
Abstract
Aim
To evaluate the effects of root canal treatment (RCT) and post-crown restoration on stress distribution in teeth with periapical bone defects using finite element analysis.
Methodology
Finite element models of mandibular second premolars and those with periapical bone defects (spherical defects with diameters of 5, 10, 15, and 20 mm) were created using digital model design software. The corresponding RCT and post-crown restoration models were constructed based on the different sizes of periapical bone defect models. The von Mises stress and tooth displacement distributions were comprehensively analyzed in each model.
Results
Overall analysis of the models: RCT significantly increased the maximum von Mises stresses in teeth with periapical bone defects, while post-crown restoration greatly reduced the maximum von Mises stresses. RCT and post-crown restoration slightly reduced tooth displacement in the affected tooth. Internal analysis of tooth: RCT dramatically increased the maximum von Mises stress in all regions of the tooth, with the most pronounced increase in the coronal surface region. The post-crown restoration balances the internal stresses of the tooth and is most effective in periapical bone defect − 20-mm model. RCT and post-crown restoration slightly reduced the tooth displacement in all regions of the affected tooth.
Conclusions
Root canal treatment seemed not to improve the biomechanical state of teeth with periapical bone defects. In contrast, post-crown restoration might effectively balance the stress concentrations caused by periapical bone defects, particularly extensive ones.
Similar content being viewed by others


Introduction
Apical periodontitis (AP) is a common inflammatory condition that affects tissues surrounding the tooth root. It is typically caused by bacteria that enter the pulp of a tooth through cavities, cracks, or other types of damage, and then spread to the tissues surrounding the root [1,2,3]. Because the surrounding alveolar bone is destroyed, AP directly affects the stress condition of the affected tooth. This has a detrimental effect on the tooth’s ability to be preserved and restored. [4]. In a preliminary study, we found that the presence of periapical bone defects significantly affected the biomechanical response of teeth, the effects of which became more pronounced as the size of the bone defects increased. However, the subsequent therapeutic and restorative processes for teeth with periapical bone defects have not yet been studied in depth.
Conventional treatments for AP include root canal treatment (RCT), apical surgery, and medication. Although these treatments can remove the infection, they lead to a certain degree of stress concentration in the tooth, which may be detrimental to tooth preservation. [4,5,6]. In recent years, as nonsurgical approaches have been advocated for the treatment of AP [7, 8], preservation and restoration of the affected tooth at a later stage have become particularly important. Post-crown restoration is a common method of dental restoration that has been shown to be beneficial in improving the stress state of teeth [9] and is widely used in clinical settings. However, owing to imperfect treatment, teeth with periapical bone defects are frequently observed even after post-crown restoration [10, 11]. However, the effect of periapical bone defects caused by AP and their change in size on the subsequent post-crown restoration of the affected teeth has not been completely elucidated.
Finite element analysis (FEA) is a powerful tool in dental biomechanics that allows researchers and clinicians to better understand the mechanical behavior of dental structures [12]. Therefore, this study aimed to investigate the effect of RCT and post-crown restorations on the biomechanical state of teeth with periapical bone defects of different sizes by establishing corresponding FEA models and evaluate the mechanical stability of teeth with periapical bone defects after treatment and restoration. The null hypotheses for this study were as follows: (1) RCT and post-crown restoration do not change the biomechanical state of the affected tooth and (2) RCT and post-crown restoration result in the same biomechanical alterations in affected teeth with different sizes of periapical bone defects.
Materials and methods
The schematic illustration of the procedures performed sequentially is presented in Fig. 1.

Schematic overview of the study design
Cone-beam computed tomography (CBCT) data
After obtaining informed consent from the volunteers, medical CBCT (iCRco, Inc., USA) digital image data of the oral and maxillofacial regions were obtained (Fig. 2). This study was approved by the Ethics Committee of Ethics Committee of the School and Hospital of Stomatology, Wenzhou Medical University Institute of Stomatology (Approval Number: WYYKQ2022022).

Typical CBCT images of periapical cysts after restoration
Model construction
First, we successfully constructed a normal mandibular second premolar FEA model, including the cortical bone, cancellous bone, enamel, dentin, periodontal ligament, pulp, and cementum using Materialise Mimics 21.0 (Materialise, Belgium) and Geomagic Wrap 2021 (Geomagic, USA). We used SOLIDWORKS 2021 (Dassault Systèmes, France) to construct the following models (Fig. 3A):

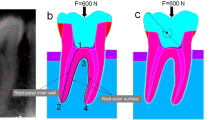
Schematic view of model structure and stress loading. A: Model A-A4 (periapical bone defect group). Models B-B4 (RCT group). Model C-C4 (post-crown restoration group). B: F = 400 N applied in a direction that was oblique (45°) to the model’s long axis
(1) Model Group A
To simulate periapical bone defects caused by AP, a Model A periapical bone defects was constructed based on normal teeth (Model A). Model A1: Spherical defects with diameters of 5 mm surrounding the apical region. Model A2: Spherical defects with diameters of 10 mm surrounding the apical region. Model A3: Spherical defects with a diameter of 15 mm surrounding apical region. Model A4: Spherical defects with diameters of 20 mm surrounding the apical region.
(2) Model Group B
Construction of the corresponding RCT models (Model B) was based on the periapical bone defect model. The round root canal enlargement (MASTAL FILE#35, 0.04 taper), intra-root canal gutta-percha (Gutta Percha Points, GC Co., Japan) obturation, and tooth crown were sealed with 3 M resin (3 M, USA). The RCT Models B1, B2, B3, and B4 were further constructed based on the different sizes of the corresponding periapical bone defects.
(3) Model Group C
A post-crown restoration model (Model C) was constructed based on the RCT model. The post-tract preparation preserves the apical 4 mm of the gutta-percha and the later fiberglass post (3 M, USA) restoration, with a simulated 0.1-mm thickness bonding layer (3 M, USA) between the dentin and the fiberglass post. Starting from the anatomical contour of the crown (Wieland, Germany), the standard preparation process was followed, with a 2-mm preparation of the occlusal, buccal, and lingual surfaces, 1- to 1.5-mm preparation of the mesiodistal surfaces, 4–6° degree of polymerization, and 1-mm width of the shoulder. The post-crown restoration Models B1, B2, B3, and B4 were constructed based on the different sizes of the corresponding periapical bone defects.
All the models were meshed using second-order cells. The number of elements and nodes in each model are listed in Table 1.
Loading mode and loading force
In this study, the lingual surface of the crown received constant loading (400 N) that was applied in a direction that was oblique (45°) to the model’s long axis [13] (Fig. 3B). A simulation was performed to determine the stress state of the tooth during occlusion. The edges of the mandible were fixed to prevent movement in the X-, Y-, and Z-directions.
Preconditions of the experiment
All tissues and materials were considered to have ideal bonding conditions and were isotropic, homogeneous, and linearly elastic. The corresponding mechanical parameters are listed in Table 2.
Biomechanical analysis
ANSYS 17.0 (ANSYS, USA) was used to calculate the stress distribution and displacement pattern of the tooth. Overall analysis of the models: The overall stress distribution and tooth displacement for each model were obtained and their maximum von Mises stress and maximum tooth displacement calculated. Internal analysis of the tooth: The tooth was divided into coronal (occlusal surface, middle, and cervix) and root (cervix, middle, and apical) sections, and the stress distribution and tooth displacement in each section were analyzed.
Results
Overall analysis of the model
Our FEA results were represented visually as the stress distribution and tooth displacement using an ANSYS 17.0 predefined progressive visual color scale (ANSYS, USA). Figure 4 shows the von Mises stress distribution cloud maps for the periapical bone defect models and corresponding RCT and post-crown restoration models.

Stress distribution in overall analysis of the models. A: von Mises stress distribution cloud map of the model cross-section; B: model maximum von Mises stress analysis
Compared with the periapical bone defect model, RCT increased the maximum von Mises stresses of the teeth, whereas post-crown restoration greatly reduced the maximum von Mises stresses of the teeth (Fig. 4A, B). However, the differences between the RCT, post-crown restoration, and periapical bone-defect groups did not change as the size of the periapical bone defect increased (Fig. 4B). Statistical description of the stress distributions for each model in Supplementary Table 1.
The tooth displacement of the root increased noticeably with an increase in the periapical bone defect size, particularly in the apical region, based on the tooth displacement distribution cloud maps of the periapical bone defect models (Fig. 5A Model A1-A4). Unlike the stress distribution, RCT and post-crown restoration only slightly reduced tooth displacement, and this effect did not change as the size of the bone defect increased (Fig. 5A, B). Statistical description of the tooth displacement for each model in Supplementary Table 2.

Tooth displacement distribution in overall analysis of the models. A: Tooth displacement distribution cloud map of the model cross-section; B: model maximum tooth displacement analysis
Internal analysis of the tooth
The von Mises stress distribution cloud maps and associated maximum von Mises stress analysis for the coronal (occlusal surface, middle, and cervix) and root (cervical, middle, and apical) sections revealed that in the coronal surface region, the maximum von Mises stresses in the RCT group greatly exceeded those in the periapical bone defect and post-crown restoration groups (Fig. 6A, B). In the coronal cervix, the maximum von Mises stress in the post-crown restoration group decreased considerably, whereas the maximum von Mises stress in the rest of the region increased slightly. In addition, similar results were obtained in the internal analysis of all models with different sizes of periapical bone defects (Supplementary Figs. 1, 2, 3).
The cloud maps of the tooth displacement distribution and the corresponding maximum tooth displacement analysis revealed that, in all regions of the tooth interior, the RCT group showed a decrease in tooth displacement in all areas of the tooth interior, which was more pronounced in the pile core crown restoration group (Fig. 6C, D). Internal analysis of all models showed similar results for periapical bone defect diameters of 5, 10, and 15 mm. However, when the periapical bone defect diameter was 20 mm, the tooth displacement in the apical region of the post-crown restoration group significantly decreased (Supplementary Fig. 3).

Von Mises stress and tooth displacement distribution in internal parts of the tooth—diameter of periapical bone defect: 5 mm. A: von Mises stress distribution cloud maps for internal parts of the tooth; B: maximum von Mises stress for internal parts of the tooth; C: tooth displacement distribution cloud maps for internal parts of the tooth; D: maximum tooth displacement for internal parts of the tooth
Discussion
According to previous studies, AP causes periapical bone resorption, which reduces the biomechanical resistance of the affected tooth and makes it more susceptible to vertical root fracture [20,21,22]. RCT and post-crown restorations are widely used in clinical treatment and restoration. In this study, we simulated the treatment and restoration of teeth with periapical defects by combining clinical situations and procedures, such as RCT and post-crown restorations, using FEA. Our results showed that (1) RCT led to increased stress concentration, and post-crown restoration greatly reduced stress, and (2) this effect changed as the size of the bone defect increased. Therefore, the null hypothesis was rejected.
FEA models reasonableness analysis
RCT, as the primary treatment modality for teeth with AP, has also been shown to be useful for the treatment of large AP [7, 8, 23]. The American Dental Association (ADA) recommends that root canals should be prepared to a depth that extends to the tip of the tooth root when performing RCT [24]. Concurrently, the root canal preparation of the premolar needs to be enlarged to a diameter of about 1.2–1.5 mm to ensure complete removal of pulp and necrotic tissue inside the root canal and provide sufficient space for subsequent filling [25]. Therefore, we constructed an access cavity based on the abovementioned criteria and removed the entire apex of the pulp chamber to create a straight path from the access port to the root canal orifice. We chose gutta-percha as the root canal filling material because of its good apical filling properties, which are widely used in clinical practice. Studies have shown that good apical filling can minimize apical condensation force during root canal therapy [26].
Post-crown restorations can improve the health, function, and appearance of teeth while providing a durable and long-lasting solution to dental issues [27, 28]. The post-tract preparation preserves the apical 4 mm of the gutta-percha, [29]and the morphology of the post-tract preparation should match the chosen post type and conform to physiological anatomical principles [30]. Recently, various forms of post restoration in clinical applications, such as fiberglass posts, one-piece custom-milled zirconia posts, and cast Ni–Cr posts exist [31]. This study used fiberglass posts for post restoration because of their high clinical usage rate. We chose zirconia crowns because studies have shown that they are good restorative material owing to their excellent aesthetic and physical properties [32]. The Young’s modulus and Poisson’s ratio of zirconia crowns are 210 GPa and 0.22, respectively, while Young’s modulus for metal-ceramic crowns is approximately 70–100 GPa, metal crowns have a Young’s modulus of approximately 100–200 GPa. [33]. It may indicate that zirconia crowns are more rigid and less flexible than metal-ceramic crowns and metal crowns. Meanwhile, previous study demonstrated that the tooth restored with zirconia crowns may be more resistant to fracture and wear, as they can better withstand the occlusal load without bending or cracking [34].
In this experiment, the structure, material selection, and parameter settings of the model construction are referred to in relevant finite element studies and reasonably adjusted according to the clinical situation; thus, the model construction is reasonable.
Von Mises stress analysis
In the overall analysis, RCT increased the maximum von Mises stresses of the teeth, while post-crown restoration greatly reduced the maximum von Mises stresses of the teeth (Fig. 4A, B), Studies have demonstrated that the cavity inside the tooth becomes larger during RCT because the pulp and nerve are removed, which makes the tooth’s structure more fragile as well [5, 35]. Therefore, recently, the concept of minimally invasive endodontics (MIE) has been proposed as a means to enhance the fracture resistance of teeth that have undergone RCT [36]. For mature teeth, the gutta-perch filling root canal system is commonly used in RCT. However, the application of apical force to the gutta-percha causes pressure on the material and, as a result, circumferential tensile stresses on the canal surface. These stresses can cause vertical root fractures (VRF) [26, 37]. In contrast to mature teeth, mineral trioxide aggregate (MTA) may be a more suitable material for RCT in immature teeth because of the shorter treatment time associated with its use [38]. However, whether this change in the filling material of the root canal system affects the tooth root mechanics requires further study.
In contrast, post-crown restoration can significantly improve the mechanical properties of the affected tooth through the reinforcement of the post and the protective effect of the crown; thus, it is widely used in the preservation and restoration of affected teeth [39, 40]. Previous studies on post-crown restorations have focused on restorative materials and methods without considering periapical bone changes in teeth with AP [41]. However, periapical bone defects are often observed in teeth with AP in the clinic [10]. Consistent with the results of normal teeth with post-crown restorations, our study showed that post-crown restoration remains an effective restorative method even when periapical bone defects are present. According to data obtained from a retrospective study, the likelihood of root fractures occurring within 3 years of receiving zirconia post-crown restoration was 1.19% [42]. This is because of the application of post-improved mechanical stability of teeth. High-strength and high-hardness materials, such as zirconia, are used for restoration, which can significantly increase the load-bearing capacity of the teeth.
To understand the internal stress changes in periapical bone-defective teeth after RCT and post-crown restoration, we further investigated von Mises stress changes in six parts of the tooth in the coronal (occlusal surface, middle, and cervix) and root (cervix, middle, and apical) sections. We found that the RCT group showed stress concentration at the occlusal surface due to the partial loss of tissue in the coronal region of the tooth due to RCT. The composite resin was more brittle than the enamel and thus could not accommodate higher stresses internally [43, 44]. The stresses in the cervical region of the root decreased considerably after the post-crown restoration, although the von Mises stresses in other areas of the tooth increased slightly (Fig. 6A, B). This may be due to the disappearance of the internal cavity of the tooth after the post-crown restoration, which resulted in a more uniform stress distribution. This mechanical change is beneficial for tooth preservation [45, 46].
Tooth displacement analysis
The maximum tooth displacement was slightly lower in the RCT and post-crown restoration groups than in the periapical bone defect group under different periapical bone defect conditions. This has a positive effect on tooth preservation. It has been demonstrated that excessive tooth displacement can cause damage to periodontal tissues or even fracture of the tooth itself [4]. This phenomenon may be related to the homogenization of the internal stress distribution after RCT and post-crown restoration of the tooth. In addition, in the internal analysis of the teeth, the tooth displacement in the apical region of the post-crown restoration group showed a precipitous decrease when the periapical bone defect was 20 mm (Supplementary Fig. 3), suggesting that post-crown restoration exerts a more pronounced effect on the preservation and restoration of teeth with extensive periapical bone defects.
However, in our study, RCT and post-crown treatment were ineffective in reducing tooth displacement in teeth with periapical bone defects. This may be due to the fact that periapical bone loss results in the loss of alveolar bone support and restriction of the tooth root [47]. The alveolar bone is the part of the jawbone that surrounds and supports the teeth. It plays a crucial role in maintaining healthy teeth by providing a rigid foundation for tooth roots to anchor into [48]. Therefore, for the restoration of teeth with periapical bone defects, other treatments, such as periapical bone-defect filling materials, are suggested to increase the support of the affected tooth [49]. However, differences in the restorative effects of different bone-filling materials exist, which requires further research.
Limitations of the current study
This study found that RCT does not improve the biomechanical state of teeth with periapical bone defects, and post-crown restoration can effectively balance stress concentrations and provide suggestions for the prevention and treatment of teeth with periapical bone defects. Some limitations to the design of the experiment are as follows: 1) This experiment chose gutta-percha because of its good biocompatibility and plasticity. Recently, root canal filling materials have more options, such as calcium silicate-based cement and bioceramics [50]. Equally noteworthy is the fact that, a sufficient bond strength at the material-dentin contact is essential to guarantee a perfect seal of the root canal system and strengthen the resistance of the cervical section of the tooth to prevent fracture [51]. Meanwhile, in a clinical study, MTA plug and bond restoration was found to be a good dental restoration to prevent or minimizing microleakage [52]. Therefore, mechanical properties of different root canal filling materials and bond at the material-dentin interface needs to be more fully considered in the subsequent studies.
2) The experiment was well constructed for each structure of the teeth and alveolar bone and effectively simulated their intra-oral biomechanical conditions. However, this study did not simulate dental osseous structures as a hydrostatic system and a Functionally Graded Material Property system. In future studies, constructing different dental models and designing in vitro validation experiments to restore the intraoral conditions more accurately are necessary.
Conclusion
Within the limitations of the present study and those of finite element analysis, it was possible to conclude that root canal treatments seemed not to reduce the stress concentration caused by periapical bone defects. In contrast, post-crown restorations might effectively balance the uneven stress distribution within teeth with periapical bone defects, and improves the stability of the tooth stability. Root canal treatment and post-crown restorations might reduce slightly the increased tooth displacement of the affected tooth due to periapical bone defects. However, these results should be further validated by in vivo studies.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
References
Garrido M, Cárdenas AM, Astorga J, et al. Elevated systemic inflammatory Burden and Cardiovascular Risk in Young adults with endodontic apical Lesions[J]. J Endod. 2019;45(2):111–5.
Möller AJ, Fabricius L, Dahlén G, et al. Influence on periapical tissues of indigenous oral bacteria and necrotic pulp tissue in monkeys[J]. Scand J Dent Res. 1981;89(6):475–84.
Nair PN. On the causes of persistent apical periodontitis: a review[J]. Int Endod J. 2006;39(4):249–81.
Jang Y, Hong HT, Roh BD, et al. Influence of apical root resection on the biomechanical response of a single-rooted tooth: a 3-dimensional finite element analysis[J]. J Endod. 2014;40(9):1489–93.
Zelic K, Vukicevic A, Jovicic G, et al. Mechanical weakening of devitalized teeth: three-dimensional finite element analysis and prediction of tooth fracture[J]. Int Endod J. 2015;48(9):850–63.
Cope AL, Francis N, Wood F et al. Systemic antibiotics for symptomatic apical periodontitis and acute apical abscess in adults[J]. Cochrane Database Syst Rev, 2018, 9(9): Cd010136.
Talpos-Niculescu RM, Popa M, Rusu LC, et al. Conservative Approach in the management of large Periapical Cyst-Like lesions. A report of two Cases[J]. Med (Kaunas). 2021;57(5):497.
Lin LM, Ricucci D, Lin J, et al. Nonsurgical root canal therapy of large cyst-like inflammatory periapical lesions and inflammatory apical cysts[J]. J Endod. 2009;35(5):607–15.
Furuya Y, Huang SH, Takeda Y, et al. Fracture strength and stress distributions of pulpless premolars restored with fiber posts[J]. Dent Mater J. 2014;33(6):852–8.
Huumonen S, Ørstavik D. Radiographic follow-up of periapical status after endodontic treatment of teeth with and without apical periodontitis[J]. Clin Oral Investig. 2013;17(9):2099–104.
Meirinhos J, Martins JNR, Pereira B, et al. Prevalence of apical periodontitis and its association with previous root canal treatment, root canal filling length and type of coronal restoration - a cross-sectional study[J]. Int Endod J. 2020;53(4):573–84.
Lisiak-Myszke M, Marciniak D, Bieliński M, et al. Application of finite element analysis in oral and maxillofacial Surgery-A literature Review[J]. Mater (Basel). 2020;13(14):3063.
Han T, Chen K, Cao R, et al. Influence of post-core material and cement peculiarities on stress of post-cores under ultrasonic vibration: a three-dimensional finite element analysis[J]. Int Endod J. 2020;53(12):1696–704.
Holmes DC, Diaz-Arnold AM, Leary JM. Influence of post dimension on stress distribution in dentin[J]. J Prosthet Dent. 1996;75(2):140–7.
Bucchi C, Marcé-Nogué J, Galler KM, et al. Biomechanical performance of an immature maxillary central incisor after revitalization: a finite element analysis[J]. Int Endod J. 2019;52(10):1508–18.
Eom JW, Lim YJ, Kim MJ, et al. Three-dimensional finite element analysis of implant-assisted removable partial dentures[J]. J Prosthet Dent. 2017;117(6):735–42.
Rees JS, Jacobsen PH. Elastic modulus of the periodontal ligament[J]. Biomaterials. 1997;18(14):995–9.
Dal Piva AM, O, Tribst JPM, Souza R, et al. Influence of alveolar bone loss and cement layer thickness on the Biomechanical Behavior of Endodontically treated Maxillary incisors: a 3-dimensional finite element Analysis[J]. J Endod. 2017;43(5):791–5.
Hu J, Dai N, Bao Y, et al. Effect of different coping designs on all-ceramic crown stress distribution: a finite element analysis[J]. Dent Mater. 2013;29(11):e291–8.
Wang J, Du L, Fu Y, et al. ZnO nanoparticles inhibit the activity of Porphyromonas gingivalis and Actinomyces naeslundii and promote the mineralization of the cementum[J]. BMC Oral Health. 2019;19(1):84.
Ma N, Yang D, Okamura H, et al. Involvement of interleukin–23 induced by Porphyromonas endodontalis lipopolysaccharide in osteoclastogenesis[J]. Mol Med Rep. 2017;15(2):559–66.
Chan CP, Tseng SC, Lin CP, et al. Vertical root fracture in nonendodontically treated teeth–a clinical report of 64 cases in Chinese patients[J]. J Endod. 1998;24(10):678–81.
Maalouf EM, Gutmann JL. Biological perspectives on the non-surgical endodontic management of periradicular pathosis[J]. Int Endod J. 1994;27(3):154–62.
Ali M. The principles of endodontics. edition[J] BDJ. 2013;215:56–6. 2.
Wolf TG, Anderegg AL, Wierichs RJ, et al. Root canal morphology of the mandibular second premolar: a systematic review and meta-analysis[J]. BMC Oral Health. 2021;21(1):309.
Chai H, Tamse A. Vertical Root fracture in Buccal roots of bifurcated Maxillary premolars from Condensation of Gutta-percha[J]. J Endod. 2018;44(7):1159–63.
Yang J, Han F, Chen C, et al. Comparison of stress distribution between zirconia/alloy endocrown and CAD/CAM multi-piece zirconia post-crown: three-dimensional finite element analysis[J]. Clin Oral Investig. 2022;26(7):5007–17.
Mattos CM, Las Casas EB, Dutra IG, et al. Numerical analysis of the biomechanical behaviour of a weakened root after adhesive reconstruction and post-core rehabilitation[J]. J Dent. 2012;40(5):423–32.
Ng YL, Mann V, Rahbaran S, et al. Outcome of primary root canal treatment: systematic review of the literature -- part 2. Influence of clinical factors[J]. Int Endod J. 2008;41(1):6–31.
Cleghorn BM, Christie WH, Dong CC. The root and root canal morphology of the human mandibular second premolar: a literature review[J]. J Endod. 2007;33(9):1031–7.
Ying S, Chen S, Wang S, et al. Outcome of teeth restored with CAD/CAM zirconium dioxide post-cores: a retrospective study with a follow-up period of 3–6 years[J]. BMC Oral Health. 2022;22(1):236.
Zhang Y, Lawn BR. Evaluating dental zirconia[J]. Dent Mater. 2019;35(1):15–23.
Lin J, Lin Z, Zheng Z. Effect of different restorative crown design and materials on stress distribution in endodontically treated molars: a finite element analysis study[J]. BMC Oral Health. 2020;20(1):226.
Pjetursson BE, Valente NA, Strasding M, et al. A systematic review of the survival and complication rates of zirconia-ceramic and metal-ceramic single crowns[J]. Clin Oral Implants Res. 2018;29(Suppl 16):199–214.
Belli S, Eraslan O, Eskitascioglu G. Effect of Root filling on stress distribution in Premolars with Endodontic-Periodontal lesion: a Finite Elemental Analysis Study[J]. J Endod. 2016;42(1):150–5.
Bürklein S, Schäfer E. Minimally invasive endodontics[J]. Quintessence Int. 2015;46(2):119–24.
Chai H, Tamse A. Fracture mechanics analysis of vertical root fracture from condensation of gutta-percha[J]. J Biomech. 2012;45(9):1673–8.
Kandemir Demirci G, Kaval ME, Güneri P, et al. Treatment of immature teeth with nonvital pulps in adults: a prospective comparative clinical study comparing MTA with ca(OH)(2)[J]. Int Endod J. 2020;53(1):5–18.
Forberger N, Göhring TN. Influence of the type of post and core on in vitro marginal continuity, fracture resistance, and fracture mode of lithia disilicate-based all-ceramic crowns[J]. J Prosthet Dent. 2008;100(4):264–73.
Iaculli F, Rengo C, Lodato V, et al. Fracture resistance of endodontically-treated maxillary premolars restored with different type of posts and direct composite reconstructions: a systematic review and meta-analysis of in vitro studies[J]. Dent Mater. 2021;37(9):e455–84.
Mezzomo LA, Corso L, Marczak RJ, et al. Three-dimensional FEA of effects of two dowel-and-core approaches and effects of canal flaring on stress distribution in endodontically treated teeth[J]. J Prosthodont. 2011;20(2):120–9.
Zhang X, Pei X, Pei X, et al. Success and Complication Rates of Root-filled Teeth restored with Zirconia posts: a critical Review[J]. Int J Prosthodont. 2019;32(5):411–9.
Chiba A, Hatayama T, Kainose K, et al. The influence of elastic moduli of core materials on shear stress distributions at the adhesive interface in resin built-up teeth[J]. Dent Mater J. 2017;36(1):95–102.
Jiang Q, Huang Y, Tu X, et al. Biomechanical properties of First Maxillary molars with different endodontic cavities: a finite element Analysis[J]. J Endod. 2018;44(8):1283–8.
Tribst JPM, Dal Piva AM, O, Madruga CFL, et al. Endocrown restorations: influence of dental remnant and restorative material on stress distribution[J]. Dent Mater. 2018;34(10):1466–73.
Correia AM, O, Pereira VEM, Bresciani E, et al. Influence of cavosurface angle on the stress concentration and gaps formation in class V resin composite restorations[J]. J Mech Behav Biomed Mater. 2019;97:272–7.
Bodic F, Hamel L, Lerouxel E, et al. Bone loss and teeth[J]. Joint Bone Spine. 2005;72(3):215–21.
Ye ZY, Ye H, Yu XX, et al. Timing selection for loosened tooth fixation based on degree of alveolar bone resorption: a finite element analysis[J]. BMC Oral Health. 2022;22(1):328.
Baek SH, Lee WC, Setzer FC, et al. Periapical bone regeneration after endodontic microsurgery with three different root-end filling materials: amalgam, SuperEBA, and mineral trioxide aggregate[J]. J Endod. 2010;36(8):1323–5.
Pirani C, Camilleri J. Effectiveness of root canal filling materials and techniques for treatment of apical periodontitis: a systematic review[J]. Int Endod J, 2022.
Neto MA, Roseiro L, Messias A, et al. Influence of Cavity geometry on the fracture strength of Dental restorations: finite element Study[J]. Appl Sci. 2021;11(9):4218.
Santos JM, Diogo P, Dias S, et al. Long-term outcome of Nonvital Immature Permanent Teeth treated with apexification and corono-Radicular Adhesive Restoration: a Case Series[J]. J Endod. 2022;48(9):1191–9.
Acknowledgements
Not applicable.
Funding
This study was supported by the Zhejiang Provincial Medical and Health Science and Technology Program General Project (grant number 2023KY916), Wenzhou Science and Technology Bureau (H20220011), National Natural Science Foundation of China (grant number 81870757 and 81901015), Zhejiang Provincial Natural Science Foundation of China / Outstanding Youth Science Foundation (grant number LR21H140002), Zhejiang Provincial Natural Science Foundation of China (grant number LY21H140003), Wenzhou Science and Technology Bureau (grant numbers Y2020116 and Y20190102), Wenzhou Major Scientific and Technological Innovation Project (grant number ZY2022022), Zhejiang Province General Research Project (grant number Y202249092). Funding body did not have any role in the design of the study, collection, analysis and interpretation of the data or in the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
ZSF, HSB and DX have conceived the experiments; SXY, WYT, ZQH, WJ, WLM, CYG, WYL, WMH and CL were involved in data collection; CSM has analyzed the results and wrote the manuscript; YZY and HXH has built the finite element models. All authors have read and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were approved by the Ethics Committee of the School and Hospital of Stomatology, Wenzhou Medical University (Approval Number: WYYKQ2022022), and conducted in accordance with the 2013 revised version of the Declaration of Helsinki. Informed consent was obtained from the individual participant included in the study.
Consent for publication
Not applicable. In this study there was no details, images, or videos relating to an individual person that needed to be agreed to publish.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, S., Hong, X., Ye, Z. et al. The effect of root canal treatment and post-crown restorations on stress distribution in teeth with periapical periodontitis: a finite element analysis. BMC Oral Health 23, 973 (2023). https://doi.org/10.1186/s12903-023-03612-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03612-9