
Abstract
Objectives
To assess the accuracy of implant placement in models and satisfaction in dynamic navigation assisted postgraduate dental students training.
Methods
Postgraduate dental students who had at least one year of dental clinical practice with no experience in dental implant surgeries were included. Students were instructed to make treatment plans in the dynamic navigation system. Each student placed two maxillary right incisors, using freehand approach at first and then under dynamic navigation. The implant position was compared with treatment plan. Factors influencing the accuracy of implants placed under dynamic navigation were analyzed. Student acceptance towards the training and use of dynamic navigation was recorded using a questionnaire.
Results
A total of 21 students placed 42 implants. For freehand implant placement, the median entry point deviation, apex point deviation, and implant axis deviation was 3.79 mm, 4.32 mm, and 10.08°. For dynamic guided implant placement, the median entry point deviation, apex point deviation, and implant axis deviation was 1.29 mm, 1.25 mm, and 4.89° (p < 0.001). The accuracy of dynamic guided implant was not influenced by student gender or familiarity with computer games. All students were satisfied with the training.
Conclusions
Dynamic navigation system assisted students in improving the accuracy of implant placement and was well accepted by students.
Similar content being viewed by others


Introduction
Tooth loss is prevalent in the world, having a negative impact on the well-being of hundreds of millions of people [1, 2]. Dental implants have become a common method of rehabilitating missing teeth. An increasing number of well-trained clinicians performing implant surgeries is required to meet the needs of patients.
Training in surgical procedures is a major part of education in implant dentistry. Students should be trained to have competence in designing a prosthesis-guided implant position and being familiar with surgical procedures. However, current education in implant dentistry mainly focuses on theory [3]. According to previous surveys, only 5% of students operated on patients in clinical practice in Europe [4] and students had an average of 0.61 surgical cases in America [5]. Lack of surgical skill training in implant dentistry could be attributed to a lack of staff availability/competence and suitable patients [6]. In addition, it is risky and not ethical for patients if an untrained clinician performs the surgery.
Dynamic navigation has been widely used as a method of student training in oral and maxillofacial surgery [7] and root canal treatment [8]. In implant dentistry, dynamic navigation is beneficial to improve the accuracy of implant placement [9,10,11,12] and provides an alternative to training in surgical procedures. Through dynamic navigation, students can design the three-dimensional implant position in software, visualize the implant site on a computer screen, receive real-time feedback and make adjustments, and compare the final implant position with the presurgical design. Previous studies have reported that dynamic guided navigation well-assisted students in improving the accuracy of implant placement and helped students improve their familiarity of surgical skills and confidence [13, 14]. In addition, a recent study reported that dynamic navigation improved the accuracy of implant placement by dental students [15]. However, it is unclear whether dynamic navigation is well accepted by students with totally no surgical experience in implant dentistry. Furthermore, to improve the quality of student training, factors influencing the accuracy of dynamic guided navigation surgeries performed by students should be explored.
Thus, in the present study, postgraduate dental students with no surgical experience were instructed to place two implants, using a freehand approach and under dynamic navigation. The accuracy of implant position using the two approaches was compared to evaluate the benefit of dynamic navigation in surgery training. In addition, factors influencing the accuracy of dynamic guided navigation surgery were investigated.
Materials and methods
The study protocol was approved by the institutional review board of the Hospital of Stomatology, Wuhan University (No. 2022[B18]). Postgraduate students who had at least one year of dental clinical practice, in the Hospital of Stomatology Wuhan University, with no surgical experience in dental implant placement, and who had not participated in previous courses, were included.
Students had received courses in implant dentistry before participating in this training course. The present course emphasized implant placement surgery and digital plans. The course included a theoretical part and a practical part. The theoretical course included the biological basis for peri-implant tissue (3 h), patient examination (2 h), treatment plan protocols (3 h), digital treatment plan (3 h), as well as surgical procedures for osteotomy preparation and implant insertion (2 h). The practical course included training on digital planning in software (1 h), freehand, and dynamic navigation assisted implant placement in models (1 h). During the practical training, each student was assigned to place two implants (4.1*10 mm, Straumann, Bone level tapered implants, Switzerland) to replace the maxillary right incisor in models. In the beginning, students made treatment plans in software (Dental Implant Navigation System v2.5.1, Digital-health Care Co.Ltd., Suzhou, China) with the consultation of an experienced surgeon. Then, students were instructed to place one implant using a conventional freehand approach and place a second implant under dynamic navigation (Digital-health Care Co.Ltd., Suzhou, China).
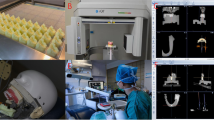
Before the training course, 3D-printed photosensitive resin maxillary models with missing right incisors were prepared (Digital-health Care Co.Ltd., Suzhou, China). The same model was used for all students. Radiopaque markers were placed on the buccal and palatal of the models, for 3D orientation of the models and subsequent superimposition. CBCT scan (NewTomVGi, Italy) of the model was taken and the DICOM file was imported into the treatment plan software. To prepare for the training, the models were stabilized onto simulation heads (Type 2 simulation head, NISSIN, Japan). The models were registered to be spatially matched to the virtual representation on screen by a single trained engineer. During osteotomy preparation, the drills were calibrated, to provide the system with information on drill position and length. The accuracy of drill position and angulation was monitored and real-time feedback was given on screen.
After implant placement, CBCT scans of all models were taken and imported into an accuracy validation software (Computer Assisted Dental Implant System v2.5.1, Digital-health Care Co.Ltd., Suzhou, China). Pre- and post-surgery CBCT was superimposed using three to five anatomy markers. The coordination of the plan and actual implants were automatically detected and manually checked. The positional deviation of the plan and actual implants was calculated, including entry point deviation, apex point deviation, and implant axis deviation (Fig. 1). The measurement was performed by one calibrated researcher (with an ICC of 0.97).

Measurement of the accuracy of implant placement. a implant coronal plane; b implant sagittal plane; c implant axial plane
After the course, students were asked to finish a questionnaire, including students’ attitudes towards the content and atmosphere of the courses, application of dynamic navigation, interest in future study, as well as overall satisfaction [14, 16,17,18,19]. The degree of satisfaction was ranked using a Likert scale, including “strongly satisfied,” “satisfied,” “neither satisfied nor unsatisfied,” “unsatisfied,” and “strongly unsatisfied” [20].
SPSS 25.0 (IBM Corp, United States) was used for data analysis. Shapiro–Wilk test indicated that the deviation of implant position did not follow the normal distribution. The median and interquartile range were used for descriptive data. Wilcoxon matched-pairs signed rank sum test was used to compare the accuracy of implant placement using a freehand approach and under dynamic navigation. To explore factors associated with the accuracy of implant placement under dynamic navigation, the Mann–Whitney U test was used. Potential factors included student gender and whether they were familiar with computer games (familiar vs, not familiar). P < 0.05 was considered statistically significant.
Results
A total of 21 postgraduate students were enrolled, of which 13 (61.9%) were females, six (28.6%) majored in implant dentistry, 17 (81.0%) spent at least two years in dental clinical practice, and nine (42.9%) reported they were familiar with computer games.
The accuracy of implant placement is listed in Table 1. Compared with treatment plan, the median (interquartile range) entry point deviation, apex point deviation, and implant axis deviation of freehand implant placement were 3.79 (2.80, 4.60) mm, 4.32 (3.23, 5.14) mm, and 10.08 (7.35, 14.99) °. The median (interquartile range) entry point deviation, apex point deviation, and implant axis deviation of dynamic guided implant placement were 1.29 (1.08, 2.00) mm, 1.25 (1.02, 1.65) mm, and 4.89 (2.27, 6.80) °. The deviation of dynamic navigation was significantly less than the freehand approach. No factor was found significantly associated with the accuracy of implant placement under dynamic navigation or freehand surgery (Table 2).
Student acceptance towards the training course is shown in Table 3. For all items, no student reported “unsatisfied” or “strongly unsatisfied”. All students were satisfied with the training interest and perspective. A majority of students showed positive attitudes towards the content and atmosphere of the training. More than 90% of the students were willing to participate in future training. Overall, all students were satisfied with the dynamic guided implant placement training.
A post hoc sample size calculation was performed to verify the results. The superiority by margin tests for the difference between two means in PASS (15.0) were used, with α = 0.01, and power = 0.8. Accuracy at entry point, apex point, and angular deviation were used. Six, 6, and 13 implants in each group were needed to detect differences regarding accuracy at the entry point, apex point, and angular deviation.
Discussion
The present study compared the accuracy of dental implant placement by postgraduate students using a freehand approach or dynamic navigation. Dynamic navigation significantly improved the accuracy of dental implants placed by students with no surgery experience, and was well accepted by students. The results indicated that dynamic navigation could be successfully used in surgery training of implant placement for dental students, regardless of gender or familiarity with computer games.
In the present study, the accuracy of implant placement by students improved significantly after using dynamic navigation. A previous model-based study [21] reported that freehand implant placement yielded a deviation of 1.44 mm at entry points, 2.00 mm at apex points, and 9.66° for implant axis, which was smaller compared with the deviation produced by freehand implant placement in this study. It could be explained that in this study implants were placed by students with no surgery experience. However, another study [22] reported that using dynamic guided navigation surgeries in models, the mean entry point deviation, apex point deviation, and implant axis deviation were 0.91 mm, 1.21 mm, and 2.78°, respectively, which was similar to the results of the present study. It was indicated that dynamic guided navigation could help students place implants in models.
The present study did not find factors associated with the accuracy of implants placed by students using dynamic navigation. A previous study reported that computer games might be beneficial for interactive virtual guidance [23]. Because they shared the characteristics that a player/dentist looked at the screen, received real-time feedback, and operated on hand. Another study reported a slight learning advantage of dynamic guided implant placement for male students [13]. They explained that males showed learning advantages because they were more familiar with video games. However, the present study did not find significant different accuracy between students familiar or not familiar with computer games. It was indicated that dynamic navigation could improve accuracy of implant placement, regardless of the gender or familiarity with computer games.
The training using dynamic guided surgery was well accepted by students, which is similar with previous studies reporting the learning curve of dynamic navigation [24, 25]. On the one hand, the digital workflow of dental implant-supported rehabilitation is developing rapidly. It is important for the surgeons to master dynamic guided navigation surgery, treat patients with compromised clinical conditions, and broaden the indications of dental implants. On the other hand, dynamic navigation benefits students in placing dental implants accurately, which might be preferred by dental students. However, the clinical conditions are usually more complex and the accuracy of implants is only part of the success of implant-supported rehabilitation. Thus, although the dynamic navigation system could help improve the accuracy of dental implants placed by students, it could not be a substitute for clinical practices.
Results from the present study indicated that dynamic navigation was beneficial to student training in dental implant placement. Practically, the advantages of dynamic navigation in student training include visualization of implant placement procedure, better accuracy, and a smoother learning curve. However, the economic cost of student training using dynamic navigation is relatively high. Dynamic navigation is not suitable for all clinical cases. The accuracy of dynamic navigation is dependent on the accuracy of pre-surgery preparation, including registration, calibration, and the inner algorithm of the system. In the future, the development of dynamic navigation and promotion of potential augmented reality can be beneficial to further improve student training in dental implant placement.
One limitation of the present study was that all implants were placed in the maxillary right incisor and the influence of implant site on accuracy was not explored. Maxillary right incisor was chosen because implant osteotomy could be directly visualized and the complexity of surgery was reduced for students. However, the influence of implant sites and extensive edentulous ridge on the accuracy of dynamic guided implant placement has been reported in previous clinical studies or model-based studies [22, 26]. Secondly, a comparison of the accuracy of dynamic guided implant placement between experienced and inexperienced dentists was not performed, which was beyond the scope of this study and has been analyzed in previous research [27, 28]. Thirdly, students performed first freehand implant placement and then navigation assisted implant placement. The order was not randomized, which might cause bias. However, the dynamic navigation assisted implant placement required clinicians to have some experience in implant placement. The postgraduate students had no experience with surgical interventions in implant dentistry. They were asked to first perform freehand implant placement to help the students get familiar with the models and drilling procedures.
In the future, research with larger sample sizes or randomized trials is recommended, to compare the dynamic guided navigation training with conventional training. Dynamic navigation equipment with different subject generations can be investigated and explored to improve the accuracy and promote the usage of dynamic navigation in student training. In addition, it could be further explored whether dynamic guided navigation could be applied in the training of other surgical techniques, such as sinus floor elevation, immediate implant placement, or alveolar ridge augmentation.
Conclusions
The dynamic guided navigation system was successfully applied in training implant placement among dental students. The accuracy of implant placement by dental students could be improved under dynamic guided navigation, regardless of student gender or familiarity with computer games. The application of dynamic guided navigation in surgery training is well accepted by students and could be promoted in dental student education.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Bernabe E, Marcenes W, Hernandez CR, Bailey J, Abreu LG, Alipour V, Amini S, Arabloo J, Arefi Z, Arora A, Ayanore MA, Bärnighausen TW, Bijani A, Cho DY, Chu DT, Crowe CS, Demoz GT, Demsie DG, DibajiForooshani ZS, Du M, El Tantawi M, Fischer F, Folayan MO, Futran ND, Geramo YCD, Haj-Mirzaian A, Hariyani N, Hasanzadeh A, Hassanipour S, Hay SI, Hole MK, Hostiuc S, Ilic MD, James SL, Kalhor R, Kemmer L, Keramati M, Khader YS, Kisa S, Kisa A, Koyanagi A, Lalloo R, Le Nguyen Q, London SD, Manohar ND, Massenburg BB, Mathur MR, Meles HG, Mestrovic T, Mohammadian-Hafshejani A, Mohammadpourhodki R, Mokdad AH, Morrison SD, Nazari J, Nguyen TH, Nguyen CT, Nixon MR, Olagunju TO, Pakshir K, Pathak M, Rabiee N, Rafiei A, Ramezanzadeh K, Rios-Blancas MJ, Roro EM, Sabour S, Samy AM, Sawhney M, Schwendicke F, Shaahmadi F, Shaikh MA, Stein C, Tovani-Palone MR, Tran BX, Unnikrishnan B, Vu GT, Vukovic A, Warouw TSS, Zaidi Z, Zhang ZJ, Kassebaum NJ. Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017 A systematic analysis for the global burden of Disease 2017 Study. J Dent Res. 2020;99(4):362–73.
Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of severe tooth loss: a systematic review and meta-analysis. J Dent Res. 2014;93(7 Suppl):20s–8s.
Chaturvedi S, Elmahdi AE, Abdelmonem AM, Haralur SB, Alqahtani NM, Suleman G, Sharif RA, Gurumurthy V, Alfarsi MA. Predoctoral dental implant education techniques-students’ perception and attitude. J Dent Educ. 2021;85(3):392–400.
De Bruyn H, Koole S, Mattheos N, Lang NP. A survey on undergraduate implant dentistry education in Europe. Eur J Dent Educ. 2009;13(Suppl 1):3–9.
Kihara H, Sun J, Sakai M, Nagai S, Da Silva J. A survey of dental implant instruction in predoctoral dental curricula in North America. J Dent Educ. 2017;81(9):1085–90.
Koole S, De Bruyn H. Contemporary undergraduate implant dentistry education: a systematic review. Eur J Dent Educ. 2014;18(Suppl 1):11–23.
Ayoub A, Pulijala Y. The application of virtual reality and augmented reality in Oral & Maxillofacial Surgery. BMC Oral Health. 2019;19(1):238.
Torres A, Boelen GJ, Lambrechts P, Pedano MS, Jacobs R. Dynamic navigation: a laboratory study on the accuracy and potential use of guided root canal treatment. Int Endod J. 2021;54(9):1659–67.
Kaewsiri D, Panmekiate S, Subbalekha K, Mattheos N, Pimkhaokham A. The accuracy of static vs dynamic computer-assisted implant surgery in single tooth space: A randomized controlled trial. Clin Oral Implants Res. 2019;30(6):505–14.
Yimarj P, Subbalekha K, Dhanesuan K, Siriwatana K, Mattheos N, Pimkhaokham A. Comparison of the accuracy of implant position for two-implants supported fixed dental prosthesis using static and dynamic computer-assisted implant surgery: A randomized controlled clinical trial. Clin Implant Dent Relat Res. 2020;22(6):672–8.
Jorba-García A, González-Barnadas A, Camps-Font O, Figueiredo R, Valmaseda-Castellón E. Accuracy assessment of dynamic computer-aided implant placement: a systematic review and meta-analysis. Clin Oral Investig. 2021;25(5):2479–94.
Jorba-García A, Figueiredo R, González-Barnadas A, Camps-Font O, Valmaseda-Castellón E. Accuracy and the role of experience in dynamic computer guided dental implant surgery: An in-vitro study. Med Oral Patol Oral Cir Bucal. 2019;24(1):e76–83.
GolobDeeb J, Bencharit S, Carrico CK, Lukic M, Hawkins D, Rener-Sitar K, Deeb GR. Exploring training dental implant placement using computer-guided implant navigation system for predoctoral students: A pilot study. Eur J Dent Educ. 2019;23(4):415–23.
Zhan Y, Wang M, Cheng X, Li Y, Shi X, Liu F. Evaluation of a dynamic navigation system for training students in dental implant placement. J Dent Educ. 2021;85(2):120–7.
Zhong X, Xing Y, Yan J, Chen J, Chen Z, Liu Q. Surgical performance of dental students using computer-assisted dynamic navigation and freehand approaches. Eur J Dent Educ. 2024;28(2):504–10. https://doi.org/10.1111/eje.12975.
Zhang B, Li S, Gao S, Hou M, Chen H, He L, Li Y, Guo Y, Wang E, Cao R, Cheng J, Li R, Zhang K. Virtual versus jaw simulation in Oral implant education: a randomized controlled trial. BMC Med Educ. 2020;20(1):272.
Nkenke E, Vairaktaris E, Bauersachs A, Eitner S, Budach A, Knipfer C, Stelzle F. Acceptance of virtual dental implant planning software in an undergraduate curriculum: a pilot study. BMC Med Educ. 2012;12:90.
Liu L, Zhou R, Yuan S, Sun Z, Lu X, Li J, Chu F, Walmsley AD, Yan B, Wang L. Simulation training for ceramic crown preparation in the dental setting using a virtual educational system. Eur J Dent Educ. 2020;24(2):199–206.
Chae YK, Lee H, Jih MK, Lee HS, Lee JW, Kim SH, Kim GT, Choi SC, Nam OH. Validation of a three-dimensional printed model for training of surgical extraction of supernumerary teeth. Eur J Dent Educ. 2020;24(4):637–43.
Bishop PA, Herron RL. Use and Misuse of the Likert Item Responses and Other Ordinal Measures. Int J Exerc Sci. 2015;8(3):297–302.
Chen CK, Yuh DY, Huang RY, Fu E, Tsai CF, Chiang CY. Accuracy of Implant Placement with a Navigation System, a Laboratory Guide, and Freehand Drilling. Int J Oral Maxillofac Implants. 2018;33(6):1213–8.
Wei SM, Zhu Y, Wei JX, Zhang CN, Shi JY, Lai HC. Accuracy of dynamic navigation in implant surgery: A systematic review and meta-analysis. Clin Oral Implants Res. 2021;32(4):383–93.
Verdaasdonk EG, Dankelman J, Schijven MP, Lange JF, Wentink M, Stassen LP. Serious gaming and voluntary laparoscopic skills training: a multicenter study. Minim Invasive Ther Allied Technol. 2009;18(4):232–8.
Spille J, Helmstetter E, Kübel P, Weitkamp JT, Wagner J, Wieker H, Naujokat H, Flörke C, Wiltfang J, Gülses A. Learning Curve and Comparison of Dynamic Implant Placement Accuracy Using a Navigation System in Young Professionals. Dent J (Basel). 2022;10(10):187. https://doi.org/10.3390/dj10100187.
Ma L, Ye M, Wu M, Chen X, Shen S. A retrospective study of dynamic navigation system-assisted implant placement. BMC Oral Health. 2023;23(1):759.
Emery RW, Merritt SA, Lank K, Gibbs JD. Accuracy of dynamic navigation for dental implant placement-model-based evaluation. J Oral Implantol. 2016;42(5):399–405.
Cushen SE, Turkyilmaz I. Impact of operator experience on the accuracy of implant placement with stereolithographic surgical templates: an in vitro study. J Prosthet Dent. 2013;109(4):248–54.
Stefanelli LV, DeGroot BS, Lipton DI, Mandelaris GA. Accuracy of a dynamic dental implant navigation system in a private practice. Int J Oral Maxillofac Implants. 2019;34(1):205–13.
Funding
The present study received no funding.
Author information
Authors and Affiliations
Contributions
Bin Shi, Qi Yan, and Junyu Shi conceived the work; Bin Shi, Qi Yan, Xinyu Wu and Junyu Shi designed the study; Qi Yan and Xinyu Wu acquired and analyzed the data. All authors contributed to the interpretation of the data, the drafting of the report, approved the final version, and agreed to be accountable for the work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of School & Hospital of Stomatology affiliated to Wuhan University (No 2022-B18). All participants signed informed consents.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yan, Q., Wu, X., Shi, J. et al. Does dynamic navigation assisted student training improve the accuracy of dental implant placement by postgraduate dental students: an in vitro study. BMC Oral Health 24, 600 (2024). https://doi.org/10.1186/s12903-024-04324-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-024-04324-4