
Abstract
Background
In 2017 WHO reported that due to a lack of menstrual hygiene management (MHM) facilities, high costs, and ignorance, 2.3 billion girls and women worldwide do not manage their menstruation properly. This leads to the use of other options, such as old clothes or other unhygienic materials, which may make them a risk group for infections and other health consequences. Despite the significant role of appropriate menstrual hygiene practices, it is still a missed opportunity to address the hygienic practice of menstruation among girls in many low-and middle-income countries, including Ethiopia.
Objective
Primarily, this study was aimed at investigating menstrual hygiene management (MHM) practice and determinant factors among young adolescent school girls in eastern Ethiopia, Gursum District 2021.
Method
An institutional-based cross-sectional survey was conducted among adolescent school girls in Gursum, Eastern Ethiopia, in 2021. 577 girls participated in this study and a multi-stage sampling procedure was employed so as to select a fair and representative sample of female students who experienced menarche. After controlling for confounding variables, binary logistic regression was fitted to identify factors affecting MHM among adolescent girls.
Result
This study revealed that 58.41% of adolescent school girls practice unsafe MHM practices. It was also reported that 193(33.45%) of the girls use reusable sanitary pads. Of those, 182(31.5%) of them keep the pads in hidden places as it is a shame to be seen Seventy-six (13.17%) of the respondents had experienced vaginal infections during menarche. Having knowledge about menstruation prior to experiencing menstruation [AOR 0.28 CI: (0.1476132, 0.5613692)], being over 15 years old [AOR 1.56, CI: (1.020577, 2.387646)], living in rural areas [AOR 1.23 CI: (1.1563013, 1.3562546)], and having infection around their vagina during menarche [AOR 4.6 CI: (2.633405, 8. 273,883)] were significant determinants of MHM practice.
Conclusion
The majority of the adolescent girls who participated in this study practice unsafe MHM practices. Results suggest that school health education focusing on improving the hygienic practices of adolescent girls during menstruation should be provided.
Similar content being viewed by others


Introduction
Even though menstruation is a natural process, it is associated with several misconceptions and malpractices which may cause serious ill-health, including reproductive tract and urinary tract infections [1]. Globally, 2.3 billion girls and women do not manage their menstruation properly due to a lack of menstrual hygiene management (MHM) facilities, high costs, and ignorance. This leads to the use of other options, such as old clothes or other unhygienic materials, which may make them a risk group for infections and other health consequences [2]. Currently, there is adequate management of menstrual hygiene in developed countries. However, it is a major problem among girls and women in poor countries, which potentially affects their health and development [3].
About 200 million women and girls from developing countries struggle to get access to clean water for personal hygiene, and private places [4]. They face major challenges as a result of poor hygiene facilities due to inadequate water supply for washing, lack of soap, lack of privacy, non-functioning or unclean toilets, and no disposal facilities for menstrual management in the school environment [3, 5,6,7].
Myths, taboos, and socio-cultural-related factors create barriers for adolescents in getting adequate information regarding proper menstrual management in low- and middle-income countries. These problems limit their routine activities and negatively affect their self-esteem, reproductive health, as well as schooling [8, 9].
Despite the significant role of appropriate menstrual hygiene practices, it is still a missed opportunity to address the hygienic practice of menstruation among girls in many low and middle income countries, including Ethiopia [10].
In Ethiopia, the majority of girls are at risk of getting genitourinary tract infections as a result of poor hygienic practices during their menstruation period [11]. Most girls do not communicate with their family about menstrual hygiene due to fear of the punishments and prevented from school [12]. Even, existing sanitation conditions in majority of schools in Ethiopia are inadequate that has potential impact on girls’ education [13]. According the previous study conducted in Ethiopia, about 43.0 to 54.5% of girl students were absent from school for 1 to 4 days in each menstrual period as result of menstruation-related problems [14, 15].
Besides these problems, there is limited information on menstruation and its hygienic management as well as its influence on girls’ education in Ethiopia [15]. Therefore, the current study is aimed to assess the hygienic menstrual management and associated risk factors among adolescent school girls in Gursum district, Eastern Ethiopia.
The findings of the current study will be used by policymakers, stakeholders, health program planners, researchers, and other bodies responsible for solving these problems by providing adequate information regarding menstruation and menstrual hygiene or by providing appropriate intervention programs for schoolgirls.
Methods and material
Study setting, and design
An institutional-based cross-sectional survey was conducted among adolescent school girls in Gursum, Eastern Ethiopia. A total of 40 schools are available in the district, five of which are found in the town and the other 35 in the rural kebeles. Gursum is distanced from Addis Ababa and Harar by 598 km and 75 km, respectively. The total population of the district is 151,931, of which 77,112 are men and 74,819 are women. The living condition of the people, both in rural and urban areas, is dependent on cash crops like Khat, ground nuts, and coffee [16].
Participants
All female students from grade 8–12 who experienced menarche and all the schools found in the district are source population. Representative sample was drawn female students’ who experienced menstruation and were available at school during the data collection was included in the study. Female students in the same grade level who experienced menarche but were seriously sick and absent from school at the time of data collection was note excluded from the study.
Sample size and sampling procedure
The total number of source population was 3237.Sample size was obtained using the 50% proportion of female students considered as properly practicing menstrual hygiene. 50% proportion of female students were taken because we could not find similar study conducted prior to this study in Ethiopia. A precision of 5% and with 95% confidence level was taken and by considering 10% non-response rates and design effect of 1.5 final obtained sample size was 634.Finaly, the response rate obtained was 91%.
A multi stage sampling procedure was employed so as to select a fair representative sample from 1152 female students who experienced menarche and attending class in the selected 8 schools. First, from a total of 40 schools 5 from urban and 35 from rural, 1 and 7 schools were selected proportionally using simple random sampling respectively. From each selected schools, sections and then individual female students who started menarche at the time of data collection was selected using simple random sampling (Fig. 1).

Schematic Presentation of sample size and sampling technique
Data collection tool, procedures, and quality control
A self-administered questionnaire adopted from the UNICEF WASH manual [17] and reviewing other relevant literature was used to collect quantitative data [18, 19]. Due to the sensitivity of the issue and to get reliable data without fear, four female data collectors (midwifery) and one supervisor were recruited from Gursum health centers. Intensive training was given for two days by the principal investigator on the process of data collection and critical ethical issues. In the Babille district of eastern Ethiopia, a pretest was conducted at Karl Hems Bom high school., eastern Ethiopia.
Data processing and analysis
After checking for completeness, collected data was entered to Epi data version 3.0 and exported to Stata version 17 statistical software for descriptive and inferential analysis. Bivariable analysis was done to determine predictable variables which has a significant association with outcome variable. Predictor variable which showed a significant association with MHM practice in bivariable analysis at p-value ≤ 0.25 were fitted into multivariable analysis. Finally, independent variables were declared statistically significant at 95% confidence interval (CI), and P < 0.05.
Outcome variable measurement (unsafe MHM practice)
World Health Organization and UNICEF’s proposed definition of menstrual hygiene management as “1.use of clean menstrual management material to absorb or collect menstrual blood that can be changed in privacy as often as necessary for the duration of a menstrual period, 2. using soap and water for washing the body as required, and 3.having access to safe and convenient facilities to dispose of used menstrual management materials (disposed in a latrine or buried) during menustruation.Accordingly, the school girls who fulfill the above three criteria during menstrual time was categorized as Safe MHM and those who do not practice at all, practice only one and/or two of the three criteria stated above were categorized as unsafe MHM practice [20, 21].
Results
Sociodemographic characteristics
Out of the total, 577 study participants, more than half (n = 299, 51.82%) of them were urban residents. The mean age at first menarche was 14 (SD 1.35). Out of a total 577 study participants, 125(42.65%) were from grade eight, while the rest were from grades 9–10 and 11–12 respectively. (Table 1).
Knowledge about menstrual hygiene
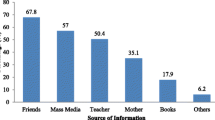
The great majority of 520(90.12%) respondents had heard about menstruation before they experienced menarche. Female friends, 209 (36.22%), were the major source of information about the menstrual cycle. The result from self-report also indicated that 275(47.66%) of the participants have experienced an irregular menstrual cycle. Regarding the duration of menstruation, 432(92.20%) of them responded that, on average, the duration of menstruation lasts up to five days. On the other hand, 514 (89.08%) of the adolescent girls knew commercially available sanitary pads (Table 2).
Hygienic practice during menarche
According to the data obtained from the respondents,369 (63.95%) of respondents use disposable sanitary pads, while 15 (2.60%) of the respondents use only underwear during menstruation. Of those who use disposable sanitary pads, 341 (59.10%) use commercially available sanitary pads. Further, among the respondents who use reusable sanitary pads, 170(29.46%) use pieces of cloth as an absorbent pad. Out of those who use reusable sanitary pad 182(31.54%) keep it in hidden places because it is perceived as a shame to be seen. More than half (332 (57.54%) of the respondents wash their genitals more than three times per day. It was also reported that 76 (13.17% of them) had experienced vaginal infection during menarche (Table 3).
Factors associated with menstrual hygiene management practice among adolescent women in eastern ethiopia, gursum district
The prevalence of unsafe MHM was found to be 58.41% with 95% CI (0.54, 0.62).The final multivariable logistic regression model indicated that having prior information about the menstruation cycle before menstruation started decreased the odds of unsafe MHM practice among adolescents by 72% [AOR.28 CI: (0.145, 0.56)] compared to their counterpart. The likelihood of unsafe MHM practice was 1.56 [AOR 1.56, CI: (1.02, 2.39)] times more likely among > 15 years old girls, compared to girls less than 15 years old (Table 4).
As the data obtained from this study being from rural areas increases the likelihood of unsafe MHM practice by 1.23 [(AOR 1.23 CI: (0.16, 1.36), compared to their counterparts. Furthermore, knowing a commercially available sanitary pad decrease the odds of unsafe MHM practice among adolescent girls by 68% [AOR 0.32 CI: (0.17, 0.60)]. The odds of unsafe MHM practice, were 4.6 times higher [AOR 4.6 CI: (2.63, 8.27)] among respondents who had experienced a health infection around their vagina during menarche (Table 4).
Discussion
Overall, this study investigated the MHM practice and factors affecting it among young adolescent school girls in eastern Ethiopia, Gursum district in 2021. In this study, it was reported that more than half (58.41%) of the study participants practiced unsafe-MHM practices. This finding is comparable with a previous studies conducted among adolescent school girls in Ambo, Holeta, Nekemte town, and Indonesia where the prevalence of unsafe MHM practice was 53.6%, 63.3%, 60.1%, and 64.1%, respectively [22,23,24,25]. On the other hand, the findings is lower than a report from Bahirdar and Uganda, where only one in four and 9.5% of them practice safe MHM [26, 27]. Perhaps, the discrepancy may be due to differences in sociodemographic status, study time frame, and study setting.
It was also reported that unsafe MHM was more likely among those older than 15-year-old adolescent girls compared to their counterparts. However, studies in Ghana and India indicated that safe MHM management is more likely among older girls compared to younger ones. [21, 28]. This difference could due to variation in study area and living standard.
The findings of this study also showed that the odds of safe MHM were higher among female adolescent girls who had heard about the menstruation cycle before experiencing menstruation when compared to their counterparts. Likewise, knowing a commercially available menstrual pad increases the odds of safe MHM practice by 68.6% [AOR 0.32 CI: (0.173355, 0.6047782)] among adolescent girls. This is supported by the study conducted in Nekemte town where prior information about menarche is significantly associated with MHM [24]. In addition, this finding is also supported by a study done in Mehalmeda, Amhara, which reported that safe MHM was more likely among adolescent girls who got information prior to menarche onset. Furthermore, a study from Nigeria indicated that safe MHM was common among adolescents who had premenarchial training [29]. A possible reason for this is that being aware of information about MHM enables adolescent girls to engage in safe MHM.
Participant residency was also found to be a predictor of MHM practice. Thus, an adolescent who is from an urban area practice safe MHM compared to a participant from a rural area. This result is congruent with findings from Amhara province and Aurangabad, India, which indicated safe menstrual hygiene management was lower among rural girls [30, 31]. The possible reasons may be due to better socio-economic status, better use of commercially available sanitary pads, and a good perception among urban resident girls [30, 32, 33]. However, this finding is in contrast with a comparative study conducted in Bahirdar where a significant difference was not observed between the rural and urban adolescent girls [27].
During menstruation, nearly 14% (n = 76, 13.17%) of adolescent girls have experienced vaginal infection. Furthermore, the odds of safe MHM practice were much lower when compared to their counterparts. A relatively much higher magnitude of infection was reported in a study conducted in Uganda where 47.2%, 54.3%, and 60.3% of the study participants experienced vaginal discharge, skin irritation, and itching or burning in the pelvic area during menstruation [26].
cause effect relationship. In addition, due to cultural sensitivity of the study and self-report it may subjected to social desirability bias.
Conclusion
More than half of the girls were practicing unsafe menstrual hygiene management. Evidence from the study indicated that having prior information about the menstruation cycle, residence area, knowing commercially available sanitary pads, the experience of infection around the vagina during menstruation, and age of the respondents were found to be factors affecting menstrual hygiene management practices among adolescent girls. As a result, we recommend that all respective stakeholders should work in collaboration to improving MHM practices during menarche among school adolescent girls.
Limitations of the study
We encountered several limitations in this study that should be considered when interpreting the findings. Data regarding the income status of a family, pocket money for the students, and the educational status of a family were not collected which might have influenced the result of this study if it had been collected. In addition, due to the cross-sectional nature of the study, it is not possible to establish a cause-effect relationship.
Data Availability
upon reasonable request to correspondent author this study’s supporting data and material is readily available.
Abbreviations
- MHM:
-
Menstrual hygiene management
- AOR:
-
Adjusted odd ratio
- COR:
-
Crude odd ratio
- CI:
-
Confidence Interval
References
Prateek S. A cross sectional study of knowledge and practices about reproductive health among female adolescents in an urban slum of Mumbai. J Fam Reprod Health. 2011, 5 (4): 117–124. 2011.
UNICEF, WHO. United Nations Children Fund and World health Organisation., “Progress on Drinking Water, Sanitation and Hygiene—Joint Monitoring Programme 2017 Update and SDG Baselines,” Who, p. 66, 2017. 2017.
Kuhlmann H. Walle. Menstrual Hygiene Management in Resource-Poor Countries. Obstet Gynecol Surv. 2017 Jun;72(6):356–376. doi: 10.1097/OGX.0000000000000443. PMID: 28661550; PMCID: PMC5482567. 2017.
Crofts F. Menstrual hygiene in Ugandan schools: an investigation of low-cost sanitary pads. J of Water, Sanit Hyg Dev. 2012;2(1):50–8. 2012.
Sommer S. Overcoming the Taboo: Advancing the Global Agenda for Menstrual Hygiene Management for Schoolgirls. Am J Public Health. 2013;103(9):1556–9. pmid:23865645. 2013.
UNICEF. Sharing sim[ple facts: useful information about menstrual health and hygiene. New Delhi, India: UNICEF India; 2008.
UNESCO. \Puberty Education & Menstrual Hygiene Management. Booklet 9. Paris, France: United Nations Educational, Scientific and Cultural Organization; 2014.
House, Mahon. Cavill. Menstrual hygiene matters: A resource for improving menstrual hygiene around the world. First Edit. London, UK: WaterAid; 2012. 1–354 p. 2012.
Kennedy S. Macintyre, Huggett, Wheen, Faiqoh. Menstrual Hygiene Management in Indonesia: Understanding practices, determinants, and impacts among adolescent school girls [Internet]. Indonesia; 2015. Available from: https://www.burnet.edu.au/system/asset/file/2034/2015_Menstrual_hygiene_management_Indonesia_FINAL_REPORT_February_2015_low_res. 2015.
Chandra-Mouli P. Mapping the knowledge and understanding of menarche, menstrual hygiene and menstrual health among adolescent girls in low- and middle-income countries. Reprod Health. 2017;14:30. doi: https://doi.org/10.1186/s12978-017-0293-6. 2017.
Annabel A. Worku, Woldemariam, Helen, Behailu. thiopia Young Adult Survey: a study in seven regions. Addis Ababa, Ethiopia: Population Council; 2010.
FMOH. Menstrual hygiene management in Ethiopia, An intersectional issue: Policy and implementation guideline. 2016.
UNICEF. Design and constraction manual for water supply and sanitary facilities in primary Schools in Ethiopia. 2012.
Fehr E. Effects of Water Security on adolescent girls in South Gondar Ethiopia. Emory University; 2011.
Tegegne S. Menstrual hygiene management and school absenteeism among female adolescent students in Northeast Ethiopia. BMC Public Health. 2014;14:1118. https://doi.org/10.1186/1471-2458-14-1118.
Gashaw T, Bantider A, Mahari A. Population dynamics and land use/land cover changes in Dera District, Ethiopia. Glob J Biol Agric Health Sci. 2014;3:137–40.
UNICEF. Water, sanitation and hygiene (WASH) in schools. Accessed on June. 2012;11:2014.
Tegegne TK, Sisay MM. Menstrual hygiene management and school absenteeism among female adolescent students in Northeast Ethiopia. BMC Public Health. 2014;14(1):1–14.
McGinnis SM, McKeon T, Desai R, Ejelonu A, Laskowski S, Murphy HM. A systematic review: costing and financing of water, sanitation, and hygiene (WASH) in schools. Int J Environ Res Public Health. 2017;14(4):442.
Dutta D, Badloe C, Lee H, House S. Supporting the Rights of Girls and Women through Menstrual Hygiene Management (MHM) in the East Asia and Pacific Region: realities, Progress and Opportunities. Bangkok, Thailand: UNICEF East Asia and Pacific Regional Office (EAPRO); 2016.
Mohammed S, Larsen-Reindorf RE, Awal I. Menstrual hygiene management and school absenteeism among adolescents in Ghana: results from a school-based cross-sectional study in a rural community. International Journal of Reproductive Medicine. 2020;2020.
Shallo SA, Willi W, Abubeker A. Factors affecting menstrual hygiene management practice among school adolescents in Ambo, Western Ethiopia, 2018: a cross-sectional mixed-method study. Risk Manage Healthc Policy. 2020;13:1579.
Sivakami M, van Eijk AM, Thakur H, Kakade N, Patil C, Shinde S et al. Effect of menstruation on girls and their schooling, and facilitators of menstrual hygiene management in schools: surveys in government schools in three states in India, 2015. J Global Health. 2019;9(1).
Upashe SP, Tekelab T, Mekonnen J. Assessment of knowledge and practice of menstrual hygiene among high school girls in western Ethiopia. BMC Womens Health. 2015;15(1):1–8.
Davis J, Macintyre A, Odagiri M, Suriastini W, Cordova A, Huggett C, et al. Menstrual hygiene management and school absenteeism among adolescent students in Indonesia: evidence from a cross-sectional school‐based survey. Tropical Med Int Health. 2018;23(12):1350–63.
Hennegan J, Dolan C, Wu M, Scott L, Montgomery P. Measuring the prevalence and impact of poor menstrual hygiene management: a quantitative survey of schoolgirls in rural Uganda. BMJ open. 2016;6(12):e012596.
Azage M, Ejigu T, Mulugeta Y. Menstrual hygiene management practices and associated factors among urban and rural adolescents in Bahir Dar city administration, northwest Ethiopia. Ethiop J Reproductive Health. 2018;10(4).
Omidvar S, Begum K. Factors influencing hygienic practices during menses among girls from south India-A cross sectional study. Int J Collaborative Res Intern Med Public Health. 2010;2(12):0.
Aniebue UU, Aniebue PN, Nwankwo TO. The impact of pre-menarcheal training on menstrual practices and hygiene of nigerian school girls. Pan Afr Med J. 2009;2(1).
Gultie T, Hailu D, Workineh Y. Age of menarche and knowledge about menstrual hygiene management among adolescent school girls in Amhara province, Ethiopia: implication to health care workers & school teachers. PLoS ONE. 2014;9(9):e108644.
Salve S, Dase R, Mahajan S, Adchitre S. Assessment of knowledge and practices about menstrual hygiene amongst rural and urban adolescent girls–A comparative study. Int J Recent Trends Sci Technol. 2012;3(3):1–3.
Paria B, Bhattacharyya A, Das S. A comparative study on menstrual hygiene among urban and rural adolescent girls of West Bengal. J family Med Prim care. 2014;3(4):413.
Thakre SB, Thakre SS, Reddy M, Rathi N, Pathak K, Ughade S. Menstrual hygiene: knowledge and practice among adolescent school girls of Saoner, Nagpur district. J Clin Diagn Res. 2011;5(5):1027–33.
Acknowledgements
We would like to acknowledge Haramaya University for covering the cost for data collection. Our gratitude also extends to Gursum Education office and data collectors for their collaboration.
Funding
This study is funded by Haramaya University. The funding organization had no role in the design and, data collection, or analysis, interpretation, and write up of this manuscript.
Author information
Authors and Affiliations
Contributions
“Y.M.D, B.Y, A.G, Y.T, and G.M.S contributed to conceptualization, design, data collection and manuscript write up whereas G.M.A and D.A contributed to data analysis, manuscript write, up drafting or revising the article.All Authors have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work”.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Prior to data collection, the proposal was reviewed and approved by Haramaya University, College of Health and Medical Sciences Institutional Health Research Ethics Review Committee/IHRERC/ using institutional ethics guide line adopted from Nuremberg code, Helsinki declaration, Belmont report, and WHO affiliated center of international organization for medical sciences (CIONS) and official ethical clearance was obtained. The study objective was explained to participant students and the participation was voluntary and confidential. A written and signed informed consent form was used to ensure willingness to participate in the study and confidentiality of data given. On top of that, informed consent was also obtained from parents/guardians, for participant less than 18 years old.
Consent for publication
During the data collection the study participants were informed and given their consent for the publication of the finding.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mulugeta Demmu, Y., Shifera, G.M., Ayana, G.M. et al. Menstrual hygiene management and associated factors among adolescent school girls in gursum district, Eastern Ethiopia: Institution-based a cross-sectional study. BMC Women's Health 23, 328 (2023). https://doi.org/10.1186/s12905-023-02461-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-023-02461-6