
Abstract
Background
Breast cancer is the greatest common cancer in women worldwide, with approximately 1.7 million new cases diagnosed each year in the world which accounts for 12% of all new cancer cases and 25% of all cancers in women. Even though the higher mortality rate of breast cancer in low and middle-income countries, the practice of early detection methods is low and the majority of the patients who appeared at an advanced stage of the disease need palliative care with little survival rates. However, evidence is scarce on the knowledge and practice of breast cancer early detection methods among women of reproductive age in Ethiopia. Therefore we aimed to assess the knowledge on risk factors and practice of early detection methods of breast cancer among female graduating students of Debre Tabor University.
Methods
Institution-based cross-sectional study was conducted. A stratified random sampling technique was used. Data were collected with a self-administer questionnaire. The collected data were processed and analyzed with the computer using SPSS version 25 software. Descriptive statistics were used to describe the socio-demographic information of participants. Binary and multivariable logistic regression with an adjusted odds ratio (AOR) and 95% confidence interval (CI) was used to identify factors associated with the outcome variable. Statistical significance was stated at p < 0.05.
Result
A total of 270 female students participated in the study. The median age (± SD) was 24.63 years (± 1.26). All of the students heard about breast cancer and early detection methods. About 206 (76.67%) of the participants had good knowledge of breast self-examination. Mass media, health professionals, and friends in combination were the main source of information 172 (63.77%), only 110 (40.70%) of students performed a breast-self-examination and the rest did not perform it due to forgetting fullness and lack of knowledge. About 208 (77.1%) of the respondents respond family history is a risk factor for breast cancer. Being a health science student (AOR = 2.32; 95% CI: 2.12, 3.52), family history of breast problems (AOR = 3.41; 95% CI: 3.22, 8.33), and having a good level of knowledge (AOR = 1.83; 95% CI: 1.01, 5.68) were the factors associated with the practice of breast self-examination.
Conclusion
Most of the participants were unaware of the benefits, appropriate timing, and techniques of doing a breast self-examination. Health science students had better awareness & practice of breast self-examination than non-health science students. Trained health professionals must give focus on giving health information regarding risk factors of breast cancer and methods of early detection of breast cancer to the public & their clients.
Similar content being viewed by others

Introduction
Background information
Breast cancer is the most common cause of malignancy in women accounting for about one-third of all cancers in women is epithelial malignancies of the breast [1,2,3]. The Guideline of the American cancer society (2007) stated sixteen main known risk factors for breast cancer, among which gender is the most important risk factor as only less than one per cent of patients with breast cancer are males [4,5,6]. Lifestyle-related risk factors for breast cancer include having no children, oral contraceptive use, tobacco smoking, obesity, and alcohol use, no history of breastfeeding, and hormone replacement therapy. Breast cancer also occurs more commonly in women with a family history of breast cancer than in the general population [2, 7, 8].
Most breast cancers will present as a hard lump, which may be related to in drawing of the nipple. Although any portion of the breast, including the axillaries tale, may be involved, breast cancer is found most frequently in the upper outer quadrant of the breasts [2, 9, 10].
Carcinoma of the breast is one of the manageable cancers if noticed early. The American Cancer Society recommends as an option breast awareness & Breast self-examination (BSE) for early detection of breast cancer [7, 11, 12]. Breast cancer can be early detected with the combination of BSE, clinical breast examination by a caregiver, and mammography [2, 13].
Early detection of breast cancer cases before advancement is a crucial factor in the prognosis and survival of breast cancer patients [1]. Breast self-examination clinical breast examination and mammography are commonly used methods of early detection in the current era [8, 11]. Among these BSE is the recommended one particularly in developing countries meanwhile it was a simple, cost-free procedure and quick[12, 14].
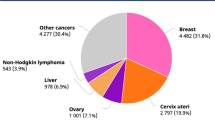
As evidence displays, the incidence of breast cancer cases in Ethiopia is growing disturbingly and growing into the most common and most commonly diagnosed tumour among women with a projected incidence rate of 43 cases per 100,000 women [1]. According to the Addis Ababa population-based cancer registry report, breast cancer accounts for 33% of all female cancer cases and 23% of all cancers in the country [11, 15, 16].
If not diagnosed and treated early, breast cancer is life treating. Advanced stage and large tumour size at diagnosis are associated with decreased survival [2]. In Ethiopia, the majority of breast cancer patients are diagnosed at an advanced stage and their survival is poor as a result most patients need palliative care [8, 13].
Carcinoma of the breast occurs commonly in the western world, accounting for 3–5% of all deaths in women [4]. In resource-poor countries, it accounts for 1–3% of deaths [17]. Breast cancer is the most common cause of death in middle-aged women in western countries. In 2004, approximately one and a half million new cases were diagnosed worldwide [18, 19].
In low- and middle-income countries, it remains a significant public health challenge incidence rates have been shown to surge yearly by as much as 5% with over 1million projected new cases annually by 2020 [5].
Women with a family history of breast cancer are riskier than the general population, and yet this has far-reaching impacts in terms of counselling and tumour prevention in these women [20, 21]. Among the epithelial tumours in adults, breast cancer is unique in that effective screening improves survival. BSE, CBE by a caregiver, and mammography have been advocated as useful screening tools. Several trials have recommended that annual or biannual screening with mammography or mammography plus CBE in normal risk women over the age of 50 decreases breast cancer mortality [1, 22, 23]. Breast self-examination makes women more "breast aware", which in turn may lead to an earlier diagnosis of breast cancer. The rationale behind extending BSE practice as a screening test is the fact that breast cancer is frequently detected by women themselves without any other symptoms [24].
As evidence shows knowledge about breast cancer, family history of breast cancer, the presence of breast abnormalities, a higher year of study and is a health science student were the most important factors associated with the practice of breast cancer early detection methods [25,26,27].
Methods and materials
Study area and period
Debre Tabor is the biggest town in the south Gondar zone in the Amhara Regional State which is placed in the central highlands of Ethiopia and situated at a distance of 667Kms away from Addis Ababa in the Northeast direction. The geographical location of Debre Tabor town is 011″0.51 N.38.1″ E and 11.850′ N.38.017 E with an elevation of 2.706 m (8.878ft) above sea level. Debre Tabor University was established as a third-generation university in Ethiopia in 2011. Currently, the university had 6 main faculty. The study was conducted from October 1- to December 15, 2020.
Study design
An institution-based cross-sectional study was conducted among DTU female graduating class students.
Source population
The source population was all Debre Tabor university Female students.
Study population
The study populations were all Debre Tabor university graduating female students.
Study unit
The study unit was each female Debre Tabor university graduating student.
Sampling technique and sample size determination
Sample size was computed based on single population proportion formula by using:
-
95% confident interval,
-
5% margin of error and.
-
proportion based on research done on screening of breast cancer screening is
$$\begin{aligned} {\text{n}} & = {\text{Z}}^{2} {\text{P}}\left( {1 - {\text{P}}} \right)/{\text{W}}^{2} \\ & = \frac{{\left( {{1}.{96}} \right)^{{2}} 0.{5}\left( {{1} - 0.{5}} \right)}}{{\left( {0.0{5}} \right)^{{2}} }} \\ & = 384 \\ \end{aligned}$$
Since our population was less than 10,000 we used correction formula (no = n/1 + n/N)
nf = 384/1 + 384/674 = 245 students
Then we added a 10% none response rate, the total sample size became 270.
P- Single population proportion for breast cancer screening to obtain the required sample size, from the total of 684 female graduating students stratified random sampling was applied to select study participants from the source population. First students were stratified by their department. Then, the sample size was proportionally allocated to all the departments in the institution based on the number of female students in each department, after which respondents were selected by simple random sampling technique. We took 40% representative from each department since the sample size is 270 which represent 40% of the total number of female graduating students.
Data collection method and procedure
The data was collected by using a structured and self-administered questionnaire that was designed by reviewing previous similar studies [1, 11, 28, 29]. The questionnaire was pre-tested and evaluated by experts in the area to assess the face and content validity. The questionnaire was organized in English and it consists of all the variables that can come across the objectives of the study which are connected to socio-demographic characteristics, knowledge, and practice towards early detection methods of breast cancer and risk factors.
Measurements
The study assessed the knowledge of risk factors and practice of participants towards risk factors and early detection methods of breast cancer. Students' knowledge regarding risk factors and BSE scores was calculated out of the total knowledge-specific questions. Each accurate response gets one point and zeroes for the incorrect one based on the respondent's response. Finally, the respondent who scores greater than or equal to the mean score were considered as having 'good knowledge and respondents who score less than the mean score was considered as having 'poor knowledge. There were 10 knowledge assessment questions and 8 practice assessment questions with a reliability coefficient of 76% and 78% respectively which was calculated using Cronbach’s alpha [1]. Before undertaking the data collection, the questionnaire was submitted to experts mainly oncologists, and other health professionals who are working in the area to test the face and content validity to assess whether they met the study objectives.
Eligibility
Inclusion criteria
All-female graduating regular students of Debre Tabor University.
Exclusion criteria
Post basic and extension female graduating students were excluded from this study.
Variables
Dependent variable Practice of breast cancer early detection methods.
Socio-demographic factors age marital status, department, year of study.
Personal and behavioral factors alcohol, smoking, use of traditional treatment, lack of information about breast cancer, fear of exposing breasts fear of being diagnosed with cancer, and lack of trust in medical care.
Clinical factors previous history of benign breast disease, family history of breast cancer, previous history of any type of cancer, previous history of co-morbidities (hypertension DM, HIV), presenting symptoms.
Operational definitions
Knowledge of breast self-examination: was measured by considering those who answered 70% and above of BSE questions as knowledgeable, and those who got < 70%non-knowledgeable [1].
The practice of BSE is defined as carrying out BSE at regular and the same time each month using a proper technique which is evidenced by the result of the questionnaire.
Regular BSE when BSE is done each month at the same time after some days of the menstrual cycle.
Occasional BSE when BSE is 1 to 3 times a year or every 3 months (irregularly at any time).
Clinical breast self-examination (CBE) when an experienced health worker examines breasts Statistical Analysis.
Mass media: Mass media refers to a diverse array of media technologies that reach a large audience via mass communication, e.g. Radio, Television, Facebook, telegram etc.
Data quality management
To uphold data quality, ten data collectors and one supervisor who were health professionals (clinical nurses) were selected based on their experience in data collection and they were trained for 3 days. The questionnaire was developed by the research team based on questions used in the previous peer-reviewed published articles. The questionnaire was first prepared in English language and then translated to the local language (Amharic) to facilitate communication. The collected data was revised and checked for mistakes, legibility of handwriting, completeness, and consistency by the principal investigator and supervisor daily during data collection. Any mistake or ambiguity was cleared on the spot.
Data processing and analysis
After data collection was finalized, the data were categorized, and then SPSS Version 25 program was used to enter and analyze knowledge and practice on early detection methods of breast cancer and other data. Suitable descriptive analysis (Median, SD) was used to describe the study population characteristics in terms of the variables and the results were presented by using tables and figures. The degrees of association between dependent and independent variables were assessed using OR and 95% CI. A P-value less than or equal to 0.05 was considered statistically significant. Bivariate and multivariate logistic regression analyses were conducted to identify the association of knowledge and practice of SBE with independent variables.
Results
Socio-demographic characteristics of study participant
A total of 270 regular female graduating students of DTU in the academic year of 2020/21 took part making the response rate 100%. The age of the participants ranged from 21 to 28 & the median age was 24.6 years (SD ± 1.26). Most of the participants were Amhara by ethnicity 109 (40.4%) and single regarding marital status 246 (91.1.1%). About 107 (39.63%) students were agricultural and other science students, 74 (27.4%) students were from technology, (4617.04%) were social science and humanity students, 25 (9.26%) were from health science students,18 (6.67%) were natural and computational science students (Table 1).
Knowledge and practice on early detection methods of breast cancer.
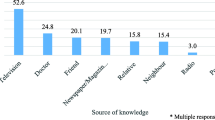
All 270 participants (100%) heard about at least one of the three methods of early detection of breast cancer. Among this Only 55 (20.3%) students were aware of all the three methods (BSE, CBE & mammography), and 207 (76.7%) of respondents heard about breast self-examination as an early detection method of breast ca. more than half of 172 (63.8%) the students had gotten the information about early detection methods of breast cancer from mass media, health professionals, friends in combination and mass media was used as the only source of information in 65 (24%) of the students. 207 (76.7%) participants have good knowledge about BSE, but only 14 (6.8%) were aware of all the benefits of BSE. One hundred forty-five (53.6%) of them stated that early detection and treatment of breast Ca is the only benefit of BSE. Regarding knowledge of early detection methods among departments, 24 (96%) health science class students had good knowledge, and 183 (74.7%) of non-health science students had good knowledge about early detection methods of breast cancer.
Awareness of breast self-examination of female graduating students:
Regarding awareness about breast self-examination from the total, the majority of the respondents 207 (76.67%) had good knowledge, and the rest of the respondents 63 (33.33%) had poor knowledge about Breast self-examination.
Female students practice at the appropriate time for doing BSE
About 110 (40.74%) of the students performed breast self-examination within the past 12 months. The main reason for not performing BSE was forgetful fullness in 159 (58.8%) & lack of knowledge in 106 (39.4%) of the participants and the rest were due to fear of detecting abnormality and other issues. Of those who did BSE only 106 (39.3%) of the respondents did it regularly every month, 99 (36.7%) of them do BSE with the frequency of fewer than 3 times per year and about 63 (23.3%) of them did BSE only when they felt unhealthy. One hundred eighty-six (68.9%) of the students did SBE after menstruation and all of the respondents who performed SBE started doing it after 20 years of age. Breast self-examination techniques were known by 207 (76.7%) of the students and the wedge technique was used in 141 (52%) of the case, and the circular technique in 86 (32%).
Regarding Knowledge of things to be checked while doing BSE 76.7% of them knew at least two early signs of breast cancer. Among these 14 (6.8%) of them knew all the signs listed and the rest 193 (93.2%) of the students listed lumps in the breast, change in colour of the breast, nipple direction, and discharge as early signs of breast cancer (Table 2).
Awareness of risk factors for breast cancer
Regarding the awareness of the risk factors for breast cancer, the most commonly known risk factor was a family history of breast cancer 208 (77.1%). Hormonal replacement therapy (HRT) use, lack of physical activity, high fat diet, ageing & late menopause were not identified as risk factors by most of the participants (Table 3).
Factors associated with the practice of students on early detection methods of breast cancer
On bivariable logistic regression; age, knowing how to perform BSE, knowing when to perform BSE, and knowing how often to do BSE were positively associated with the practice Of BSE. Whereas, being a health science student and Family history of a breast problem and having a good level of knowledge remained significantly associated with the practice of BSE on the multivariable logistic regression. Participants who have good knowledge about breast cancer early detection methods were 1.83 times more likely to practice breast self-examination than those who have poor knowledge (AOR: 1.83; 95% CI: 1.01–5.68). The odds of practising BSE was 3.41 times higher among graduating female students who had a family history of breast problems than hadn't family history (AOR: 3.41 (96%CI; 3.8–33.16). Graduating students from health Science were 2.32times more likely to practice breast self-examination compared to no health graduating students (2.32, 95% CI: 2.12–3.52) (Table 4).
Discussion
Breast cancer is one of the most common causes of death & morbidity in middle-aged women but also is one of the manageable cancers if once detected early [17]. In this cross-sectional study 270, regular female students of Debre Tabor University with a median age of 21 years participated.
About 76.67% of the participants had good knowledge about breast self-examination which was lower than the figure from a study done in Saud Arabia which was 93.7% of the respondents were aware of BSE [21], But higher than the study figure from Debre Birhan university where (64%).such difference might be due to there was no health science students included on the research at Debre Birhan university or might be sample size difference[1, 10].
Mass media, health professionals, and friends were a detected source of the information in about 63.77% of the case and mass media was the only source of information in about 24.14% of them. There was some difference at Bahir Dar University where more than half (54%) of the students got the information from lectures (school) and mass media used in about only 22.1% of them [18]. The difference may be due to poor attitudes towards mass Media in some parts of the population. A similar study conducted at Debre Birhan University and the numbers on the source of information stated that about 40% of them got the information from mass media which was close to our study [5, 10, 29].
About 53.6% of the study participants knew the benefits of BSE though only 6.8% [14] were aware of all the benefits of BSE which is almost similar to the study at Ibadan was 53.2%[29].
Regarding breast self-examination practice, 40.7% of the respondents performed BSE within the past 12 months and 39.6% of them did BSE monthly, which is higher than at Debre Birhan University (28.3%) but lower than the study at Bahir Dar University which was 54.1% [10, 28]. A similar cross-sectional study was done in Nigeria [30], Austria [31] and Egypt [32, 33] on the practice of BSE, and the figure were 43.2%, 99%, and 10.4% respectively. Such difference might be explained by socio-demographic factors since local researchers had comparable figures. It might also be due to a lack of facilities for privacy and cultural misconception as doing repeated BSE increases the risk of acquiring cancer.
Regarding techniques of BSE from those who practised BSE 52% of the students practised wedge techniques and 32% of them used circular techniques. A similar study was done at Bahir Bar University and the figures were 22.1%, 12.6%, 9% for circular, wedge, and vertical strips respectively, and 41.1% used all of the three methods [1, 10].
Regarding Knowledge of things to be checked while doing BSE 76.7% of them knew at least two early signs of breast cancer. Among these 6.8%, [8] of them knew all the signs listed and the rest 93.2% (193) of the students' listed lumps in the breast, change in colour of the breast, nipple direction, and discharge as early signs of breast cancer. This figure is almost similar to the study at Bahir Dar University, lump in the breast was known by 90% of them, discharge from the breast by 85.8%, and discolouration or dimpling of the breast by 90% of them [1].
Regarding awareness of risk factors of breast cancer, the most commonly known risk factor was a family history of breast cancer (77.1%). HRT use, lack of physical activity, high fat diet, ageing & late menopause were not identified as risk factors by most of the participants. In contrast to the study at the Ibadan University of Nigeria where the personal history of breast Ca is the most known one [29]. A similar study was also done at Addis Ababa on nurses and family history of breast cancer 69.6%, smoking 54.4% were the most known risk factors which were comparable to our study [34]. There was also a similar study in Cameroon on risk factors awareness, radiation exposure (58.9%), hormone replacement therapy (58.2%), smoking (58.2%), alcohol consumption (46.7%), and high-fat diet (45.4%) were the most frequently indexed risk factors for breast cancer. Whereas late menopause (9.2%), early age at first menstruation (8.2%) and not having a child (7.9%) were the least recognized risk factors.
After controlling the effect of confounding factors good level of knowledge, having a history of a breast problem and being a health science student were the factors associated with the practice of breast cancer early detection. This finding is similar to other studies conducted in different countries [27, 35].
Conclusion
Most of the students were unaware of the benefits, appropriate timing & techniques of doing breast self-examinations. Age of students, being a health science student, family history of a breast problem, and having a good level of knowledge were the factors associated with the practice of breast self-examination. Attention given to methods of early detection and risk factors for breast cancer by mass Media & health professionals was low.
Therefore based on the findings of our study, the following recommendations are forwarded;
Mass Media should give more focus on giving Health information regarding risk factors of breast cancer and practice of early detection methods for students.
Trained health professionals should give health education to their school friends, and families on breast cancer and breast self-examination.
Health education must be delivered to female students in high schools and higher institutions through gender clubs & organizations.
Further large-scale studies must be done in this area.
Limitation of the study
Due to the cross-sectional nature of the study, we could not ascertain the cause-and-effect relationship between the factors and the outcome.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- WHO:
-
World Health Organization
- DM:
-
Diabetes Mellitus
- HTN:
-
Hypertension
- CI:
-
Confidence interval
- COR:
-
Crude odds ratio
- AOR:
-
Adjusted odds ratio
- DTU:
-
Debre Tabor University
References
Tewabe T, Mekuria Z. Knowledge and practice of breast self-examination among undergraduate students in Bahir Dar University, North-West Ethiopia, 2016: a cross-sectional study. J Public Health Africa. 2019;10(1).
Shallo SA, Boru JD. Breast self-examination practises and associated factors among female healthcare workers in West Shoa Zone, Western Ethiopia 2019: a cross-sectional study. BMC Res Notes. 2019;12(1):1–6.
Koc G, Gulen-Savas H, Ergol S, Yildirim-Cetinkaya M, Aydin N. Female university students’ knowledge and practice of breast self-examination in Turkey. Niger J Clin Pract. 2019;22(3):410–5.
Andegiorgish AK, Kidane EA, Gebrezgi MT. Knowledge, attitude, and practice of breast cancer among nurses in hospitals in Asmara, Eritrea. BMC Nurs. 2018;17(1):1–7.
Mengie T, Yifru A, Fikre A, Niguse W, Demsie D, Ekubay M. Assessment of knowledge, attitude and practice regarding breast self-examination among female students in Debre Birhan University, North Shewa Ethiopia. Am J Clin Exp Med. 2020;8(3):42–8.
Shrivastava S, Shrivastava PS, Ramasamy J. Self breast examination: a tool for early diagnosis of breast cancer. Am J Public Health Res. 2013;1(6):135–9.
Birhane K, Alemayehu M, Anawte B, Gebremariyam G, Daniel R, Addis S, et al. Practices of breast self-examination and associated factors among female debre berhan university students. Int J Breast Cancer. 2017;2017:1–6.
Poorolajal J, Nafissi N, Akbari ME, Mahjub H, Esmailnasab N. Breast cancer survival analysis based on immunohistochemistry subtypes (ER/PR/HER2): a retrospective cohort study. Arch Iran Med. 2016;19(10).
Mohite R, Mohite V, Kakade S. Knowledge of breast feeding among primigravida mothers. Bangladesh J Med Sci. 2012;11(4):312–6.
Azage M, Abeje G, Mekonnen A. Assessment of factors associated with breast self-examination among health extension workers in West Gojjam Zone, Northwest Ethiopia. Int J Breast Cancer. 2013;2013:1–6.
Kantelhardt E, Zerche P, Mathewos A, Trocchi P, Addissie A, Aynalem A, et al. Breast cancer survival in Ethiopia: a cohort study of 1,070 women. Int J Cancer. 2014;135(3):702–9.
Sama C-B, Dzekem B, Kehbila J, Ekabe CJ, Vofo B, Abua NL, et al. Awareness of breast cancer and breast self-examination among female undergraduate students in a higher teachers training college in Cameroon. Pan African Med J. 2017;28(1):164.
Mekonnen BD. Breast self-examination practice and associated factors among female healthcare workers in Ethiopia: A systematic review and meta-analysis. PLoS ONE. 2020;15(11): e0241961.
Alwan NA, Al-Diwan JK, Wafa’M A-A, Eliessa RA. Knowledge, attitude & practice towards breast cancer & breast self examination in Kirkuk University. Iraq Asian Pac J Reprod. 2012;1(4):308–11.
Abeje S, Seme A, Tibelt A. Factors associated with breast cancer screening awareness and practices of women in Addis Ababa, Ethiopia. BMC Womens Health. 2019;19(1):1–8.
Gebremedhin A, Shamebo M. Clinical profile of Ethiopian patients with breast cancer. East Afr Med J. 1998;75(11):640–3.
Dutta T, Meyerson B, Agley J. African cervical cancer prevention and control plans: a scoping review. J Cancer Policy. 2018;16:73–81.
Solomon LJ, Mickey RM, Rairikar C, Worden JK, Flynn BS. Three-year prospective adherence to three breast cancer screening modalities. Prev Med. 1998;27(6):781–6.
Gupta R, Gupta S, Mehrotra R, Sodhani P. Risk factors of breast cancer and breast self-examination in early detection: systematic review of awareness among Indian women in community and health care professionals. J Public Health. 2020;42(1):118–31.
Ameer K, Abdulie SM, Pal SK, Arebo K, Kassa GG. Breast cancer awareness and practice of breast self-examination among female medical students in Haramaya University, Harar, Ethiopia. Ethiopia IJIMS. 2014;2(2):109–19.
Ahmed A, Zahid I, Ladiwala ZFR, Sheikh R, Memon AS. Breast self-examination awareness and practices in young women in developing countries: a survey of female students in Karachi, Pakistan. J Educ Health Promot. 2018;7:90.
Doshi D, Reddy BS, Kulkarni S, Karunakar P. Breast self-examination: Knowledge, attitude, and practice among female dental students in Hyderabad city, India. Indian J Palliat Care. 2012;18(1):68.
Özdemir A, Akansel N, Tunc GÇ, Aydin N, Erdem S. Determination of breast self-examination knowledge and breast self-examination practices among women and effects of education on their knowledge. Int J Caring Sci. 2014;7(3):792–8.
Alwan N, Al Attar W, Eliessa R, Madfaic Z, Tawfeeq F. Knowledge, attitude and practice regarding breast cancer and breast self-examination among a sample of the educated population in Iraq. Eastern Mediterr Health J. 2012;18(4):337–45.
Akram M, Iqbal M, Daniyal M, Khan AU. Awareness and current knowledge of breast cancer. Biol Res. 2017;50(1):1–23.
Duffy SW, Morrish OW, Allgood PC, Black R, Gillan MG, Willsher P, et al. Mammographic density and breast cancer risk in breast screening assessment cases and women with a family history of breast cancer. Eur J Cancer. 2018;88:48–56.
Avci IA. Factors associated with breast self-examination practices and beliefs in female workers at a Muslim community. Eur J Oncol Nurs. 2008;12(2):127–33.
Bouya S, Balouchi A, Ahmadidarehsima S, Badakhsh M. Knowledge and source of information about early detection techniques of breast cancer among women in Iran: a systematic review. J Cancer Prev. 2018;23(1):51.
Oluwatosin OA, Oladepo O. Knowledge of breast cancer and its early detection measures among rural women in Akinyele Local Government Area, Ibadan, Nigeria. BMC Cancer. 2006;6(1):1–6.
Ibrahim NA, Odusanya OO. Knowledge of risk factors, beliefs and practices of female healthcare professionals towards breast cancer in a tertiary institution in Lagos, Nigeria. BMC Cancer. 2009;9(1):1–8.
Nafissi N, Saghafinia M, Motamedi MHK, Akbari ME. A survey of breast cancer knowledge and attitude in Iranian women. J Cancer Res Ther. 2012;8(1):46–9.
Omar S, Khaled H, Gaafar R, Zekry A, Eissa S, El Khatib O. Breast cancer in Egypt: a review of disease presentation and detection strategies. Eastern Mediterr Health J. 2003;9(3):448–63.
Eltwansy MS. Early detection of breast cancer: knowledge, perception and barriers among females: a cross sectional study at Zagazig District. Egypt J Commun Med 2018;36(4).
Zeru Y, Sena L, Shaweno T. Knowledge, attitude, practice, and associated factors of breast cancer self-examination among urban health extension workers in Addis Ababa, Central Ethiopia. J Midwif Reprod Health. 2019;7(2):1662–72.
Akuoko CP, Armah E, Sarpong T, Quansah DY, Amankwaa I, Boateng D. Barriers to early presentation and diagnosis of breast cancer among African women living in sub-Saharan Africa. PLoS ONE. 2017;12(2): e0171024.
Acknowledgements
The authors would like to express their deepest and heartfelt thanks to all study participants.
Funding
No specific funding has been received from any individual or institution for this research.
Author information
Authors and Affiliations
Contributions
GM, AM, AT, made substantial contributions to the conception and design of the study, the formulation of the methodology, analysis, interpreted the data, and reviewed the final version submitted for publication. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This research has been registered in the Medical Ethical Review Committee of Debre Tabor University College of Medical and Health Sciences with the number: IRB.scho/med/879/2021, and written informed consent was obtained from all participants. All methods were performed under the relevant guidelines and regulations.
Consent for publication
Not applicable as there are no image or other confidentiality-related issues.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mehiret, G., Molla, A. & Tesfaw, A. Knowledge on risk factors and practice of early detection methods of breast cancer among graduating students of Debre Tabor University, Northcentral Ethiopia. BMC Women's Health 22, 183 (2022). https://doi.org/10.1186/s12905-022-01768-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-022-01768-0