
Abstract
Background
The increased metabolic activity required to sustain breastfeeding and its associated milk production helps to reduce maternal fat stores accumulated during pregnancy. This study aims to assess the association between breastfeeding duration and fatness indices in middle-aged women.
Methods
The analysis was carried out in a group of 7500 parous 55.5 ± 5.3 year old women included body mass index, body fat percentage, and waist-to-height ratio. The likelihood of excessive weight or obesity in relation to total breastfeeding time using multivariate logistic regression analyses.
Results
An analysis of adjusted odds ratios did not show significant associations between breastfeeding duration and the risk of excessive weight and obesity in premenopausal women. After menopause, women who gave birth to 2 children and breastfed 1–6 and > 12 months had a lower risk of abdominal obesity (OR 0.70; 95% CI 0.50–0.99; p = 0.042; and OR 0.68; 95% CI 0.47–0.98; p = 0.039). Women who gave birth to 3 or more children and breastfed for 1–6 months, also showed a lower risk of overweight (OR 0.52; 95% CI 0.27–0.99; p = 0.047), compared to those ones that have never breastfed. There was no relationship found between the duration of lactation and the risk of excessive body fat.
Conclusion
Breastfeeding may have some beneficial, long-term effect on the risk of excessive weight and abdominal obesity in women.
Similar content being viewed by others


Background
Excessive body fat is a significant risk factor for many diseases including type 2 diabetes, cardiovascular disease, and cancer [1,2,3,4,5,6]. Epidemiological data indicate that obesity is more common in women than in men [7, 8]. Female-specific factors related to the risk of obesity include the duration of lactation, parity, and menopausal status. Pregnant women have increased energy demands associated with the development and growth of the fetus, placenta, enlargement of the uterus, mammary glands, and an increased in blood volume. During pregnancy, the female body also prepares for breastfeeding by storing nutrients and energy needed for milk production. During this period, excessive energy intake in relation to needs, may increase the body's fatty tissue, making it difficult to return to the pre-pregnancy weight, and maintain normal body mass over a longer period of time [9, 10].
The increased metabolic activity required to sustain breastfeeding and its associated milk production helps to reduce maternal fat stores accumulated during pregnancy [11]. It has been estimated that breastfeeding mothers need about 2.8 megajoules (MJ) (670 kcal) of additional energy per day to produce milk, of which about 2.1 MJ (500 kcal) should be acquired from food; the rest should come from fat stores accumulated during pregnancy [12]. Breastfeeding can therefore have a beneficial effect on the body fat index in women. From 8 retrospective studies a positive association between breastfeeding and weight changes was noted in only 2 papers, whereas 14 of 35 prospective studies in which women were evaluated for weight ≤ 2 years after delivery, found a beneficial effect of breastfeeding on body weight changes. The remaining 21 studies did not show such relationships [13]. Of the 5 studies that were considered to be of high methodological quality, 4 showed a positive association between breastfeeding and weight change. McClure et al. found that 7 years post-partum, the amount of visceral fat measured by computed tomography was greater among those women who breastfed for less than 3 months after the birth of each child, compared to those who breastfed longer [14]; however, they did not observe such a relation regarding body mass index (BMI) and other fatness indicators. Bobrow et al. showed that postmenopausal women who had breastfed, had a significantly lower BMI than those who had never breastfed [15]. Snyder et al. found that breastfeeding was significantly associated with smaller waist circumference after a mean follow-up period of 11 (7–15) years [16]. Results of a cluster-randomized controlled trial did not confirm that a longer time spent breastfeeding led to any significant reduction in fatty tissue more than 11 years postpartum [17]. Studies on the relationship between breastfeeding and long-term weight changes in women are inconclusive. It is therefore important to examine breastfeeding history as an independent factor that can potentially have a long-term influence on female fatness.
Most studies have confirmed that parity strongly increases the risk of excess body mass in women whilst extended breastfeeding duration has the opposite effect i.e. lower body mass [15, 18, 19]. Weight gain in women who have given birth is much greater than in those who have never given birth [18, 19]. Many studies show that menopausal transformation in women leads to an increased risk of obesity [20,21,22,23,24]. Menopause onset is associated with decreased energy expenditure and fat oxidation which can predispose to excess of body fat mass [20, 24].
The aim of the study was to assess the relationship between breastfeeding duration and body fat indices: BMI, body fat percentage (%BF) and waist-to-height ratio (WHtR) in middle-aged women. All analyzes were carried out separately for premenopausal and postmenopausal women, in three fertility categories.
Methods
Design and sample
The research material consists of the data of 8725 participants of the PONS (POlish-Norwegian Study) project, carried out 2010–2012, in the province of Świętokrzyskie in Poland. Ethics Committee from the Cancer Centre and Institute of Oncology in Warsaw, No. 69/2009/1/2011 (data collection), and Committee on Bioethics at the Faculty of Health Sciences, Jan Kochanowski University in Kielce, Poland (No. 29/2015) (data analysis) approved the study.
This was a secondary data analysis aiming to assess the health status of the female adult population of the Świętokrzyskie region in Poland. Anthropometric and blood pressure measurements were performed, and body composition analysis and biochemical blood analysis were carried out. An extensive questionnaire interview was conducted to gather socio-economic data, lifestyle information, and medical history. The study protocol is described in detail in previously published articles [25,26,27].
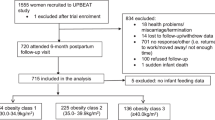
The analysis excluded 327 women with diagnosed cancer, 263 with incomplete data and 635 women who had never given birth. The final sample consisted an ethnically-homogenous, Caucasian population of 7500 parous women (Additional file 1: Fig. SM1).
Measurements
All measurements were obtained by trained nurses. The following data was used in this study: anthropometric measurements of body weight, height and waist circumference, from which BMI (kg/m2) and WHtR (waist circumference/height) were calculated, as well as body fat percentage (% BF) measurement using the bioelectrical impedance method.
Sociodemographic and lifestyle data
The questionnaire interview was conducted by trained nurses. The following socio-demographic and lifestyle information was collected in the survey: age (years), education (years), place of residence (urban; rural), marital status (married or in a stable relationship; single or widower), parity (1, 2, 3 and more children), menopausal status (premenopausal, postmenopausal), total duration of breastfeeding in months (then divided into breastfed 1–6; 7–12; > 12 months or never breastfed) and the use of hormone therapy (ever, never). The subjects were also divided into never, former or current smokers. The long form International Physical Activity Questionnaire (IPAQ) was used to assess physical activity, and it was expressed as Moderate-to-Vigorous (MVPA) and light physical activity (LPA) (Metabolic Equivalent of Task—MET/min/day−1) [28].
Sitting time was expressed in minutes/day. Food consumption data was collected using the Food Frequency Questionnaire (FFQ), based on a previously-developed and validated FFQ for the Polish branch of the PURE study [29]. As it was not possible to calculate the calorific value of the subjects’ diets based on the collected data, the analysis included 3 groups of products that could potentially have the greatest impact on fatness: fats (butter, lard, margarine, mayonnaise, rapeseed oil, soya, sunflower oil, olive oil, and other oils), sweets (sugar, chocolate and chocolate-products, candies, cakes, cookies), whole grains (whole grain bread, groats, cereals). Answers related to the consumption frequency of products with standard portion sizes, and were transformed into daily consumption doses and standardized by z-score.
Definition of terms
The overweight group included women with BMI ≥ 25.0 kg/m2, it was assumed that excess fatty tissue indicating obesity was > 35% BF [30], and for abdominal obesity it was WHtR ≥ 0.5 [31]. The North American Menopause Society, postmenopausal women include those with amenorrhea for at least 12 months [32].
Statistical analysis
All categorical variables were expressed as frequency and percentage (n, %) and all continuous variables were reported as means and standard deviations (X ± SD). Differences in baseline characteristics between normal and abnormal adiposity were assessed using the Mann–Whitney U test for continuous variables and the Chi-square test for categorical variables. The probability of excessive weight and/or obesity in relation to total breastfeeding duration was assessed using multivariate logistic regression analyses, calculating the odds ratios (ORs) and 95% confidence intervals (CIs). The analyses were carried out separately in three categories of parity, in raw and adjusted models for confounding variables. The control group (ref.) consisted of women who had never breastfed. In models adjusted as confounders, the following were adopted: age; years of education, MVPA, LPA, sitting time, consumption of fats, sweets, whole grains, (continuous variables), and place of living (ref. urban), marital status (ref. single), smoking (ref. never smokers), and hormone therapy (ref. never). Confounders were chosen based on relationships found in previous analyses of the collected data [23, 26, 33, 34] as well as literature analysis [13]. Analyses were performed using the statistical package Statistica 13.3 (TIBCO SOFTWARE INC, Polish version, PL, Cracow). A p value ≤ 0.05 represented statistical significance.
Results
The average age of the women studied was 55.5 ± 5.3 years. In the premenopausal group, overweight and obese women were older, less well-educated, inhabited rural areas more than urban, and were more often in stable relationships compared to those with normal weight (Table 1). They also devoted less time to LPA, and declared a lower consumption of sugar and sweets. Women with more body fat (%BF > 35%) more often declared limiting fat intake. Women with abdominal obesity (WHtR ≥ 0.5) consumed sweets with a similar frequency as women without abdominal obesity, while declaring a lower intake of whole grains. In the compared groups (BMI ≥ 25 kg/m2 vs. < 25 kg/m2, %BF > 35% vs. ≤ 35%, and WHtR ≥ 0.5 vs. < 0.5), no significant differences were found in the time spent in MVPA or sitting time. The percentage of smokers was similar in the compared groups. Overweight and obese women more often gave birth to 3 or more children and less often used hormonal therapy. The percentage of women who breastfed for > 12 months was higher in the overweight group (BMI ≥ 25 kg/m2) than in the normal weight group. Differences between the compared groups were not statistically significant for the other obesity indices.
Among postmenopausal women, overweight and obese women were also older, less well-educated and inhabited rural areas more often than urban, compared to women with normal weight (Table 2). Marital status was not a significant factor in the occurrence of excessive weight and abdominal obesity, though participants in stable relationships had a higher body mass (%BF > 35%). Overweight and obese women spent less time in LPA, smoked less often, used hormone therapy less often, and declared lower sugar and sweets consumption, while women with abdominal obesity (WHtR ≥ 0.5) also declared a lower consumption of whole grains. There were no significant differences in fat intake or sitting time between groups. The percentage of overweight women who gave birth to 3 or more children was higher, whereas the percentage who gave birth to only 1 child was lower. A higher percentage breastfed > 12 months, and a lower percentage breastfed 1–6 months.
An analysis of the unadjusted ORs in premenopausal women showed no significant association between the duration of lactation and the risk of excessive weight and obesity in any of the three parity categories (Additional file 2: Table SM1). In postmenopausal women who gave birth to 2 children, the risk of abdominal obesity was significantly lower in those who breastfed for 1–6, as well as > 12 months, compared to those who had never breastfed (Additional file 2: Table SM2). In the group who gave birth to 3 or more children, the risk of excessive weight (BMI ≥ 25 kg/m2) and abdominal obesity (WHtR ≥ 0.5), was significantly lower in those who breastfed for 1–6 months compared to non-breastfeeding mothers. A similar tendency was observed with longer lactation, but it was not statistically significant. There was no association between the duration of lactation and the risk of excessive body fat (%BF > 35%).
The analysis of adjusted ORs did not show any significant associations between the length of breastfeeding and the risk of excessive weight and obesity in premenopausal women of any parity (Table 3). The results for those in the breastfeeding group who gave birth to 3 or more children were 0.39 to 0.51 for BMI ≥ 25 kg/m2, and 0.54 to 0.76 for WHtR ≥ 0.5. Although not statistically significant, these values were similar and sometimes lower than in the postmenopausal group. Postmenopausal women who gave birth to one child and breastfed for 7–12 months had a higher risk of abdominal obesity compared to those who did not breastfeed (Table 4). Among women who gave birth to 2 children, breastfeeding was associated with a lower risk of abdominal obesity (WHtR ≥ 0.5). Participants who gave birth to 3 or more children and breastfed for 1–6 months had a lower risk of being overweight (BMI ≥ 25 kg/m2) compared to those who had never breastfed.
Discussion
This study showed that in postmenopausal women who had given birth to 2, 3 or more children, breastfeeding was associated with a lower risk of excessive weight and abdominal obesity, compared to women of the same parity who did not breastfeed at all. Adjustment for confounding factors did weaken the associations slightly, but they remained statistically significant in many groups.
Most studies confirm an inverse association between breastfeeding duration and the risk of obesity [15, 35,36,37]. In the Norwegian population, the probability of obesity in women under the age of 50, who had never breastfed, was 3.37 times higher compared to those who had breastfed for at least 24 months [38]. Bobrow et al. reported that in postmenopausal women, the mean BMI was 0.22 kg/m2 lower for each additional 6 months of breastfeeding [15].
Some studies, however, have not confirmed the association between the lactation duration and fatness [17, 39]. Sharma et al. found that women with obesity six years postpartum and who fully complied with the recommendations regarding breastfeeding at that time (i.e., they were exclusively breastfeeding for ≥ 4 months and continuing breastfeeding for ≥ 12 months) had a lower body mass than obese women who had never breastfed; they did not find such associations in women with normal weight or who were overweight [40].
The results of our study are largely consistent with those studies which demonstrate a positive effect of breastfeeding on reducing the risk of abdominal obesity. In a cross-sectional study of American women who were on average 7 years postpartum, the amount of visceral adipose tissue measured by computed tomography was over 20 cm2 higher among mothers who breastfed for < 3 months after the birth of each child, compared to those who breastfed longer [14, 36]. Women of diverse ethnicity (Filipino, Caucasian, and African-American) who breastfed > 3 months had lower volumes of visceral fat at age 55–80 years than those who breastfed ≤ 3 months [36]. These relationships in both studies were independent of covariates. Women who breastfed for > 6 months, had a significantly smaller waist circumferences 10 years postpartum than those who breastfed for a shorter period [16]. Kirkegaard et al. who showed a weak but significant inverse association between breastfeeding duration and body weight 7 years postpartum, and found this association to be much stronger in BMI-adjusted waist circumference analysis [37]. The mechanism by which a longer period of breastfeeding can reduce the risk of abdominal obesity in the long term is poorly understood. Visceral adipose tissue is more susceptible to reduction compared to subcutaneous adipose tissue because adipocytes of the epiploic and mesenteric adipose tissue, the main components of visceral fat, show greater metabolic activity and lipolytic sensitivity [41,42,43]. Subcutaneous and visceral adipocytes show differences in the expression of certain genes [44]; visceral adipocytes are characterised by higher lipolytic activity (significantly higher expression of the lipoprotein lipase gene) than subcutaneous adipocytes [45]. This may be important for fat mobilisation during lactation. Studies on rats [46] and humans [47, 48] have confirmed the preferential use of visceral fat over subcutaneous fat during lactogenesis. The CARDIA study showed that in a group of 910 participants, any duration of lactation was associated with significantly lower amounts of visceral fat [48]. The authors of that study did not, however, find a significant relationship between lactation and volume of subcutaneous, intermuscular, and total abdominal fat, after allowing for pre-pregnancy cardiometabolic factors. Kirkegaard et al., however, explain greater reduction of visceral than subcutaneous fat by the strong confounding effects of visceral adipose tissue before pregnancy [37]. If the greater amount of abdominal fat pre-pregnancy is associated with shorter breastfeeding duration, this may also explain the direct relationship between breastfeeding and waist circumference postpartum.
In the postmenopausal women we studied, those who gave birth to one child and breastfed for 7–12 months, had increased risk of abdominal obesity compared to those who did not breastfeed, which is contrary to expectations. This result may be due to the relatively small number of women who gave birth to only one child, but breastfed more than 6 months (3.19%). Our results did not reveal any significant association between breastfeeding and risk of excessive weight and obesity in premenopausal women. The values of adjusted ORs in this group, however, indicate a lower probability of lactating women to be overweight and have abdominal obesity, compared to those who have never breastfed. Our study also showed no correlation between the duration of lactation and percentage of body fat. Similarly, McClure et al., found increased visceral adipose tissue, measured by computed tomography 7 years postpartum among women who breastfed for > 3 months after the birth of each child, compared to those who breastfed longer [14]; they did not observe the same relationship for BMI and other body fat indices. Only Wiklund et al. found that women who breastfed their children for < 6 months had a higher body fat mass and %BF measured using dual-energy X-ray absorptiometry (DEXA), compared to those who breastfed for longer [35]. It is therefore possible that these associations are only revealed by more precise measurements of body fat, such as DEXA.
The main limitation of the study is that is was cross-sectional. The nutritional status of the participants before pregnancy was not known, nor was the amount of pregnancy weight gain. Therefore, these variables could not be included in the analysis as confounders. We also lacked detailed information on the intensity and regularity of breastfeeding. Some studies indicate that the effect of lactation on the risk of obesity may depend on whether the women breastfed their children exclusively or not [49]. The primary strength of the study is the large number of women included in the analysis (7500), taking into account the large number of confounding factors, including physical activity levels and nutritional factors, as well as conducting separate analyses according to parity and menopausal status.
Conclusions
In women who gave birth to at least 2 children, breastfeeding was associated with a slightly lower risk of excessive weight and abdominal obesity after menopause, compared to women of the same parity who did not breastfeed at all. Breastfeeding may therefore have some beneficial, long-term effect on female fatness. Long-term studies are required in order to confirm the proposed association.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Change history
16 June 2021
A Correction to this paper has been published: https://doi.org/10.1186/s12905-021-01378-2
Abbreviations
- %BF:
-
Body Fat Percentage
- BMI:
-
Body Mass Index
- CI:
-
Confidence Intervals
- LPA:
-
Light Physical Activity
- MET:
-
Metabolic Equivalent of Task
- MJ:
-
Megajules
- MVPA:
-
Moderate to Vigorous Physical Activity
- OR:
-
Odds Ratio
- PA:
-
Physical Activity
- WHtR:
-
Waist to Height Ratio
References
GBD 2015 Obesity Collaborators, Afshin A, Forounzafar MH, Reitsma MB, Sur P, Estep K, Lee A, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377:13–27.
Khan SS, Ning H, Wilkins JT, Allen N, Carnethon M, Berry JD, et al. Association of body mass index with lifetime risk of cardiovascular disease and compression of morbidity. JAMA Cardiol. 2018;3:280–7.
Marott SCW, Nordestgaard BG, Tybjærg-Hansen A, Benn M. Causal associations in type 2 diabetes development. J Clin Endocrinol Metab. 2019;104:1313–24.
Lauby-Secretan B, Scoccianti C, Loomis D, Grosse Y, Bianchini F, Straif K. Body fatness and cancer—viewpoint of the IARC working group. N Engl J Med. 2016;375:794–8.
Hawksworth G, Hales J, Martinez F, Hynes A, Hamilton A, Fernandez V. Pancreatic cancer trends in Europe: epidemiology and risk factors. Med Stud/Studia Medyczne. 2019;35:164–71.
Biskup M, Macek P, Król H, Nogajczyk M, Terek-Derszniak M, Skowronek T, et al. Predictions of the incidence of gastrointestinal cancers in the Świętokrzyskie region by the year 2025. Med Stud/Studia Medyczne. 2019;35:32–40.
NCD Risk Factor Collaboration. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet. 2016;387:1377–96.
Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in obesity among adults in the United States, 2005 to 2014. JAMA. 2016;315:2284–91.
Rooney BL, Schauberger CW. Excess pregnancy weight gain and long-term obesity: one decade later. Obstet Gynecol. 2002;100:245–52.
Mannan M, Doi SA, Mamun AA. Association between weight gain during pregnancy and postpartum weight retention and obesity: a bias-adjusted meta-analysis. Nutr Rev. 2013;71:343–52.
Stuebe AM, Rich-Edwards JW. The reset hypothesis: lactation and maternal metabolism. Am J Perinatol. 2009;26:81–8.
Butte NF, King JC. Energy requirements during pregnancy and lactation. Public Health Nutr. 2005;8:1010–27.
Neville CE, McKinley MC, Holmes VA, Spence D, Woodside JV. The relationship between breastfeeding and postpartum weight change - a systematic review and critical evaluation. Int J Obes (Lond). 2014;38:577–90.
McClure CK, Catov J, Ness R, Schwarz EB. Maternal visceral adiposity by consistency of lactation. Matern Child Health J. 2012;16:316–21.
Bobrow KL, Quigley MA, Green J, Reeves GK, Beral V. Persistent effects of women’s parity and breastfeeding patterns on their body mass index: results from the Million Women Study. Int J Obes (Lond). 2013;37:712–7.
Snyder GG, Holzman C, Sun T, Bullen B, Bertolet M, Catov JM. Breastfeeding greater than 6 months is associated with smaller maternal waist circumference up to one decade after delivery. J Womens Health (Larchmt). 2019;28:462–72.
Oken E, Patel R, Guthrie LB, Vilchuck K, Bogdanovich N, Sergeichick N, et al. Effects of an intervention to promote breastfeeding on maternal adiposity and blood pressure at 11.5 y postpartum: results from the Promotion of Breastfeeding Intervention Trial, a cluster-randomized controlled trial. Am J Clin Nutr. 2013;98:1048–56.
Zoet GA, Paauw ND, Groenhof K, Franx A, Gansevoort RT, Groen H, et al. Association between parity and persistent weight gain at age 40–60 years: a longitudinal prospective cohort study. BMJ Open. 2019;9:e024279.
Rosenberg L, Palmer JR, Wise LA, Horton NJ, Kumanyika SK, Adams-Campbell LL. A prospective study of the effect of childbearing on weight gain in African-American women. Obes Res. 2003;1:1526–35.
Ko SH, Kim HS. Menopause-associated lipid metabolic disorders and food beneficial for postmenopausal women. Nutrients. 2020;12(1):202.
Mauvais-Jarvis F, Clegg DJ, Hevener AL. The role of estrogens in control of energy balance and glucose homeostasis. Endocr Rev. 2013;34:309–38.
Kohrt WM, Wierman ME. Preventing fat gain by blocking follicle-stimulating hormone. N Engl J Med. 2017;377:293–5.
Suliga E, Kozieł D, Cieśla E, Rębak D, Głuszek S. Factors associated with adiposity, lipid profile disorders and the metabolic syndrome occurrence in premenopausal and postmenopausal women. PLoS ONE. 2016;11:e0154511.
Lovejoy JC, Champagne CM, de Jonge L, Xie H, Smith SR. Increased visceral fat and decreased energy expenditure during the menopausal transition. Int J Obes. 2008;32:949–58.
Zatonski WA, Manczuk M. Kielce PONS Team: POlish-Norwegian Study (PONS): Research on chronic non-communicable diseases in European high risk countries—study design. Ann Agric Environ Med. 2011;18:203–6.
Suliga E, Koziel D, Ciesla E, Gluszek S. Association between dietary patterns and metabolic syndrome in individuals with normal weight: a crosssectional study. Nutr J. 2015;14:55.
Suliga E, Kozieł D, Cieśla E, Rębak D, Głuszek S. Sleep duration and the risk of obesity—a cross-sectional study. Med Stud/Studia Medyczne. 2017;33:176–83.
International Physical Activity Questionnaire (IPAQ) - The Long Form. Available online:http://www.sdp.univ.fvg.it/sites/default/files/IPAQ_English_self-admin_long.pdf. Accessed on 15 March 2010.
Dehghan M, Ilow R, Zatonska K, Szuba A, Zhang X, Mente A, Regulska-Ilow B. Development, reproducibility and validity of the food frequency questionnaire in the Poland arm of the Prospective Urban and Rural Epidemiological (PURE) study. J Hum Nutr Diet. 2012;25:225–32.
AACE/ACE Obesity Task Force. AACE/ACE position statement on the prevention, diagnosis, and treatment of obesity. Endocr Pract. 1998;4:297–350.
Browning LM, Hsieh SD, Ashwell M. A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes: 0.5 could be a suitable global boundary value. Nutr Res Rev. 2010;23:247–69.
Shifren JL, Gass ML, Group NRfCCoMWW. The North American Menopause Society recommendations for clinical care of midlife women. Menopause. 2014;21: 1038–62.
Suliga E, Cieśla E, Rębak D, Kozieł D, Głuszek S. Relationship between sitting time, physical activity, and metabolic syndrome among adults depending on body mass index (BMI). Med Sci Monit. 2018;24:7633–45.
Suliga E, Kozieł D, Cieśla E, Rębak D, Głuszek S. Dietary patterns in relation to metabolic syndrome among adults in Poland: a cross-sectional study. Nutrients. 2017;9:1366.
Wiklund P, Xu L, Lyytikäinen A, Saltevo J, Wang Q, Völgyi E, et al. Prolonged breastfeeding protects mothers from later-life obesity and related cardio-metabolic disorders. Public Health Nutr. 2012;15:67–74.
Armenta RF, Kritz-Silverstein D, Wingard D, Laughlin GA, Wooten W, Barrett-Connor E, et al. Association of breastfeeding with maternal visceral adiposity postmenopause among three racial/ ethnic groups. Obesity (Silver Spring). 2015;23:475–80.
Kirkegaard H, Stovring H, Rasmussen KM, Abrams B, Sørensen TIA, Nohr EA. How do pregnancy-related weight changes and breastfeeding relate to maternal weight and BMI-adjusted waist circumference 7 y after delivery? Results from a path analysis. Am J Clin Nutr. 2014;99:312–9.
Natland ST, Nilsen TI, Midthjell K, Andersen LF, Forsmo S. Lactation and cardiovascular risk factors in mothers in a population-based study: the HUNT-study. Int Breastfeed J. 2012;7:8.
Schwarz EB, Ray RM, Stuebe AM, Allison MA, Ness RB, Freiberg MS, et al. Duration of lactation and risk factors for maternal cardiovascular disease. Obstet Gynecol. 2009;113:974–82.
Sharma AJ, Dee DL, Harden SM. Adherence to breast-feeding guidelines and maternal weight 6 years after de-livery. Pediatrics. 2014;134(Suppl 1):S42–9.
Bjørndal B, Burri L, Staalesen V, Skorve J, Berge RK. Different adipose depots: their role in the development of metabolic syndrome and mitochondrial response to hypolipidemic agents. J Obes. 2011;2011:490650.
Letexier D, Pinteur C, Large V, Fréring V, Beylot M. Comparison of the expression and activity of the lipogenic pathway in human and rat adipose tissue. J Lipid Res. 2003;44:2127–34.
Tchernof A, Bélanger C, Morisset AS, Richard C, Mailloux J, Laberge P, et al. Regional differences in adipose tissue metabolism in women. minor effect of obesity and body fat distribution. Diabetes. 2006;55:1353–60.
Ronquillo MD, Mellnyk A, Cárdenas-Rodríguez N, Martínez E, Comoto DA, Carmona-Aparicio L, Herrera NE, Lara E, Pereyra A, Floriano-Sánchez E. Different gene expression profiles in subcutaneous & visceral adipose tissues from Mexican patients with obesity. Indian J Med Res. 2019;149:616–26.
Małodobra-Mazur M, Cierzniak A, Pawełka D, Kaliszewski K, Rudnicki J, Dobosz T. Metabolic differences between subcutaneous and visceral adipocytes differentiated with an excess of saturated and monounsaturated fatty acids. Genes (Basel). 2020;11:1092.
Moore BJ, Olsen JL, Marks F, Brasel JA. The effects of high fat feeding during one cycle of reproduction consisting of pregnancy, lactation and recovery on body composition and fat pad cellularity in the rat. J Nutr. 1984;114:1566–73.
McClure CK, Schwarz EB, Conroy MB, Tepper PG, Janssen I, Sutton-Tyrrell KC. Breastfeeding and subsequent maternal visceral adiposity. Obesity (Silver Spring). 2011;19:2205–13.
Appiah D, Lewis CE, Jacobs DR, Shikany JM, Quesenberry CP, Gross M, Carr J, Sidney S, Gunderson EP. The association of lactation duration with visceral and pericardial fat volumes in parous women: the CARDIA study. J Clin Endocrinol Metab. 2021;1:dgaa980. https://doi.org/10.1210/clinem/dgaa980.
Jarlenski MP, Bennett WL, Bleich SN, Barry CL, Stuart EA. Effects of breastfeeding on postpartum weight loss among US women. Prev Med. 2014;69:146–50.
Acknowledgements
The data collection was supported by the Maria Sklodowska-Curie Institute of Oncology in Warsaw (Poland) and the Polish-Norwegian Foundation Research Fund.
Funding
The project was supported under the program of the Minister of Science and Higher Education under the name “Regional Initiative of Excellence” in 2019–2022, project number: 024/RID/2018/19, financing amount: 11.999.000,00PLN.
Author information
Authors and Affiliations
Contributions
Conceptualization, E.Su., E.C., E.St., and S.G.; Funding acquisition, E.Su., and S.G.; Methodology, E.Su., E.C., and S.G.; Software, E.C. Supervision, E.S. and S.G.; Writing—original draft preparation, E.Su., E.C., and E.St.; Writing—review and editing, E.C., and E.St.;. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent was obtained from all study participants. All methods were performed in accordance with the relevant guidelines and regulations. Ethics approval was obtained through the Cancer Centre and Institute of Oncology in Warsaw, No. 69/2009/1/2011 (data collection), and Committee on Bioethics at the Faculty of Health Sciences, Jan Kochanowski University in Kielce, Poland (No. 29/2015) (data analysis) approved the study.
Consent for publication
Not aplicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised:Following the publication of the original article, we were notified that the titles of the two Supplementary materials had been reversed.
Supplementary Information
Additional file 1: Figure SM1
. Study flowchart.
Additional file 2: Table SM1
. Multivariable logistic regression analysis for overweight and obesity in relation to breastfeeding duration in premenopausal women (unadjusted). Table SM2: Multivariable logistic regression analysis for overweight and obesity in relation to breastfeeding duration in postmenopausal women (unadjusted).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cieśla, E., Stochmal, E., Głuszek, S. et al. Breastfeeding history and the risk of overweight and obesity in middle-aged women. BMC Women's Health 21, 196 (2021). https://doi.org/10.1186/s12905-021-01332-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-021-01332-2