
Abstract
Background
The quality of life (QoL) of patients with endometriosis and infertility was assessed in different stages and correlated with the clinical features of the cases.
Methods
The present study was a cross-sectional study; 106 women were included, divided in two endometriosis groups (Grade I/II, 26 women, and Grade II/IV, 74 women). All participants attended the Endometriosis and Infertility Outpatient Clinic of the Instituto Ideia Fértil de Saúde Reprodutiva, Faculdade de Medicina do ABC, São Paulo, Brazil, were and responded to the Short Form (SF) Health Survey-36. Convenience sampling was used due to the authors’ access to the study population; however, the sample number was calculated to be sufficient for 95% power in both groups.
Results
Homogeneity was observed between Grade I/II and Grade III/IV staging, with similar mean ages (35.27, ±3.64 years and 34.04, ±3.39 years, respectively, p = 0.133); types of infertility (p = 0.535); infertility time (p = 0.654); degrees of pain (p = 0.849); and symptoms common to endometriosis, namely, dysmenorrhea (p = 0.841), dyspareunia (0.466), chronic pelvic pain (p = 0.295), and intestinal (p = 0.573) or urinary (p = 0.809) diseases. Comparisons of median scores in the QoL domains demonstrated that the distributions of QoL and clinical symptoms were significantly related between the types of dyspareunia and the following domains: physical functioning (p = 0.017), role- emotional (p = 0.013), and general health (p = 0.001). Regarding pain outside of menstruation, there was significance in the pain domain (p = 0.017), and degree of pain was significance in physical functioning (p = 0.005) and role-physical (p = 0.011) domains.
Conclusions
The present study pointed out that it is not the stage of endometriosis that interferes in the quality of life of women with endometriosis and infertility but rather the clinical manifestations, such as dyspareunia and pain. Thus, we can conclude that the patient’s perception of the disease should be considered in health care and that the losses are independent of the degree of endometriosis in this population with the aggravating factor of infertility.
Similar content being viewed by others


Background
Endometriosis is a heterogeneous disease characterized by the presence of endometrial tissue outside the uterine cavity. It may be asymptomatic or could include clinical manifestations such as chronic pelvic pain, dysmenorrhea, dyspareunia, dysuria, pain after the menstrual period, and infertility [1,2,3,4].
Endometriosis occurs in women in the reproductive phase with a high incidence, and worsens their quality of life (QoL) [5, 6], causing discomfort, psychic, physiological, marital, and social liability [7].
It is a disease that can lead to social isolation; and such behavior may be related to pain and fatigue that also trigger psychological alterations; loss of productivity and yield at work; whilst its recurrence has the greatest negative impact on psychological health, vitality, financial conditions, and reduction in social activities [8,9,10,11].
According to recent data, endometriosis is a very complex condition, and psychological aspects play an important role in determining both, its severity of symptoms and effectiveness of treatments [12].
Due to the chronicity of endometriosis, it may be associated with considerable physical and emotional morbidity; and it is also known that disease carriers experience harm in their daily activities, which has an economic impact due to a reduction or loss of working hours and hospitalizations [13, 14].
The reduction of QoL in this population can be explained by the complexity of disease etiology and manifestations, as well as by the interference in women’s reproductive capacity. In addition, treatment does not necessarily guarantee a cure or complete remission of symptoms but may only contribute to improving the patients’ QoL [15].
Since endometriosis is one of the most common benign gynecological diseases, it has a 10% prevalence among women of reproductive age [16]. Patients with endometriosis are 20 times more likely to experience infertility; in addition to its being considered a cause for spontaneous abortion [17]. Moreover, 25–50% of infertile women have endometriosis, and 30–50% of women with endometriosis are infertile [18].
The present study’s aim was to verify the levels of QoL in women with endometriosis and infertility; and to compare these levels between staging groups as well as the clinical symptoms of endometriosis with aggravating factors of infertility. This proposal would be of interest in providing improvements and specificity in the monitoring of this population, considering interdisciplinary aspects.
Methods
Design and setting of the study
For verifying QoL by comparing the staging groups and clinical symptoms of endometriosis, this cross-sectional and observational study that was carried out at the Instituto Ideia Fértil (IIF), Faculdade de Medicina do ABC, Santo André - SP, Brazil used a quantitative approach and adopted the STROBE guidelines [19].
Characteristics of participants and setting
A total of 106 women, who did not become pregnant 6 months after diagnosis by laparoscopy; and who had attended the IIF Endometriosis and Infertility Clinic from April to December 2015, were included. They were recruited after a specific consultation in the endometriosis outpatient clinic and were personally invited by the first author. From the 210 who were invited, 106 accepted; while those who declined reported no interest in research.
A convenience sample was used because the authors had direct access to the IIF endometriosis outpatient clinic, and the minimum sample size of 100 participants was stipulated by a free statistical software program (G*Power Software) to achieve 95% power considering the proposed analytical model, studied variables, and the number of groups.
Considering the differences in symptomatology described in the literature; the participants were divided according to the staging of endometriosis into two groups: stage I/II (26 women) and stage III/IV (80 women).
All the patients had only undergone a laparoscopy, in which the diagnosis of endometriosis was made. They had performed the laparoscopy procedure due to their symptom of chronic pain.
Selection criteria
The inclusion criteria were infertile and endometriosis women whose diagnosis and staging of the disease had been confirmed by laparoscopy; and those who had agreed to participate in the study and had signed the consent and post-consent forms. The exclusion criteria comprised: age less than 18 years; carriers of endometriosis whose infertility included an associated male factor; used analgesics or anti-inflammatory drugs or hormonal treatment in the past 3 months; as well as diagnosed and/or being treated for depression or anxiety; that were all factors that could interfere with responses to the Medical Outcomes Study 36-item short-form health survey (SF-36) questionnaire.
Data collection and measures
The participants were personally invited to participate in the research, only if they accepted, signed the informed consent form, responded to the SF-36, and gave researchers access to their medical records. Each participant took, on an average, 15 min to complete the questionnaire.
For data collection, the SF-36 [20], which measures impairment in an individual’s QoL in a generic manner was used. Since it was validated in 1999 in Brazil by Ciconelli et al. [21], as well as in 2014, for the population with endometriosis [22]; it facilitates measuring the QoL of patients with endometriosis, and can be used as a prognostic indicator of clinical improvement [23]. The SF-36 which evaluates eight QoL domains: physical functioning, role-physical, bodily pain, role-emotional, general health, vitality, social functioning, and mental health; is among the most used instruments worldwide [14, 15, 22,23,24,25,26,27,28,29]. The cutoff points or domains for interpreting the QoL levels were based on the Bieleman study [30], which adopted a criterion in which values above 60 points (on a scale of 0 to 100) indicated preservation of QoL.
The clinical data verified in the electronic medical record included age; infertility time (in years); menarche age; infertility type (primary or secondary); previous oral conceptive pill use (yes-no) and usage time (in years); miscarriage (yes-no); staging of endometriosis according to the “Revised American Society for Reproductive Medicine (ASRM) classification of endometriosis: 1996” [31]; and confirmation of endometriosis from the results of a pathology examination. The degree of pain during menstruation was assessed by a clinical questionnaire on five levels: 0-absent, 1-mild, 2-moderate, 3-severe, and 4-disabling. The presence or absence of dyspareunia was assessed as: superficial – pain in entrance of the vagina, deeper – pain during penetration or thrusting of the penis, and superficial and deeper – both types) [32]. Similarly, chronic pelvic pain, dysmenorrhea, intestinal (tenesmus and/or enterorrhagia during menstruation), and urinary (dysuria and/or hematuria during menstruation) disorders were also assessed. All medical visits were performed by a gynecologist specialized in endometriosis and infertility (the third author).
Statistics
The descriptive variables were verified using frequency analysis. The non-normal quantitative variables were presented as medians and interquartile ranges (IQR), the normal quantitative variables were presented as means and Standard Deviation (SD). The power for the intragroup tests was 95% for both groups, tested by the G*Power Software. The data missing were verified and found to be non-existent. The data were verified for normality through the Kolmogorov-Smirnov test, with a partially non normal distribution; to reach the proposed goal, nonparametric and parametric tests were used. Mann-Whitney tests or t-Tests were used to verify the QoL domains’ relationship with the type of infertility; and the degree of endometriosis and QoL with the profile of the participants. Kruskal-Wallis or ANOVA tests were used to verify the association between the QoL domains and the clinical aspects of endometriosis or the participants’ profiles. The chi-squared test was also used to associate the profile of the participants with the staging of endometriosis. Spearman or Pearson’s correlations were used for continuous variables (complete analysis can access in supplementary material). The program for statistical analyses was SPSS 21 for Windows. Considering the difference in the sample size of the groups, the specific “n power” for the intergroup comparison tests was calculated to be 73% in the t-Test/Mann-Whitney test and 99% in the ANOVA/Kruskal-Wallis tests, both with a medium effect size. The significance level adopted for all analyses was p ≤ 0.05.
Results
Patient profiles
The 106 participants, who were divided according to stage I/II (n = 26) and stage III/IV (n = 80), exhibited mean ages of 35.27 ± 3.64 years and 34.04 ± 3.27 years, respectively, (p = 0.133). Both groups underwent laparoscopy and were homogeneous for the type of infertility (p = 0.536), menarche age (p = 0.254), infertility time (p = 0.654), miscarriage (p = 0.528), previous oral conceptive pill usage (p = 0.606), degree of pain (p = 0.194), dysmenorrhea (p = 0.841), dyspareunia (p = 0.466), chronic pelvic pain (p = 0.295), intestinal disorders (p = 0.573), and urinary disorders (p = 0.809). The stage III/IV group had used contraceptive pills longer than the stage I/II group (p = 0.012) (Table 1).
QoL related to disease staging
No statistically significant differences were found in the QoL domains between the groups based on the degree of endometriosis. Moreover, most domains exhibited good scores. When the adopted cutoffs were verified, lower values were identified for stage I/II in the domains of general health (mean 58.69, SD ±16.56), vitality (mean 54.42, SD ±14.72), and mental health (mean 59.54, SD ±21.18); and for stage III/IV in the domains of pain (median 57.00, IQR 43.00), vitality (mean 56.24, SD ±11.38), and mental health (mean 59.23, SD ±18.52) (Table 2).
QoL and clinical symptomatology of endometriosis
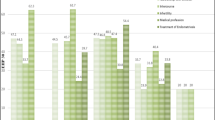
After considering the homogeneity of the clinical characteristics of endometriosis between the groups studied, that may have been due to the laparoscopy performed 6 months prior; it was decided to verify possible associations between the clinical characteristics of endometriosis and the QoL of the patients, without any distinctions between the mentioned groups. The scores of the QoL domains of the SF-36 were compared with all the clinical symptom types and profiles of participants. The results showed that the distribution of QoL differed significantly between the types of dyspareunia and the following domains: general health (p = 0.001), role-emotional (p = 0.013) and physical functioning (p = 0.017); with the “penetration” group presenting the lowest value between the previous oral conceptive pill use and role-emotional (p = 0.020); between the chronic pelvic pain and bodily pain (p = 0.017); and between degree of pain and physical functioning (p = 0.005); and role-physical (p = 0.011). The domains of the SF-36 that exhibited some significant differences by clinical symptomatology are described in Table 3.
Discussion
From the results, it can be verified that the staging of endometriosis in the present sample was not associated with a difference in their QoL scores. This suggests that the reduction of QoL in the infertile and endometriosis population would require a more complex explanation than just the stages of endometriosis [15, 33]; and that infertility associated with endometriosis would impair QoL [34].
In this sense, the association of QoL with clinical manifestations rather than the degree of endometriosis as observed in this study, may be partially justified due to the homogeneity of the groups’ characteristics due to the laparoscopy that had been previously performed. Moreover, since the pain related to endometriosis was not explained by the disease itself [35], this suggests aspects related to the clinical manifestation with subsequent QoL impairment. Such an association can be verified in dyspareunia and degree of pain, which tend to interfere with the activities of daily living, causing, for example, mood swings and pain [36].
The physiological aspect should, therefore, be considered. An Italian study [37] identified that treatment for endometriosis reduced pain symptoms, such as dysmenorrhea, dyspareunia, and dysuria; and the reduction was positively associated with QoL. Thus, the pain sensations that impaired the perception of health can be seen in the present study in the relationship between degrees of pain and dyspareunia as well as the QoL domains (physical functioning, role-physical, role-emotional and general health).
Dyspareunia was the clinical symptom that was most associated with lower levels of QoL in the present study, and this finding was also corroborated by Caruso et al. [26]. Although dyspareunia is generally associated with more advanced degrees of the disease; women with minimal pelvic involvement may also experience intense pain, which again supports that the discomfort of the clinical manifestations of endometriosis does not occur exclusively because of staging [12, 38]. Therefore, physical and mental aspects may interfere with QoL [27].
The present study found QoL levels that were below the cutoff values in the following domains: vitality, general health, pain, and mental health. These results are consistent with studies from other countries, such as Austria [39] and Sweden [40], which used the SF-36, and the literature review of Silva and Marqui [29]. The reduced scores in these domains deserve attention because it indicates that individuals tended to feel tired most of the time; evaluated their personal health as precarious; experienced pain that was severe and limiting; and felt the presence of a constant feeling of nervousness, anxiety, stress, and depression [41, 42].
Finally, the present research was carried out in a reference center that specialized in endometriosis and infertility, which explains the high number of women with grade III/IV (75.5%). The present study’s generalizations are limited by aspects such as the numerical differences between the groups of endometriosis that were compared; limited number of participants in the subgroups of symptoms of endometriosis and profiles of the participants; the use of a single reference center to perform the research characterizing a convenience sample; not investigating coexisting autoimmune disease; and studying a population with endometriosis and infertility. However, this study has the following strengths: a precise examination of the population with endometriosis and infertility; confirmation of endometriosis staging by laparoscopy; the use of an internationally validated scale for QoL; and electronic medical records collected by a gynecologist specialized in endometriosis and infertility (third author).
Conclusion
The present study demonstrated that the clinical manifestations of endometriosis such as dyspareunia and pain, interfered with the QoL levels, whereas the stages of endometriosis did not interfere. These findings indicate that the participants’ perception of endometriosis and infertility are aspects that should be considered in health care, since the loss of QoL would not depend directly on the staging of the disease but on how the participants perceive it.
Availability of data and materials
The all datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ANOVA:
-
Analysis of variance
- ASRM:
-
American Society of Reproductive Medicine
- IFF:
-
Instituto Ideia Fértil
- IQR:
-
Interquartile Ranges
- QoL:
-
Quality of Life
- SD:
-
Standard Deviation
- SF-36:
-
Short-Form Health Survey
- SPSS:
-
Statistical Package for the Social Sciences
- STROBE:
-
Strengthening the Reporting of Observational studies in Epidemiology
References
Fourquet J, Baez L, Figueroa M, Iriarte RI, Flores I. Quantification of the impact of endometriosis symptoms on health-related quality of life and work productivity. Fertil Steril. 2011;96(1):107–12.
Giudice LC, Kao LC. Endometriosis. Lancet. 2004;364(9447):1789–99.
Zhu X, Hamilton KD, McNicol ED. Acupuncture for pain in endometriosis. Sao Paulo Med J. 2013;131(6):439.
Lagana AS, Garzon S, Gotte M, Vigano P, Franchi M, Ghezzi F, et al. The Pathogenesis of Endometriosis: molecular and cell biology insights. Int J Mol Sci. 2019;20(22):5615.
Afors K, Murtada R, Centini G, Fernandes R, Meza C, Castellano J, et al. Employing laparoscopic surgery for endometriosis. Womens Health (Lond). 2014;10(4):431–43.
Vitale SG, La Rosa VL, Rapisarda AMC, Lagana AS. Impact of endometriosis on quality of life and psychological well-being. J Psychosom Obstet Gynaecol. 2017;38(4):317–9.
Rodrigues PSC, da Silva TASM, de Melo M. Endometriose–importância do diagnóstico precoce e atuação da enfermagem para o desfecho do tratamento. Revista Pró-univerSUS. 2015;6(1):13–6.
Moradi M, Parker M, Sneddon A, Lopez V, Ellwood D. Impact of endometriosis on women’s lives: a qualitative study. BMC Womens Health. 2014;14(123):1–12.
Spigolon DN, Amaral VF, Barra CMCM. Endometriose: impacto econômico e suas perspectivas. Femina. 2012;40(3):129–34.
Lagana AS, Condemi I, Retto G, Muscatello MR, Bruno A, Zoccali RA, et al. Analysis of psychopathological comorbidity behind the common symptoms and signs of endometriosis. Eur J Obstet Gynecol Reprod Biol. 2015;194:30–3.
Vitale SG, Petrosino B, La Rosa VL, Rapisarda AM, Lagana AS. A systematic review of the association between psychiatric disturbances and endometriosis. J Obstet Gynaecol Can. 2016;38(12):1079–80.
Lagana AS, La Rosa VL, Rapisarda AMC, Valenti G, Sapia F, Chiofalo B, et al. Anxiety and depression in patients with endometriosis: impact and management challenges. Int J Womens Health. 2017;9:323–30.
Weir E, Mustard C, Cohen M, Kung R. Endometriosis: what is the risk of hospital admission, readmission, and major surgical intervention? J Minim Invasive Gynecol. 2005;12(6):486–93.
Szpak R, Bugala-Szpak J, Drosdzol A, Skrzypulec V. Health-related quality of life in women with endometriosis. Wiadomosci Lekarskie. 2009;62(2):129–34.
Minson FP, Abrao MS, Sarda Junior J, Kraychete DC, Podgaec S, Assis FD. Importance of quality of life assessment in patients with endometriosis. Rev Bras Ginecol Obstet. 2012;34(1):11–5.
Parazzini F, Esposito G, Tozzi L, Noli S, Bianchi S. Epidemiology of endometriosis and its comorbidities. Eur J Obstet Gynecol Reprod Biol. 2017;209:3–7.
Muse KN, Wilson EA. How does mild endometriosis cause infertility? Fertil Steril. 1982;38(2):145–52.
D'Hooghe TM, Debrock S, Hill JA, Meuleman C. Endometriosis and subfertility: is the relationship resolved? Semin Reprod Med. 2003;21(2):243–54.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–8.
Ware Junior JE. Comments on the use of health status assessment in clinical settings. Med Care. 1992;30(5, supplement):MS205–MS9.
Ciconelli RM, Ferraz MB, Santos W, Meinão I, Quaresma MR. Tradução para língua portuguesa e validação do questionário genérico de avaliação de qualidade de vida SF-36 (Brasil SF-36). Rev Bras Reumatol. 1999;39:143–50.
Stull DE, Wasiak R, Kreif N, Raluy M, Colligs A, Seitz C, et al. Validation of the SF-36 in patients with endometriosis. Qual Life Res. 2014;23(1):103–17.
Marqui ABT. Uso de questionários para avaliação da qualidade de vida em Endometriose. Rev Bras Qual Vida. 2014;6(2):104–14.
Ashraf DM, Ali D, Azadeh DM. Effect of infertility on the quality of life, a cross- sectional study. J Clin Diagn Res. 2014;8(10):Oc13–5.
Porto BT, Ribeiro HS, Galvao MA, Sekula VG, Aldrigui JM, Ribeiro PA. Histological classification and quality of life in women with endometriosis. Rev Bras Ginecol Obstet. 2015;37(2):87–93.
Caruso S, Iraci M, Cianci S, Casella E, Fava V, Cianci A. Quality of life and sexual function of women affected by endometriosis-associated pelvic pain when treated with dienogest. J Endocrinol. 2015;38(11):1211–8.
da Cunha Araújo RS, Ribeiro HS, Sekula VG, da Costa Porto BT, Ribeiro PA. Long-term outcomes on quality of life in women submitted to laparoscopic treatment for bowel endometriosis. J Minim Invasive Gynecol. 2014;21(4):682–8.
Vitale SG, La Rosa VL, Rapisarda AMC, Laganà AS. Endometriosis and infertility: the impact on quality of life and mental health. J Endometr Pelvic Pain Disord. 2017;9(2):112–5.
Silva MPC, Marqui ABT. Qualidade de vida em pacientes com endometriose: um estudo de revisão. Rev Bras Promoç Saúde. 2014;27(3):413–21.
Bieleman HJ, Reneman MF, van Ittersum MW, van der Schans CP, Groothoff JW, Oosterveld FG. Self-reported functional status as predictor of observed functional capacity in subjects with early osteoarthritis of the hip and knee: a diagnostic study in the CHECK cohort. J Occup Rehabil. 2009;19(4):345–53.
Canis M, Donnez JG, Guzick DS, Halme JK, Rock JA, Schenken RS, Vernon MW. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril. 1997;67(5):817–21.
Sorensen J, Bautista KE, Lamvu G, Feranec J. Evaluation and treatment of female sexual pain: a clinical review. Cureus. 2018;10(3):e2379.
Casu G, Ulivi G, Zaia V, Martins MD, Barbosa CP, Gremigni P. Spirituality, infertility-related stress, and quality of life in Brazilian infertile couples: Analysis using the actor-partner interdependence mediation model. Res Nurs Health. 2018;41:156–65.
Wu MH, Su PF, Chu WY, Lin CW, Huey NG, Lin CY, et al. Quality of life among infertile women with endometriosis undergoing IVF treatment and their pregnancy outcomes. J Psychosom Obstet Gynaecol. 2020;28:1–10.
São Bento PA, Moreira MC. The experience of illness of women with endometriosis: narratives about institutional violence. Ciênc Saúde Coletiva. 2017;22(9):3023–32.
González-Echevarría AM, Rosario E, Acevedo S, Flores I. Impact of coping strategies on quality of life of adolescents and young women with endometriosis. J Psychosom Obstet Gynecol. 2018;40:1–8.
Sansone A, De Rosa N, Giampaolino P, Guida M, Lagana AS, Di Carlo C. Effects of etonogestrel implant on quality of life, sexual function, and pelvic pain in women suffering from endometriosis: results from a multicenter, prospective, observational study. Arch Gynecol Obstet. 2018;298(4):731–6.
Montanari G, Di Donato N, Benfenati A, Giovanardi G, Zannoni L, Vicenzi C, et al. Women with deep infiltrating endometriosis: sexual satisfaction, desire, orgasm, and pelvic problem interference with sex. J Sex Med. 2013;10(6):1559–66.
Friedl F, Riedl D, Fessler S, Wildt L, Walter M, Richter R, et al. Impact of endometriosis on quality of life, anxiety, and depression: an Austrian perspective. Arch Gynecol Obstet. 2015;292(6):1393–9.
Lovkvist L, Bostrom P, Edlund M, Olovsson M. Age-related differences in quality of life in Swedish women with endometriosis. J Womens Health (Larchmt). 2016;25(6):646–53.
Yong PJ, Williams C, Yosef A, Wong F, Bedaiwy MA, Lisonkova S, et al. Anatomic sites and associated clinical factors for deep dyspareunia. Sex Med. 2017;5(3):e184–e95.
Brasil DL, Montagna E, Trevisan CM, La Rosa VL, Laganà AS, Barbosa CP, et al. Psychological stress levels in women with endometriosis: systematic review and meta-analysis of observational studies. Minerva Med. 2019;111:90–102.
Acknowledgments
The authors thank the Instituto Ideia Fértil de Saúde Reprodutiva and the patients who participated in this study.
Funding
Fundação de Amparo à Pesquisa do Estado de São Paulo - FAPESP#2020/07948-3.
Author information
Authors and Affiliations
Contributions
VZ, CPB, FLV and MPFR participated in the study design. VZ and MPFR contributed to the writing the article. VZ, FLV, CPB and ASBM contributed to the review of the article. VZ, LSP and LVAS participated in the statistical analyses and contributed to the description of the results. MPFR and ASBM participated in data collection. VZ, FLV and ASBM contributed to data interpretation. All authors read and approved the final version of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The research was approved by the Research Ethics Committee of Faculdade de Medicina do ABC (located at Avenida Lauro Gomes, 2000, Vila Sacadura Cabral - Santo André - SP, 09060–870, Brazil), number: 999.295 of March 25, 2015. All participants of the present study were informed about the procedures to be performed and read, accepted and signed the Consent and Post-consent Term.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pessoa de Farias Rodrigues, M., Lima Vilarino, F., de Souza Barbeiro Munhoz, A. et al. Clinical aspects and the quality of life among women with endometriosis and infertility: a cross-sectional study. BMC Women's Health 20, 124 (2020). https://doi.org/10.1186/s12905-020-00987-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-020-00987-7