
Abstract
Background
Nodular Fasciitis is a benign fibroblastic proliferation in soft tissues, which mostly occurs in the upper extremities, trunk, head and neck region. It is rarely reported to occur in the breast.
Case presentation
Herein, we present sonograms of nodular fasciitis in the breast at different durations in three cases. In Case 1, we provided the longest follow-up time in all literatures. In Case 2 and Case 3, we provided the automated breast ultrasound finding of breast nodular fasciitis for the first time.
Conclusion
Nodular Fasciitis shows clinical features and ultrasonography findings are similar to those of breast cancer. For superficially located breast lesions with a single and rapid growth, nodular fasciitis may be considered in the differential diagnosis of benign entities resembling malignant tumors on breast imaging.
Similar content being viewed by others


Background
Nodular fasciitis (NF) is a benign reactive proliferative lesion of fibroblasts that can occur throughout the body [1]. The most common site of NF is the upper limbs, followed by the head, neck and trunk [2]. The most typical features are the sudden appearance and rapid growth of palpable lesions [3]. However, it has rarely been reported to occur in the breast. NF can mimic breast cancer clinically, radiologically, and histopathologically. We present three cases of NF in the breast.
Case presentation
Case no. 1
A 43-year-old woman presented to the hospital because of a swelling mass in her right breast of 8 months’ duration. Through physical examination, a firm mobile 2 × 3 cm mass was detected at the 1-o’clock position of the right breast. There was no tenderness on palpation, and the patient showed no covering skin changes or nipple discharge. Axillary and supraclavicular lymph nodes were not touched. The patient denied any recent trauma and had no family history of breast cancer. The handheld breast ultrasonography (US) examination (Fig. 1) revealed that a lesion was located at the 1 o’clock position of the right breast. It was a 10 × 10 × 8 mm, irregular, indistinct and heterogeneous hypoechoic mass, which had no posterior shadowing. The lesion showed no vascularity on Dopple US examination. Subsequently,an excisional biopsy was performed. Histopathologic features were diagnosed as NF. At the most recent follow-up, twelve years postoperatively, no recurrence was observed in the case.

a, b transverse, sagittal and coronal US showed the lesion at 1 o 'clock in the right breast. It was a 10 × 10 × 8 mm irregular, indistinct and heterogeneous hypoechoic mass, which had no posterior shadowing. c Color Doppler shows no vascularity in the mass (white arrows)
Case no. 2
A 37-year-old Asian woman presented with a palpable, painless mass in the right lower inner breast for 15 days. There was no history of trauma. She had no family history of breast cancer. The handheld and automated breast ultrasound (ABUS) examination (Fig. 2) revealed that a lesion was located 30 mm from the nipple at the 3 o’clock position in the right breast and was surrounded by subcutaneous adipose tissue, with attachments to the anterior mammary fascia. It was a 22 × 13 × 21-mm, irregular, indistinct, without associated calcification, heterogeneous hypoechoic mass which was surrounded by a faint halo of high echo and posterior enhancement. The lesion and the surroundings showed some vascular distribution on Dopple US examination (Fig. 2). The elastography revealed a Tsukuba stiffness score of 3 of the lesion (Fig. 2). The core biopsy of the lesion was then performed with a 16 gauge needle. Although tumor spindle cell proliferation was suspected, no definite diagnosis was made. Finally, the percutaneous removal of the mass was performed. The pathologic findings led to a diagnosis of NF.

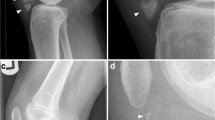
a The hand-held ultrasound revealed an irregular and uneven 22 × 13 × 21 mm hypoechoic mass at 3 o 'clock in the right breast with an echo halo extending from the anterior edge of the breast area to the peribreast adipose layer (white arrow). b Color Doppler imaging showed some vascular distribution in the mass(white arrows). c Ultrasound elastography showed a Tsukuba stiffness score of 3 of the lesion (white arrows). d By ABUS, the lesion showed an irregular shape, an indistinct margin, heterogeneous hypoechoic with an echogenic halo (white arrows)
Case no. 3
A 29-year-old woman presented the clinic with a swelling palpable mass in her right breast, which was noticed 6 months before presentation by her. Through examination, the mass was firm, mobile and smooth margin without tenderness to palpation. No palpable axillary and supraclavicular lymph nodes were noted. There was no reported history of breast trauma and breast cancer. The handheld and ABUS examination revealed that a lesion was located 30 mm from the nipple at the 9 o’clock position in the right breast. It was an irregular and markedly hypoechoic nodule measured 9 × 8 × 8 mm, which edges are angular and echogenic halo (Fig. 3). The lesion was almost surrounded by subcutaneous adipose tissue with attachments to the anterior mammary fascia. In addition, the surrounding adipose tissue showed an increased vascular distribution on Doppler US examination (Fig. 3). The elastography revealed a Tsukuba stiffness score of 1 of the lesion. By ABUS (Fig. 3), the lesion showed a retraction pattern on the coronal plane (Fig. 3). Subsequently, US-guided core needle biopsy was performed on the lesion using a 16-gauge needle. Based on the pathological findings, a phyllodes tumor was suspected. The wide excision was then performed, demonstrating a 10-mm area of NF.

a The handheld US revealed an irregularly shaped and markedly hypoechoic nodule with angular edges and an echogenic halo surrounded by subcutaneous adipose tissue and attached to the superficial fascia of the breast (white arrows). b The surrounding adipose tissue showed an increased vascular distribution on Doppler US examination (white arrows). c Ultrasound elastography showed a Tsukuba stiffness score of 1 of the lesion (white arrows). d By ABUS, the lesion showed a retraction pattern on the coronal plane (white arrows)
Discussion and conclusions
NF, described for the first time in 1955 by Konwaler et al. [4], is a benign disorder characterized by a pseudo neoplastic proliferation of myofibroblasts. The etiology of NF is uncertain. The clinical progression of NF seems to be a single and rapidly growing lesion [1]. NF can occur anywhere in the body [5]. NF can be divided into subcutaneous, intramuscular and fascial subtypes according to anatomical location. NF can also be classified into three histological subtypes: myxoid, cellular, and fibrous. The same mass may also have different histologic combinations. The different histologic types are roughly correlated with the duration of the nodule [3]. Old lesions are fibrous (such as our first and third cases) while recent cases show myxoid lesions (such as our second case).
Reports of NF in the breast exist but are rare. NF of the breast was listed as one of benign mesenchymal breast tumors by the World Health Organization in 2012 [6]. Although 10–15% of patients have a history of trauma prior to such lesions [3], there was no history of trauma in our three cases. In a previously study, the mean age of the patients with NF of the breast was 39 years (ranging 17–84 years) [7]. Our three cases were conforming to the study. Paliogiannis et al. described that the mean size of the lesion was approximately 20 mm (ranging 6–60 mm) [1], which was also in agreement with our cases. The upper outer quadrants of the breasts were most frequently affected [1], which were not consistent with our first two cases. Our second case was managed within 2 weeks from the first symptoms and signs. This pattern was similar to the previously cases [8]. Such a rapid growth is not common in other breast nodules, especially malignant nodules, and this may indicate even a feature of NF [1].
In Case 2 and Case 3, we provided the ABUS finding of breast nodular fasciitis for the first time. The US of NF may lead to a false impression of malignancy. The US findings may be depend on the histologic characteristics of NF [9]. The lesions that infiltrate into the surrounding fatty tissues make them irregular and unclear boundaries or partial unclear when examined on US. Lee et al. [10] reported that hyperechoicity around the lesion may be associated with marginal interlobular septal fibrosis and infiltrating inflammatory changes. The inhomogeneous hypo-echogenicity may be somewhat related to the uneven distribution of focal keloid-like collagen bundles [10]. The capillary hyperplasia of the lesions make them some vascularity on Dopple US examination.
Since most cases are diagnosed after surgical resection, the natural course of NF is unknown. However, spontaneous regression was observed [11]. Relapse of NF after surgical removal is rare [12]. In Case 1, we provided the longest follow-up time in all literatures. Due to its benign clinical course and limited capacity for recurrence, NF of the breast does not require radical surgical resection. Most patients can be successfully treated with local resection alone, while some may spontaneously resolve without any treatment [13, 14].
In summary, the present three cases demonstrate clinical and US features of NF in the breast. For single, rapidly growing superficial breast lesions, NF can be considered in the differential diagnosis of benign entities resembling malignant tumors on breast imaging.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Abbreviations
- NF:
-
Nodular fasciitis
- US:
-
Ultrasonography
- ABUS:
-
Automated breast ultrasound
References
Paliogiannis P, Cossu A, Palmieri G, Scognamillo F, Pala C, Nonnis R, Sotgiu G, Fois A, Palomba G, Attene F. Breast nodular fasciitis: a comprehensive review. Breast Care. 2016;11(4):270–4.
Lu L, Lao IW, Liu X, Yu L, Wang J. Nodular fasciitis: a retrospective study of 272 cases from China with clinicopathologic and radiologic correlation. Ann Diagn Pathol. 2015;19(3):180–5.
Choi HY, Kim SM, Jang M, Yun BL, Ahn HS, Park SY, Kim SW, Kang EY. Nodular fasciitis of the breast: a case and literature review. Ultraschall Med. 2015;36(3):290–1.
Konwaler BEKL, Kaplan L. Subcutaneous pseudosarcomatous fibromatosis (fasciitis). Am J Clin Pathol. 1955;25(3):241–52.
Squillaci ST, Patarino F, Bisceglia R. Nodular fasciitis of the male breast: a case report. Int J Surg Pathol. 2007;15(1):69–72.
Erinanc H, Turk E. The rare benign lesion that mimics a malignant tumor in breast parenchyma: nodular fasciitis of the breast. Case Rep Pathol. 2018;2018:1612587.
Hayashi S, Yasuda S, Takahashi N, Okazaki S, Ishibashi K, Kitada M, Miyokawa N. Nodular fasciitis of the breast clinically resembling breast cancer in an elderly woman: a case report. J Med Case Rep. 2017;11(1):1–3.
Bernstein KELR. Nodular (pseudosarcomatous) fasciitis, a nonrecurrent lesion: clinicopathologic study of 134 cases. Cancer. 1982;49(8):1668–78.
Son YM, Nahm JH, Moon HJ, Kim MJ, Kim EK. Imaging findings for malignancy-mimicking nodular fasciitis of the breast and a review of previous imaging studies. Acta Radiol Short Rep. 2013;2(8):2047981613512830.
Lee KJ, Jin W, Kim GY, Rhee SJ, Park SY, Park JS, Ryu KN. Sonographic features of superficial-type nodular fasciitis in the musculoskeletal system. J Ultrasound Med. 2015;34(8):1465–71.
Stanley MW, Skoog L, Tani EM, Horwitz CA. Nodular fasciitis: spontaneous resolution following diagnosis by fine-needle aspiration. Diagn Cytopathol. 1993;9(3):322–4.
Brown V, Carty NJ. A case of nodular fasciitis of the breast and review of the literature. Breast. 2005;14(5):384–7.
Cloutier JM, Kunder CA, Charville GW, Hosfield EM, Garcia JJ, Brown RA, Troxell ML, Allison KH, Bean GR. Nodular fasciitis of the breast: clinicopathologic and molecular characterization with identification of novel USP6 fusion partners. Mod Pathol. 2021;34(10):1865–75.
Zhao M, Yin X, Wen Y, Ru G, Meng X. Nodular fasciitis of the breast: Report of two cases illustrating the diagnostic implications for USP6 gene rearrangement and brief review of the literature. Exp Mol Pathol. 2021;123:104690.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
W.L.L. collected and wrote the manuscript; L.Y.B. reviewed and revised the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
The patients signed informed consent for the publication of this case report and any associated images. A copy of the consent form is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lin, W., Bao, L. Nodular fasciitis of the breast: the report of three cases. BMC Women's Health 22, 54 (2022). https://doi.org/10.1186/s12905-022-01631-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-022-01631-2