
Abstract
Background
This study compared the area and minimal section of the nasal cavity, nasopharynx, oropharynx, and hypopharynx in cases treated with different methods of microimplant-assisted expansion.
Methods
Based on a pilot study to calculate the sample size, 30 patients with transverse maxillary deficiency over 14 years of age were retrospectively selected. These patients had received two different types of microimplant-assisted maxillary expansion treatment (MARPE and BAME). The patient underwent Cone-Beam computed tomography (CBCT) before and after treatment (mean time 1.5 months) with MARPE or BAME and upper airway measurements (volume and minimum cross-sectional area) were taken to assess upper airways changes and compare changes between the groups. A paired sample t-test was performed to evaluate the T0-T1 change of airway measurements obtained with MARPE and BAME, and a student t-test to compare changes in airway measurements between MARPE and BAME.
Results
This investigation shows a statistically significant increase in total nasopharyngeal airway volume (0.59 ± 1.42 cm3; p < 0.01), total oropharyngeal airway volume (3.83 ± 7.53 cm3; p < 0.01) and minimum oropharyngeal cross-section (53.23 ± 126.46 mm2; p < 0.05) in all cases treated with micro-screw assisted expansion. The minimal cross-sectional area of the oropharynx ((79.12 ± 142.28 mm2; p < 0.05) and hypopharynx (59.87 ± 89.79 mm2; p < 0.05) showed significant changes for cases treated with BAME. As for the comparison between cases treated with MARPE and BAME, no differences in upper airway changes have been observed, except for the minimum cross-sectional area of the nasal cavity, which increases for MARPE (52.05 ± 132.91 mm2) and decreases for BAME (-34.10 ± 90.85 mm2).
Conclusions
A significant increase in total area and minimal section at the level of nasopharynx and oropharynx was observed in cases treated with BAME. Regarding the comparison of MARPE and BAME treatments, no differences were found in the total airway volume and minimal section in upper airway except for the minimum cross section of the nasal cavity that increases for MARPE and decreases for BAME.
Similar content being viewed by others


Background
Posterior crossbite is a malocclusion present in 5% of the world’s population with permanent dentition [1, 2]. Rapid palatal expansion (RPE) in adults causes a purely orthodontic expansion. Dental effects include increased labiolingual angulation of the molars [3, 4]. This limitation is due to the mid-palatal suture ossification, which makes the separation of hemimaxillary portions impossible with tooth-supported separators [3]. The effects of RPE in the upper airway in young patients [5,6,7,8,9] and adult patients [10, 11] have also been described.
The classic approach to posterior crossbite in adults has been Surgically Assisted Rapid Palatal Expansion (SARPE) [12,13,14,15]. This approach involves carrying out a surgical separation of the already ossified mid-palatal suture. By means of an intraoral expansion device, the skeletal transverse dimension can be increased.
The Microimplant-Assisted Rapid Palatal Expansion (MARPE) technique has been widely described in the literature [16,17,18,19,20,21,22] and is characterized by a reduction of the excessive load exerted by conventional appliances on the labial periodontal ligament of the teeth used as anchorage. It consists of a tooth-bone borne device with 2–4 bicortical microscrews from the palatal cortical bone to the nasal floor as a retention, placed in the posterior area of the palate, regardless of the age or sex of the patient. Bone-Anchored Maxillary Expansion (BAME) therapy has recently been described for the cases in which less dental effect is desired [23, 24]. With this therapy the activation forces are directed directly to the basal bone.
Rapid palatal expansion has been reported to confer significant benefits to patients’ airway [5,6,7,8, 10,11,12, 22, 25]. In particular, MARPE has been shown to increase the transverse dimension and volume of the upper airway [5, 6, 8, 10, 23], increased nasal width [5, 26, 27], improved airflow [8, 24, 28] and decreased respiratory resistance [24, 27]. Such effects have been reported in adults that underwent SARPE [11]. However, there is a dearth of information pertaining to different MARPE therapies; Bazzani et al. [29] compared skeletal changes in patients treated with MARPE and BAME with microimplants that were placed in different ways.
This investigation had two primary objectives. One was to analyze and compare the area and minimal section of the nasal cavity, nasopharynx, oropharynx, and hypopharynx for different bone-separation therapies. The second was to compare the area and minimal section of the nasal cavity, nasopharynx, oropharynx, and hypopharynx for MARPE- and BAME-type separation devices.
Our findings provide orthodontists with important information about expansion therapies that could most benefit patients’ upper airways.
Materials and methods
Design and participants
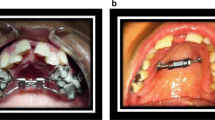
Patient data were analyzed retrospectively from September 2021 to September 2022. Data were exploited from September 2022 to February 2023. These patients were undergoing treatment with MARPE or BAME in a private dental clinic (Clinic Athenea Dental Institute). MARPE technique consists of a tooth-bone-borne appliance with a retention using four bicortical microscrews from the palatal cortical bone to the nasal floor (Fig. 1). In 2013, BAME concept described by Winsauer et al. [23] was introduced (Fig. 2). It is an expansion screw attached to four or six microimplants in the palatal area without tooth support.

Pre and postexpansion MARPE device design

Pre and postexpansion BAME device design
The inclusion criteria of the study were patients with maxillary compression without counter-indications for surgery and who had undergone microimplant-assisted maxillary expansion treatment. The exclusion criteria from the study were patients with craniofacial malformations, patients with fissured palate. All patients were informed of the orthodontic procedure with the potential risks and benefits, and an informed consent was obtained to undergo treatment and be included in the study. The age of inclusion was set at 14 years of age or older, since it is considered more complicated to perform a conventional separation after that age. These are the subjects in which a microimplant-assisted expansion is indicated [30,31,32]. Demographics and sample images were used and the information was anonymized. The study protocol was reviewed and approved by the Ethics Committee of the Rey Juan Carlos University, with internal number (1504202110721).
The sample size was calculated using Jamovi 2.3.18 assuming a study power of 80% and an alpha error of 5%. As there were no previous studies comparing dimensional changes in the upper airway comparing BAME and MARPE, sample size calculations were based on the results of a pilot study performed in ten patients. The calculated mean ± standard deviation (SD) of the total nasopharyngeal volume change of BAME and MARPE was 1.33 cm3 ± 2.6 and 0.05 cm3 ± 1.3, respectively. Based on comparison of means, using two-tailed test, it was calculated that accepting an alpha risk of 0.1 and a beta risk of 0.2 in a bilateral contrast, 13 subjects per group are required to detect a difference equal to or greater than 1.28 cm3 units. The common standard deviation is assumed to be 1.3 cm3. This was eventually increased to 15 per group, bringing the total sample size required to 30 patients.
Procedure and measurements
Palalign® Round Head Type microimplants (Osteonic Co. Ltd., Seoul, Republic of Korea), made of Ti6Al4V alloy, with a 1.8 mm diameter and lengths of 10, 12, 14, or 16 mm, depending on the case, were used to ensure bicortical fixation, thus increasing stability and reducing the risk of microimplant deformation and fracture [29]. All devices were digitally designed, and the placement of microscrews was guided digitally to minimize clinical placement errors [33]. The Power MARPE Type 1 screw (Osteonic Co. Ltd., Seoul, Republic of Korea) was used, with an activation rate of 4 turns per day until the interincisal diastema appeared, and then 2 turns per day until the overcorrection of 1.5 mm per side was achieved. All treatments were performed by the same orthodontist.
The patient was subjected to a CT-type radiographic recording (NewTom Giano HR with 300 μm voxel size and a 16 × 18 cm FOV) before and after MARPE or BAME treatment, and the following indicators were calculated on that 3D X-ray before (T0) and after treatment (T1) to confirm the midpalatal suture opening to avoid the surgery. The mean time between measurements was 1.5 months.
For the study of the upper airway, it is anatomically divided (Fig. 3) according to the tomographic description of Smith et al. [26] The division is performed in the nasal cavity, nasopharynx, oropharynx and hypopharynx in the Cone-Beam Computed Tomography (CBCT) (Table 1). It is not acceptable to use 2D radiography because of the overlapping structures described in the literature [28].

Anatomical regions of the upper airway: (A) Nasal cavity, (B) Nasopharynx, (C) Oropharynx, (D) Hypopharynx
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences version 28.0 for Windows (SPSS, IBM, Armonk, NY). A descriptive analysis was carried out to expose the details of the sample such as age, sex, type of appliance and airway measurements. Three measurements were also carried out for each indicator and for each investigation time, and the Measurement Error (ME) was calculated. Measurements were repeated after two weeks to assess intraexaminer reliability using the intraclass correlation coefficient (ICC). The ICC was calculated considering ICC < 0.4 as low, between 0.4 and 0.75 as acceptable and > 0.75 as high. The Shapiro-Wilks test is performed to check the normality of the variables. Finding a non-significant p-value and therefore establishing parametric tests. Subsequently, a paired sample t-test was performed to evaluate the T0-T1 change of airway measurements obtained with MARPE and BAME, and a student t-test to compare changes in airway measurements between MARPE and BAME. In addition, Cohen's d was used for the effect of the sample in the analysis of the differences of the means with the t-test. A measure with low effect was considered d ≈ 0.2, medium d ≈ 0.5 and high d ≈ 0.8 [34].
Results
General descriptive analysis
Thirty patients were included in our analysis. The MARPE technique was used in 15 patients (50%), and the BAME technique was used in 15 patients (50%). Thirteen of the patients were men and 17 were women. The mean age of the cohort was 21.8 ± 6.0 years. The youngest patient was 14 years old, and the oldest patient was 34 years old.
Microimplant-Assisted Rapid Palatal Expansion therapy was used in 6 of the male subjects, and BAME was used in the remaining 7. Microimplant-Assisted Rapid Palatal Expansion therapy was used in 9 of the female subjects, and BAME was used in the remaining 6. There were no differences in gender distribution (X (1) = 0.136; p = 0.713). We evaluated the age-related characteristics of the two groups at T0 and found no significant differences (MARPE group: 20.53 ± 5.74 years; BAME group: 23.07 ± 6.21 years; t = 1.16, p = 0.256).
We also evaluated airway differences at T0: NCTAV (p = 0.879); NCMCS (p = 0.493); NPTAV (p = 0.623); NPMCS (p = 0.123); OPTAV (p = 0.523); OPMCS (p = 0.600); HPTAV (p = 0.154); HPMCS (p = 0.606). No statistically significant differences were found between the two groups at T0 (ICC > 0.9).
Comparison of volumetric measurements at T0 – T1 throughout the sample
Table 2 lists total airway volume and minimum airway cross-section at T0 and T1. Increases in NCTAV, NCMCS, NPMCS, HPTAV and HPMCS were observed, but the differences were not statistically significant. However, statistically significant increases were observed between T0 and T1 for OPTAV (p < 0.01), OPMCS (p < 0.05) and NPTAV (p < 0.05).
Comparison of volumetric measurements at T0-T1 in patients treated with MARPE and BAME
Table 3 lists the measurements obtained at T0 and T1 for patients treated with MARPE. An increase was found in NCTAV, NCMCS, NPTAV, NPMCS, OPTAV, OPMCS and HPTAV, but none of the differences were statistically significant.
Table 4 lists the measurements obtained from the BAME-treated patients at T0 and T1. An increase that was not statistically significant was observed in all study variables; the exception was NCMCS, which decreased.
Table 5 compares data from patients treated with MARPE and BAME for T0-T1. For both the MARPE and BAME therapies, there was an increase in all of the indicators except for two: the minimum cross section of the hypopharynx for MARPE, which decreased slightly, and the minimum cross section of the nasal cavity for BAME, which also decreased. We found differences between MARPE and BAME at T0-T1 in terms of the minimum cross section of the nasal cavity, which increased for MARPE (52.05 ± 132.91 mm2) and decreased for BAME (-34.10 ± 90.85 mm2).
Discussion
MARPE and BAME are microimplant-assisted separators techniques indicated in cases of transverse maxillary deficiency. The primary adverse effect associated with MARPE is the buccolingual angulation (BLA) of the posterior teeth [35]. Additionally, increased molar torque has been linked to bone dehiscence with MARPE [36]. CBCT studies have revealed alterations in molar BLA following treatment with either MARPE or BAME [17, 24, 35, 37, 38]. Other factors, such as root resorption of the first molars, have been examined in prior studies [39], and root resorption has been revealed in teeth not directly linked to the appliance. Nevertheless, cases treated with skeletal-supported appliances exhibited reduced levels of resorption [40].
The objectives of this study were to investigate the volumetric and minimal section changes of the upper airway of patients with maxillary compression treated with MARPE and BAME. The different measurements were taken in the CBCT carried out before (T0) and after (T1) the maxillary expansion therapy. Other methodologies have been described in the literature, including upper airway aerodynamics [41] and superimposition with semi-automatic software [42]. Lo Giudice et al. [42] compared 20 CBCT records by superimposition with semi-automatic software and obtained proper results in terms of accuracy and efficiency.
The volumetric changes that we recorded in patients treated with MARPE were larger than those obtained in other studies [11, 43, 44]. Li et al. [10] performed a MARPE therapy on 22 patients and also obtained a volumetric increase of the nasal cavity of 2.92 ± 4.97 cm3. That increase was slightly smaller than what we obtained (3.03 ± 7.45 cm3). We noted a significant increase in the size of the nasal cavity and nasopharynx observed one and a half months after MARPE and BAME. However, further research is required to examine the enduring stability of these changes. It was not possible to compare the volumetric changes in the remaining topographic areas of the upper airway between both studies because different anatomical boundaries were used.
The volumetric changes that we recorded in the nasopharynx for both MARPE- and BAME-treated cases exhibited a slight increase. That finding is consistent with the published literature [10, 43,44,45,46]. Kim et al. [43] performed MARPE therapy on 14 adult patients and also obtained a volumetric increase of 0.64 ± 0.82 cm3 at the level the nasopharynx. That increase is slightly larger than what we obtained (0.16 ± 1.46 cm3). Unfortunately, the anatomical boundaries that Kim et al. used differed slightly from ours. Variations in the volumetric changes between these two studies may be attributed to changes in the placement location of the four micro-implants; they were more posterior in our study.
We recorded changes at the oropharynx level of 1.66 ± 5.63 cm3. That is consistent with the findings of previous studies [44, 45]. However, Yi et al. [46] reported a decrease of 1.08 ± 5.47 cm3 in a sample of 19 young adult patients who underwent BAME. But it is important to note that this change was not statistically significant. The activation rate used by Yi et al. was much slower than the one we used.
An increase in the hypopharynx was also observed following both MARPE and BAME therapies, but the difference was not statistically significant. Tang et al. [45] performed MARPE on 30 adult patients and performed CBCT prior to the expansion and after 3 months of retention. These authors recorded a volumetric decrease at the level of the hypopharynx. However, that study was carried out in a different way than ours; Tang et al. placed the anatomical limit between the hypopharynx and oropharynx at the tip of the epiglottis. Our results revealed a statistically significant increase in air volume at the nasopharynx and oropharynx level in cases treated with BAME.
This study does have limitations. First of all, our sample size was small and was characterized by a wide spread of ages. Also it is necessary to take into consideration that sample groups are different. Second, our observational period was relatively short (1.5 months); taking measurements after device removal may be useful to corroborate our findings. Additionally, changes in airway could have been studied using dynamic measures such as spirometry, peak expiratory and inspiratory flow or computational fluid dynamics. In addition, there was possible bias that derived from positioning the patients’ heads during the X-rays.
The results of this study have important implications for orthodontists. Microimplant-assisted separation devices can yield increases in the upper airway. However, there do not appear to be any statistically significant differences between MARPE and BAME therapies in terms of airway improvement; both therapies yielded similar results (with the exception of NCMCS).
Conclusions
-
An increase in total area and minimal section at the level of nasopharynx and oropharynx was observed in cases treated with microimplant-assisted expansion.
-
No differences were found between MARPE and BAME treatments in terms of total airway volume and minimal section of the nasal cavity; the exception was NCMCS, which increased for MARPE and decreased for BAME.
Availability of data and materials
All of the material is owned by the authors and/or no permissions are required. The datasets generated during and analyzed during the current study are not publicly available due to [national data protection law] but are available from the corresponding author on reasonable request.
Abbreviations
- RPE:
-
Rapid Palatal Expansion
- SARPE:
-
Surgical-Assisted Rapid Palatal Expansion
- MARPE:
-
Microimplant-Assisted Rapid Palatal Expansion
- BAME:
-
Bone-Anchored Maxillary Expansion
- CBCT:
-
Cone-Beam Computed Tomography
- NCTAV:
-
Nasal Cavity Total Air Volume
- NCMCS:
-
Nasal Cavity Minimum Cross-Section
- NPTAC:
-
Nasopharynx Total Air Volume
- NPMCS:
-
Nasopharynx Nasal Cavity Minimum Cross-Section
- OPTAC:
-
Oropharynx Total Air Volume
- OPMCS:
-
Oropharynx Nasal Cavity Minimum Cross-Section
- HPTAV:
-
Hypopharynx Total Air Volume
- HPMCS:
-
Hypopharynx Nasal Cavity Minimum Cross-Section
- ICC:
-
Intraclass Correlation Coeficieny
- ME:
-
Measurement Error
References
Lombardo G, Vena F, Negri P, Pagano S, Barilotti C, Paglia L, et al. Oral health status and Unmet Restorative Treatment Needs (UTN) in disadvantaged migrant and not migrant children in Italy. Eur J Paediatr Dent. 2019;20(1):10–4.
Alhammadi MS, Halboub E, Fayed MS, Labib A, El-Saaidi C. Global distribution of malocclusion traits: A systematic review. Dental Press J Orthod. 2018;23(6):e1-10.
Lee RJ, Moon W, Hong C. Effects of monocortical and bicortical mini-implant anchorage on bone-borne palatal expansion using finite element analysis. Am J Orthod Dentofacial Orthop. 2017;151(5):887–97.
Moon HW, Kim MJ, Ahn HW, Kim SJ, Kim SH, Chung KR, et al. Molar inclination and surrounding alveolar bone change relative to the design of bone-borne maxillary expanders: A CBCT study. Angle Orthod. 2020;90(1):13–22.
Doruk C, Sökücü O, Sezer H, Canbay EI. Evaluation of nasal airway resistance during rapid maxillary expansion using acoustic rhinometry. Eur J Orthod. 2004;26(4):397–401.
Storto CJ, Garcez AS, Suzuki H, Cusmanich KG, Elkenawy I, Moon W, et al. Assessment of respiratory muscle strength and airflow before and after microimplant-assisted rapid palatal expansion. Angle Orthod. 2019;89(5):713–20.
Fastuca R, Perinetti G, Zecca PA, Nucera R, Caprioglio A. Airway compartments volume and oxygen saturation changes after rapid maxillary expansion: A longitudinal correlation study. Angle Orthod. 2015;85(6):955–61.
Sadeghian S, Ghafari R, Feizbakhsh M, Dadgar S. Dimensional changes of upper airway after rapid maxillary expansion evaluated with cone beam computed tomography. Orthod Waves. 2016;75(1):10–7.
El H, Palomo JM. Three-dimensional evaluation of upper airway following rapid maxillary expansion: a CBCT study. Angle Orthod. 2014;84(2):265–73.
Li Q, Tang H, Liu X, Luo Q, Jiang Z, Martin D, et al. Comparison of dimensions and volume of upper airway before and after mini-implant assisted rapid maxillary expansion. Angle Ortho. 2020;90(3):432–41.
Deeb W, Hansen L, Hotan T, Hietschold V, Harzer W, Tausche E. Changes in nasal volume after surgically assisted bone-borne rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2010;137(6):782–9.
de Oliveira CB, Ayub P, Ledra IM, Murata WH, Suzuki SS, Ravelli DB, et al. Microimplant assisted rapid palatal expansion vs surgically assisted rapid palatal expansion for maxillary transverse discrepancy treatment. Am J Orthod Dentofacial Orthop. 2021;159(6):733–42.
Koudstaal MJ, Smeets JBJ, Kleinrensink GJ, Schulten AJM, van der Wal KGH. Relapse and Stability of Surgically Assisted Rapid Maxillary Expansion: An Anatomic Biomechanical Study. J Oral Maxillofac. 2009;67(1):10–4.
Asscherickx K, Govaerts E, Aerts J, Vande VB. Maxillary changes with bone-borne surgically assisted rapid palatal expansion: A prospective study. Am J Orthod Dentofacial Orthop. 2016;149(3):374–83.
Kayalar E, Schauseil M, Kuvat SV, Emekli U, Firatli S. Comparison of tooth-borne and hybrid devices in surgically assisted rapid maxillary expansion: A randomized clinical cone-beam computed tomography study. J Craniomaxillofac Surg. 2016;44(3):285–93.
Choi SH, Shi KK, Cha JY, Park YC, Lee KJ. Nonsurgical miniscrew-Assisted rapid maxillary expansion results in acceptable stability in young adults. Angle Orthod. 2016;86(5):713–20.
Kapetanovic A, Theodorou CI, Bergé S, Schols JGJH, Xi T. Efficacy of Miniscrew-Assisted Rapid Palatal Expansion (MARPE) in late adolescents and adults: a systematic review and meta-analysis. Eur J Orthod. 2021;43(3):313–23.
Carlson C, Sung J, McComb RW, MacHado AW, Moon W. Microimplant-assisted rapid palatal expansion appliance to orthopedically correct transverse maxillary deficiency in an adult. Am J Orthod Dentofacial Orthop. 2016;149(5):716–28.
Garcez AS, Suzuki SS, Storto CJ, Cusmanich KG, Elkenawy I, Moon W. Effects of maxillary skeletal expansion on respiratory function and sport performance in a para-athlete – A case report. Phys Ther Sport. 2019;36:70–7.
Nojima LI, Nojima M da CG, da Cunha AC, Guss NO, Sant’anna EF. Mini-implant selection protocol applied to MARPE. Dental Press J Orthod. 2018;23(5):93–101.
Carneiro da Cunha A, Lee H, Nojima LI, Nojima M da CG, Lee KJ. Miniscrew-assisted rapid palatal expansion for managing arch perimeter in an adult patient. Dental Press J Orthod. 2017;22(3):97–108.
Yavan MA, Kaya S, Kervancioglu P, Kocahan S. Evaluation of effects of a modified asymmetric rapid maxillary expansion appliance on the upper airway volume by cone beam computed tomography. J Dent Sci. 2021;16(1):58–64.
Winsauer H, Vlachojannis J, Winsauer C, Ludwig B, Walter A. A bone-borne appliance for rapid maxillary expansion. J Clin Orthod. 2013;47(6):375–88.
Lagravère MO, Gamble J, Major PW, Heo G. Transverse dental changes after tooth-borne and bone-borne maxillary expansion. Int Orthod. 2013;11(1):21–34.
El H, Palomo JM. An airway study of different maxillary and mandibular sagittal positions. Eur J Orthod. 2013;35(2):262–70.
Smith T, Ghoneima A, Stewart K, Liu S, Eckert G, Halum S, et al. Three-dimensional computed tomography analysis of airway volume changes after rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2012;141(5):618–26.
Johal A, Patel SI, Battagel JM. The relationship between craniofacial anatomy and obstructive sleep apnoea: A case-controlled study. J Sleep Res. 2007;16(3):319–26.
Tso HH, Lee JS, Huang JC, Maki K, Hatcher D, Miller AJ. Evaluation of the human airway using cone-beam computerized tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(5):768–76.
Bazzani M, Cevidanes LHS, Al Turkestani NN, Annarumma F, McMullen C, Ruellas ACO, et al. Three-dimensional comparison of bone-borne and tooth-bone-borne maxillary expansion in young adults with maxillary skeletal deficiency. Orthod Craniofac Res. 2023;26(2):151–62.
Angelieri F, Cevidanes LHS, Franchi L, Gonçalves JR, Benavides E, McNamara JA. Midpalatal suture maturation: Classification method for individual assessment before rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2013;144(5):759–69.
Persson M, Thilander B. Palatal suture closure in man from 15 to 35 years of age. Am J Orthod. 1977;72(1):42–52.
Korbmacher H, Schilling A, Püschel K, Amling M, Kahl-Nieke B. Age-dependent three-dimensional micro-computed tomography analysis of the human midpalatal suture. J Orofac Orthop. 2007;68(5):364–76.
Ronsivalle V, Venezia P, Bennici O, D’Antò V, Leonardi R, Giudice A Lo. Accuracy of digital workflow for placing orthodontic miniscrews using generic and licensed open systems. A 3d imaging analysis of non-native .stl files for guided protocols. BMC Oral Health. 2023;23(1):494
Cohen JM. Statistical power analysis for the behavioral sciences. New York: Lawrence Eribaum Associates Publishers; 1988.
Garib DG, Henriques JFC, Janson G, de Freitas MR, Fernandes AY. Periodontal effects of rapid maxillary expansion with tooth-tissue-borne and tooth-borne expanders: A computed tomography evaluation. Am J Orthod Dentofacial Orthop. 2006;129(6):749–58.
Kim H, Park SH, Park JH, Lee KJ. Nonsurgical maxillary expansion in a 60-year-old patient with gingival recession and crowding. Korean J Orthod. 2021;51(3):217–27.
Park JJ, Park YC, Lee KJ, Cha JY, Tahk JH, Choi YJ. Skeletal and dentoalveolar changes after miniscrew-assisted rapid palatal expansion in young adults: A cone-beam computed tomography study. Korean J Orthod. 2017;47(2):77–86.
Lim HM, Park YC, Lee KJ, Kim KH, Choi YJ. Stability of dental, alveolar, and skeletal changes after miniscrew-assisted rapid palatal expansion. Korean J Orthod. 2017;47(5):313–22.
Leonardi R, Ronsivalle V, Barbato E, Lagravère M, Flores-Mir C, Lo Giudice A. External root resorption (ERR) and rapid maxillary expansion (RME) at post-retention stage: a comparison between tooth-borne and bone-borne RME. Prog Orthod. 2022;23(1).
Leonardi R, Ronsivalle V, Isola G, Cicciù M, Lagravère M, Flores-Mir C, et al. External root resorption and rapid maxillary expansion in the short-term: a CBCT comparative study between tooth-borne and bone-borne appliances, using 3D imaging digital technology. BMC Oral Health. 2023;23(1):558.
Feng X, Chen Y, Hellén-Halme K, Cai W, Shi XQ. The effect of rapid maxillary expansion on the upper airway’s aerodynamic characteristics. BMC Oral Health. 2021;21(1).
Lo Giudice A, Ronsivalle V, Gastaldi G, Leonardi R. Assessment of the accuracy of imaging software for 3D rendering of the upper airway, usable in orthodontic and craniofacial clinical settings. Prog Orthod. 2022;23(1).
Kim SY, Park YC, Lee KJ, Lintermann A, Han SS, Yu HS, et al. Assessment of changes in the nasal airway after nonsurgical miniscrew-assisted rapid maxillary expansion in young adults. Angle Orthod. 2018;88(4):435–41.
Hur JS, Kim HH, Choi JY, Suh SH, Baek SH. Investigation of the effects of miniscrew-assisted rapid palatal expansion on airflow in the upper airway of an adult patient with obstructive sleep apnea syndrome using computational fluidstructure interaction analysis. Korean J Orthod. 2017;47(6):353–64.
Tang H, Liu P, Xu Q, Hou Y, Guo J. A comparative analysis of aerodynamic and anatomic characteristics of upper airway before and after mini-implant-assisted rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2021;159(4):e301–10.
Yi F, Liu S, Lei L, Liu O, Zhang L, Peng Q, et al. Changes of the upper airway and bone in microimplant-assisted rapid palatal expansion: A cone-beam computed tomography (CBCT) study. J Xray Sci Technol. 2020;28(2):271–83.
Acknowledgements
Not applicable.
Funding
I declare that the authors have not received any type of funding for this study.
Author information
Authors and Affiliations
Contributions
J.E-N: contributed to acquisition, drafted manuscript and critically revised manuscript. MJ.G-O: Contributed to conception and design contributed to analysis and interpretation drafted manuscript and critically revised manuscript. P.E-L: contributed to acquisition, drafted manuscript and critically revised manuscript. M.R: contributed to conception and design and critically revised manuscript. All authors gave their final approval and agree to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for this study was obtained from the Ethics Commission for Research at the Rey Juan Carlos University. All methods were performed in accordance with the relevant guidelines and regulations. The informed consent procedure was approved by the Research Ethics Committee. Participants signed written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Fig. 1. CBCT measurement of the nasal cavity in T0. Fig. 2. CBCT measurement of the nasopharynx in T0. Fig. 3. CBCT measurement of the oropharynx in T0. Fig. 4. CBCT measurement of the hypopharynx in T0. Fig. 5. CBCT measurement of the nasal cavity in T1. Fig. 6. CBCT measurement of the nasopharynx in T1. Fig. 7. CBCT measurement of the oropharynx in T1. Fig. 8. CBCT measurement of the hypopharynx in T1.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Echarri-Nicolás, J., González-Olmo, M.J., Echarri-Labiondo, P. et al. Short-term outcomes in the upper airway with tooth-bone-borne vs bone-borne rapid maxillary expanders. BMC Oral Health 23, 714 (2023). https://doi.org/10.1186/s12903-023-03461-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03461-6