
Abstract
Background
Oral aphthous stomatitis is a chronic inflammatory condition. Numerous medications have been investigated to treat the symptoms of the disease. However, these days patients prefer herbal medicines due to lower side effects. Considering the anti-inflammatory, analgesic, and anti-oxidant properties of Caffeic acid and its few side effects, the aim of this study was to assess the impact of Caffeic acid on recurrent aphthous stomatitis (RAS). investigating the effect of caffeic acid mucoadhesive tablets on the size and pain intensity of the aphthous lesions.
Methods
in this double-blinded clinical trial study, 47 patients who met the inclusion criteria were selected by convenient sampling method. The patients were assigned to two groups randomly; the control group (placebo recipients) and the intervention group (Caffeic acid recipients). Patients were followed up for 7 days following the intervention. The diameter of the inflammatory lesion was measured in millimeters, and the pain intensity was recorded based on the VAS scale (Visual Analogue Scale). This trial was approved by the medical ethics committee of Mazandaran University of Medical Sciences (Ethical code: IR.MAZUMS.REC.1401.261) and received IRCT code of IRCT20220815055700N1on 03/09/2022.
Results
the diameter of the lesion in both groups decreased over time, and there was no significant difference between the intervention and control groups, except on the fifth day when the diameter of the lesion was significantly greater in the control group (P = 0.012). From the second day, the control group’s average pain intensity was significantly higher than the intervention group’s pain intensity (P < 0.05).
Conclusions
when comparing mucoadhesive tablets containing Caffeic acid and placebo, the findings demonstrated that Caffeic acid has a significant efficacy in reducing aphthous lesions’ diameter and pain intensity of the patients and are suggested for palliative oral aphthous lesions treatment since they showed significant anti-inflammatory and analgesic effects on recurrent aphthous stomatitis.
Similar content being viewed by others


Background
The oral mucosa is affected by the chronic inflammatory condition known as recurrent aphthous stomatitis. It is characterized by excruciating oral lesions unrelated to a primary disease [1]. The incidence rate ranges from 5 to 60% in different communities; generally, it is more common among younger people, women, and people from higher socioeconomic levels [2]. Genetics, nutritional deficits, stress, and immunological dysfunction are typical etiological variables. Other factors include systemic disorders, hormonal imbalance, mechanical trauma, viral and bacterial infections, dietary allergies, vitamin and microelement shortages, hereditary predisposition, and stress [3, 4]. RAS (Recurrent Aphthous Stomatitis) lesions are recurrent; stress and anxiety play a crucial role in their development and recurrence [5, 6].
All of these factors have the potential to upset the body’s balance between oxidants and antioxidants, which would then lead to the production of free radicals. The oxidative stress brought on by increased free radical concentrations can impair immune system function, leading to cellular damage [6]. The most crucial free radicals in a biological system are those produced by oxygen [7]. Increased oxidative stress and an imbalance of oxidants and anti-oxidants are the primary causes of oral aphthous stomatitis. Oxidative stress develops when the intracellular levels of Reactive oxygen species (ROS) are higher than the normal levels produced intra or extra-cellular [8]. Both internal and external processes can produce free radicals. Endogenous generation of free radicals is caused by a variety of processes, including ischemia, infection, immune cell activation, inflammation, mental stress, cancer, excessive exercise, and aging. Exposure to environmental toxins, heavy metals (Pb, Cd, Fe, As, and Hg), specific medications (bleomycin, gentamycin, cyclosporine, and tacrolimus), cigarette, smoke, chemical solvents, cooking (smoked meat, fat, and used oil), radiations, and alcohol can result in the production of exogenous free radicals [9].
Numerous medications and techniques including laser therapy, a widely used treatment in craniofacial area, have been investigated to treat the symptoms of the disease because the cause is unknown. Multifocal treatment is used, and it varies depending on the risk factors. In all cases, treatment is symptomatic and aims to alleviate pain and aphthous inflammation [10,11,12,13].
Due to adverse side effects of pharmaceutical medicines, most patients choose herbal remedies [14]. Plants, food, and samples of propolis commonly include caffeic acid (3,4-dihydroxycinnamic acid), an essential phenolic compound, especially in the form of caffeic acid phenethyl ester (CAPE) [15]. This substance has neuroprotective, antibacterial, anti-inflammatory, cytotoxic, anti-chemotherapy, and anti-radiotherapy toxicity [16].
Some applications of this material in dentistry to date include the prevention of tooth decay, the reduction of chemotherapy-induced oral mucositis, the treatment of oral cancer, the management of gum and periodontal diseases, the inhibition of plaque, and anti-inflammatory properties [17]. Additionally, caffeic acid possesses biological effects that are anti-proliferative, anti-oxidant, anti-neoplastic, and antifungal [15, 18].
It has been demonstrated that Caffeic acid is a potent antioxidant that can neutralize ROS and protect cell membranes from lipid peroxidation. With a strong antioxidant impact and modest antibacterial activity, it is also a carcinogenic inhibitor. Along with many other advantages, it can also aid in preventing from atherosclerosis and cardiac problems [19]. According to research on the anti-inflammatory properties of this chemical, caffeic acid lowers the levels of interleukin-1beta, interleukin-6, and TNF-alpha [20].
Since caffeic acid contains anti-inflammatory and anti-oxidant characteristics and is a plant-based substance, it is safe, and no study has been done that has precisely examined the compound’s impact on recurrent aphthous stomatitis. This study aimed to assess the effects of caffeic acid on pain intensity, inflammatory lesion diameter, and the treatment duration of recurrent aphthous stomatitis lesions. By this study we are looking for introducing a novel treatment using a new medicine made of Caffeic acid, a natural substance whose anti-inflammatory and analgesic effects has been proven in the treatment of other medical and dental problems.
Methods
This randomized double-blinded clinical trial is conducted based on CONSORT reporting guidelines [21] and was approved by the medical ethics committee of Mazandaran University of Medical Sciences (Ethical code: IR.MAZUMS.REC.1401.261). It also received IRCT code of IRCT20220815055700N1on 03/09/2022.
Before participating in the trial, all patients signed a consent form after receiving a complete description of the treatment process and any potential complications.
Participants and eligibility criteria
According to the research done by Ghorbani et al. (2020), which the mean and standard deviation of the lesion diameter in the intervention group was 1.9 ± 1.3, and in the control group was 4.1 ± 2, with a confidence level of 95%, a test power of 90%, and for the two-way test, by using the formula for comparing the two averages in the G-power software; the sample size of the current study was calculated at 13 in each group, and taking into account a 50% decline, it was increased to 25 participants in each group (totally 50 participants) [22].
Initially, 50 participants were chosen using a convenient selection technique based on the inclusion criteria. To divide the samples into two groups, the blocking approach was applied. In each block, two patients were in the intervention group and two patients in the control group, making the blocks quadrable. Samples were allocated randomly using a blocking technique and random number generator software. The patients were chosen based on the inclusion criteria among those who were referred to the Mazandaran dental school with recurrent aphthous stomatitis in the age range of 20 to 40 and reported a history of mild aphthous lesions in parts like the lips and buccal mucosa. The patients were randomized into two groups at random: 25 patients in the intervention group and 25 patients in the control group. The chief nurse of the dental clinic registered the patients and administered the participants’ medication (either caffeic acid mucoadhesive tablets or a placebo), who was not an analyst or an evaluator. The intervention lasted seven days.
Patients with minor recurrent aphthous stomatitis, those with aphthous lesions in the lips or buccal mucosa (these areas are more accessible and less mobile), those not using dentures, not taking antibiotics, and overall good health are all required for inclusion in this study.
Patients who were pregnant, smoked, unable to use mucoadhesive tablets, had Behcet’s syndrome or other syndromes characterized by aphthous-like lesions, had myopathy or muscular disorders, had skin and mucosal auto-immune diseases, had liver failure, had urticaria or experienced skin and mucosal itching, or couldn’t participate in the study for personal or social reasons were all excluded from the study [23].
Developing mucoadhesive tablets
Mucoadhesive tablets were produced in the laboratory of Mazandaran University of Medical Sciences (Faculty of Pharmacy). Mucoadhesive tablets were made by eccentric punching machine and by direct compression method. The mucoadhesive tablet formulation was prepared with a confirmed percentage of Caffeic acid as an active pharmaceutical ingredient (API), Carbopol as a bioadhesive and biocompatible polymer to adhere the tablets to the mucosa and to control the release of the active pharmaceutical ingredient, mannitol as a filler and sweetener, magnesium stearate was prepared as a lubricant and microcrystalline cellulose (Avicel®) was used as a diluent and anti-adhesion to improve the formulation.
Study protocol
The evaluator and each patient in both groups were blinded in this investigation. The initial visit to the dental clinic was considered the baseline (day 0), and the patients were instructed to refer during the first 24 h following the appearance of aphthous lesions. Patients were first reassured of the project’s safety during the initial visit, and they were then requested to read, sign, and complete a questionnaire outlining their medical and dental histories. Notably, the examiner in this study was blinded and unaware of the medication provided to each patient. The first mucoadhesive tablet was applied by the examiner to the patient’s aphthous lesion during the same session. Three times a day, in the morning, noon, and evening, the patients were instructed to take the tablets. The mucoadhesive tablet consumption instruction was explained to them in detail, and they were urged to remove the tablet after 30 min and refrain from eating or drinking for 30 min. The same technique was carried out in the control group using a placebo, which comprised all the ingredients found in caffeic acid mucoadhesive tablets but not the caffeic acid that serves as their main component. Every patient was instructed to abstain from using further anti-inflammatory medications during the study.
The diameter of the lesions and the inflammatory halo around them were measured using a metal caliper at 0 (baseline), 3, 5, and 7 days later to assess the healing of the lesions.
Additionally, patients were asked to use the Visual Analogue Scale (VAS) to assess the severity of their discomfort. Zero on this scale indicates no pain, while ten indicates the most severe pain. The patients determined the point on this scale that best described their level of discomfort and estimated it using a numerical scale (for example, from 1 to 10). After every meal, patients completed the questionnaire three times a day, recording their VAS. Following the stimulation brought on by chewing, ingesting, and food particles, the pain increases. Patients were deemed to have improved when their pain score was 1 and the diameter of their lesions was smaller than 1 mm [23].
Statistical analysis
The data were reported using descriptive indicators of frequency, mean, percentage, and standard deviation. Shapiro Wilk test was used to check the hypothesis of normal distribution of the data, and the results showed that the data did not follow the hypothesis of normal distribution. Chi-square (compare qualitative variables in two group), Mann-Whitney (compare non normal value in two group) and GEE tests (compare non normal value in different times) were used in the present study. All obtained data were entered into SPSS 24 software and analyzed. The significance level was considered less than 0.05.
Results
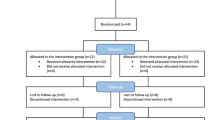
50 patients initially enrolled in the study; however, 47 patients continued to participate through the study’s conclusion and 3 participants withdrew in the middle of the study (Fig. 1). Participants didn’t claim any side effects related to the medicine.

CONSORT flowchart
The mean (standard deviation) age of the subjects was 29.70 ± 6.10; 6.4% had a history of systemic illnesses, and 3% of participants were female. Regarding age, gender, and history of systemic disorders, there was no discernible difference between the two groups (P > 0.05) (Table 1). As these variables did not have any statistically significant difference, we can perceive no confounding effect of these variables on the results of the present study (P > 0.05).
Table 2 displays a statistically significant decreasing trend of lesion diameter in both groups when comparing intra-grouply from days 0 to 7 (P < 0.001). Compared to the control group, this trend was more pronounced in the intervention group. When comparing the groups, there was no noticeable difference in the lesion diameter on day 0. Greater lesion diameter decrease was seen in the intervention groups on days three and seven of the trial, though this difference was not statistically significant. On the 5th day of the trial, the mean lesion diameter of the treated group was significantly lower than the control group (P = 0.012).

The intra-group and inter-group comparison of the lesions’ mean diameter showing a decreasing trend, which is more significant in the intervention group
Figure 2 demonstrates that the intervention group’s mean lesion diameter was greater than it was in the control group on day 0; However, this difference was not statistically significant. The lesion diameter decreased more noticeably in the intervention group compared to the control group.
Table 3; Fig. 3 show that both groups’ mean pain intensity showed a significant decreasing trend (P < 0.001) in the intra-group comparison.
Pain intensity showed a significant decreasing trend in both groups from day 2 to day 7, with the intervention group showing a more significant decrease than the control group so that patients in the intervention group were deemed entirely improved by day 5.

The average pain intensity of the patients showed a significant decreasing trend in both groups from day 2 to day 7, and was more significant in the intervention group
Discussion
This study aimed to determine the effect of caffeic acid mucoadhesive tablets on the size of the inflammatory lesion and the pain intensity associated with aphthous lesions in participants. The average diameter of the lesion in both groups’ intra-group examinations indicated a declining trend and a significant difference, according to the study’s findings. Except on the fifth day, the average diameter in the intergroup comparison did not reveal a statistically considerable difference.
Studies have revealed that caffeic acid enhances wound healing. Through anti-inflammatory mechanisms, this compound regulates neutrophil infiltration [24, 25]. Typically found in plants, meals, and propolis samples, caffeic acid is a phenolic molecule that is most commonly found as caffeic acid phenethyl ester (CAPE) [15].
As a secondary metabolite, caffeic acid phenethyl ester has anti-inflammatory therapeutic effects in the flavonoid form. Flavonoids have both analgesic and anti-inflammatory effects. The inhibition of the enzymes involved in generating inflammatory chemical mediators is the mechanism through which flavonoids work. Through the NF-κB pathway, CAPE, a substance in flavonoids, can block the synthesis of inflammatory cytokines such as TGF- β12, TNF-α, IL-6, and IL-1 [26, 27]. Numerous studies have investigated the anti-inflammatory, anti-oxidant, and analgesic capacities of caffeic acid to date. Still, it is impractical to compare the findings precisely because there hasn’t been any research on the use of caffeic acid mucoadhesive tablets for recurrent aphthous stomatitis treatment. Thus, we will review other studies on the anti-inflammatory and tissue repair capabilities of caffeic acid.
Puspasari et al. investigated the impact of topical caffeic acid phenethyl ester treatment on fibroblast expression and fibroblast growth factor-2 in diabetic traumatic wounds in the lower lip of rats. On days 5 and 7, the intervention group received topical treatment of caffeic acid phenethyl ester, which boosted the expression of FGF-2 and fibroblasts. Additionally, there was an association between higher fibroblast numbers and FGF-2 expression. This study showed that the local administration of caffeic acid phenethyl ester enhances fibroblast and FGF-2 expression during the healing of traumatic lesions [28].
In the study of Diab et al., the impact of a substance containing caffeic acid phenethyl ester on the healing and repairing of buccal mucosal wounds in the mouths of male rats showed that a group of mice that were treated with caffeic acid phenethyl ester had more epithelialization and collagen fibers formation than the control group [29].
The lesion size was assessed on days 1, 3, 5, and 8 in a trial that examined the impact of Proaftol (Extract Propolis 25%) mucoadhesive tablets on recurrent aphthous stomatitis, and the findings revealed a substantial decreasing trend. By the eighth day, the average of 5.7 mm from the first day had decreased to zero, signifying complete recovery [30]. Similar results were found in the current investigation, and on the seventh day, the average is almost zero. Even though caffeic acid is present in both formulations of these two mucoadhesive tablets, there may be a slight discrepancy in the results.
Ozório et al., Parolia et al. and, Wickiewicz et al. employed caffeic acid phenethyl ester-containing materials in the oral cavity as an intracanal medication and pulp covering agent in root canal therapy, wound healing, bone regeneration, and the construction of dental bridges. Their findings on wound healing and regeneration concurred with those of the present study [31,32,33].
The outcomes of the patient’s pain intensity from the first to seventh study days were another outcome. According to the findings, the mean pain intensity within each group significantly decreased in both groups. In the intergroup comparison, there was a notable difference in the two groups’ mean pain intensity from the second to the seventh day, with the control group experiencing more pain than the experimental group. Caffeic acid phenethyl ester was utilized by Moon et al. to promote wound healing and lessen post-tonsillectomy pain. The VAS scale measured pain severity on days 0, 1, 2, 3, and 7 to 10 following surgery. The caffeic acid phenethyl ester group experienced much less pain than the control group following tonsillectomy on days 3 and 7 to 10 [34]. As a result, their outcomes were in line with those of the current study.
Furthermore, the investigation of Proaftol (Propolis Extract 25%) mucoadhesive tablets on recurrent aphthous stomatitis and the pain it caused using the VAS scale on days 1, 3, 5, and 8 of the study shows a decreasing trend, so that on the first day, the average number was 3. On the eighth day, the number was zero, meaning the pain had utterly improved [30]. According to the VAS scale used in the current study, the intervention group’s pain level was zero on the seventh day.
Caffeic acid is also used for intrabuccal wound healing, epithelial repair following tooth extraction, and pain relief in the mouth. It has also effectively treated the painful dry socket problem following tooth extraction [35,36,37,38]. Anti-inflammatory, immune system balancing, and anti-oxidant characteristics are all possessed by caffeic acid. Additionally, this chemical lessens tissue damage brought on by oxidative stress and promotes epithelial regeneration during wound healing [39, 40]. The balance of oxidative and anti-oxidant components is generally necessary for the routine healing of wounds. Wound healing is hampered by higher levels of ROS and oxidative stress. By regulating this process, caffeic acid, as an anti-oxidant, enhances wound healing [41]. In addition, caffeic acid phenethyl ester has anti-bacterial effects and promotes wound healing and repairing by reducing the microorganisms’ growth [42]. As a result, it is anticipated that using caffeic acid mucoadhesive tablets will reduce the size of lesions, the intensity of pain, and discomfort in recurrent aphthous patients. This conclusion is based on the findings of the present study, the anti-inflammatory effect of caffeic acid, and the various properties of this substance that have been mentioned.
These days, treating aphthous lesions using mucoadhesive tablets impregnated with chemicals and herbal remedies is a widespread practice, and numerous studies have been done on this subject.
The use of mucoadhesive tablets made of medicinal components has been successful because they increase the medicine’s effectiveness and prolong its duration in the wound site [14, 23, 43]. The wound is protected by this treatment procedure, which lessens the lesion’s discomfort and suffering during the healing process. A secondary infection can be avoided, which lowers the requirement for antibiotics and antifungals [44]. It is hoped that mucoadhesive tablets containing caffeic acid will be used frequently as a treatment option in patients with recurrent aphthous stomatitis due to the positive results observed in their use. This is the first study examining the impact of caffeic acid mucoadhesive tablets on recurrent aphthous stomatitis. Thus, a thorough comparison of the findings was impossible. More examinations with greater sample sizes are needed. The lack of access to the patients during the study was another limitation.
Conclusion
The findings of the present study demonstrated the noticeable effect of Caffeic acid on reducing the mean diameter of the aphthous lesions due to its wound healing property. Also, this substance reduced the pain intensity of the subjects. Thus, Caffeic acid mucoadhesive tablets are suggested for palliative treatment since they have anti-inflammatory and analgesic effects on recurrent aphthous stomatitis.as herbal-based medicines are mainly made of natural substances and have fewer side effects, patients’ tendency to these treatments is increasing and we believe that this medicine would also be welcomed. Furthermore, we suggest more studies on different form of this substance including its nanoform, applying them in the management of other oral diseases, and comparing them with the base form of the substance.
Data availability
All data generated or analyzed during this study are included in this published article.
Abbreviations
- VAS:
-
Visual analogue scale
- RAS:
-
Recurrent aphthous stomatitis
- ROS:
-
Reactive oxygen species
- CAPE:
-
Caffeic acid phenethyl ester
- API:
-
Active pharmaceutical ingredient
- GEE:
-
Generalized estimated equation
References
Sánchez J, Conejero C, Conejero R. Recurrent aphthous stomatitis. Actas Dermo-Sifiliográficas. (English Edition). 2020;111(6):471–80.
Cui RZ, Bruce AJ, Rogers RS III. Recurrent aphthous stomatitis. Clin Dermatol. 2016;34(4):475–81.
Chiang C-P, Chang JY-F, Wang Y-P, Wu Y-H, Wu Y-C, Sun A. Recurrent aphthous stomatitis–Etiology, serum autoantibodies, anemia, hematinic deficiencies, and management. J Formos Med Assoc. 2019;118(9):1279–89.
Manoj MA, Jain A, Madtha SA, Cherian TM. Prevalence and risk factors of recurrent aphthous stomatitis among college students at Mangalore, India. PeerJ. 2023;11:e14998.
Gallo CB, Mimura MAM, Sugaya NN. Psychological stress and recurrent aphthous stomatitis. Clinics. 2009;64:645–8.
Doddamani LG, Khan M, Gupta N, KR V KN. Association of Psychological Factors like stress, anxiety and depression in recurrent Apthous Stomatitis. Int J Oral Health Med Res. 2017;3(5):18–23.
Phaniendra A, Jestadi DB, Periyasamy L. Free radicals: properties, sources, targets, and their implication in various diseases. Indian J Clin Biochem. 2015;30:11–26.
Farhad-Mollashahi L, Pouramir M, Motalebnejad M, Honarmand M, Bijani A, Shirzad A. Comparison of salivary total antioxidant capacity and lipid peroxidation in patients with recurrent aphthous stomatitis and healthy persons. J Babol Univ Med Sci. 2013;15(5):39–44.
Pizzino G, Irrera N, Cucinotta M, Pallio G, Mannino F, Arcoraci V et al. Oxidative stress: harms and benefits for human health. Oxidative medicine and cellular longevity. 2017;2017.
Belenguer-Guallar I, Jiménez-Soriano Y, Claramunt-Lozano A. Treatment of recurrent aphthous stomatitis. A literature review. J Clin Experimental Dentistry. 2014;6(2):e168.
Altenburg A, El-Haj N, Micheli C, Puttkammer M, Abdel-Naser MB, Zouboulis CC. The treatment of chronic recurrent oral aphthous ulcers. Deutsches Ärzteblatt International. 2014;111(40):665.
Aldelaimi AA, Ahmed RF, Enezei HH, Aldelaimi TN. Gummy smile esthetic correction with 940 nm Diode Laser. Int Med J. 2019;26(6):1–3.
Aldelaimi TN, Khalil AA. Clinical application of diode laser (980 nm) in maxillofacial surgical procedures. J Craniofac Surg. 2015;26(4):1220–3.
Molania T, Malekzadeh Shafaroudi A, Saeedi M, Moosazadeh M, Valipour F, Rostamkalaei SS, et al. Evaluation of cinnamaldehyde mucoadhesive patches on minor recurrent aphthous stomatitis: a randomized, double-blind, placebo-controlled clinical trial. BMC Oral Health. 2022;22(1):235.
Sardi JCO, Gullo FP, Freires IA, de Souza Pitangui N, Segalla MP, Fusco-Almeida AM, et al. Synthesis, antifungal activity of caffeic acid derivative esters, and their synergism with fluconazole and nystatin against Candida Spp. Diagn Microbiol Infect Dis. 2016;86(4):387–91.
Murtaza G, Karim S, Akram MR, Khan SA, Azhar S, Mumtaz A et al. Caffeic acid phenethyl ester and therapeutic potentials. Biomed Res Int. 2014;2014.
LS VK. Propolis in dentistry and oral cancer management. North Am J Med Sci. 2014;6(6):250.
Dziedzic A, Kubina R, Kabała-Dzik A, Wojtyczka RD, Morawiec T, Bułdak RJ. Caffeic acid reduces the viability and migration rate of oral carcinoma cells (SCC-25) exposed to low concentrations of ethanol. Int J Mol Sci. 2014;15(10):18725–41.
Spagnol CM, Assis RP, Brunetti IL, Isaac VLB, Salgado HRN, Corrêa MA. In vitro methods to determine the antioxidant activity of caffeic acid. Spectrochim Acta Part A Mol Biomol Spectrosc. 2019;219:358–66.
Zhang M, Zhou J, Wang L, Li B, Guo J, Guan X, et al. Caffeic acid reduces cutaneous tumor necrosis factor alpha (TNF-α), IL-6 and IL-1β levels and ameliorates skin edema in acute and chronic model of cutaneous inflammation in mice. Biol Pharm Bull. 2014;37(3):347–54.
Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. J Pharmacol Pharmacotherapeutics. 2010;1(2):100–7.
Ghorbani A, Akbari J, Boorboor M, Nekoukar Z, Eslami G. Evaluation of zinc sulfate mucoadhesive formulation on recurrent aphthous stomatitis: a randomized double-blind, placebo-controlled clinical trial. BMC Oral Health. 2020;20:1–6.
Molania T, Akbari J, Babaei A, Lotfizadeh A, Moosazadeh M, Mesgarani A, et al. Atorvastatin mucoadhesive tablets in the management of recurrent aphthous stomatitis: a randomized clinical study. BMC Oral Health. 2023;23(1):1–8.
Olgierd B, Kamila Ż, Anna B, Emilia M. The pluripotent activities of caffeic acid phenethyl ester. Molecules. 2021;26(5):1335.
Romana-Souza B, Dos Santos JS, Monte-Alto-Costa A. Caffeic acid phenethyl ester promotes wound healing of mice pressure ulcers affecting NF-κB, NOS2 and NRF2 expression. Life Sci. 2018;207:158–65.
Heldayani I, Wahyuni I, Effectiveness of the natural-based products and mucoadhesive for recurrent aphthous. Stomatitis therapy: a systematic review. Int J Appl Pharm. 2021;13:7–13.
Nurhayati W, Dewi VYK, Djajakusumah TM. Anti-inflammatory effect of Trigona spp. propolis in restricting edema volume. Althea Med J. 2015;2(1):96–9.
Puspasari A, Harijanti K, Soebadi B, Hendarti HT, Radithia D, Ernawati DS. Effects of topical application of propolis extract on fibroblast growth factor-2 and fibroblast expression in the traumatic ulcers of diabetic Rattus norvegicus. J oral Maxillofacial Pathology: JOMFP. 2018;22(1):54.
Diab A, Helal ME, Abdel Rahman M. The impact of topical application of propolisonbuccal mucous membranewounds healing. Mansoura J Dentistry. 2015;2(1):43–6.
Stojanovska AA, Popovska M, Muratovska I, Mitic K, Stefanovska E, Nikolovska VR. The Rapeutic Effect of Proaftol in Treatment of Recurrent Aphthous Stomatitis. Prilozi. 2014;35(3):195–202.
Ozório JEV, de Oliveira DA, de Sousa-Neto MD, Perez DEC. Standardized propolis extract and calcium hydroxide as pulpotomy agents in primary pig teeth. J Dent Child. 2012;79(2):53–8.
Parolia A, Kundabala M, Rao N, Acharya S, Agrawal P, Mohan M, et al. A comparative histological analysis of human pulp following direct pulp capping with Propolis, mineral trioxide aggregate and Dycal. Aust Dent J. 2010;55(1):59–64.
Więckiewicz W, Miernik M, Więckiewicz M, Morawiec T. Does propolis help to maintain oral health? Evidence-based complementary and alternative medicine. 2013;2013.
Moon JH, Lee MY, Chung Y-J, Rhee C-K, Lee SJ. Effect of topical propolis on wound healing process after tonsillectomy: randomized controlled study. Clin Exp Otorhinolaryngol. 2018;11(2):146–50.
Velnar T, Bailey T, Smrkolj V. The wound healing process: an overview of the cellular and molecular mechanisms. J Int Med Res. 2009;37(5):1528–42.
Paulino N, Dantas AP, Bankova V, Longhi DT, Scremin A, de Castro SL, et al. Bulgarian propolis induces analgesic and anti-inflammatory effects in mice and inhibits in vitro contraction of airway smooth muscle. J Pharmacol Sci. 2003;93(3):307–13.
Kamburoğlu K, Özen T. Analgesic effect of Anatolian propolis in mice. Agri. 2011;23(2):47–50.
Kuropatnicki AK, Szliszka E, Krol W. Historical aspects of propolis research in modern times. Evidence-based complementary and alternative medicine. 2013;2013.
Kızıldağ A, Arabacı T, Albayrak M, Taşdemir U, Şenel E, Dalyanoglu M, et al. Therapeutic effects of caffeic acid phenethyl ester on alveolar bone loss in rats with endotoxin-induced periodontitis. J Dent Sci. 2019;14(4):339–45.
Gül M, Günay A, Tanik A. An evaluation of the effects of caffeic acid phenethyl ester and ankaferd blood stopper on secondary wound healing of oral mucosal tissue. Turk J Med Sci. 2020;50(1):248–57.
Merlini R, Parolia A, Pau A, Amalraj FD. The role of Propolis in inflammation and Orofacial Pain: a review. P; 2013.
Kaya S, Yilmaz DE, Akmayan I, Egri O, Arasoglu T, Derman S. Caffeic acid phenethyl ester loaded electrospun nanofibers for wound dressing application. J Pharm Sci. 2022;111(3):734–42.
Eslami G, Ghorbani A, Akbari J, Farmoudeh A, Faghih F, Moghimi M. Efficacy of oral mucoadhesive N-acetylcysteine tablets in treatment of recurrent aphthous stomatitis: a Randomized Double-Blind, placebo-controlled clinical trial. Front Dentistry. 2023.
Giammarinaro E, Cosola S, Oldoini G, Gulia F, Peñarrocha-Oltra D, Marconcini S, et al. Local formula with mucoadhesive property: a randomized clinical trial of a therapeutic agent for the treatment of oral aphthous ulcers. J Contemp Dent Pract. 2019;20(11):1249–53.
Acknowledgements
We would like to thank all participants who contributed to this study, the research center of Mazandaran University of Medical Sciences, and all who helped in the completion of this study.
Funding
No funding resources were used in this research.
Author information
Authors and Affiliations
Contributions
Maedeh Salehi and Tahereh Molania contributed to the study conception and design. Material preparation, data collection and analysis were performed by Majid Saeedi, Reza Negarandeh, Azin Savabi and Abolfazl Hosseinnataj. The first draft of the manuscript was written by Anahita Lotfizadeh and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations. Informed consent was obtained from all subjects and/or their legal guardian(s). This trial was approved by the medical ethics committee of Mazandaran University of Medical Sciences (Ethical code: IR.MAZUMS.REC.1401.261) and received IRCT code of IRCT20220815055700N1.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Salehi, M., Saeedi, M., Negarandeh, R. et al. Evaluation of caffeic acid mucoadhesive tablets on minor recurrent aphthous stomatitis: a randomized, double-blind, placebo-controlled clinical trial. BMC Oral Health 24, 210 (2024). https://doi.org/10.1186/s12903-024-03936-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-024-03936-0