July 2014 when the final participating infant completed follow-up.

Study design and sampling scheme
Intervention
L. reuteri DSM 17938 (BioGaia, Sweden), in liquid drops, was stored and transported to the field at 4–8 °C; each dose was five drops. B. longum subspecies infantis 35624 (Proctor and Gamble), a powder-containing capsule, was stored and transported at ambient temperature. Immediately before administration the capsule was opened and the power was mixed with < 500ul sterile water to create a liquid suspension. Both probiotics were fed to infants by study staff using sterile Pasteur pipets in participating infants’ homes. Mothers were encouraged to breastfeed infants after each probiotic administration to ensure that the probiotic was swallowed. Infants were monitored by study staff for at least 30 min for immediate adverse reactions.
Data collection
Demographic and socioeconomic data were collected at enrollment. Health information, including gastrointestinal and respiratory symptoms as well as breastfeeding practices, was collected from caregivers on each of the seven days after the first and last probiotic doses and weekly at all other times covering the interval since last visit (Fig. 1). Exclusive breastfeeding was defined as the reported receipt of only breast milk in the prior 24 h [28]. At the end of the study, data were collected regarding the caretakers’ perceptions of probiotics. All survey data were collected electronically by study staff with Open Data Kit (ODK) software (https://opendatakit.org/) on portable tablets [29]. All infant hospitalizations were immediately reported to and reviewed by the Data Safety Monitoring Board (DSMB) at the ICCDR,B. Infants who were hospitalized continued in the study after they were released from the hospital unless they were withdrawn from the study by their parents.
Statistical analysis
Intent-to-treat analysis of those who initiated the study after randomization was performed; infants for whom no follow-up data were available were not included. Baseline demographic characteristics of infants and their households were compared among arms using the Kruskal-Wallis or chi-squared test. The primary outcomes of gastrointestinal and respiratory symptoms per infant (days with symptoms/total follow-up days) were compared with the Kruskal-Wallis test and a test for trend. Withdrawals, symptoms and monthly household income within and between the arms were compared using two-way ANOVA or chi-squared tests. Rates of exclusive breastfeeding among arms were compared using difference in proportion or chi-squared tests.
There were concerns by the ICDDR,B review committee that oral administration of probiotics could affect breastfeeding rates. Therefore, a stopping rule was implemented that if probiotics caused a reduction in breastfeeding, the trial would be stopped. At midline, interim analysis on breastfeeding data only was conducted and reported to the Data Safety Monitoring Board.
Results
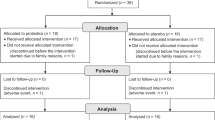
A total of 613 infants were screened; 275 were considered eligible (45 %) and 160 were enrolled (26 %), with 40 randomized to each study arm (Fig. 2). The most common reasons for ineligibility were moving outside of Dhaka (n = 97) or the infant was not currently healthy (n = 122). A total of 23 infants withdrew or were lost to follow-up after baseline data collection but before the intervention began, leaving 137 infants (86 %) contributing post-intervention data with a median follow-up of twelve weeks. These 137 infants were similar across arms (Table 1) although monthly household income was slightly lower in the weekly and daily treatment arms (p = 0.04). Of the 137 babies who contributed post-intervention data, 113 infants (82 %) completed the three months post-intervention of the study.

Flow-chart of study screening, enrollment, and retention
Withdrawals
A total of 47 infants (29 %) withdrew, 23 before and 24 after initiation of the intervention (Fig. 2). The primary reason for withdrawal after the intervention was a move away from Dhaka (58 %), followed by the family was too busy (13 %), and the family perceived no benefit from study (13 %). Families in the control arm withdrew more frequently (40 %) than the biweekly (28 %), weekly (28 %), or daily arms (23 %); they also withdrew sooner. Within the lowest household income group (<$100 per month), 70 % in the control arm withdrew, compared to 40 %, 31 %, and 14 % in the biweekly, weekly and daily arms respectively (p = 0.04). At baseline 156 infants were being breastfed, three were already weaned, and one withdrew before any baseline information was collected.
Safety
Cough and congestion were the most commonly reported symptoms (median 12 % and 14 % of follow-up days, respectively). Gastrointestinal symptoms were rare (Table 2). No differences were observed in percentage of follow-up time with diarrhea, watery or soft stool, vomiting, poor feeding, colic, cough, congestion, or difficulty breathing across arms (Table 2). Seventy percent of infants were being exclusive breastfed at eight weeks of age, while only 30 % were being exclusively breastfed at twenty weeks of age. No differences in exclusive breastfeeding rates were seen among study arms throughout the study. Eight infants (four from the biweekly arm, two from the weekly arm, two from the daily arm, and zero from the control arm) were hospitalized a total of ten times—six for pneumonia and four for diarrhea; all infants recovered fully. No hospitalization was temporally related to probiotic use or considered probiotic-related by the DSMB. Three infants had been weaned before enrollment; all three were hospitalized (50 % of hospitalizations). No allergic responses or other reactions were observed after probiotic administration.
Perception of probiotics
When caretakers in the intervention arms were asked about probiotics, 48 % reported the probiotics improved the health of the baby, 6 % reported no benefit, and 46 % were undecided. This finding was similar across intervention arms (p = 0.54).
Discussion
In this study, it was found that two probiotics were safe – did not cause sudden reactions, increase symptom rates, or diminish breastfeeding rates – and acceptable in infants younger than six months of age. No problems administering the probiotics were identified, with infants able to suck and swallow the formulations without difficulty or aversion. No differences in rates of any reported symptoms were observed among arms; additionally, no sudden adverse or allergic reactions were found after probiotic administration, and no hospitalizations were deemed related to probiotics administration.
The World Health Organization and Bangladeshi public health authorities strongly recommend exclusive breast-feeding for the first six-months of life to promote optimal growth, development, and health, and reduce infant mortality from common childhood diseases such as diarrhea and pneumonia [30]. Thus, it is important to ensure that oral administration of probiotics to infants did not negatively affect breastfeeding rates. No evidence was found that oral administration of probiotics decreased breastfeeding, preserving this important health practice.
There had been concern that underlying dysbiosis or impaired intestinal integrity might render infants susceptible to microbial translocation of the gut and infection by probiotic strains [31–33]. In this study no evidence of infection by probiotic strains was found; no illnesses were attributable to the probiotics. Although two investigations of probiotics in children in Bangladesh previously demonstrated safety, the children studied were older than those of our research [34, 35]. However, early gut microbiome assembly may be important in preventing dysbiosis; thus, testing probiotics in younger infants was imperative [36–40].
There have been some studies that suggest multistrain or multispecies probiotics may improve colonization or efficacy over monostrain probiotics [41, 42]; therefore, two probiotics were selected to test in combination in this study. While the selected probiotics have been well-studied for safety and efficacy in other situations, we cannot say that this choice of probiotics is optimal for infant health in Bangladesh. We are currently assessing duration of infant colonization and any physiologic signal of benefit in anticipation of a larger phase II-III trial. Other limitations of this study include a dropout rate of 29 % and the lack of blinding in the control arm, although this is not imperative in a phase I trial.
Conclusions
In conclusion, this study found that a L. reuteri DSM 17938 and B. longum subspecies infantis 35624 combination, even given daily, is safe and well-tolerated in very young infants in Bangladesh. The confirmation of safety and acceptability of these probiotics in this study population lays the groundwork for investigation of the efficacy of these probiotics in improving the health of Bangladeshi infants.
Abbreviations
- ICDDR,B:
-
International center for diarrheal disease research, Bangladesh
- DSMB:
-
Data safety monitoring board
References
WHO/FAO. Health and nutritional properties of powder milk with live lactic acid bacteria. Córdoba, Argentina: WHO/FAO; 2001.
Thomas DW, Greer FR. Nutrition AAoPCo, American Academy of Pediatrics Section on Gastroenterology H, and Nutrition: Probiotics and prebiotics in pediatrics. Pediatrics. 2010;126(6):1217–31.
Ng SC, Hart AL, Kamm MA, Stagg AJ, Knight SC. Mechanisms of action of probiotics: recent advances. Inflamm Bowel Dis. 2009;15(2):300–10.
Lin A, Bik EM, Costello EK, Dethlefsen L, Haque R, Relman DA, et al. Distinct distal gut microbiome diversity and composition in healthy children from Bangladesh and the United States. PLoS One. 2013;8(1), e53838.
Mckay S, Gaudier E, Campbell DI, Prentice AM, Albers R. Environmental enteropathy: new targets for nutritional interventions. Int Health. 2010;2(3):172–80.
Reid G, Anand S, Bingham MO, Mbugua G, Wadstrom T, Fuller R, et al. Probiotics for the developing world. J Clin Gastroenterol. 2005;39(6):485–8.
Topcuoglu S, Gursoy T, Ovalı F, Serce O, Karatekin G. A new risk factor for neonatal vancomycin-resistant Enterococcus colonisation: bacterial probiotics. J Matern Fetal Neonatal Med. 2014;1–4.
Deshpande GC, Rao SC, Keil AD, Patole SK. Evidence-based guidelines for use of probiotics in preterm neonates. BMC Med. 2011;9:92.
Heimbach J, BioGaia AB. GRAS Notice 000254: Generally Recognized as Safe (GRAS) Determination of Lactobacillus reuteri Strain DSM 17938 Center for Food Safety and Applied Nutrition, Food and Drug Administration 2008:1–134
Weizman Z, Alsheikh A. Safety and tolerance of a probiotic formula in early infancy comparing two probiotic agents: a pilot study. J Am Coll Nutr. 2006;25(5):415–9.
Mangalat N, Liu Y, Fatheree NY, Ferris MJ, Van Arsdall MR, Chen Z, et al. Safety and tolerability of Lactobacillus reuteri DSM 17938 and effects on biomarkers in healthy adults: results from a randomized masked trial. PLoS One. 2012;7(9), e43910.
Oberhelman RA, Kosek MN, Penataro-Yori P, Paredes-Olortegui M, Connolly E. A Phase One Safety Study of Lactobacillus reuteri Conducted in the Peruvian Amazon: Observations from the Field. Am J Trop Med Hyg. 2014;90(4):777–80.
Weizman Z, Asli G, Alsheikh A. Effect of a probiotic infant formula on infections in child care centers: comparison of two probiotic agents. Pediatrics. 2005;115(1):5–9.
Gutierrez-Castrellon P, Lopez-Velazquez G, Diaz-Garcia L, Jimenez-Gutierrez C, Mancilla-Ramirez J, Estevez-Jimenez J, et al. Diarrhea in preschool children and Lactobacillus reuteri: a randomized controlled trial. PEDIATRICS. 2014;133(4):e904–9.
Dinleyici EC, Dalgic N, Guven S, Metin O, Yasa O, Kurugol Z, et al. Lactobacillus reuteri DSM 17938 shortens acute infectious diarrhea in a pediatric outpatient setting. J Pediatr. 2015;91(4):392–6.
Savino F, Fornasero S, Ceratto S, De Marco A, Mandras N, Roana J, et al. Probiotics and gut health in infants: A preliminary case–control observational study about early treatment with Lactobacillus reuteri DSM 17938. Clin Chim Acta. 2015;451(Pt A):82–7.
Romani Vestman N, Chen T, Lif Holgerson P, Öhman C, Johansson I. Oral Microbiota Shift after 12-Week Supplementation with Lactobacillus reuteri DSM 17938 and PTA 5289. Randomized Control Trial PloS one. 2015;10(5), e0125812.
Szajewska H, Gyrczuk E, Horvath A. Lactobacillus reuteri DSM 17938 for the management of infantile colic in breastfed infants: a randomized, double-blind, placebo-controlled trial. J Pediatr. 2013;162(2):257–62.
Savino F, Cordisco L, Tarasco V, Palumeri E, Calabrese R, Oggero R, et al. Lactobacillus reuteri DSM 17938 in infantile colic: a randomized, double-blind, placebo-controlled trial. Pediatrics. 2010;126(3):e526–33.
Chau K, Lau E, Greenberg S, Jacobson S, Yazdani-Brojeni P, Verma N, et al. Probiotics for infantile colic: a randomized, double-blind, placebo-controlled trial investigating Lactobacillus reuteri DSM 17938. J Pediatr. 2015;166(1):74–8.
Francavilla R, Lionetti E, Castellaneta SP, Magistà AM, Maurogiovanni G, Bucci N, et al. Inhibition of Helicobacter pylori infection in humans by Lactobacillus reuteri ATCC 55730 and effect on eradication therapy: a pilot study. Helicobacter. 2008;13(2):127–34.
Coccorullo P, Strisciuglio C, Martinelli M, Miele E, Greco L, Staiano A. Lactobacillus reuteri (DSM 17938) in infants with functional chronic constipation: a double-blind, randomized, placebo-controlled study. J Pediatr. 2010;157(4):598–602.
Romano C, Ferrau’ V, Cavataio F, Iacono G, Spina M, Lionetti E, et al. Lactobacillus reuteri in children with functional abdominal pain (FAP). J Paediatr Child Health. 2014;50(10):E68–71.
Agustina RB-OI, Lukito W, Fahmida U, van de Rest O, Zimmermann MB, Firmansyah A, et al. Probiotics Lactobacillus reuteri DSM 17938 and Lactobacillus casei CRL 431 modestly increase growth, but not iron and zinc status, among Indonesian children aged 1–6 years. J Nutr. 2013;143(7):1184–93.
Grönlund M-M, Gueimonde M, Laitinen K, Kociubinski G, Grönroos T, Salminen S, et al. Maternal breast-milk and intestinal bifidobacteria guide the compositional development of the Bifidobacterium microbiota in infants at risk of allergic disease. Clin Exp Allergy. 2007;37(12):1764–72.
Proctor and Gamble Company. New Dietary Ingrediant Notification Information - Bifidobacterium infantis 35624. In: US Regulatory Affairs. April 29, 2005.
Lin A, Luby S. Personal communication - unpublished data from the WASH Benefits Study. 2013
WHO. Global Strategy for Infant and Young Child Feeding. 2000, 1–5:1–37.
Hartung C, Anokwa Y, Brunette W, Lerer A, Tseng C, Borriello G. Open Data Kit: Tools to Build Information Services for Developing Regions. ICTD. 2010;1–11.
WHO. Infant and young child nutrition: Global strategy on infant and young child feeding. Fifty-Fifth World Health Assembly. Provisional Agenda Item. 2002;13.10(A55/15):1–18.
Floch MH. Probiotic safety and risk factors. J Clin Gastroenterol. 2013;47(5):375–6.
Boyle RJ, Robins-Browne RM, Tang MLK. Probiotic use in clinical practice: what are the risks? Am J Clin Nutr. 2006;83(6):1256–64. quiz 1446–1257.
Liong M-T. Safety of probiotics: translocation and infection. Nutr Rev. 2008;66(4):192–202.
Sarker SA, Sultana S, Fuchs GJ, Alam NH, Azim T, Brüssow H, et al. Lactobacillus paracasei strain ST11 has no effect on rotavirus but ameliorates the outcome of nonrotavirus diarrhea in children from Bangladesh. PEDIATRICS. 2005;116(2):e221–8.
Matsuda F, Chowdhury MI, Saha A, Asahara T, Nomoto K, Tarique AA, et al. Evaluation of a probiotics, Bifidobacterium breve BBG-01, for enhancement of immunogenicity of an oral inactivated cholera vaccine and safety: a randomized, double-blind, placebo-controlled trial in Bangladeshi children under 5 years of age. Vaccine. 2011;29(10):1855–8.
Neu J. The developing intestinal microbiome: probiotics and prebiotics. World Rev Nutr Diet. 2014;110:167–76.
Murgas Torrazza R, Neu J. The developing intestinal microbiome and its relationship to health and disease in the neonate. J Perinatol. 2011;31 Suppl 1:S29–34.
Cox Laura M, Yamanishi S, Sohn J, Alekseyenko Alexander V, Leung Jacqueline M, Cho I, et al. Altering the Intestinal Microbiota during a Critical Developmental Window Has Lasting Metabolic Consequences. Cell. 2014;158(4):705–21.
Round JL, Mazmanian SK. The gut microbiota shapes intestinal immune responses during health and disease. Nat Rev Immunol. 2009;9(5):313–23.
Arrieta M-C, Stiemsma LT, Amenyogbe N, Brown EM, Finlay B. The intestinal microbiome in early life: health and disease. Front Immunol. 2014;5:427.
Timmerman HM, Koning CJM, Mulder L, Rombouts FM, Beynen AC. Monostrain, multistrain and multispecies probiotics--A comparison of functionality and efficacy. Int J Food Microbiol. 2004;96(3):219–33.
Gardiner GE, Casey PG, Casey G, Lynch PB, Lawlor PG, Hill C, et al. Relative ability of orally administered Lactobacillus murinus to predominate and persist in the porcine gastrointestinal tract. Appl Environ Microbiol. 2004;70(4):1895–906.
Acknowledgements
We acknowledge the valuable contributions of the field team manager Md. Mostafiz Rahman, and the field team: Md. Mizanur Rahman, Md. Fieak Fozol, Twouhid Uddin Rana, Ashan Habib, Nepen Chandra Das, Jugal Majumder, Debashis Roy, Md. Sahfiq Reza, Salahuddin Hossain, Rabi Sultana, Abdus Salam, Farida Begum, and Md. Alauddin Khandaker. We thank Dr. Patricia Hibberd and Dr. Christine Wanke for their review of our protocol. We thank BioGaia and Proctor and Gamble for providing the probiotic products used in this study. We thank Catherine Ley for her statistical advice and help with manuscript editing. We thank all of the participating infants and their families for their time and cooperation and all funders for financial support.
Funding
This study was supported by the Thrasher Research Fund Early Career Award (YEHS), Freeman Spogli Institute Underdevelopment Grant (JP), Stanford Center for Innovation in Global Health Seed Grant (JP), Global Health Equity Scholars Fellowship (YEHS), Stanford Medical Scholars Fund (TR), University of California, Berkeley’s Center for Global Public Health Fellowship (SHZ), Stanford Child Health Research Institute Postdoctoral Grant through Lucile Packard Foundation for Children’s Health and the Stanford CTSA (UL1 RR025744) (YEHS), and the TL1 Clinical Research Training Program of the Stanford Clinical and Translational Science Award to Spectrum (NIH TL1 TR 001084) (YEHS). The ICDDR,B acknowledges with gratitude the commitment of the donors to their research efforts and is thankful to the Governments of Australia, Bangladesh, Canada, Sweden and the UK for providing core/unrestricted support (KJ, LU). Funders had no role in the study design, data collection, data analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
YEHS contributed to the study conception and design, study set-up, survey design, study management, data collection and cleaning; performed analyses; and drafted and edited the manuscript. KJ contributed to the study design, study management, survey design, and data collection and cleaning. TR contributed to the survey design, study set-up, and data collection, processing, and cleaning. SHZ contributed to study design, study set-up, and data collection. LU contributed to study design. SL participated in the study conception and design, advised study management, and helped edit the manuscript. JP participated in the study conception and design, advised study management, oversaw data management and analysis, and helped draft and edit the manuscript. All authors were involved in editing the manuscript and read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hoy-Schulz, Y.E., Jannat, K., Roberts, T. et al. Safety and acceptability of Lactobacillus reuteri DSM 17938 and Bifidobacterium longum subspecies infantis 35624 in Bangladeshi infants: a phase I randomized clinical trial. BMC Complement Altern Med 16, 44 (2015). https://doi.org/10.1186/s12906-016-1016-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-016-1016-1