
Abstract
Background
With increasing global availability of medication abortion drugs, a safer option exists for many women to terminate a pregnancy even in legally restrictive settings. However, more than 22,000 women die each year from unsafe abortion, most often in developing countries where abortion is highly legally restricted. We conducted a systematic review to compile existing evidence regarding factors that influence women’s abortion-related decision making in countries where abortion is highly legally restricted.
Methods
We searched ten databases in two languages (English and Spanish) for relevant literature published between 2000 and 2019 that address women’s decision-making regarding when, where and how to terminate a pregnancy in sub-Saharan African, Latin American and the Caribbean countries where abortion is highly legally restricted.
Results
We identified 46 articles that met the review’s inclusion criteria. We found four primary factors that influenced women’s abortion-related decision-making processes: (1) the role of knowledge, including of laws, methods and sources; (2) the role of safety, including medical, legal and social safety; (3) the role of social networks and the internet, and; (4) cost affordability and convenience.
Conclusions
The choices women make after deciding to terminate a pregnancy are shaped by myriad factors, particularly in contexts where abortion is highly legally restricted. Our review catalogued the predominant influences on these decisions of when, where and how to abort. More research is needed to better understand how these factors work in concert to best meet women’s abortion needs to the full limit of the law and within a harm reduction framework for abortions outside of legal indications.
Similar content being viewed by others


Background
Globally, approximately 45% of abortions are considered unsafe, defined as a “procedure for terminating an unwanted pregnancy either by persons lacking the necessary skills or in an environment lacking minimal medical standards, or both” [1]. Nearly all of these unsafe abortions (97%) occur in low-resource settings where safe abortion is legally restricted and postabortion care services are limited [2]. However, medication abortion drugs, particularly misoprostol, have become increasingly available in low- and middle-income countries in recent years [3]. Access to and use of medication abortion drugs has dramatically impacted the abortion landscape in legally-restrictive settings and even more permissive settings with limited safe abortion services, presenting a safer option for women who self-manage their abortion outside the formal healthcare system [4,5,6,7,8,9]. Indeed, informal use of these drugs (e.g. obtaining them without prescription or from a source such as an online seller) in settings where abortion is illegal has been associated with decreased abortion-related complications [10,11,12]. In addition, because medication abortion drugs expand access to safe abortion care, people are better able to avoid unsafe abortion and its sequelae, exercise their rights, build healthy families and make better decisions about their futures [13].
Despite the availability of medication abortion, even in legally restrictive settings, evidence suggests use remains low [14, 15]. Understanding how women make decisions about what methods and sources to use when seeking to terminate a pregnancy can help to identify points of intervention that can shift women’s choices towards safer termination options, like medication abortion [16]. However, we currently lack a synthesis of the evidence regarding factors influencing women’s decision making around their abortion trajectory and the barriers that restrict some women’s use of safer termination methods and sources – especially in countries where abortion is highly legally restricted. Nearly all studies related to abortion decision making focus on the decision of whether or not to abort [17], and much is already known about individual characteristics and predictors of decision making [18].
Other systematic reviews on abortion in low-and middle-income countries have covered topics such as knowledge, attitudes, and practices among adolescents [19], abortion stigma [20] and abortion and long-term mental health outcomes [21]. These reviews help to shape our understanding of abortion overall but fail to synthesize evidence related to women’s experiences once they determine they will have an abortion. One recent review [22] points to myriad of reasons why women choose informal sector abortions, such as fear of mistreatment by staff, long waiting times, cost, privacy concerns, and insufficient knowledge – but this review is in the context of settings where abortion is legal.
Our review fills this gap by systematically synthesizing the literature related to how, when, and where women terminate their pregnancies and the factors that influence these decisions in legally restrictive settings after making the decision to terminate. In this review, we focus on the micro-level aspects of the abortion-seeking process in legally restrictive settings, synthesizing findings from studies exploring women’s individual decision-making processes. The review covers peer-reviewed studies published on countries in sub-Saharan Africa (SSA) and Latin America and the Caribbean (LAC) where abortion was ‘highly legally restrictedFootnote 1’ at the time of the study according to the Guttmacher-developed categorization [23]. We choose these geographies because they are under-represented in the literature on abortion-related decision making, because our team members work in these regions and could best interpret the literature, and to keep the scope manageable.
Methods
The Coast et al framework for women’s abortion-related care
We began our work by reviewing a conceptual framework developed by Coast et al. [24] for understanding women's trajectories in seeking abortion care. We found this framework useful as an anchoring point as it is evidence-based and comprehensively incorporates factors that may influence a woman’s trajectory to obtain abortion-related care. In the framework, the authors suggest that abortion-related care for an individual pregnancy includes the interaction of women’s abortion-specific experiences, their individual context, and the regional, national, and international context [24]. Given our aim to understand the individual factors related to women’s experiences making decisions about how, when, and where to abort, we concentrated on the domains of abortion-specific experiences (such as ability to access resources), as well as individual context (such as knowledge, beliefs, and individual characteristics). Throughout our analysis, we returned to this framework to cross-check our findings against the domains and individual components to ensure we were comprehensively capturing all content.
Search strategy
We searched PubMed, EMBASE, the Cochrane Library (reviews, protocols, and trials), WHO Regional Indexes, Ovid Global Health, JSTOR, POPLINE, CINAHL, and the Web of Science databases for relevant peer-reviewed articles in English and Spanish; we excluded French studies given the language limitations of the team. We restricted our search for articles published from 2000 to correspond with the signing of the United Nations Millennium Declaration—which signified the global community’s commitment to combating poverty and disease and whose indicators directed attention toward the need for safe abortion care—and to limit the review to a manageable twenty-year period that would reflect a contemporary summary of the evidence.
To keep the review narrow in scope, reflect the nature of the Coast et al. [24] framework, and focus explicitly on those whose experiences we sought to understand (i.e. women and girls themselves), we restricted our search to research involving women who had obtained an induced abortion. We included studies on all forms of induced abortion that met the criteria, including legal and illegal and safe and unsafe induced abortions. Studies focusing solely on the decision made regarding whether or not to abort and reasons for abortion were excluded. We also excluded studies on women treated for spontaneous abortion and those focused on the perspectives of providers and/or male partners of women who obtained an induced abortion.
We focused our search on the abortion-related decision-making process for women who obtained an induced abortion. Specifically, we focused on the individual aspects of how, when, and where women choose to induce an abortion. Decision-making for ‘how’ related to who performed the abortion (e.g. the woman herself, a trained clinician, or an unlicensed provider) and the type of procedure (e.g. medication or surgical). Decisions related to ‘when’ focused on the point in time during the pregnancy that women sought and obtained the abortion, or factors that contributed to delays in seeking or obtaining care. Finally, decisions on ‘where’ involved geographic considerations (such as proximity to women’s homes) and the provider/facility type (e.g. private, public, informal healthcare sector). We cross-checked our search terms against relevant components of the Coast et al. framework throughout the search process [24]. This review is limited to peer-reviewed articles published in English or Spanish and that focused on the direct experiences of women who report obtaining an induced abortion. The countries included in the study also have vastly differing types of legal restrictions related to abortion. But they share several similar trends related to abortion. Rates for abortion are fairly similar in the two regions, ranging between 36 (Africa) [25] and 44 per 1000 women (Latin America) [26]. In both regions, more than 95% of women of reproductive age live with restrictive abortion laws [23].
We conducted the search in two phases. The first search took place in June 2019 and the second was an update to the review in June 2022, during which time we screened articles published after mid-2019 through mid-2022. While the exact search terms varied by database, the searches all included three components: (1) abortion; (2) women’s experience/decision-making, and; (3) geography. Our final list of search terms is included in Additional file 1: Document 1. We registered the protocol for the systematic review to PROSPERO and reported results using PRISMA guidelines [27].
Article selection, article quality evaluation and analysis
After removing duplicate search results, we imported all remaining articles into Covidence online systematic review software for title, abstract, and full-text screening [28]. Two reviewers independently screened the title and abstract of each article identified in the search to determine whether the study met the inclusion criteria. Any discrepancy between reviewers was resolved by the full team of reviewers, who jointly made the final decision about whether the paper was included in the full-text review. Once the title and abstract screening was complete, two reviewers independently conducted the full text review of each potentially eligible article. Reviewers again resolved any disagreement over the inclusion of an article through discussion. We evaluated the quality of all included studies using an adaptation of the Critical Appraisal Programme (CASP) quality assessment tool [27]. Results of quality assessment are available on request. Two reviewers independently assessed each article and assigned an overall quality ranking of “low”, “medium”, or “high” quality. Reviewers resolved all discrepancies in these rankings through discussion. We used a standardized form to extract data relevant to the following categories: author names and title; publication and study years; study aim(s); study design; sampling strategy; data collection methods and setting; sample size and characteristics; inclusion and exclusion criteria; analysis methods; and relevant sample for the systematic review. We did not exclude any studies based on the quality assessment. Relying on Thomas and Harden’s [29] thematic synthesis approach, we iteratively and collaboratively abstracted findings into analytical themes. Table 1 [see end of document] highlights the studies included in the review.
We uploaded included articles into Nvivo and coded them using a codebook based on the Coast et al. framework. We double coded approximately 20% of articles for inter coder reliability, resolving all discrepancies in coding and finalizing the codebook. We coded relevant sections of the articles, mainly in the results sections, pertaining to findings that fit within our inclusion criteria. This meant that we included any findings related to women who had an induced abortion in the included countries/regions. Content from countries or regions outside our scope, from additional perspectives beyond women who had induced abortions, or not related to the decision-making process around when, where and how to abort was excluded.
Results
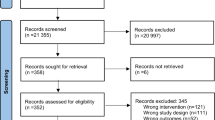
The initial Phase 1 search conducted in 2019 yielded 11,620 articles. After removing duplicates in EndNote, we imported 6787 articles into Covidence, which identified a further 17 duplicates, and screened the titles and abstracts of 6770 unique articles. We identified 95 potentially relevant articles and retrieved the full text manuscript for further evaluation. After completing full text reviews, we excluded 59 articles from the sample, leaving 36 articles that met study inclusion criteria. The Phase 2 search began with 2043 articles, of which 1874 were imported into Covidence for title and abstract screening, after duplications were removed. We identified 23 potentially relevant articles and reviewed the full text of each manuscript; of these, ten were included.
See Fig. 1 for the flow diagram of the search.

PRISMA Flow diagram of study inclusion process
Of the 46 studies included in the systematic review, 40 were qualitative, four employed a mix of quantitative and qualitative methods, and two were exclusively quantitative. Our analysis synthesized findings from primary research conducted across 21 countries: twelve countries in sub-Saharan Africa and nine in Latin America and the Caribbean. The studies varied greatly with regard to methodological rigor and depth of analysis. Most studies (n = 20) met the high-quality rating on our CASP quality assessment tool while 18 articles were rated medium quality and eight were rated low quality. The characteristics of the 46 studies included in our synthesis are reported in Table 1, along with their CASP assessment rating.
Thematic findings
The findings of this review are organized across four broad themes: (1) the role of knowledge; (2) the role of safety; (3) role of social networks and the internet, and; (4) cost, affordability and convenience. In addition to direct quotes from participants cited in the reviewed studies, we use quotes from authors that summarize findings from their own research.
The role of knowledge
The role of knowledge factored prominently into women’s decisions regarding how, when, and where to terminate their pregnancy. This included aspects broadly related to knowledge of the abortion law and knowledge of methods and sources of abortion. These two categories of knowledge acted upon women’s abortion-related decisions directly and indirectly as described below.
Knowledge of law
Knowledge of abortion laws affected women’s abortion-related decision-making by impacting their perceived or actual choices [30,31,32,33,34,35,36,37,38,39,40]. The impact of one’s knowledge of the abortion law varied by what those views entailed. Women’s understanding that abortion was broadly illegal, regardless of whether their knowledge was accurate, was associated with fear of potential legal or other repercussions of seeking care at a formal health facility. Thus, perceptions of illegality restricted women’s choices were linked to use of less medically safe (as distinct from socially or legally safe) abortion methods and sources [31,32,33, 36, 37]. This perception is illustrated by one woman in Atkaro et al. [31] I knew that it is illegal to have an abortion in Ghana and so I could not have gone to any facility to have by pregnancy terminated. All my friends that I asked only recommended some herbal mixture called agbeve for me… Although I know I could bleed to death from terminating my own pregnancy, I didn’t have a choice or options. So, I used the agbeve herbal mixture.
Many women who were unsure of the law or who had anxiety about whether their situation qualified as a legal indication tended to seek abortion outside the formal health sector [31,32,33, 36, 37]. As Izugbara et al. [36] summarized: Respondents generally believed that abortion is illegal in Kenya, mentioning the Kenyan media, religious leaders, health providers, family, friends, and schools as sources of their information on the criminality of abortion. Given the presumed illegality of abortion in Kenya, safe abortion was also understood in terms of procedures and providers that shielded women from the law and arrest.
As such, not knowing the legality of abortion or the exceptions in the law presented barriers to timely care [33]. Conversely, learning about conditions under which women could seek or be eligible for legal abortion services tended to positively impact women’s abortion-related decision-making [32, 34, 37], for example, giving participants more confidence to advocate for themselves and their desires, and empowered to make well-informed decisions [34]. The process of learning about available legal services was often facilitated by an advocacy group or legitimate service provider [33].
Knowledge of methods and sources
Women’s knowledge of specific abortion methods and sources was a proximal factor that directly impacted their abortion-related decisions. Lacking awareness of methods and sources was common [30, 31, 33, 34, 39, 41,42,43,44,45,46,47,48] and was an obstacle to women using a medically safe method or source in one of two ways: either women would act upon the limited knowledge they had, which tended to lead them to obtain an unsafe abortion; [31, 39, 46] or their lack of knowledge led to delays, which in effect limited their options as a result of later gestational age [33, 34]. Regarding the latter experience, Seid et al. [39] summarized findings as such: Lack of information and knowledge about safe abortion services is the barrier. If they (women) do not have information, they hesitate to decide and as time goes, they do not have the chance to terminate their pregnancy. The only option they have may be giving birth.
Whether a woman had or could access information about safe abortion methods and sources was often related to her demographics. Rural, older, and less educated women, as well as those with less social capital (namely not having medical providers in their social network) were unlikely to have adequate information to make an informed decision and use a safe method [39, 47,48,49] While many women are aware of both safe and unsafe methods or sources, knowledge of misoprostol and mifepristone specifically appeared more common among younger women [48]. In one Kenyan study, information about abortions came from informal social networks from high school and from friends with a prior abortion experience [30, 50].
A lack of knowledge about methods and sources was not necessarily linked with a preference for a certain type of method; in fact, incomplete information led to significant misperceptions and heterogeneity in preferences [42]. It also resulted in incorrect use of medical abortifacients and concerns about product effectiveness. In some cases, this contributed to women preferring surgical abortion while for others, it led to a preference for medical abortion.
In societies where abortion is highly stigmatized, women tend to lack access to information about safe abortion methods or where they can be procured [51, 52]. As Kebede et al. [51] points out: ‘all [women in the study] struggled to access information about abortion possibilities and attributed this difficulty to the morally charged silence surrounding abortion and premarital sexual activity.’ Even in countries with more permissive laws, participants were often unaware of them because of the shroud of taboo [34].
The role of safety
In addition to women’s knowledge, their perceptions of medical, legal, and social safety were significant factors in their decision making regarding how and where to terminate their pregnancy [31, 33, 36,37,38,39,40,41,42, 44, 47, 48, 51,52,53,54,55,56,57,58,59,60,61]. While women strongly preferred their abortions to be medically safe, concerns about legal and social safety often prevailed, leading women to have a medically unsafe termination.
Perceptions of medical safety and quality
In the absence of other influencing factors, women strongly preferred medically safe abortion methods and services [37, 48, 52, 55, 56, 62]. Based on a study in Ghana, Esia et al. [55] summarized that ‘All the respondents indicated that they preferred to have abortion at recognized facilities and by recognized practitioners so as to make it safe’ However, there was significant variation in what methods women perceived as most safe. One study found that women perceived abortions induced by ingesting substances to be safer than surgical abortions because they associated surgical equipment with a greater risk of complications like infections [51]. In other cases, women stated preferences specifically for medical abortion due to the perception of lower health risks [48, 58, 63]. Regardless of preferred method or source, women’s preferences for medically safe abortions were often overridden by greater concerns about legal and social safety.
Women’s perceptions of the quality of care provided at facilities played a role in the decision-making process regarding where to seek abortion services [36, 37, 43, 44, 47, 51, 55,56,57, 59, 62] These perceptions included likelihood of respectful care and willingness of the provider to perform the requested procedure [33, 34, 57]. In Nigeria, perception of care had more to do with having a good reputation, i.e. not being a “quack [43, 62]”: “They noted that individuals who seek care from so-called “quacks” suffered from side effects and “regret it,” but for those who obtain services from a qualified provider “there won’t be any problem [62].”
Respectful care was generally identified as provider(s) having the interpersonal skills necessary to treat women with unwanted pregnancies – regardless of sociodemographic or marital status – with empathy and respect [33, 34]. Two studies found that women expected to experience disrespectful care (such as manipulating women to carry to full term or belittling a woman’s decision to abort) at public health facilities, leading them to instead choose facilities or providers recommended by friends [40, 57].
Perceptions of legal safety
Fear of legal repercussions often superseded women’s preferences for medically safe abortion methods and services, leading them to attempt to self-induce using unsafe methods and/or seek care from clandestine providers [31, 37, 38, 40, 49, 64]. In other instances this led women to withhold information from postabortion care (PAC) providers about their previous attempts to self-induce [40, 48, 58]. As Rominski, Lori, and Morhe [38] found: The legal status of abortion was mentioned by all groups of participants as a reason for why women self-induce rather than come to facilities for abortion services. Prosecution of women, or their providers, due to inducing an abortion is rare, but women are afraid of this potentiality.
As reported by Manriquez et al. [46]. women often lie to PAC providers about their attempts to self-induce for fear of legal consequences. This is in accordance with advice from harm reduction information handbooks, which enabled women to receive treatment while ‘reducing the risk of rejection and denunciation’ [48]. In interactions with providers, these investigators observed that ‘None of these women mentioned they had induced an abortion. They had all decided not to tell in advance. To ensure they succeeded in this they kept silent, denied it, lied, accepted rough treatment, did not express any pain, and did not ask for information.’ [48].
Even if providers had their suspicions, women’s fears of legal punishment often led them not to reveal prior attempts to self-induce or receipt of induced abortion care from clandestine providers [38, 46].
Perceptions of social safety
Of all three types of safety concerns—medical, legal, and social—concerns for social safety had the greatest influence on women’s decisions regarding how and where to terminate their pregnancy [33, 36, 38, 39, 41, 43, 44, 47, 48, 51, 53, 56, 58,59,60,61,62, 65]. Social safety encompasses abortion providers’ and others’ ability to maintain the secrecy of a woman’s abortion experience. Fear of stigma or social repercussions influenced women’s decisions about which method to use, but not consistently towards or away from any particular method [48, 53, 58, 59, 62, 66]. Women who preferred medical abortion cited the increased privacy possible through minimizing the number of hours spent in a hospital, as well as the risk of being recognized by or experiencing unwanted attention from others at or near the facility [38, 41, 44, 48, 58, 59, 64,65,66]. As one participant reported from Chile: “I am grateful that I was able to do this (abortion) quietly, alone in my home, and not with doctor [64].” However, the same motivation for privacy led other women to select other methods or sources [36, 38, 44, 56, 59]. Women who preferred surgical abortion appreciated a sense of privacy from fewer visits in comparison to medical abortion, which women believed may involve multiple visits in the case of excessive bleeding, which they perceived as a common side effect [44, 56, 59].
Fear of stigma or social repercussions caused many women—particularly young, unmarried women—to choose riskier methods or services in order to reduce the social risks [33, 38, 41, 47, 51]. Young women were likely to ingest harmful substances and/or avoid formal healthcare settings initially because of a desire to keep the abortion private and avoid involving their parents [47, 51, 53, 60] or social network [39, 47, 51, 53, 60, 61]. The perceived lack of confidentiality in high-profile health facilities led women to prefer to terminate elsewhere even when the high-profile facilities were thought to have the best equipment and providers [36, 51]. These concerns were particularly acute for young girls, who feared that these more legitimate facilities may contact their parents or guardians [41, 59].
Finally, fear of stigma or social repercussions led some women to choose services distant from their home [41, 42, 47, 48, 51, 52], and to choose discrete albeit unsafe methods and places to terminate the pregnancy [51, 53, 58, 60]. As Mohamed et al.[60] found: ‘In addition to strong religious and cultural beliefs preventing women from seeking out abortion services at healthcare facilities, many communities also use stigma, isolation and shame as tools to ensure that women do not break from tradition.’
Role of social networks and the internet
Social networks mainly influenced women’s decision regarding how and where to terminate a pregnancy through sharing of information and experiences [30,31,32,33, 35, 36, 38, 40, 41, 43, 45, 47, 50, 59, 61, 62, 64, 65, 67,68,69,70,71,72,73]. There was no uniform narrative about who a woman tells, gets information from, or involves in her decision-making process. Women most often involved their friends [32, 35,36,37, 40, 41, 43, 46,47,48, 50, 55, 58, 62, 65, 70, 71, 73], partners [30, 31, 34,35,36,37,38, 41, 46, 48, 54, 64, 67, 68, 70, 71, 74], and/or family [32, 35, 36, 48, 52, 61, 62, 70, 72, 74], in the decisions related to how, when, and where to abort. Health providers [32, 61, 68] and strangers or acquaintances [43], neighbors [32, 62], “feminist activists [64]” or other NGO staff [32] and abortion ‘brokers’ [45, 51] were also consulted, but with less frequency.
These articles suggested that social networks have significant influence over whether a woman ultimately has a safe or unsafe abortion by affecting her perceptions of methods and sources and their corresponding social and medical safety. In some cases, friends led women to have safe abortions [32, 33, 45, 47, 62], but in many cases they recommended unsafe options [31, 46, 47, 51, 70, 71]. The information and support that women received from friends was often related to her and her network’s social standing. Women of higher socioeconomic status and education, as well as those with connections to people in academic and health sectors, were more likely to experience safe abortion [33, 47, 54, 61, 62, 67], whereas women from social networks who lacked information or connections to knowledge or knowledgeable people tended to experience unsafe abortions [31, 36, 70, 71]. Regardless of the actual method or service they chose, women perceived that their choices were safer if they relied on information from trusted friends [32, 36, 37, 40, 41, 47, 48, 55, 57, 62, 70] or people who had previously successfully aborted [30, 38, 42, 48, 62, 64, 73]. In many cases, involving family members resulted in less safe abortions, especially when it involved unskilled family members as the providers of the abortion method [35, 36, 56, 61, 72]. In contrast, one article suggested that a lack of involvement of any friend or family member in the decision-making process, whether a result of preference or social isolation, led to less safe abortions [51].
When male partners were involved, they were typically most instrumental during the procurement phase—e.g. going as a surrogate to a chemist or pharmacy, identifying a facility-based provider, or financing the procedure [30, 31, 35, 36, 38, 41, 44, 46, 48, 52, 54, 67, 70, 74] In many of these instances, male partners also made the decisions about method and source on behalf of the woman; however, it was not always clear whether this was a situation preferred by the woman or whether she would have liked to be involved in the decision-making.
Women who sought an induced abortion sometimes (but not always) used the internet for abortion decision-making. In some cases, the internet was the main source of information for determining where and how to abort, especially for determining legality of abortion in different states and/or how to get pills [32, 64, 75]. In other cases, women with strong networks did not use the internet or support services to navigate the abortion-seeking process: “[In Chile], Most participants did not contact [Women Help Women] WHW during the abortion process because they did not need more information, or because they had support from other feminist organizations, acquaintances who had had abortions and trusted health professionals, with whom they could communicate via instant phone messaging [64].”
Cost, affordability and convenience
Evidence suggests that the perceived cost and affordability of specific services often influenced women’s decision-making related to abortion care seeking [30, 34, 36, 40, 41, 51,52,53, 55, 61, 65]. Some women’s knowledge of safe methods and sources was high, but barriers such as cost and affordability prevented utilization of those methods and sources [30, 36, 49, 51, 53], with perceptions of service affordability linked to women’s economic status and ability to pay [34, 59]. The most obvious way that cost and affordability impacted decision making was regarding whether to get services in public or private facilities. Women with more limited financial resources opted almost unanimously to patronize public clinics or other non-clinical providers in contrast to wealthier women who were more likely to seek services at private facilities [40, 53, 55, 65]. Further, women who were financially better off could procure pregnancy tests earlier following suspicion of pregnancy, which meant the gestational age at which they were making decisions regarding how, when, and where to terminate was earlier compared to women who were economically disadvantaged [54]. As such, because access to early care skewed towards wealthier women, less financially secure women were confronted with greater challenges and vulnerabilities as a consequence of delayed care seeking [51, 53].
Cost and affordability also impacted decision-making on which method—surgical or medical—women chose for their abortion. In general, if women could afford it, they wanted a method that they perceived as quick, efficient, and as painless as possible [44]. Some women viewed a surgical procedure conducted by a doctor as the best option, while others viewed going to a chemist for a medical procedure as best [30, 44, 49]. As reported by Loi et al.[30] Some women [i.e. participants] stated they knew about Marie Stopes, a reliable abortion provider; however, due to high transportation fees they opted for medical abortions using Misoprostol, which was provided by chemists.
Thus, poorer women were more likely to be constrained in their ability to operationalize their abortion preferences. In some situations, such as in Chile, affordability was a main reason for why women chose to use certain services, including abortion access organizations like Women Help Wome [64]. However, a few studies did not find that cost or affordability were predominant factors in women’s decisions related to when, where, and how they terminated [47, 56, 57, 66].
Finally, several studies showed that decisions about where and how to abort were related to convenience, including factors such as distance to the provider [32, 65], time spent waiting on medical abortion (i.e. pill) shipments [64], or simply a lack of other options: As one Nigerian participant stated, “The reason I came to [clinic name] is because I do not have any alternative” (Age 41, clinic) [62].
Discussion
Our systematic review findings illustrate there are many factors that influence the decision-making process of women obtaining an abortion in highly restrictive legal settings. These results resonate with the Coast et al. conceptual framework of explanatory factors influencing women’s abortion trajectories and, like the framework suggests, highlight how these factors are interrelated and dynamic [24].
Women’s perceptions of abortion method/source safety matter in terms of how, when, and where they induce. Concerns such as fears of legal repercussions and social stigma often supersede preferences for medical safety in these contexts. The ability to maintain discretion and keep the abortion secret is a significant factor motivating many women’s abortion-related decisions; women seek an abortion far from home, in low-quality facilities, or use potentially unsafe methods to minimize the likelihood of being seen by or having their personal information shared with family, friends, or community members. The importance of safety, especially as it relates to discretion, has been shown in other literature as well [20, 76, 77] including for women seeking informal sector abortions in legally permissive settings [22]. This review adds further context of how these perceptions continue to complexly influence those individuals who have already decided to abort. It also extends scholarly understanding of the intersections of women’s abortion care-seeking choices with national legal contexts, highlighting the combination of factors that weigh on women’s decisions as they negotiate access to services.
We found that knowledge of laws, sources, and methods play an important role in women’s abortion decisions related to how, when and where to abort. Similar to what has been found elsewhere, women resort to making choices that are less medically safe where knowledge is limited and abortion is highly stigmatized [22, 76, 78]. Conversely, when women access accurate information even in contexts with highly restrictive abortion laws, they make safer choices and can act more quickly, reducing delays and potential for complications associated with later termination.
The social environment plays a critical role in women’s decision-making. Social networks are key, and women’s decision-making processes and resultant experience of safety is related to the information and resources in their network. Other studies have similarly found that social networks can help women determine how to obtain a clandestine and safe abortion [22, 79] and drive them to a safe abortion experience [76]. Demographics are also related to one’s social network, which has direct implications for the types and quality of information and resources women receive from people within those networks. One’s socioeconomic characteristics can narrow available options, either directly through cost and logistical barriers or indirectly through a less connected and knowledgeable social network and decrease the likelihood that those options involve a medically safe abortion experience. We also found that where social norms dictate that abortion is highly stigmatized, women know little about the abortion laws, have less social support, and thus have fewer viable options regarding where and how to terminate a pregnancy [20].
Our findings speak to the interrelatedness of these three domains, a central aspect of the Coast et al. framework [24]. Women with inaccurate or incomplete information, as well as those who are delayed in learning their pregnancy status and/or with limited social connectivity or support delay care-seeking and have fewer options available to them. While similar findings are echoed in more legally permission settings [22, 76], highly restrictive settings such as those seen in this review may further stigmatize, limit and negatively shape women’s choices and the consequences of those choices.
To support women’s decision-making and their use of safer methods, we must consider how women’s individual perceptions – of care, cost, and safety in the broader sense–shape their choices, and are shaped by their environment, including their social networks.
Policy and programmatic interventions that emphasize and maintain confidentiality are a high priority for women and providers alike, as are social and behavior change interventions that provide women with information about legal exceptions and where they can obtain safe abortion methods. Even in highly restrictive settings, policies, resources, information and counseling services focused on strengthening women’s knowledge of legal indications and supporting them to self-manage their abortion could be made more broadly available [80, 81]. Policies that promote access to quality and timely reproductive health knowledge will ensure that women in all settings have the requisite information to make life-saving decisions that are within legal limits, but that also do not compromise their health. Abortion policy interventions need not only to connect to legal stipulations, but also to what is happening on the ground and to the lived realities of women. Program and policies that support women’s resort to health promoting social networks will save lives and improve long-term wellbeing. Sustained evidence-informed policy engagement is also urgently needed to ensure that decision-makers always rely on robust data to design and implement reproductive health and other policies.
Several studies have shown how even in highly legally restricted countries, women can be supported with information on what to do about an unplanned pregnancy, where to seek support, and how to arrive at a safe decision [76, 79]. The internet and hotlines can be a resource for many women, regardless of their social network and demographics, that increases knowledge of safe methods, sources, and what to expect. Our review shows the internet is burgeoning space for consultation and action. Formal harm reduction programs – including internet-based telemedicine, hotlines, and accompaniment models – that present safe abortion options in legally restrictive settings have had success supporting women to terminate safely [14, 76,77,78,79,80,81,82,83,84,85,86]. However, existing laws constrain such programmatic efforts; thus, program managers need to exercise caution to limit program’s exposure to legal or other repercussions. One such way is to work closely with local stakeholders and civil society organizations to ensure buy in and support for these harm reduction efforts.
Our findings underscore that many women still know about and use a range of unsafe methods to terminate an unintended pregnancy; thus, even in highly restrictive settings, quality PAC must be available for treatment of abortion-related complications. Although medical abortion is gaining popularity and may meet some women’s preferences for what they deem most ‘safe’ (socially), some women will continue to prefer surgical abortion for a variety of reasons, even with all safety considerations being equal.
Although this review unearthed several important findings, gaps remain – especially as we reflect on the Coast et al.[24] framework, such as how previous abortion experiences and women’s autonomy and self-efficacy influence decision-making. Available literature used as part of this review only superficially addressed women’s disclosure experiences, especially related to negotiation during the decision-making process, which suggests this is an area of further inquiry. We reviewed little information about power imbalances within relationships and gender norms facilitate or inhibit women’s ability to enact their abortion preferences. In addition, the literature in this review did not untangle how non-linear trajectories impact decision-making on how, when, and where to abort. More research is needed to fully understand the many factors that influence women’s abortion decision-making in highly legally restrictive settings, and to make comprehensive programmatic and policy recommendations. Our findings also highlight the need for more research on whether and how interventions to promote access to safe abortion in highly restrictive legal contexts are addressing the decision-making trajectories of women seeking abortion and promoting access to services that are both medically and socially safe for women.
We conducted our review within the bounds of the search criteria and the assets of the team, which constrained the geographic, linguistic, and timeframe scope. This is especially true for articles in French and Portuguese, as many of the countries included in this review speak those language predominantly. Relatedly, included studies concentrated in only a few of the many countries in Latin America and Africa so findings and recommendations may not be representative of or relevant to the entirety of those regions. We also restricted our search to peer-reviewed articles. As such, we may have excluded pertinent literature, including studies published in the grey literature or in French. Other decisions we made to focus the scope of our review, such as including only articles presenting data from women with first-hand experience, meant some rich, seminal articles about the decisions of how, when and where to abort were excluded (e.g. those showcasing providers’ perspectives). Included literature is likely limited to individuals identifying as women, and as such does not reflect the experiences of individuals who may not identify as women, to which the issue of abortion decision-making may still apply. Guttamcher’s 2017 country categorization of legality [23] is one of several tools available for understanding the legal context of abortion globally, and our use of it means we included countries with vastly differing legal contexts into this review. Many of the same factors influencing the decision to abort are the same as those influencing when, where and how; as such we may not have full distinction between the two decision-making processes in our synthesis.
The abortion decision-making process is complex. We focused on articles that explicitly discussed the choices and decisions that individuals made in varying contexts; most often, these were decisions that women were aware they were making. However, women make implicit decisions, in these cases often forced on them by circumstance – be that poverty, option scarcity, or within limited social networks. Our review does not cover passive or implicit decision making nor an investigation of the cognitive aspects related to decision-making that might be at play in one’s abortion trajectory.
Despite these limitations, our review contributes knowledge on decisions that women make related to abortion care-seeking after they have made the decision to terminate in a legally restrictive setting. This is a priority research area as the decisions a woman makes during this time determine whether she obtains a safe abortion, can exercise her human right to bodily autonomy, and impacts the likelihood of experience related injuries or even death. We used rigorous and comprehensive search methods involving 10 databases and employed a thorough article screening process involving two reviewers. Diversity on our team allowed us to include articles in Spanish, in addition to English, and represent research across diverse settings.
Conclusion
Women’s decision-making process related to how, when and where to terminate a pregnancy in SSA and LAC countries with highly restrictive abortion laws is complex and shaped by myriad factors. This review provides important insight regarding what influences women’s termination trajectories and their impact on the safety of women’s abortions and their ability to decide their future. Understanding what aspects of available abortion options, or lack thereof, women prioritize in their decision-making process can enable stakeholders to better meet women’s abortion needs to the full limit of the law and maximize access to safer options within a harm reduction framework for those abortions obtained outside legal indications. More research is needed to understand these factors and make comprehensive policy and programmatic recommendations in legally restrictive settings.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study. All data used in this paper has been published elsewhere, and the full list of references is available in the paper.
Notes
We used Guttmacher’s ‘Abortion Legality Worldwide’ map and their definition of any country scoring between 1 and 4 as ‘highly legally restrictive’[86]. We did not include countries ranked as a 5 or 6, which related to countries where abortion was defined as broadly legal.
References
Organization WH. Preventing unsafe abortion. 2021.
Ganatra B, Gerdts C, Rossier C, Johnson BR, Tunçalp Ö, Assifi A, et al. Global, regional, and subregional classification of abortions by safety, 2010–14: estimates from a Bayesian hierarchical model. Lancet. 2017;390(10110):2372–81.
Footman K, Keenan K, Reiss K, Reichwein B, Biswas P, Church K. Medical abortion provision by pharmacies and drug sellers in low- and middle-income countries: a systematic review. Stud Fam Plann. 2018;49(1):57–70.
Stillman M, Owolabi O, Fatusi AO, Akinyemi AI, Berry AL, Erinfolami TP, et al. Women’s self-reported experiences using misoprostol obtained from drug sellers: a prospective cohort study in Lagos State, Nigeria. BMJ Open. 2020;10(5):e034670.
Moore AM, Blades N, Ortiz J, Whitehead H, Villarreal C. What does informal access to misoprostol in Colombia look like? a mystery client methodology in Bogotá and the coffee axis. BMJ Sex Reprod Heal. 2020;46:294–300.
Hyman A, Blanchard K, Coeytaux F, Grossman D, Teixeira A. Misoprostol in women’s hands: a harm reduction strategy for unsafe abortion. Contraception. 2013;87:128–30.
Erdman JN, Jelinska K, Yanow S. Understandings of self-managed abortion as health inequity, harm reduction and social change. Reprod Health Matters. 2018;26:13–9.
Moseson H, Herold S, Filippa S, Barr-Walker J, Baum SE, Gerdts C. Self-managed abortion: a systematic scoping review. Best Pract Res Clin Obstet Gynaecol. 2020;63:6387–7110.
Harper CC, Blanchard K, Grossman D, Henderson JT, Darney PD. Reducing maternal mortality due to elective abortion: potential impact of misoprostol in low-resource settings. Int J Gynecol Obstet. 2007;98(1):66–9.
Faúndes A, Santos LC, Carvalho M, Gras C. Post-abortion complications after interruption of pregnancy with misoprostol. Adv Contracept. 1996;12(1):1–9.
Juarez F, Singh S, Garcia SG, Olavarrieta CD. Estimates of induced abortion in Mexico: what’s changed between 1990 and 2006? Int Fam Plan Perspect. 2008;34(4):158–68.
Miller S, Lehman T, Campbell M, Hemmerling A, Brito Anderson S, Rodriguez H, et al. Misoprostol and declining abortion-related morbidity in Santo Domingo, Dominican Republic: a temporal association. BJOG Int J Obstet Gynaecol. 2005;112(9):1291–6.
Center for Reproductive Rights. Safe and legal abortion is a woman’s human right. New York; 2011.
Bell SO, Sheehy G, Hyacinthe AK, Guiella G, Moreau C. Induced abortion incidence and safety in Côte d’Ivoire. PLoS ONE. 2020;15(5):e0232364.
Bell SO, Omoluabi E, Olaolorun F, Shankar M, Moreau C. Inequities in the incidence and safety of abortion in Nigeria. BMJ Glob Heal. 2020;5(1):1814.
World Health Organization. Safe abortion: technical and policy guidance for health systems Second edition technical and policy guidance for health systems. Geneva; 2012.
Yao Gbagbo F, Amo-Adjei J, Laar A. Induced abortion decision-making in accra decision-making for induced abortion in the accra metropolis, Ghana. Afr J Reprod Health March. 2015; 19
Chae S, Desai S, Crowell M, Sedgh G, Singh S. Correction: Characteristics of women obtaining induced abortions in selected lowand middle-income countries. PLoS ONE. 2017;12(3):e0172976. https://doi.org/10.1371/journal.pone.0172976.
Munakampe MN, Zulu JM, Michelo C. Contraception and abortion knowledge, attitudes and practices among adolescents from low and middle-income countries: a systematic review. BMC Health Serv Res. 2018;18:1–13.
Hanschmidt F, Linde K, Hilbert A, Riedel- Heller SG, Kersting A. Abortion stigma: a systematic review. Perspect Sex Reprod Health. 2016;48(4):169–77.
Charles VE, Polis CB, Sridhara SK, Blum RW. Abortion and long-term mental health outcomes: a systematic review of the evidence. Contraception. 2008;78:436–50.
Chemlal S, Russo G. Why do they take the risk? A systematic review of the qualitative literature on informal sector abortions in settings where abortion is legal. BMC Womens Health. 2019;19(1):1–11.
Guttmacher Institute. Abortion Legality Worldwide. 2017.
Coast E, Norris AH, Moore AM, Freeman E. Trajectories of women’s abortion-related care: a conceptual framework. Social Sci Med. 2018;200:199–210.
Guttmacher Institute. Fact Sheet: Abortion in Africa. New York; 2018.
Guttmacher Institute. Fact Sheet: Abortion in Latin America and the Caribbean. New York; 2018.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7): e1000097.
Covidence systematic review software. Melbourne, Australia.: Veritas Health Innovation;
Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):45.
Loi UR, Lindgren M, Faxelid E, Oguttu M, Klingberg-Allvin M. Decision-making preceding induced abortion: a qualitative study of women’s experiences in Kisumu, Kenya 11 medical and health sciences 1117 public health and health services. Reprod Health. 2018;15(1):1–12.
Atakro CA, Addo SB, Aboagye JS, Menlah A, Garti I, Amoa-Gyarteng KG, et al. Contributing factors to unsafe abortion practices among women of reproductive age at selected district hospitals in the Ashanti region of Ghana. BMC Womens Health. 2019;19(1):1–17.
Juarez F, Bankole A, Palma JL. Women’s abortion seeking behavior under restrictive abortion laws in Mexico. PLoS ONE. 2019;14(12):1–22.
Brack CE, Rochat RW, Bernal OA. “It’s a race against the clock”: a qualitative analysis of barriers to legal abortion in Bogotá. Colombia Int Perspect Sex Reprod Health. 2017;43(4):173–82.
Depiñeres T, Raifman S, Mora M, Villarreal C, Foster DG, Gerdts C. “I felt the world crash down on me”: women’s experiences being denied legal abortion in Colombia. Reprod Health. 2017;14(1):1–9.
Hill ZE, Tawiah-Agyemang C, Kirkwood B. The context of informal abortions in rural Ghana. J women’s Heal. 2009;18(12):2017–22.
Izugbara CO, Egesa C, Okelo R. “High profile health facilities can add to your trouble”: women, stigma and un/safe abortion in Kenya. Soc Sci Med. 2015;141:9–18.
Keefe-Oates B, Makleff S, Sa E, Forero LJ, Mendoza D, Olaya MA, et al. Experiences with abortion counselling in Mexico City and Colombia: addressing women’s fears and concerns. Cult Heal Sex. 2019;0(0):1–16.
Rominski SD, Lori JR, Morhe ESK. My friend who bought it for me, she has had an abortion before. The influence of Ghanaian women’s social networks in determining the pathway to induced abortion. J Fam Plan Reprod Heal Care. 2017;43(3):216–21.
Seid A, Yeneneh H, Sende B, Belete S, Eshete H, Fantahun M, et al. Barriers to access safe abortion services in East Shoa and Arsi Zones of Oromia regional state. Ethiopia Ethiop J Heal Dev. 2015;29(1):13–21.
Yegon E, Kabanya P, Echoka E, Osur J. Abortion-related stigma and unsafe abortions: perspectives of women seeking abortion care in Machakos and Trans-Nzoia Counties. Kenya East Afr Med J. 2016;93(8):327–32.
Lafaurie MM, Grossman D, Troncoso E, Billings DL, Chávez S. Women’s perspectives on medical abortion in Mexico, Colombia, Ecuador and Peru: a qualitative study. Reprod Health Matters. 2005;13(26):75–83.
Oyeniran AA, Bello FA, Oluborode B, Awowole I, Loto OM, Irinyenikan TA, et al. Narratives of women presenting with abortion complications in Southwestern Nigeria: a qualitative study. PLoS ONE. 2019;14(5):1–17.
Baum SE, Maria A. It’s not a seven - headed beast: abortion experience among women who received support from helplines for medication abortion in restrictive settings. Health Care Women Int. 2020;41:1–27.
Ouédraogo R, Sundby J. Social determinants and access to induced abortion in Burkina Faso: from two case studies. Obstet Gynecol Int. 2014;2014:1–6.
Baxerres C, Boko I, Konkobo A, Ouattara F, Guillaume A. Abortion in two francophone African countries: a study of whether women have begun to use misoprostol in Benin and Burkina Faso. Contraception. 2018;97(2):130–6.
Manríquez IP, Moreno Standen C, Álvarez Carimoney A, Richards A. Experience of clandestine use of medical abortion among university students in Chile: a qualitative study. Contraception. 2018;97(2):100–7.
Appiah-Agyekum NN. Medical abortions among university students in ghana: Implications for reproductive health education and management. Int J Womens Health. 2018;10:515–22.
Szwarc L, Fernández VSS. "Lo quería hacer rápido, lo quería hacer ya”: tiempos e intervalos durante el proceso de aborto. Sex Salud y Soc Latinoam. 2011;28(8):90–115.
Chareka S, Crankshaw TL, Zambezi P. Economic and social dimensions influencing safety of induced abortions amongst young women who sell sex in Zimbabwe. Sex Reprod Heal Matters [Internet]. 2021;29(1):121. https://doi.org/10.1080/26410397.2021.1881209.
Ferrari W, Peres S. Itinerários de solidão: aborto clandestino de adolescentes de uma favela da Zona Sul do Rio de Janeiro, Brasil. Cad Saude Publica. 2020;36(Suppl 1):e00198318.
Kebede MT, Middelthon AL, Hilden PK. Negotiating the social and medical dangers of abortion in Addis Ababa: an exploration of young, unmarried women’s abortion-seeking journeys. Health Care Women Int. 2018;39(2):186–207.
Freeman C. The crime of choice: abortion border crossings from Chile to Peru. Gender Place Cult. 2017;24(6):851–68.
Cleeve A, Faxelid E, Nalwadda G, Klingberg-Allvin M. Abortion as agentive action: reproductive agency among young women seeking post-abortion care in Uganda. Cult Heal Sex. 2017;19(11):1286–300.
Petracci M, Pecheny M, Mattiolo M, Capriati A. El aborto en las trayectorias de mujeres y varones de la ciudad de Buenos Aires. Sex Salud y Soc Rev Latinoam. 2012;61(12):164–97.
Esia-Donkoh K, Darteh EKM, Blemano H, Asare H. Who cares? Pre and post abortion experiences among young females in Cape Coast metropolis. Ghana Afr J Reprod Health. 2015;19(2):43–51.
Penfold S, Wendot S, Nafula I, Footman K. A qualitative study of safe abortion and post-abortion family planning service experiences of women attending private facilities in Kenya. Reprod Health. 2018;15(1):1–8.
Ramos S, Romero M, Aizenberg L. Women’s experiences with the use of medical abortion in a legally restricted context: the case of Argentina. Reprod Health Matters. 2015;22(44):4–15.
Bury L, Aliaga Bruch S, MacHicao Barbery X, Garcia PF. Hidden realities: What women do when they want to terminate an unwanted pregnancy in Bolivia. Int J Gynecol Obstet. 2012;118(SUPPL. 1):4–9.
Mitchell EMH, Kwizera A, Usta M, Gebreselassie H. Choosing early pregnancy termination methods in Urban Mozambique. Soc Sci Med. 2010;71(1):62–70.
Mohamed D, Diamond-Smith N, Njunguru J. Stigma and agency: exploring young Kenyan women’s experiences with abortion stigma and individual agency. Reprod Health Matters. 2018;26(52):1492285.
Frederico M, Michielsen K, Arnaldo C, Decat P. Factors influencing abortion decision-making processes among young women. Int J Environ Res Public Health. 2018;15(2):329.
Katz AJ, Ramirez AM, Bercu C, Filippa S, Dirisu O, Egwuatu I, et al. “I just have to hope that this abortion should go well”: perceptions, fears, and experiences of abortion clients in Nigeria. PLoS One [Internet]. 2022;17:1–16. https://doi.org/10.1371/journal.pone.0263072.
Makleff S, Wilkins R, Wachsmann H, Gupta D, Wachira M, Bunde W, et al. Exploring stigma and social norms in women’s abortion experiences and their expectations of care. Sex Reprod Heal Matters [Internet]. 2019;27(3):50. https://doi.org/10.1080/26410397.2019.1661753.
Larrea S, Hidalgo C, Jacques-Aviñó C, Borrell C, Palència L. “No one should be alone in living this process”: trajectories, experiences and user’s perceptions about quality of abortion care in a telehealth service in Chile. Sex Reprod Heal Matters. 2022;29(3):1948953.
Byrne ME, Omoluabi E, OlaOlorun FM, Moreau C, Bell SO. Determinants of women’s preferred and actual abortion provision locations in Nigeria. Reprod Health [Internet]. 2021;18(1):1–9. https://doi.org/10.1186/s12978-021-01290-w.
Solheim IH, Moland KM, Kahabuka C, Pembe AB, Blystad A. Beyond the law Misoprostol and medical abortion in Dar es Salaam, Tanzania. Soc Sci Med [Internet]. 2020;245:112676. https://doi.org/10.1016/j.socscimed.2019.112676.
Biney AAE, Atiglo DY. Examining the association between motivations for induced abortion and method safety among women in Ghana. Women Health. 2017;57(9):1044–60.
Berry-Bibee EN, St Jean CJ, Nickerson NM, Haddad LB, Alcime MM, Lathrop EH. Self-managed abortion in urban Haiti: a mixed-methods study. BMJ Sex Reprod Health. 2018;44(3):193–9.
Burkhardt G, Scott J, Onyango MA, Rouhani S, Haider S, Greiner A, et al. Sexual violence-related pregnancies in eastern Democratic Republic of Congo: a qualitative analysis of access to pregnancy termination services. Confl Health. 2016;10(1):1–9.
Hess RF. Women’s stories of abortion in southern Gabon. Africa J Transcult Nurs. 2007;18(1):41–8.
Omideyi AK, Akinyemi AI, Aina OI, Adeyemi AB, Fadeyibi OA, Bamiwuye SO, et al. Contraceptive practice, unwanted pregnancies and induced abortion in Southwest Nigeria. Glob Public Health. 2011;6:S52.
Da Domingos SRF, Merighi MAB, De Jesus MCP, De Oliveira DM. The experience of women with abortion during adolescence as demanded by their mothers. Rev Lat Am Enfermagem. 2013;21(4):899–905.
Osur J, Orago A, Mwanzo I, Bukusi E. Social networks and decision making for clandestine unsafe abortions: evidence from Kenya. Afr J Reprod Health. 2015;19(1):34–43.
Oyefara JL. Power dynamics, gender relations and decision-making regarding induced abortion among university students in Nigeria. Afr Popul Stud. 2017. https://doi.org/10.11564/31-1-991.
Szulik D, Zamberlin N. La legalidad oculta: Percepciones de estigma en los recorridos de mujeres que descubren y acceden a la interrupción legal del embarazo por causal salud. Sex Salud y Soc Rev Latinoam. 2020;34:46–67.
Coast E, Murray SF. These things are dangerous: understanding induced abortion trajectories in urban Zambia. Soc Sci Med. 2016;153:201–9.
Marlow HM, Wamugi S, Yegon E, Fetters T, Wanaswa L, Msipa-Ndebele S. Women’s perceptions about abortion in their communities: perspectives from western Kenya. Reprod Health Matters. 2014;22(43):149–58.
Assifi AR, Berger B, Tunçalp Ö, Khosla R, Ganatra B. Women’s awareness and knowledge of abortion laws: a systematic review. PLoS ONE. 2016;11(3):e0152224.
Rossier C. Abortion: an open secret? abortion and social network involvement in Burkina Faso. Reprod Health Matters. 2007;15(30):230–8.
Coeytaux F. Facilitating women’s access to misoprostol through community-based advocacy in Kenya and Tanzania. Int J Gynecol Obstet. 2014;125(1):53–5.
Yegon EK, Kabanya PM, Echoka E, Osur J. Understanding abortion-related stigma and incidence of unsafe abortion: experiences from community members in machakos and trans Nzoia counties Kenya. Pan Afr Med J. 2016. https://doi.org/10.11604/pamj.2016.24.258.7567.
Gerdts C, Jayaweera RT, Baum SE, Hudaya I. Second-trimester medication abortion outside the clinic setting: an analysis of electronic client records from a safe abortion hotline in Indonesia. BMJ Sex Reprod Heal. 2018;44(4):286–91.
Gerdts C, Hudaya I. Quality of care in a safe-abortion hotline in indonesia: beyond harm reduction. Am J Public Health. 2016;106(11):2071–5.
Aiken ARA, Digol I, Trussell J, Gomperts R. Self reported outcomes and adverse events after medical abortion through online telemedicine: population based study in the Republic of Ireland and Northern Ireland. BMJ. 2017. https://doi.org/10.1136/bmj.j2011.
Jelinska K, Yanow S. Putting abortion pills into women’s hands: realizing the full potential of medical abortion. Contraception. 2018;97:86–9.
Singh S, Remez L, Sedgh G, Kwok L, Onda T. Abortion worldwide 2017: uneven progress and unequal access. New York; 2018.
Acknowledgements
This review was funded by a general support grant from the Hewlett Foundation. We are also grateful for Ivy Garner, Library Specialist at Welch Medical Library at Johns Hopkins University, who supported the search process.
Funding
This work was funded by the William and Flora Hewlett Foundation, under Grant # 2018 – 7756.
Author information
Authors and Affiliations
Contributions
LH was involved in the entire systematic review process, from conceptualization to writing of this manuscript. LH led development of the manuscript. AB was involved in the entire systematic review process, from conceptualization to writing of this manuscript. MS was involved in the entire systematic review process, from conceptualization to writing of this manuscript. SB was involved in the entire systematic review process, from conceptualization to writing of this manuscript. SB provided senior technical input throughout the process. MSt was involved in the entire systematic review process, from conceptualization to writing of this manuscript. CT was the librarian on the project and developed the search terms and conducted the search. CI was involved in the entire systematic review process, from conceptualization to writing of this manuscript. CI provided senior technical input throughout the process. All authors reviewed and contributed to the final manuscript. All authors read and approved final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was submitted to the International Center for Research on Women (ICRW)’s Internal Review Board (IRB) for determination of ethical approval. It was determined to be non-human subjects and was not submitted for ethical approval. All data for the review comes from already existing, de-identified published studies.
Consent for publication
Not applicable.
Competing interests
None of the authors have any competing interests to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search terms.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hinson, L., Bhatti, A.M., Sebany, M. et al. How, when and where? A systematic review on abortion decision making in legally restricted settings in sub-Saharan Africa, Latin America, and the Caribbean. BMC Women's Health 22, 415 (2022). https://doi.org/10.1186/s12905-022-01962-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-022-01962-0