
Abstract
Background
Access to palliative care is an emerging global public health challenge. In Chile, a palliative care law was recently enacted to extend palliative care coverage to the non-oncologic population. Thus, a reliable and legitimate estimate of the demand for palliative care is needed for proper health policy planning.
Objective
To estimate the demand for Palliative Care in Chile.
Methodology
Diseases likely to require palliative care were identified according to literature and expert judgement. Annual deaths of diseases identified were estimated for the periods 2018–2020. Demand estimation corresponds to the identification of the proportion of deceased patients requiring palliative care based on the burden of severe health-related suffering. Finally, patient-years were estimated based on the expected survival adjustment.
Results
The estimated demand for palliative care varies between 25,650 and 21,679 patients depending on the approximation used. In terms of annual demand, this varies between 1,442 and 10,964 patient-years. The estimated need has a minor variation between 2018 and 2019 of 0.85% on average, while 2020 shows a slightly higher decrease (7.26%).
Conclusion
This is a replicable method for estimating the demand of palliative care in other jurisdictions. Future studies could approach the demand based on the decedent population and living one for a more precise estimation and better-informed health planning. It is hoped that our methodological approach will serve as an input for implementing the palliative care law in Chile, and as an example of estimating the demand for palliative care in other jurisdictions.
Similar content being viewed by others


Background
Palliative care (PC) is the active total care of patients whose disease does not respond to curative treatment. PC aims to achieve the best possible quality of life for patients and their families [1]. World Health Organization (WHO) emphasizes that PC is a component of universal health coverage, integrated into the Sustainable Development Goals. [2,3,4].
PC is not only designed for patients with end-stage cancer but also for people suffering from non-oncological diseases from stages before the so-called end-of-life stage [5]. PC is focused on those patients who experience severe health-related suffering (SHS), that is when the suffering produced by an injury or illness cannot be alleviated without the intervention of a professional and when it compromises physical, social, spiritual, and/or emotional functioning [6]. Thus, people suffering from a disease with SHS can benefit from PC, which not only contemplate therapies focused on managing the pathology, but also those actions and research-oriented to understand and manage ─ more efficiently ─ the distressing clinical complications suffered by these patients [7].
Access to PC is an emerging challenge for global public health. Patients with diseases that require end-of-life PC experience a significant economic burden [8]. Several studies have reported that the costs related to end-of-life care represent around 25–30% of insurer medical expenditures [9,10,11]. In addition, there is a relevant cost component related to patient care that is incurred by society. [12,13,14]. Thus, access to PC in the coverage schemes should be prioritized because the evidence supports that this health service alleviates the suffering of patients, families, and saves money for healthcare systems and society [15,16,17]. Moreover, annually more than 61 million people worldwide experience about 6 billion days of SHS that can be potentially alleviated with access to a PC [18]. Regarding the need for PC, it is estimated that by 2060, 47% of worldwide deaths will experience a high SHS burden, potentially requiring PC [19].
Chile has made progress in providing access to PC since the implementation of the Explicit Health Guarantees (GES) regime, which included access to a set of PC services for cancer patients [20]. Although this is an important achievement, there is still a need to promote interdisciplinary management, provide continuous care with good quality home assistance and extend its coverage to non-oncologic diseases. [21].
According to the Global Atlas of Palliative Care report, around 30% of the population requiring PC are patients with malignant neoplasms [9]. In the Chilean settings, the latter reveals a major gap in terms of access to PC, with a significant fraction of the target population (around 70% of patients who experience SHS) excluded from the social security system. Regarding the distributional consequences of the lack of access, this is more detrimental to patients with low socioeconomic status, since they tend to have greater barriers to access to health care, and therefore, to PC [22]. In addition, the demand for non-oncological PC may be increasing by demographic and epidemiological changes that result in a high incidence of complications of chronic diseases. [9, 23, 24].
However, in the context of a new palliative care law which was recently launched in Chile [25], PC services will be expanded to patients with non-oncologic diseases. For this purpose, the local authority required a precise estimate of the resources needed to provide them to the healthcare sector adequately. Although some efforts have been made to develop estimates of the population in need of PC [6, 7, 19, 26,27,28,29,30,31,32]; none of them has reached the technical robustness and legitimacy to support the national health policy. This report is the result of the collaboration between the Ministry of Health of Chile (MoH) and the technical group of Health Technology Assessment at Pontificia Universidad Católica de Chile, to generate a validated methodology and a reliable estimate of the demand for PC in Chile.
Methodology
To estimate the need for PC, we considered the aim of the law project proposed by the Chilean Ministry of health, which is to provide PC coverage in the last year of life through domiciliary care. Thus, a retrospective approach was used based on annual death records. This approach assumes that the number of people needing palliative care during the year represents those who finally died during the same period. This approach is considered adequate in those cases where palliative care services are focused on providing end-of-life care [6, 28, 31], which is precisely the purpose of the present study.
The estimation of the need for PC was carried out according to the following steps: (1) Identification of the diseases susceptible to receiving non-oncological PC; (2) Estimation of the annual deaths whose cause corresponds to the group of diseases identified; (3) Estimation of the proportion of deceased patients for each disease that will require palliative care; (4) Estimation of the number of patient-years based on the expected survival adjustment.
Identification of diseases susceptible to receiving non-oncologic palliative care
There are several sources related to the identification of diseases susceptible to receiving PC. Three different approaches were considered to explore those variations for the identification of diseases susceptible to non-oncologic PC. For the first approach, a group of diseases defined according to their ICD-10 category (International Classification of Diseases, 10th edition) were identified based on the proposal of Murtagh et al.[28] and the Lancet Commission report [6], which included a larger number of diseases. In addition, we validated this list with local clinical experts (a physician specializing in PC with more than ten years of clinical expertise, academic training in this field and advisor experience to the Health Ministry in PC policies), which led to the incorporation some additional codes. Oncologic pathologies were discarded, but the code for specific neoplasms associated with HIV.
For the second approach, we restricted the set of diseases identified in the first approach excluding those, according to expert judgment, who have a low probability of utilization of PC for end-of-life care. They included HIV-related infectious diseases, acute life-threatening diseases such as acute myocardial infarction, pulmonary embolism, acute pericarditis, acute myocarditis, acute renal failure, or infectious diseases of the respiratory system. The main assumption is that the patient suffering any of these conditions as the cause of death and diagnosed close to the date of death, would not have been a candidate for PC before that date. Finally, for the third approach, we used the group of pathologies proposed by Murtagh et al. [28]. The groups of pathologies to be considered for each approach, together with the ICD-10 codes, are presented in Table 1.
Estimate of annual deaths
Data on the number and causes of death were obtained from the Department of Health Statistics and Information of the MoH which is publicly available [33]. This provides cause of death data for each fatality in Chile and other demographic details. These data were filtered according to the cause of death for 2018–2020 and by month.
Estimate the proportion of deceased patients for each disease receiving palliative care
To estimate the proportion of deceased patients receiving PC for each disease, we used the weights developed by the Lancet Commission [6]. Briefly, the expert’s commission developed a multiplier that informs the proportion of people from each health condition experiencing SHS [6] and hence who required PC. For those pathologies not considered by the Lancet Commission, similarities were discussed with clinical experts to match each code in order to provide an equal proportion of palliative care needs [6]. Supplementary Table 1 reports the proportion of patients who will require PC for each pathology. We applied this approach to all scenarios, including the one that considers the set of pathologies reported by Murtagh et al.
Estimation of the number of patient-years based on the expected survival adjustment
The purpose of the present study was to estimate the demand expressed as the number of patient-years. This estimate is equivalent to the expected number of patients who will require PC for a whole year. Standardization is needed because not all patients who die in a year require the same amount of PC time. While some will require a few days, others will require full-year support.
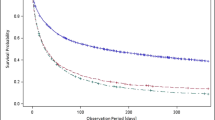
To estimate the average non-oncologic PC length of stay (LOS), similar derivation between oncologic and non-oncologic average PC LOS were assumed. This derivation was obtained from Jordan et al. [34]. This study reported an average oncologic PC LOS of 28 days and 24.27 days for non-oncologic PC LOS. Consequently, 13.3% of reduction was calculated and applied to Chilean data regarding the average oncologic PC. In addition, there is an average of 180 days of survival for cancer patients who receive PC in Chile [35]. Thus, the expected average non-oncologic average PC LOS were 156 days. This approach assumes that the hazard of death between day one and the day end of the month is constant. This value provides information for forecasting deaths and can be applied to allocating resources to palliative care.
Results
Table 2 presents the total deaths and the population that will effectively require PC according to the diseases susceptible to receiving non-oncologic PC for each one of the proposed approaches over the years 2018–2020. An average variation (considering estimates i, ii, and iii) of 0.85% is observed between the periods 2018–2019; and an average decrease of 7.26% between the periods 2019–2020. It should be noted, that for approaches (i) and (iii), about 55% of the registered deaths would require PC, whereas, for the approach (ii), the proportion is about 61%.
Regarding the expected PC LOS for non-oncologic diseases, Table 3 reports the total PC LOS expected by the three estimates. It is shown a minimum of 526,149 days and a maximum of 4,001,950 days. Moreover, it is expected between 1,442 and 10,964 patient-years when standardization is applied.
Discussion
The present study estimated the expected number of patients who need PC in one year in Chile, evaluating different scenarios. Estimates range from 12,825 to 10,839 patient-years, with a minor variation between 2018 and 2019 of 0.85% on average, and a more significant decrease in 2020 (7.26%). The variation in the need for PC in the 2020 period could be explained by the fact that the groups of diseases considered in our estimate could be an aggravating factor for the mortality of COVID-19 [36], with this disease being the main cause of death.
This is the first estimate of the need for PC for non-oncology patients in Chile and South America. However, other studies have reported some estimates worldwide [19] [7], England [1, 37], Scotland [38], Australia [29], Germany [30], Italy [39], and Malaysia [31]. Nevertheless, different estimates used alternative methodologies and a different health conditions. In this context, alternative approaches like the one reported in this manuscript may add value because it proposes a new set of conditions that achieved consensus and legitimacy to support the demand estimates.
Some of the differences between our approach and others refer to the consideration of oncologic diseases. As mentioned above, in Chile PC for cancer is provided through a different coverage scheme (20). Regarding non-oncologic PC, through the weights revealed by the Lancet Commission, which inform the fraction of individuals who will require PC by illness, based on SHS, our approach could be considered more refined in terms of demand estimation [6, 9]. Most studies assumed that all patients who will die from PC-susceptible disease will receive such care, because this does not hold for all patients, an overestimation of the actual demand will occur [27, 28, 37].
Although Etkind et al. attempt to address this issue by introducing pain prevalence in their estimates, the results of the present work can be understood as more accurate because the use of the SHS encompasses the requirement for PC in more dimensions than pain, and because we considered a more individualized PC requirement weight. In contrast, Etkind et al. considered an expected pain prevalence by disease groups (organ failure, dementia, and others) that might ignore within-group heterogeneity [1].
Our estimation also considered the PC LOS needed. This information is relevant as it allows us to make a more precise estimate of the expected annual demand. Thus, the range of total expected PC LOS was estimated between 1,442 and 10,964 patient year depending on the set of assumptions made.
The results obtained allow us to identify the first challenges of implementing PC at the primary health care level. This is of utmost importance as primary health care has an essential role to play in the fight against health inequities. Integrating non-oncological PC into primary health care could help to reduce these inequalities, something that specialist palliative care teams have not been able to achieve [40].
Our estimates have some limitations, the data are collected according to death registries, which may be underreported. This may occur with diseases such as dementia or Parkinson’s disease, which lack of registry may impact underestimating the need for PC [28, 41,42,43]. Also, as our estimate is based on the diagnosis of the first cause of death, the need for PC may be underestimated because of comorbidities that could increase its demand [19, 44, 45]. Furthermore, although we used the weights validated by both the Lancet Commission expert panel and our experts (for those conditions not included in the Lancet Commission), they are not precise estimates and should be validated in future research [19]. Additionally, our non-oncologic PC LOS estimation lacks local reliable data. The assumptions made may not reflect the average non-oncologic PC LOS despite the discussion with clinical expert. Therefore, new registers are needed in order to make more accurate estimate.
Other methods of estimating PC demand have been reported [6, 32, 46, 47]. The Lancet Commission develops a robust estimate based on the deceased considering that population in their last year of life, and of the non-deceased, considering PC requirements before the last year of life [6, 9]. To undertake the above approximation, prevalence data are required for all disease groups considered in the methodology, which is a major challenge for future research. In addition, given that the estimate of the present study is within the context of a future law on non-oncological PCs, this estimate is plausible since the law considers, in the first place, PCs in the last six months of life.
Estimating the demand for PC is a key resource for the planning of health policies that take care of the lack of access to PC. Coverage of diseases requiring PC care needs to increase over time, as health policies for non-oncological PC provision have the potential to alleviate the suffering of a large proportion of patients and their families. It is hoped that this estimate will allow accounting for the relevance of addressing this public health problem to organize patient-centred PC provision, improve coordination of healthcare, and thus strengthen the public health system by ensuring equity in access to PC.
Availability of data and materials
This paper reports an analysis of publicly available summary data on mortality. The datasets supporting the conclusions of this article is available in the Department of Health Statistics and Information of the Ministry of Health of Chile repository as follow: Mortality data: https://deis.minsal.cl/#datosabiertos Accessed June 2021.
Abbreviations
- PC:
-
Palliative Care
- WHO:
-
World Health Organization
- SHS:
-
Health-related suffering
- GES:
-
Explicit Health Guarantees
- MoH:
-
Ministry of Health of Chile
- ICD-10:
-
International Classification of Diseases 10th edition
References
Etkind SN, Bone AE, Gomes B, Lovell N, Evans CJ, Higginson IJ, et al. How many people will need palliative care in 2040? Past trends, future projections and implications for services. BMC Med. 2017;15(1):102.
World Health Organization. Universal health coverage (UHC) 2021. Available at: https://www.who.int/news-room/factsheets/detail/universal-health-coverage-(uhc). Accessed 10 Aug 2021.
World health statistics 2018: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO.
World health statistics 2021: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
Radbruch L, De Lima L, Knaul F, Wenk R, Ali Z, Bhatnaghar S, et al. Redefining palliative care-a new consensus-based definition. J Pain Symptom Manag. 2020;60(4):754–64.
Knaul FM, Farmer PE, Krakauer EL, De Lima L, Bhadelia A, Jiang Kwete X, et al. Alleviating the access abyss in palliative care and pain relief-an imperative of universal health coverage: the Lancet Commission report. Lancet (London England). 2018;391(10128):1391–454.
Morin L, Aubry R, Frova L, Macleod R, Wilson DM, Loucka M, et al. Estimating the need for palliative care at the population level: a cross-national study in 12 countries. Palliat Med. 2017;31(6):526–36.
Dzingina MD, Higginson IJ. Public health and palliative care in 2015. Clin Geriatr Med. 2015;31(2):253–63.
Worldwide Palliative Care Alliance. WHO Global Atlas of Palliative Care. 2021. Available from: http://www.thewhpca.org/resources/global-atlas-on-end-of-life-care. Accesed 18 Aug 2021.
Campbell DE, Lynn J, Louis TA, Shugarman LR. Medicare program expenditures associated with hospice use. Ann Intern Med. 2004;140(4):269–77.
Lubitz JD, Riley GF. Trends in Medicare payments in the Last Year of Life. N Engl J Med. 1993;328(15):1092–6.
Gott M, Allen R, Moeke-Maxwell T, Gardiner C, Robinson J. ‘No matter what the cost’: a qualitative study of the financial costs faced by family and whānau caregivers within a palliative care context. Palliat Med. 2015;29(6):518–28.
Haltia O, Färkkilä N, Roine RP, Sintonen H, Taari K, Hänninen J, et al. The indirect costs of palliative care in end-stage cancer: a real-life longitudinal register- and questionnaire-based study. Palliat Med. 2018;32(2):493–9.
Round J, Jones L, Morris S. Estimating the cost of caring for people with cancer at the end of life: a modelling study. Palliat Med. 2015;29(10):899–907.
Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-Dewan S, et al. High-quality health systems in the sustainable development goals era: time for a revolution. Lancet Global Health. 2018;6(11):e1196–252.
Chalkidou K, Marquez P, Dhillon PK, Teerawattananon Y, Anothaisintawee T, Gadelha CA, et al. Evidence-informed frameworks for cost-effective cancer care and prevention in low, middle, and high-income countries. Lancet Oncol. 2014;15(3):e119-31.
Smith S, Brick A, O’Hara S, Normand C. Evidence on the cost and cost-effectiveness of palliative care: a literature review. Palliat Med. 2014;28(2):130–50.
Bhadelia A, De Lima L, Arreola-Ornelas H, Kwete XJ, Rodriguez NM, Knaul FM. Solving the global crisis in access to pain relief: lessons from country actions. Am J Public Health. 2019;109(1):58–60.
Sleeman KE, De Brito M, Etkind S, Nkhoma K, Guo P, Higginson IJ, et al. The escalating global burden of serious health-related suffering: projections to 2060 by world regions, age groups, and health conditions. Lancet Global Health. 2019;7(7):e883–92.
MINSAL. AUGE 85. Listado específico de prestaciones. Ministerio de Salud de Chile. Available at: https://auge.minsal.cl/problemasdesalud/lep. Accessed 10 Oct 2021.
Del Río MI, Palma, AJBedmu. Pontificia universidad católica de Chile. Cuidados Paliativos: Historia y Desarrollo. 2007;32(1):16–22.
Moine S, Murray SA, Boyd K, Engels Y, Mitchell G. Palliative care and the endless cycle of serious health-related suffering. Lancet. 2018;392(10146):471–2.
Albala C. EL envejecimiento de la Población Chilena Y los desafíos para la salud y el bienestar de las personas mayores. Revista Médica Clínica Las Condes. 2020;31(1):7–12.
Martínez-Sanguinetti MA, Leiva-Ordoñez AM, Petermann-Rocha F, Celis-Morales C. Cómo ha cambiado el perfil epidemiológico en Chile en los últimos 10 años? Revista Médica Chile. 2021;149(1):149–52.
Senado. A Sala proyecto que entrega cuidados paliativos a enfermos terminales. Available at: https://www.senado.cl/noticias/eutanasia/a-sala-proyecto-que-entrega-cuidados-paliativos-a-enfermos-terminales. Accessed 10 Aug 2021.
Higginson IJ, Hart S, Koffman J, Selman L, Harding R. Needs assessments in palliative care: an appraisal of definitions and approaches used. J Pain Symptom Manag. 2007;33(5):500–5.
Kane PM, Daveson BA, Ryan K, McQuillan R, Higginson IJ, Murtagh FEM. The need for palliative care in Ireland: a population-based estimate of palliative care using routine mortality data, inclusive of nonmalignant conditions. J Pain Symptom Manag. 2015;49(4):726-33.e1.
Murtagh FE, Bausewein C, Verne J, Groeneveld EI, Kaloki YE, Higginson IJ. How many people need palliative care? A study developing and comparing methods for population-based estimates. Palliat Med. 2014;28(1):49–58.
Rosenwax LK, McNamara B, Blackmore AM, Holman CD. Estimating the size of a potential palliative care population. Palliat Med. 2005;19(7):556–62.
Scholten N, Günther AL, Pfaff H, Karbach U. The size of the population potentially in need of palliative care in Germany - an estimation based on death registration data. BMC Palliat Care. 2016;15(1):26.
Yang SL, Woon YL, Teoh CCO, Leong CT, Lim RBL. Adult palliative care 2004–2030 population study: estimates and projections in Malaysia. BMJ Supportive Palliat Care. 2020;12:e129.
Gómez-Batiste X, Martínez-Muñoz M, Blay C, Espinosa J, Contel JC, Ledesma A. Identifying needs and improving palliative care of chronically ill patients: a community-oriented, population-based, public-health approach. Curr Opin Support Palliat Care. 2012;6(3):371–8.
DEIS. Defunciones por causa de muerte 2016–2021 (Actualización semanal): Departamento de Estadística e Información en Salud; 2021. Available at: https://deis.minsal.cl/#datosabiertos. Accessed 22 June 2021.
Jordan RI, Allsop MJ, Elmokhallalati Y, Jackson CE, Edwards HL, Chapman EJ, et al. Duration of palliative care before death in international routine practice: a systematic review and meta-analysis. BMC Med. 2020;18(1):368.
HSJD. El ingreso precoz a cuidados paliativos de los pacientes oncológicos mejora su calidad de vida y sobrevida: Hospital San Juan de Dios - CDT Asistencial Docente; 2020. Available at: http://www.hsjd.cl/web/el-ingreso-precoz-a-cuidados-paliativos-delos-pacientes-oncologicos-mejora-su-calidad-de-vida-y-sobrevida/. Accessed 25 Oct 2022.
Singh AK, Gillies CL, Singh R, Singh A, Chudasama Y, Coles B, et al. Prevalence of co-morbidities and their association with mortality in patients with COVID -19: A systematic review and meta-analysis. Diabetes, Obes Metab. 2020;22(10):1915–24.
Jeba J, Taylor C, O’Donnell V. Projecting palliative and end-of-life care needs in Central Lancashire up to 2040: an integrated palliative care and public health approach. Public Health. 2021;195:145–51.
Finucane AM, Bone AE, Etkind S, Carr D, Meade R, Munoz-Arroyo R, et al. How many people will need palliative care in Scotland by 2040? A mixed-method study of projected palliative care need and recommendations for service delivery. BMJ Open. 2021;11(2):e041317.
Benini F, Bellentani M, Reali L, Lazzarin P, De Zen L, Pellegatta F, et al. An estimation of the number of children requiring pediatric palliative care in Italy. Italian J Pediatr. 2021;47(1):4.
Murray SA, Kendall M, Mitchell G, Moine S, Amblàs-Novellas J, Boyd K. Palliative care from diagnosis to death. BMJ. 2017;356:j878.
Burger EH, Groenewald P, Bradshaw D, Ward AM, Yudkin PL, Volmink J. Validation study of cause of death statistics in Cape Town, South Africa, found poor agreement. J Clin Epidemiol. 2012;65(3):309–16.
Harteloh P, De Bruin K, Kardaun J. The reliability of cause-of-death coding in the Netherlands. Eur J Epidemiol. 2010;25(8):531–8.
Lloyd-Jones DM, Martin DO, Larson MG, Levy D. Accuracy of death certificates for coding coronary heart disease as the cause of death. Ann Intern Med. 1998;129(12):1020–6.
Stirland LE, González-Saavedra L, Mullin DS, Ritchie CW, Muniz-Terrera G, Russ TC. Measuring multimorbidity beyond counting diseases: systematic review of community and population studies and guide to index choice. BMJ. 2020;368:160.
McIlfatrick S. Assessing palliative care needs: views of patients, informal carers and healthcare professionals. J Adv Nurs. 2007;57(1):77–86.
Howard M, Hafid A, Isenberg SR, Hsu AT, Scott M, Conen K, et al. Intensity of outpatient physician care in the last year of life: a population-based retrospective descriptive study. CMAJ Open. 2021;9(2):E613-E22.
Kaur S, Kaur H, Komal K, Kaur P, Kaur D, Jariyal VL, et al. Need of palliative care services in rural area of Northern India. Indian J Palliat Care. 2020;26(4):528–30.
Acknowledgements
To the Department of Health Statistics and Information of the Ministry of Health who provided the data for this work timely. To the former Minister of Health Dr Enrique Paris and the Dean of the Faculty of Medicine, Pontificia Universidad Católica de Chile, Dr. Felipe Heusser who promoted this collaborative work facilitating the time and interaction of researchers with colleagues in the MoH. To Dr Pedro Perez, from Pontificia Universidad Católica de Chile, for sharing his expertise in this work.
Funding
The present study was performed without funding.
Author information
Authors and Affiliations
Contributions
NA contributed to analysis, protocol development, interpretation, drafting and approved the final draft. TA contributed to analysis, interpretation, drafting and approved the final draft. ME contributed to analysis development, protocol development, expertise in projections methodology, interpretation, drafting and approved the final draft. XN contributed to analysis and approved the final draft. CB contributed to oversight of analysis and drafting and approved the final draft. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations. Experimental protocols and informed consent were not applicable since analysis were carried out from public data set available in the Department of Health Statistics and Information of the Ministry of Health of Chile repository.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests for this study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
The estimated proportion of decedents requiringpalliative care (PC).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Armijo, N., Abbot, T., Espinoza, M. et al. Estimation of the demand for palliative care in non-oncologic patients in Chile. BMC Palliat Care 22, 5 (2023). https://doi.org/10.1186/s12904-022-01122-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12904-022-01122-z