
Abstract
Background
Radiotherapy improves survival for many cancer patients. However, some patients still refuse radiotherapy despite the recommendations of their physicians. We aimed to investigate the impact of refusing recommended radiotherapy on overall survival in patients with gynecological cancers (GC) and attempted to describe what characteristics are associated with the refusal of radiotherapy.
Methods
Data were extracted from the Surveillance, Epidemiology and End Result (SEER) database for patients who were diagnosed with GC and recommended for radiotherapy between 1988 and 2016. Kaplan–Meier and multivariate Cox regression analyses were utilized to analyze the impact of refusal of radiotherapy on overall survival. Univariate and multivariate logistic regression analyses were used to identify characteristics associated with refusal of radiotherapy.
Results
In total, 1,226 of 208,093 patients (0.6%) refused radiotherapy. Multivariate Cox regression analysis showed that refusal of radiotherapy was associated with poorer overall survival in GC patients with stage I/II [hazard ratio (HR) = 1.64; 95% confidence interval (CI), 1.50–1.79], but may not affect overall survival in patients with stage III/IV (HR = 1.03; 95%CI, 0.84–1.25). Multivariate logistic regression analysis demonstrated that factors such as older age (40–65 years, > 65 years), unmarried status (divorced, single, widowed), higher foreign-born rate (1.87-2.82%, 1.51–2.19), refusal of surgery (recommended but not performed), and higher grade (poorly differentiated, undifferentiated/anaplastic) may increase the likelihood of refusing radiotherapy (all P < 0.05). Factors that may reduce the likelihood of refusing radiotherapy include higher income (> 42,810$), lower grade (well-differentiated), primary site of ovarian cancer, and no/unknown chemotherapy (all P < 0.05).
Conclusion
Refusal of radiotherapy is related to worse overall survival in GC patients with stage I/II, and many characteristics may affect a patient’s choice of refusal of radiotherapy.
Similar content being viewed by others


Background
Gynecological cancers (GC) are cancers that affect the ovaries, uterus, cervix, vulva, and vagina [1], and they are the second most common cancers in women after breast cancer [2]. In 2020, there were an estimated 981,234 new diagnoses of GC, including 604,127 cervical cancers, 313,959 ovarian cancers, 45,240 vulvar cancers, and 17,908 vaginal cancers [2]. In addition, there were 574,505 new deaths from GC worldwide [2]. Most early-stage GC, such as cervical, vulvar, and endometrial cancers, can be cured with surgery, or in combination with adjuvant radiotherapy or chemotherapy [3,4,5]. However, approximately 20–80% of cancer patients experience cancer recurrence after adequate treatment [6, 7]. Radiotherapy was used in isolated patients with local recurrence based on disease location and prior treatments.
Radiotherapy plays a central role in the treatment of GC, especially for some cancers that can also be cured with radiotherapy alone [8, 9]. Radiotherapy in combination with surgery and systemic therapy plays an important role in improving patient local control and prolonging overall survival of patients [10]. Despite these benefits of radiotherapy, it is not uncommon for patients to refuse radiotherapy in clinical practice. Aizer et al. indicated that about 0.9% of cancer patients refused radiotherapy despite the recommendations of their physicians [11]. Parsons et al. found that 5.9% of patients with endometrial cancer refused radiotherapy [12]. Importantly, the refusal of radiotherapy has been reported to be associated with poor survival outcomes in several cancers [13,14,15]. For example, refusal of radiotherapy has been found to be related to worse survival in patients with esophageal adenocarcinoma [14]. The study by Schwam et al. showed that head and neck cancer patients who refused postoperative radiotherapy had a significantly lower 3-year overall survival rate than patients who received postoperative radiotherapy [15]. However, few studies have reported the effect of refusal of radiotherapy on the survival of GC patients. Furthermore, there is limited evidence to assess characteristics associated with refusal of radiotherapy when recommended by the physician.
This study aimed to investigate the impact of refusal of recommended radiotherapy on overall survival of patients with GC based on a large national database. In addition, we attempted to describe what characteristics are associated with the refusal of radiotherapy.
Methods
Data source and patients
Data used in this retrospective cohort study were extracted from the Surveillance, Epidemiology and End Result (SEER)-18 registries (Nov 2020 Sub) database between 1988 and 2016. SEER database covers approximately 28% of the United State population and collects information on cancer statistics to reduce the cancer burden (https://seer.cancer.gov/). Patients diagnosed with GC were identified using the International Classification of Diseases for Oncology, version 3 (ICD-3) codes, including cervical cancer (C530-539), ovarian cancer (C569), vaginal cancer (C529), vulvar cancer (C510-519) and endometrial cancer (C540-549, C559). Patients who met the following inclusion criteria were included: (1) patients with pathological diagnosis of primary GC; (2) patients’ age ≥ 18 years; (3) patients with only one primary tumor; (4) patients received radiotherapy or radiotherapy was recommended but not performed due to the refusal of patients; (5) patients with complete data on marital status, tumor stage, and surgery, etc. Patients diagnosed with GC by autopsy or death certificate were excluded. Because this study used de-identified patient information from a public database (SEER database), this study was exempted from the Institutional Review Board of Beijing Ditan Hospital, Capital Medical University. The need for written informed consent was waived by the Institutional Review Board of Beijing Ditan Hospital, Capital Medical University due to retrospective nature of the study. All methods were performed in accordance with the relevant guidelines and regulations.
Variables
The primary outcomes of this study were overall survival and refusal of radiotherapy. Patients were followed up until 2017, and follow-up ended if the patient died during this period. Patient information including age (< 40, 40–65, and > 65 years), race (white, black, and others), marital status at diagnosis (divorced, married, separated, single, and widowed), residence (rural and urban), proxy measures (country-level data) of socioeconomic status [family income (< 36,580, 36,580–42,810, and > 42,810 $), unemployed (percentage of individuals with unemployed in a county; <52.4%, 52.4–71.4%, and > 71.4%), education (percentage of individuals with less that high-school education in a county; <18.75%, 18.75–28.20%, and > 28.20%), language isolation (percentage of people with English-language difficulties; <1.87%, 1.87–2.82%, and > 2.82%), foreign born (percentage of foreigners born in a county)], surgery (yes, recommended but not performed, and not performed), grade (well differentiated, moderately differentiated, poorly differentiated, and undifferentiated/anaplastic), primary site (cervical cancer, uterine cancer, ovarian cancer, and vulval cancer), chemotherapy (yes and no/unknown), the American Joint Committee on Cancer (AJCC) stage (I/II and III/IV), and overall survival status (survival and death) were collected.
Statistical analysis
Categorical variables were expressed as numbers and percentages [n (%)], and the Chi-square test (χ2) was used for comparison between groups. Characteristics of GC patients were described according to patients who received radiotherapy and those who refused radiotherapy. Kaplan-Meier (KM) survival curves and log-rank test or two-stage test were performed to calculate the survival time for patients who refused radiotherapy. Variables with P < 0.05 in the comparison of the characteristics of patients who received radiotherapy and those who refused radiotherapy were included in the multivariate Cox regression and logistic regression analyses for adjustment. Multivariate Cox regression analysis was utilized to assess the association between refusal of radiotherapy and overall survival, and reported as hazard ratio (HR) and 95% confidence interval (CI). Then, univariate- and multivariate logistic regression analyses were used to identify factors associated with refusal of radiotherapy, and presented as odds ratio (OR) and 95%CI. All statistical tests were two-tailed, and P-value < 0.05 was defined as significant. Statistical analyses were performed using the SAS 9.4 software (SAS Institute Inc., Cary, NC, USA) and RStudio 4.0.3 software.
Results
Characteristics of patients
A total of 343,435 patients diagnosed with GC were identified from the SEER database between 1988 and 2016. After screening, 135,342 patients were excluded, and 208,093 patients who met the inclusion criteria were included in the analysis (Fig. 1). Table 1 presents the characteristics of all included patients. Of the 208,093 patients, 118,284 (56.8%) were 40–65 years, 169,831 (81.6%) were whites, and 109,802 (52.8%) were married. In the terms of county-level data, 69,269 (33.3%) patients had an income of 36,580 − 42,810$, 69,825 (33.6%) patients had a regional unemployed percentage of 52.4-71.4%, 70,021 (33.6%) patients with education level less than high school of 18.75-28.20%, and 68,648 (33.0%) patients with regional language isolation percentage of 1.87-2.82%. There were 182,462 (87.7%) patients in stage I/II and 25,631 (12.3%) patients in stage III/IV. For treatment, 186,047 (89.4%) patients underwent surgery, and 71,269 (34.2%) patients received chemotherapy. There were 206,867 (99.4%) patients received radiotherapy and 1,226 (0.6%) patients refused radiotherapy. The median follow-up time for all patients was 56.00 (21.00, 120.00) months, while the median follow-up time for patients who refused radiotherapy was 27.50 (11.00, 72.00) months. At the end of follow-up, 128,204 (61.6%) patients were alive and 79,889 (38.4%) patients had died. Figure 2 demonstrates trends in the percentage of GC patients who refused radiotherapy from 1988 to 2016. The proportion of GC patients who refused radiotherapy increased from 1988 to 2016.

Flow chart for selection of patients

Trends in the percentage of gynecological cancers (GC) patients who refused radiotherapy from 1988 to 2016
Furthermore, there were significant differences in patients who received and refused radiotherapy among age, marital status, income, unemployed, education, foreign born, surgery, grade, primary site, chemotherapy, and overall survival (all P < 0.05).
Impact of refusal of radiotherapy on overall survival
Figure 3 shows the K-M survival curves for the impact of receiving and refusing radiotherapy on the overall survival of patients with different AJCC stages. GC patients who refused radiotherapy were associated with a poorer overall survival (Fig. 3A; P < 0.001). In addition, patients with AJCC stage I/II who refused radiotherapy also had worse overall survival than those who received radiotherapy (Fig. 3B; P < 0.001). However, no significant difference in overall survival was observed in AJCC stage III/IV patients who refused radiotherapy and those who received radiotherapy (Fig. 3C; P = 0.71). Since the K-M curves of patients with AJCC stage III/IV crossed, a two-stage test was used to further examine the difference in overall survival of these patients. The results indicated that there was still no significant difference in overall survival among AJCC stage III/IV patients who refused radiotherapy and those who received radiotherapy (P = 0.337).

Kaplan–Meier (K-M) curves for the impact of receiving and refusing radiotherapy on the overall survival of GC patients with different stages. (A) total patients; (B) patients with stage I/II; (C) patients with stage III/IV
Table 2 presents the impact of refusal of radiotherapy on overall survival in different populations. For GC patients with different AJCC stages, refusal of radiotherapy was associated with worse overall survival in patients with AJCC stage I/II (HR = 1.64; 95%CI, 1.50–1.79), but may not affect overall survival in patients with AJCC stage III/IV (HR = 1.03; 95%CI, 0.84–1.25). For patients with different years at diagnosis, refusal of radiotherapy was related to poorer overall survival in patients with years at diagnosis < 2000 (HR = 1.48; 95%CI, 1.22–1.79), years at diagnosis 2000–2013 (HR = 1.69; 95%CI, 1.54–1.85), and years at diagnosis > 2013 (HR = 1.56; 95%CI, 1.19–2.03). In addition, refusal of radiotherapy was associated with worse overall survival in both patients who received surgery (HR = 1.57; 95%CI, 1.42–1.72) or those who did not (HR = 1.29; 95%CI, 1.11–1.49).
Characteristics associated with refusal of radiotherapy
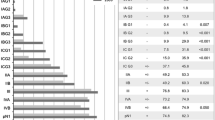
Table 3 displays univariate and multivariate logistic regression analyses of factors associated with refusal of radiotherapy in AJCC stage I/II patients. Univariate analysis indicated that factors that may affect refusal of radiotherapy include age, marital status, income, unemployed, education, foreign born, surgery, grade, primary site, and chemotherapy.
For multivariate analysis, factors include older age [40–65 years, OR = 1.60, 95%CI, 1.20–2.16; >65 years, OR = 2.89, 95%CI, 2.15–3.96], unmarried status [divorced, OR = 1.45, 95%CI, 1.19–1.76; single, OR = 1.34, 95%CI, 1.13–1.59; widowed, OR = 1.35, 95%CI, 1.14–1.59], higher foreign born [1.87-2.82%, OR = 1.82, 95%CI, 1.51–2.19; >2.82%, OR = 1.60, 95%CI, 1.30–1.97], refused surgery [recommended but not performed, OR = 5.52, 95%CI, 4.03–7.60], and higher grade [poorly differentiated, OR = 1.73, 95%CI, 1.49–2.01; undifferentiated/anaplastic, OR = 2.39, 95%CI, 1.91–2.95] may increase the likelihood of refusing radiotherapy. Factors that may reduce the likelihood of refusing radiotherapy include higher income [> 42,810$, OR = 0.26, 95%CI, 0.20–0.33], lower grade [well differentiated, OR = 0.54, 95%CI, 0.45–0.64], primary site of ovarian cancer (OR = 0.13, 95%CI, 0.09–0.20), and no/unknown chemotherapy (OR = 0.28, 95%CI, 0.22–0.35).
Discussion
Radiotherapy is one of the important methods in cancer treatment, especially for localized or solid cancers. However, some cancer patients may refuse radiotherapy despite the recommendations of their physicians. Our results found that the proportion of GC patients who refused radiotherapy increased from 1988 to 2016. Refusal of radiotherapy was associated with decreased overall survival in patients with AJCC stage I/II GC, but refusal of radiotherapy may not affect overall survival in patients with AJCC stage III/IV. Furthermore, factors that may increase the likelihood of refusal of radiotherapy include older age, unmarried status, higher foreign born, refusal of surgery, and higher grade. Patients with higher income, lower tumor grades, and those who did not receive chemotherapy were more likely to receive radiotherapy.
Previous studies have focused more on the effect of refusal of surgery on survival in cancer patients [16,17,18]. Radiotherapy is one of the three common ways of cancer treatment, and the impact of refusal of radiotherapy on patient survival needs to be concerned [19]. Our results found that patients with AJCC stage I/II GC who refused radiotherapy had a lower overall survival compared to those who received radiotherapy, while there was no difference in overall survival between the two groups in patients with AJCC stage III/IV. Aizer et al. showed that cancer-specific mortality in ovarian cancer and uterine cancer patients who refused radiotherapy was significantly higher than in patients who received radiotherapy [11]. A large sample study conducted by Parsons et al. demonstrated that refusal of radiotherapy was associated with a significantly lower 5-year overall survival in patients with endometrial cancer [12]. Hanna et al. indicated that radiotherapy can provide important and irreplaceable local control and overall survival benefits in GC patients under optimal utilization [20]. Furthermore, a meta-analysis found that the 5-year overall survival rate was 50–61% in patients with stage I/II cervical cancer who received radiotherapy only, and 24% in stage III/IV patients [9]. Our results showed a significant difference in overall survival between patients who refused radiotherapy and those who received radiotherapy in patients with stage I/II GC.
Characteristics that may be associated with refusal of radiotherapy in patients with GC were also explored in this study. Patients with older age, unmarried status, the county of higher foreign born, refused surgery, and higher tumor grade was more likely to refuse radiotherapy. Parsons et al. also found that higher age was associated with a higher likelihood of refusal of radiotherapy [12]. This phenomenon may be related to the underestimation of their survival expectations and the fear of treatment options in older cancer patients [21, 22]. Married patients were more likely to receive radiotherapy than divorced/single/widowed patients. This may be attributed to the fact that married patients may receive more social support to face the stress of receiving radiotherapy [23, 24]. Patients who refused surgery may also refuse radiotherapy, possibly because patients who refused recommended surgery may also be negative about alternative recommended treatments. In addition, our results also indicated that patients with higher income and those who did not receive chemotherapy were more likely to receive radiotherapy. Socioeconomic status has an important influence on the treatment compliance of cancer patients [25]. Patients with higher socioeconomic status are less worried about the financial burden of treatment and more likely to trust physician recommendations [26, 27]. For patients who did not receive chemotherapy, perhaps because they did not receive other treatments, they would not refuse radiotherapy, which is commonly used in cancer treatment. Patients who do not receive recommended radiotherapy may not understand the benefits of radiotherapy for survival in patients with cancers and may be distrustful of the health care system [28]. Surveys of patients and physicians revealed significant differences in their knowledge about radiotherapy, such as how radiotherapy works and whether patients are able to work during treatment [29]. In addition, precision management of GC plays an important role in patient survival due to differences in secondary and tertiary prevention of different types of GC [30]. Therefore, for patients with GC who may refuse radiotherapy (e.g., older and unmarried), clinicians may need to spend more time making patients clearly understand their condition, the recommended treatments, the benefits of the treatments, and the impact of the treatments on their daily life.
We used a large sample and nearly 30 years of data from the SEER database to explore the impact of refusal of radiotherapy on overall survival in GC patients and to analyze characteristics associated with refusal of radiotherapy. This study may provide evidence for the relationship between refusal of radiotherapy and overall survival in patients with GC. However, there are several limitations to our study. First, due to database-based study, such a database can often be associated with miscoding and missing data. Second, insurance status had a significant impact on patient treatment choices but was not included in the analysis because the relevant data in the database were not recorded until 2007. We measure the effect of insurance status by incorporating other relevant variables such as income, education level, etc. Third, there are only “yes” and “no/unknown” statuses regarding the use of chemotherapy, with unclear information about chemotherapy was recommended but refused by patients. Fourth, comorbidities are associated with overall survival, but information related to comorbidities was not available due to limitations of the SEER data. Fifth, the impact of changes in radiotherapy guidelines for GC on patient survival could not be assessed due to limitations of the SEER database.
Conclusions
A large national database was used to investigate the impact of refusing recommended radiotherapy on overall survival in patients with GC. Refusal of radiotherapy was associated with poorer overall survival in GC patients with stage I/II, but it may not affect overall survival in patients with stage III/IV. Factors include older age, unmarried status, higher foreign born, refused surgery, and higher grades may increase the likelihood of refusal of radiotherapy. Factors that may reduce the likelihood of refusal of radiotherapy include higher income, lower grade, the primary site of ovarian cancer, and no/unknown chemotherapy.
Data Availability
All data relevant to the study are included in the article is available from SEER database, https://seer.cancer.gov/. The dataset used in this study is presented in the Supplementary Material (“Raw data.xlsx”).
Abbreviations
- GC:
-
Gynecological cancers
- SEER:
-
Surveillance, Epidemiology and End Result
- ICD-3:
-
International Classification of Diseases for Oncology, version 3
- AJCC:
-
the American Joint Committee on Cancer
- KM:
-
Kaplan-Meier
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- OR:
-
Odds ratio
References
Yamagami W, Nagase S, Takahashi F, Ino K, Hachisuga T, Aoki D, et al. Clinical statistics of gynecologic cancers in Japan. J Gynecologic Oncol. 2017;28:e32.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. Cancer J Clin. 2021;71:209–49.
Zigras T, Lennox G, Willows K, Covens A. Early Cervical Cancer: current dilemmas of staging and Surgery. Curr Oncol Rep. 2017;19:51.
Ang C, Bryant A, Barton DP, Pomel C, Naik R. Exenterative surgery for recurrent gynaecological malignancies. The Cochrane database of systematic reviews. 2014; 2014: Cd010449.
Deleon MC, Ammakkanavar NR, Matei D. Adjuvant therapy for endometrial cancer. J Gynecologic Oncol. 2014;25:136–47.
Long-term outcomes for. Neoadjuvant versus adjuvant chemotherapy in early Breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018;19:27–39.
Geurts SM, de Vegt F, van Altena AM, van Dijck JA, Tjan-Heijnen VC, Verbeek AL, et al. Considering early detection of relapsed Ovarian cancer: a review of the literature. Int J Gynecol cancer: Official J Int Gynecol Cancer Soc. 2011;21:837–45.
Suneja G, Viswanathan A. Gynecologic malignancies. Hematol Oncol Clin N Am. 2020;34:71–89.
Hanna TP, Shafiq J, Delaney GP, Barton MB. The population benefit of radiotherapy for Cervical cancer: local control and survival estimates for optimally utilized radiotherapy and chemoradiation. Radiotherapy and Oncology: Journal of the European Society for Therapeutic Radiology and Oncology. 2015;114:389–94.
Backes FJ, Martin DD. Intraoperative radiation therapy (IORT) for gynecologic malignancies. Gynecol Oncol. 2015;138:449–56.
Aizer AA, Chen MH, Parekh A, Choueiri TK, Hoffman KE, Kim SP, et al. Refusal of curative radiation therapy and Surgery among patients with cancer. Int J Radiat Oncol Biol Phys. 2014;89:756–64.
Parsons MW, Francis S, Maurer KA, Grant J, Gaffney DK. Refusal of Radiation results in Inferior Survival in Endometrial Cancer. Am J Clin Oncol. 2020;43:399–410.
Matsuo K, Machida H, Ragab OM, Garcia-Sayre J, Yessaian AA, Roman LD. Patient compliance for postoperative radiotherapy and survival outcome of women with stage I endometrioid endometrial cancer. J Surg Oncol. 2017;116:482–91.
Parsons M, Lloyd S, Johnson S, Scaife C, Varghese T, Glasgow R, et al. Refusal of local therapy in Esophageal Cancer and Impact on overall survival. Ann Surg Oncol. 2021;28:663–75.
Schwam ZG, Husain Z, Judson BL. Refusal of postoperative radiotherapy and its association with survival in Head and Neck cancer. Radiotherapy and Oncology: Journal of the European Society for Therapeutic Radiology and Oncology. 2015;117:343–50.
Straubhar AM, Parsons MW, Francis S, Gaffney D, Maurer KA. Refusal of Surgery and survival outcomes in endometrial cancer. Int J Gynecol cancer: Official J Int Gynecol Cancer Soc. 2021;31:1236–41.
Gaitanidis A, Alevizakos M, Tsalikidis C, Tsaroucha A, Simopoulos C, Pitiakoudis M. Refusal of Cancer-Directed Surgery by Breast Cancer patients: risk factors and survival outcomes. Clin Breast Cancer. 2018;18:e469–e76.
Hu X, Ye H, Yan W, Sun Y. Factors Associated with Patient’s refusal of recommended Cancer Surgery: based on Surveillance, Epidemiology, and end results. Front Public Health. 2021;9:785602.
Atun R, Jaffray DA, Barton MB, Bray F, Baumann M, Vikram B, et al. Expanding global access to radiotherapy. Lancet Oncol. 2015;16:1153–86.
Hanna TP, Delaney GP, Barton MB. The population benefit of radiotherapy for gynaecological cancer: local control and survival estimates. Radiotherapy and Oncology: Journal of the European Society for Therapeutic Radiology and Oncology. 2016;120:370–7.
Maxfield M, Pyszczynski T, Kluck B, Cox CR, Greenberg J, Solomon S, et al. Age-related differences in responses to thoughts of one’s own death: mortality salience and judgments of moral transgressions. Psychol Aging. 2007;22:341–53.
Rothman MD, Van Ness PH, O’Leary JR, Fried TR. Refusal of medical and surgical interventions by older persons with advanced chronic Disease. J Gen Intern Med. 2007;22:982–7.
Tuinman MA, Van Nuenen FM, Hagedoorn M, Hoekstra-Weebers JE. Distress, problems and referral wish of cancer patients: differences according to relationship status and life phase. Psycho-oncology. 2015;24:699–704.
Hughes S, Jaremka LM, Alfano CM, Glaser R, Povoski SP, Lipari AM, et al. Social support predicts inflammation, pain, and depressive symptoms: longitudinal relationships among Breast cancer survivors. Psychoneuroendocrinology. 2014;42:38–44.
Arrossi S, Matos E, Zengarini N, Roth B, Sankaranayananan R, Parkin M. The socio-economic impact of Cervical cancer on patients and their families in Argentina, and its influence on radiotherapy compliance. Results from a cross-sectional study. Gynecol Oncol. 2007;105:335–40.
Blendon RJ, Benson JM, Hero JO. Public trust in physicians–U.S. medicine in international perspective. N Engl J Med. 2014;371:1570–2.
Ohri N, Rapkin BD, Guha D, Haynes-Lewis H, Guha C, Kalnicki S, et al. Predictors of radiation therapy noncompliance in an urban academic cancer center. Int J Radiat Oncol Biol Phys. 2015;91:232–8.
Bickell NA, Weidmann J, Fei K, Lin JJ, Leventhal H. Underuse of Breast cancer adjuvant treatment: patient knowledge, beliefs, and medical mistrust. J Clin Oncol. 2009;27:5160–7.
Bolderston A. Mixed messages? A comparison between the perceptions of radiation therapy patients and radiation therapists regarding patients’ educational needs. Radiography. 2008;14:111–9.
D’Augè TG, Giannini A, Bogani G, Dio CD, Laganà AS, Donato VD et al. Prevention, Screening, Treatment and Follow-Up of Gynecological Cancers: State of Art and Future Perspectives. Clinical and Experimental Obstetrics & Gynecology. 2023; 50: 160.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
SZ and JL designed the study. SZ wrote the manuscript. JH collected, analyzed and interpreted the data. JL critically reviewed, edited and approved the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Because this study used de-identified patient information from a public database (SEER database), this study was exempted from the Institutional Review Board of Beijing Ditan Hospital, Capital Medical University. The need for written informed consent was waived by the Institutional Review Board of Beijing Ditan Hospital, Capital Medical University due to retrospective nature of the study. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, S., He, J. & Liu, J. Characteristics and survival of patients with gynecological cancers who refuse radiotherapy: a retrospective cohort study. BMC Women's Health 23, 562 (2023). https://doi.org/10.1186/s12905-023-02720-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-023-02720-6