
Abstract
Background
The objective of this systematic review and meta-analysis was to evaluate the effects of non-surgical periodontal therapy (NSPT) on inflammatory-related cytokines/adipocytokines in periodontitis patients with or without obesity.
Methods
We followed the preferred reporting items for systematic reviews and meta-analyses statement and registered the study (CRD42022375331) in the Prospective International Register of Systematic Reviews. We screened randomized-controlled trials and controlled clinical trials from six databases up to December 2022. Quality assessment was performed with RoB-2 and ROBINS-I tools for randomized trials and non-randomized trials, respectively. Meta-analysis was carried out using a random-effect model.
Results
We included seventeen references in the systematic analysis, and sixteen in the meta-analysis. Baseline results of pro-inflammatory biomarkers, including serum interleukin (IL)-6, serum and gingival crevicular fluid (GCF), tumor necrosis factor (TNF)-a, serum C-reactive protein (CRP)/hs-CRP, and serum and GCF resistin, were higher in obesity subjects than in normal weight subjects. The effect of NSPT with respect to levels of cytokines/adipocytokines, including IL-6, TNF-a, CRP/hs-CRP, resistin, adiponectin, leptin and retinol binding protein 4 (RBP4), were then analyzed in the systematic and meta-analysis. After three months of NSPT, serum (MD = -0.54, CI = -0.62 – -0.46), and GCF (MD = -2.70, CI = -4.77 – -0.63) levels of IL-6, along with the serum RBP4 (MD = -0.39, CI = -0.68–0.10) decreased in periodontitis individuals with obesity. NSPT also improved GCF adiponectin levels after three months (MD = 2.37, CI = 0.29 – 4.45) in periodontitis individuals without obesity.
Conclusions
Obese status altered the baseline levels of cytokines/adipocytokines (serum IL-6, serum and GCF TNF-a, serum CRP/hs-CRP, and serum and GCF resistin). Then NSPT can shift the levels of specific pro-inflammatory mediators and anti-inflammatory mediators in biological fluids, both in obesity and non-obesity individuals. NSPT can reduce serum and GCF IL-6 levels together with serum RBP4 level in individuals with obesity after 3 months, besides, there is no sufficient evidence to prove that obese patients have a statistically significant decrease in the levels of other cytokines compared to patients with normal weight. NSPT can also increase GCF adiponectin level in normal weight individuals after 3 months. Our findings imply the potential ideal follow-up intervals and sensitive biomarkers for clinical bioanalysis in personalized decision-making of effect of NSPT due to patients’ BMI value.
Similar content being viewed by others

Background
Periodontitis is a chronic, multifactorial, inflammatory disease related to dysbiotic plaque biofilms and is characterized by progressive destruction of the tooth-supporting apparatus [1,2,3]. The primary clinical features of periodontitis include the loss of periodontal tissue support, and is typically identified by bleeding on probing, deepened probing depth, loss of attachment, gingival recession, halitosis, and tooth mobility [1, 4]. The present adopted periodontitis classification scheme, unlike the former single category, is based on characterization of the disease due to the multi-dimensional staging and grading system, which is a better assessment for the severity, risk-evaluation, anticipated outcome and management of the disease. Moreover, the current revised classification according to pathophysiology is categorized as periodontitis, necrotizing periodontitis and the one as the direct manifestation of systemic diseases [1]. Periodontitis is associated with the elevation of inflammatory molecules in systemic diseases and the development of several systemic co-morbidities, such as cardiovascular disease and type 2 diabetes [5, 6]. Obesity, which manifested as the accumulation of excess body fat, is another common health concern that results in a significant economic and societal burden worldwide. WHO currently accepts a body mass index of 25 kg/m2 or greater as abnormal and when BMI is 30 kg/m2 or over the objects are categorized as obese [7, 8]. Furthermore, obesity is currently recognized as a state of low-grade systemic inflammation (LGSI) [9]. Research has demonstrated negative associations between bone metabolism, periodontitis, and obesity. Clinical studies have found that obesity is correlated with reduced bone mass, which can lead to varying degrees of osteoporosis and alveolar bone resorption as present in periodontitis [7, 10]. Obese individuals also tend to have higher levels of serum inflammatory biomarkers, such as cytokines (adipokines), which are secreted from adipocytes in adipose tissues. These biomarkers include interleukins (IL-6 and IL-8), tumor necrosis factor α (TNF-α), interferon-γ (IFN-γ), C-reactive protein (CRP), monocyte chemoattractant protein-1 (MCP-1), chemerin, adiponectin, omentin, isthmin 1, nesfatin-1, leptin, retinol-binding protein 4 (RBP4), resistin, and visfatin. They modulate inflammatory, immune, and metabolic responses [11,12,13,14].
Studies have also demonstrated that the levels of the inflammatory cytokines or adipokines mentioned above exhibit varying trends of change in patients with periodontitis at different stages of the disease. The association between periodontal disease and obesity was initially discovered in obese Zucker rats by Perlstein and Bissada [15]. Moreover, recent studies and reviews have further revealed the association between obesity and periodontal disease [16,17,18]. Additionally, periodontal disease and obesity/overweight status may have a bidirectional relationship, to be specific, not only are obese/overweight individuals prone to periodontal disease, but also periodontal disease may exacerbate dyslipidemia [19,20,21]. In fact, during the local and systemic comorbid pathological condition, both periodontal tissues and adipocytes as host immune responsive cells, when triggered by pathogens, can secret higher levels of pro-inflammatory cytokines in obese individuals (such as IL-1, IL-1β, IL-6, TNF-a, etc.) to exacerbate both disease conditions [22]. Also, obesity is related to the increased susceptibility towards bacterial infection; while periodontal tissues affected by periodontal disease (a source of bacteremia) may potentially worsen the obesity condition via pathways that involve the enhanced generation of reactive oxygen species (ROS) [23, 24]. And the recent discovery revealed that the association between periodontal disease and obesity is the outcome of an overall imbalance between health and systemic health [16].
Non-surgical periodontal therapy (NSPT) remains the gold standard for managing chronic periodontitis. The removal of supragingival plaque and subgingival scaling and root planning is the gold standard non-surgical therapy. Nevertheless, the mere mechanical debridement may not eradicate all subgingival periopathogens, and the adjunctive non-surgical measures are sometimes utilized to eliminate bacterial biofilm and deposits and restore a balanced microbiota environment for periodontal health [25]. NSPT also reduces local inflammatory stimulation, decreases pocket depth, and promotes the recovery of clinical attachment by restoring highly perfused and collagen-rich connective tissues. As there is a correlation between periodontal disease and obesity, exploring the effectiveness of NSPT for obese patients with periodontitis is reasonable [26,27,28,29].
The 2017 World Workshop had demonstrated one of the issues that should be addressed in the future research was the identification of microbial, genetic, or host response‐associated biomarkers that discriminate between the periodontitis phenotypes, also the ones that can reflect whether the initiation or progression of periodontitis [1]. As far as we concern, the aforementioned cytokines seem to get involved in the mechanisms of periodontitis and obesity comorbid condition, and the levels of those cytokines before and after the NSPT are expected to provide the adjunctive measurements for the effect of the therapy and the primary prediction the role of these markers involved in the recovery of the comorbid. However, limited studies or weak evidence make it unclear whether NSPT significantly impacts clinical periodontal outcomes in obese individuals compared to non-obese individuals. Additionally, the role of related cytokines or adipokines before and after NSPT, as well as their impact on treatment outcomes, remains unclear. Therefore, the purpose of this study is to systematically review the efficacy of NSPT in managing periodontitis in both obese and non-obese individuals while considering the levels of biomarkers.
Materials and methods
Protocol and registration
This systematic review and meta-analysis were carried out in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines [30] and registered in the Prospective International Register of Systematic Reviews (PROSPERO), with approval from all authors (CRD42022375331).
Focused question and selection criteria
One specific clinical focused question was constructed according to the Participants, Interventions, Control, and Outcomes (PICO) principle [31]: “what is the efficacy of NSPT with respect to cytokine/adipocytokine levels in obese individuals? Does NSPT reduce their biofluid levels of related cytokines/ adipocytokines (IL-6, TNF-a, CRP/hs-CRP, resistin, adiponectin, leptin, and RBP4)?
-
(P) Participants: individuals with obesity and periodontitis
-
(I) Types of intervention: NSPT
-
(C) Comparison: without periodontal treatment
-
(O) Outcome: biofluid levels of related cytokines/ adipocytokines
The secondary focused question was: “what is the efficacy of NSPT with respect to cytokine/ adipocytokine levels in obese individuals compared to non-obese chronic periodontitis patients? Are obese people more responsive to treatment in cytokines/ adipocytokines levels?”
-
(P) Participants: individuals with obesity and periodontitis
-
(I) Types of intervention: NSPT
-
(C) Control intervention: NSPT in non-obese patients with chronic periodontitis
-
(O) Outcome measures: biofluid levels of cytokines/adipocytokines from measured from the baseline to the follow-up
Studies were considered eligible once they reached the following criteria: (1) Randomized clinical trials (RCTs) were deemed the most appropriate study design, along with controlled clinical trials (CCTs), for evaluating the efficacy of NSPT on cytokine/adipocytokine levels in individuals with or without obesity. (2) the study reported the association of given cytokines/ adipocytokines level with patients affected by obesity and the control group was necessary; (3) NSPT should be applied; (4) full-text were published in English. Studies were excluded once they were (1) laboratory animal studies, case–control studies, cross-sectional studies, case series, systematic reviews, literature reviews, conference abstracts; (2) studies lacking complete data on levels of targeted cytokines/adipocytokines (despite efforts to retrieve raw values from the original authors); (3) clinical analyses involving periodontitis patients with systemic conditions other than obesity or who received treatments beyond NSPT were excluded. Please refer to Table S1 for details on the inclusion and exclusion criteria.
Criteria for obesity and periodontal diagnosis
The WHO definition of obesity in adults considers measurements such as waist circumference, waist-hip ratio, and body fat [32]; we followed the WHO obesity BMI diagnostic criterion (Table 1). According to WHO criteria, individuals with BMI over 30 kg/m2 are categorized as obese [7], and BMI over 27.5 kg/m2 is the recommended BMI cut-off point for obesity in Asian populations according to the interpretation of WHO expert consultation [33]. Previous studies measured metabolic [29, 34,35,36,37,38,39,40,41] and anthropometric [34,35,36,37, 41,42,43,44,45] parameters following NSPT to determine whether participants remained classified as obese during follow-up, particularly for longer-term studies. Various definitions and criteria for periodontitis were used by different authors and were accepted for the purposes of this review. The NSPT interventions included professional oral hygiene instructions, full-mouth scaling and root planning (SRP), or SRP combined with local or systemic antimicrobial agents. No surgical procedures, such as periodontal flap surgery, were involved in the NSPT.
Information sources and search protocol
Two reviewers, Z. YW and Z. YF, conducted a systematic search for articles addressing the research question in English from 1977 to November 2022. They searched six electronic databases, including PubMed, ISI Web of Knowledge, ScienceDirect, Web of Science, Scopus, and OpenGrey, and limited the searches to the first 200 hits in Google Scholar. In addition, a manual search of the relevant literature was performed. The search strategy included keywords related to ((periodontal disease OR periodontitis OR chronic periodontitis OR adult periodontitis OR attachment loss OR aggressive periodontitis OR juvenile periodontitis) AND (root planning OR periodontal treatment OR non-surgical periodontal therapy) AND (obesity OR obese OR body mass index) AND (cytokine OR adipocytokine OR IL-6 OR TNF-a OR CRP OR hs-CRP OR resistin OR adiponectin OR leptin OR RBP4)). Any disagreements between the two reviewers were resolved by a third author, J. R.
Study selection
The reviews screened titles and abstracts based on the inclusion and exclusion criteria. Full-text articles were obtained for references that did not provide sufficient information for inclusion or exclusion based on their titles and abstracts. After removing duplicates, all articles that met the eligibility criteria were included. Any disagreements between the two reviewers were resolved through discussion and consensus with a third author (J. R). The Kappa score for this stage was 0.79, indicating substantial agreement.
Data extraction and quality assessment
The same two reviewers undertook data extraction independently. Information from the accepted studies was tabulated according to the author(s), publication year, study designs, settings, participant characteristics, sample characteristics, periodontal and obesity criteria for inclusion, and follow-up outcomes with cytokines/adipocytokines investigated. Data collection was based on the focused question addressed in the systematic review. Data on baseline and post-treatment follow-up timepoints that compared the levels of cytokines/ adipocytokines among obese and nonobese patients were also extracted and calculated. The reviewers cross-checked all extracted data, and any dissent was resolved by discussion until consensus was reached. The Kappa score was 0.89. The selected studies were assessed for quality by the reviewers using the Cochrane-advocated ROB-2 tool for assessing the risk of bias in RCTs [52]. For non-RCTs, the ROBINS-I tool was used for assessing risk of bias by looking into pre-intervention, intervention and post-intervention domains. Studies were evaluated as low risk of bias (≤ one moderate concern in the included domains, comparable), moderate (≤ four moderate concerns, credible but cannot considered comparable); serious risk of bias (at least one serious concern or multiple moderate concerns; with important problems in the design) and critical risk of bias (critical concerns or multiple serious concerns; unreliable) [46].
Synthesis of results
Studies with methodological homogeneity were pooled together in a meta-analysis using Review Manager 5.4, which was provided by the Cochrane Collaboration. We assessed statistical inconsistency and heterogeneity by examining the forest plots, Tau2, and the I2 statistics. Significance levels of overall effects were determined by Z test, and forest plots were provided to demonstrate effect sizes and the corresponding 95% CI. Between-study heterogeneity was estimated by I2 statistic, which was based on the Cochran Q statistics [47]. Additionally, unlike merely focus on I2 > 50% or not, we evaluated clinical heterogeneity to determine the appropriate effect model. Most of the included studies reported cytokine/adipokine levels in biofluids using medians. For studies that reported median and interquartile ranges, we estimated means and standard deviations through the given series estimation formulas through simulation studies provided by Wan X, McGrath, S. et al. [48, 49, 51]. The significance p value was set as 0.05.
Subgroup analysis
Fifty-four subgroup analyses were conducted based on the biomarker category, biofluid type (serum, saliva, and gingival crevicular fluid (GCF)), participant group, and time of follow-up after NSPT. Subgroup meta-analyses were performed using mean differences (MD) and 95% confidence intervals (CI). The synthesis of results instructions was followed for all subgroup analyses, and sensitivity analysis was performed.
Results
Study selection
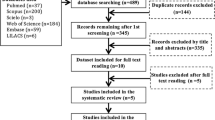
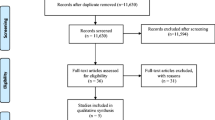
A total of 1,695 studies were identified in the electronic databases, and no additional record was found from manual searching (duplicated) or the gray literature. Initial screening of the titles and abstracts was followed to remove 925 duplicates and 737 irrelevant studies from the inclusions. Thus, 33 studies were selected for eligibility. After assessment of the full texts of the 33 articles, 16 studies were excluded, and the specific reasons were listed in Table S1 (Supplementary Information File). Seventeen studies were eventually included in the present systematic review, and sixteen were included in meta-analysis. A flowchart presenting all the above-stated phases is displayed in Fig. 1.

Flowchart presenting the search and the selection phases of the incorporated articles of the systematic review
Study characteristics
The characteristics of the 17 incorporated studies are depicted in Table 1. The studies reflected the diversity of ethnicities as they were conducted in different countries; meanwhile, all included studies were published in English. All studies consisted of a group of obese individuals with periodontitis who were treated with NSPT. As for defining parameters of obesity in the included studies, the WHO criteria with or without assistant measures such as body fat, waist-hip ratio, and so on were taken into account. Notably, given by two BMI cut-off point [7, 33] for obesity recommended by WHO as stated in the Obesity and periodontitis criterion, BMI over 27.5 kg/m2 in Asian obesity populations [33] was applied by three included studies in Asian settings [39, 53, 54]. The number of individuals in each study ranged from 40 to 231. The follow-up time of each one ranges from six weeks to two years; the majority is about three months [34,35,36,37, 39, 40, 42,43,44,45, 54,55,56] and six months [41, 42, 45, 53] after the NSPT. All studies provided related professional oral hygiene instructions and sufficient periodontal parameters at the follow-up timepoints.
NSPT and inflammatory-related cytokines/adipokines
Our systematic analysis revealed that among the various inflammatory cytokines, IL-6 and CPR/hs-CRP were the most commonly investigated by researchers. TNF-a, IL-1β, IL-10, and interferon-γ were investigated to a lesser extent. In terms of adipokines, resistin, adiponectin, and leptin were the most widely studied, while RBP4 and vastatin were studied to a lesser extent. The efficacy of NSPT in respect to each of these cytokines and adipokines in different biological fluids (serum, saliva, and GCF) are presented in Tables S2 and S3.
Evaluation of the methodological quality of the incorporated studies
According to the critical evaluation instruments used (see Supplementary Tables S4 and S5), all randomized and non-randomized studies included in this systematic review and meta-analysis showed a relatively high degree (low or moderate risk of bias) of methodological quality, however, our findings should be interpreted with caution, as most of the published studies were at moderate risk of bias. The basic methodological deficiencies resulted in moderate risk of bias were the missing data due to the dropouts of more than 5% in two studies [43, 45] during follow-up, and failure to prospectively calculate sample size in two studies [37, 41] and the low to moderate quality could be partially attributed to the inevitable presence of confounders (confounders such as unstated smoking issues, degree of pathological condition, etc.).
Non-surgical periodontal therapy and IL-6
In the subgroup analysis that compared serum levels of IL-6 (pg/mL), five studies [34, 35, 40, 42, 43] showed that the baseline IL-6 levels of people with obesity and periodontitis (OP) were higher than those of normal-weight patients with periodontitis (NP) before treatment (MD = 0.51, CI = 0.09–0.93) (Figure S1). However, there was a reduction in serum levels of IL-6 in OP individuals three months after non-surgical periodontal treatment (NSPT) compared to before treatment (MD = -0.54, CI = -0.62–-0.46) [1,2,3, 7, 8, 39, 42] (Fig. 2), while there was no difference in serum levels of IL-6 in NP individuals (MD = -0.19, CI = -0.62–0.24) [34, 35, 40, 42, 43] (Figure S2). Furthermore, at the 3-month follow-up, five studies [34, 35, 40, 42, 43] showed that serum IL-6 levels in OP patients did not differ from those in NP patients (MD = 0.42, CI = -0.06–0.90) (MD = 0.42, CI = -0.06–0.90) (Figure S3).

Subgroup analysis comparing serum levels of IL-6 before and three months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) group
In the subgroup analysis that compared GCF levels of IL-6 (pg/mL), three studies [35, 36, 42] showed no difference in IL-6 levels between OP and NP patients at baseline (MD = 0.27, CI = -0.59–1.13) (Figure S4). However, four studies [35, 36, 42, 54] demonstrated a decline in IL-6 levels in OP individuals three months after NSPT compared to before treatment (MD = -2.70, CI = -4.77–-0.63) (Fig. 3), while three studies [35, 36, 42] showed no difference in NP patients (MD = -0.60, CI = -1.38–0.18) (Figure S5). At the 3-month follow-up, three studies showed no difference in GCF IL-6 levels between OP and NP patients (MD = 0.15, CI = -0.32–0.62) [35, 36, 42] (Figure S6). With regard to the long-term effects of NSPT, three studies indicated no difference in IL-6 levels in OP patients (MD = -1.48, CI = -3.37–0.41) [35, 36, 42] (Figure S7) or NP patients (MD = -0.54, CI = -1.54–0.46) [35, 36, 42] (Figure S8) before and after therapy. Overall, four studies [35, 36, 42, 57] reported that the GCF IL-6 levels of OP patients were higher than those of normal-weight periodontitis patients in the longest follow-up time (MD = 1.69, CI = 0.21–3.17) (Fig. 4).

Subgroup analysis comparing GCF levels of IL-6 before and three months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups

Comparison of distal follow-up time GCF levels of IL-6 after non-surgical periodontal therapy among patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups
NSPT and TNF-a
In the subgroup analysis comparing serum levels of TNF-a (pg/mL), five included studies [34, 35, 40, 42, 43] suggested that the level of the OP group was higher than that of the NP group at baseline (MD = 10.36, CI = 4.58–16.15) (Figure S9). Besides, six studies [34, 35, 40, 42,43,44] indicated that there was no difference of serum TNF-a levels among OP patients before and 3 months after the NSPT (MD = -3.69, CI = -10.29–2.92) (Figure S10), also, five studies [34, 35, 40, 42, 43] indicated there was no difference in NP patients (MD = -3.16, CI = -8.79–2.48) (Figure S11). By the end of 3-month follow-up, five studies [34, 35, 40, 42, 43] suggested the serum TNF-a level of the OP group was still higher than that in NP group (MD = 8.08, CI = 4.52–11.64) (Fig. 5).

Comparison of follow-up serum levels of TNF-a three months after non-surgical periodontal therapy among patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups
As for the subgroup analysis comparing GCF levels of TNF-a (pg/mL), three included studies [35, 36, 42] suggested that the level of the OP group was higher than that in the NP group at baseline (MD = 0.38, CI = 0.17 – 0.59) (Figure S12). Four studies [35, 36, 42, 54] indicated that, for the OP group (MD = -5.49, CI = -11.01 – 0.02) (Fig. 6), or for the NP group (MD = -1.43, CI = -2.84 – 0.03) [35, 36, 42] (Figure S13), the GCF TNF-a level tended to be higher before the NSPT than at the 3-month follow-up. Meanwhile, three studies [35, 36, 42] suggested that there was no difference in GCF TNF-a level between the OP and NP groups at the 3-month follow-up (MD = 0.25, CI = -0.70 – 1.21) (Figure S14). Concerning the distal time effect, four studies [35, 36, 42, 54] indicated that there was hardly any difference before and after the longest follow-up intervals for either the OP group (MD = -5.13, CI = -10.86 – 0.59) (Figure S15) or the NP group (suggested by three studies [35, 36, 42]) (MD = -1.49, CI = -3.22 – 0.25) (Figure S16) individually. Moreover, four studies [35, 36, 42, 57] indicated that the GCF TNF-a level tended to be higher before the NSPT, while actually showing no difference compared to the longest follow-up time points (MD = 1.16, CI = -0.01 – 2.33) (Figure S17).

Subgroup analysis comparing GCF levels of TNF-a before and three months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups
NSPT and CRP/hs-CRP
As for the subgroup analysis comparing serum levels of CRP/hs-CRP (mg/L), six studies [35, 37, 40, 41, 43, 58] suggested that the level of OP group was higher than that in NP group at baseline (MD = 5.41, CI = 2.63 – 8.19) (Figure S18). In contrast, four studies [35, 37, 40, 43] suggested that there was no obvious reduction 3 months after the NSPT among OP patients (MD = -2.93, CI = -6.74 – 0.61) (Figure S19) and neither in NP group (MD = -1.39, CI = -3.57 – 0.79) [35, 37, 40, 43] (Figure S20). Further, these same four studies [35, 37, 40, 43] demonstrated that the level of OP individuals was no significant difference as compared with NP individuals 3 months after therapy in serum CRP/hs-CRP level (MD = 5.87, CI = -0.61 – 12.35) (Figure S21).
NSPT and resistin
In the subgroup analysis comparing salivary levels of resistin (ng/mL), merely two included studies [39, 53] suggested that there was no difference before and after the NSPT within the OP group (MD = -4.60, CI = -12.40–3.20) (Figure S22).
In the subgroup analysis comparing GCF levels of resistin (ng/mL), two included studies [29, 42] indicated that the baseline level of OP individuals was higher than that of NP patients (MD = 2.99, CI = 0.76–5.23) (Figure S23). Moreover, the same two studies [29, 42] suggested the GCF resistin level of OP individuals showed no difference before and after the NSPT (MD = 1.45, CI = -5.60 – 8.50) (Figure S24) as well as that among NP patients (MD = -0.71, CI = -8.14 – 6.73) [29, 42] (Figure S25) with the longest follow-up timepoints. Overall, at the end of the longest follow-up, the GCF resistance level of OP individuals were much higher than that of NP patients (MD = 5.36, CI = 4.18–5.91) [29, 42] (Figure S26).
In the subgroup analysis comparing serum levels of resistin (ng/mL), three included studies [29, 42, 55] indicated that the baseline level of OP individuals was higher than that of NP patients (MD = 4.98, CI = 0.26–9.71) (Figure S27). Nevertheless, no difference was discovered among the OP group before and after the therapy (MD = 1.03, CI = -0.70 – 2.76) [29, 42, 55] (Figure S28), nor among the NP groups with the longest follow-up (MD = -0.25, CI = -3.89–3.38) [29, 42, 55] (Figure S29). At the end of the longest follow-up, the serum resistin level of OP individuals were higher than that of NP patients (MD = 6.30, CI = 0.54–12.05) [29, 42, 55] (Figure S30).
NSPT and adiponectin
In the subgroup analysis comparing serum levels of adiponectin (ng/mL), only two included studies [42, 45] suggested that the level of the OP group was not different from that in the NP group at baseline (MD = 3.72, CI = -12.39–19.83) (Figure S31). Moreover, three studies [35, 42, 45] suggested that there was no difference before and three months after the NSPT among OP patients (MD = 0.76, CI = -1.96–3.47) (Figure S32), and the same was observed among NP groups (MD = 2.28, CI = -5.57–10.13) [35, 42, 45] (Figure S33). Overall, three studies [35, 42, 45] concluded that there was no difference in serum adiponectin level between OP and NP individuals three months after the NSPT (MD = 0.63, CI = -10.13 – 11.38) (Figure S34). Two studies [42, 45] indicated that there was no difference before and six months after the NSPT among OP patients (MD = -5.48, CI = -22.16–11.21) (Figure S35), and the same was observed in NP [42, 45] groups (MD = -3.83, CI = -18.92–11.26) (Figure S36). Moreover, there was no difference in serum adiponectin level between OP and NP individuals six months after the NSPT (MD = 1.76, CI = -11.84–15.36) [42, 45] (Figure S37).
In the subgroup analysis comparing GCF levels of adiponectin (mg/L), only two included studies [35, 42] suggested that the levels of the OP group were not different from those in the NP group at baseline (MD = -0.18, CI = -1.66–1.29) (Figure S38). Moreover, two studies [35, 42] suggested that there was no difference before and three months after the NSPT among OP patients (MD = 1.06, CI = -1.58–3.70) (Figure S39). However, there was an increase in GCF levels of adiponectin three months after the NSPT among NP groups (MD = 2.37, CI = 0.29–4.45) [35, 42] (Fig. 7). Furthermore, there was no difference in GCF levels of adiponectin between the OP and NP individuals three months after the NSPT (MD = -1.15, CI = -3.90–1.60) [35, 42] (Figure S40).

Subgroup analysis comparing GCF levels of adiponectin before and three months after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups
NSPT and leptin
For the subgroup analysis comparing serum levels of leptin (pg/mL), three studies [40, 42, 45] suggested that there was no difference in the level of the OP group compared to that of the NP group at baseline (MD = 126.57, CI = -35.67 – 288.82) (Figure S41). Furthermore, there was no difference before and three months after the NSPT among OP patients (MD = -4.22, CI = -20.92–12.48) [40, 42, 45] (Figure S42) and among NP patients (MD = -3.44, CI = -10.84 – 3.96) [40, 42, 45] (Figure S43). Overall, three studies [40, 42, 45] suggested that there was no difference of serum leptin level between the OP group and the NP group at the 3-month follow-up (MD = 117.94, CI = -32.81–268.70) (Figure S44). Besides, two studies [42, 45] suggested there was no difference before and six months after the NSPT among OP patients (MD = -80.21, CI = -218.17–57.75) (Figure S45) and among NP patients (MD = -8.19, CI = -84.74–68.37) [42, 45] (Figure S46). Overall, two studies [42, 45] suggested that the serum leptin level of the OP group was higher than that of the NP group at the 6-month follow-up (MD = 139.93, CI = 65.09–214.76) (Fig. 8).

Subgroup analysis comparing 6 months follow-up serum levels of leptin after non-surgical periodontal therapy among patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups
NSPT and RBP4
In the subgroup analysis comparing serum levels of RBP4 (mg/dL), only two studies [43, 44] were incorporated, suggesting that the serum RBP4 level of the OP group was higher before the therapy compared with the level at the 3-month follow-up (MD = -0.39, CI = -0.68–0.10) (Fig. 9). Given the clinical heterogeneity of the incorporated studies in the present meta-analysis, the random-effects model was applied in all subgroup analyses. The results of the subgroup analyses are tabulated in Table S3 (Supplementary Information File).

Subgroup analysis comparing serum levels of RBP4 before and 3 months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups
Discussion
Although the underlying mechanisms of the association between obesity and periodontitis, as well as the interactions between NSPT and both conditions, remain to be fully clarified, research has confirmed the essential role of pro-inflammatory and anti-inflammatory mediators in the development of each condition and their interaction. The link between periodontitis and obesity is dominated by pro-inflammatory factors that exacerbate the severity of both conditions [59, 60]. A meta-analysis has shown that obesity can alter serum levels of pro-inflammatory mediators (i.e., IL-6, CRP, TNF-a, resistin and leptin) in patients with periodontitis, while periodontitis can alter the levels of these mediators in patients with obesity, aggravating the inflammatory profile [61].
Previous studies have primarily focused on observational studies (basically cross-sectional studies) without the introduction of intervention like NSPT, thus unable to assess the changes in levels of relevant mediators after treatment through intervention measures. With the implementation of NSPT, there is bound to be a redistribution of pro-inflammatory and anti-inflammatory mediators, such as a decrease in typical pro-inflammatory mediators like IL-6 and an increase in anti-inflammatory mediators like adiponectin, which is the main focus of our current study. We have analyzed the levels of these mediators in different biological fluids, including whole saliva, GCF, and serum. Saliva and GCF are known to carry local inflammatory mediators. GCF, in particular, is an oral fluid/ exudate that resides in close proximity to gingival tissues and contains various biomarkers and products derived from both hosts and bacteria [62]. Saliva and GCF are reliable tools widely used to detect even small changes during disease processes. They can be collected non-invasively to provide a more precise reflection of the condition of periodontitis. However, unlike whole saliva, which can represent the systemic conditions in general, GCF seems to be more specific. Samples of GCF taken from deep or shallow sites of the periodontal pocket represent different pathological conditions [63]. Meanwhile, serum can reflect the course of multiple diseases more comprehensively, serving as an indicator of the whole system [64].
Interleukin-6, a pro-inflammatory mediator, is known to regulate the host response to both periodontitis bacterial infection and obesity-related disorders [65, 66]. The results of a meta-analysis suggest that individuals with periodontitis and obesity have higher baseline serum levels of IL-6. However, after NSPT, the reduction of IL-6 levels is statistically significant in patients with obesity in a 3-month follow-up period, while no such impact is observed in normal-weight individuals with periodontitis. Thus, IL-6 levels after a 3-month follow-up interval may be an ideal clinical serum bioanalysis to detect the actual effect of NSPT in obesity patients.
Furthermore, the reduction of IL-6 levels in GCF after NSPT is also statistically significant in patients with obesity in a 3-month follow-up period. However, in follow-up periods longer than 3 months but less than 12 months, the impact of NSPT starts to diminish, as the IL-6 levels in GCF gradually increase in obese individuals, resulting in higher levels than those observed in non-obesity groups. These findings suggest that more frequent follow-up assessments are necessary to detect patients' conditions in a timely manner and initiate supplement treatment measures to improve prognosis, considering the time effect of the efficacy of NSPT.
TNF-α, as a pro-inflammatory mediator, has been shown to have high serum levels in individuals with periodontitis, indicating its involvement in the pathologic process of periodontitis. Moreover, TNF-α has been reported to be associated with several diseases, including diabetes, cardiovascular disease, cancer, and metabolic disorders [67]. Notably, TNF-α levels are correlated with the degree of adiposity and the associated insulin resistance [9]. According to the quantitative analysis, the serum level of TNF-α did not change three months after NSPT. Furthermore, both the baseline and three-month follow-up showed higher levels in obesity participants than in normal-weight participants, indicating that the positive effect of treatment on TNF-α serum levels was offset. Additionally, NSPT did not have an impact on TNF-α levels in GCF for either obese or non-obese participants, both at the three-month and distal timepoints. Interestingly, obesity participants presented with higher baseline GCF levels of TNF-α than non-obesity participants.
Elevated plasma levels of CRP, or hs-CRP, have been reported to be linked to obesity and insulin resistance [68, 69], with the latter being implicated in the association between obesity and periodontitis [23, 70]. The meta-analysis results suggest that NSPT may be more effective in reducing overall serum levels of CRP/hs-CRP at the 3-month follow-up, as there was no significant difference between individuals with and without obesity. However, at baseline, serum levels of CRP/hs-CRP were significantly higher in obesity patients than in those without obesity. Despite this, there was no apparent reduction in systemic inflammation in either obesity or non-obese patients as measured by serum levels of CRP/hs-CRP at the 3-month follow-up. Therefore, a 3-month follow-up interval may not be sufficient to support the actual effect of NSPT, and more timepoints need to be accumulated for stronger evidence.
Intriguingly, resistin, a member of the adipokine family, is also a pro-inflammatory mediator that plays a critical role in the development of obesity, insulin resistance, and related comorbidities [71]. Previous studies have shown that resistin levels increase with the severity of periodontal disease and decrease after periodontal therapy [72]. However, the results of quantitative research suggest that NSPT may not have a positive effect on either the GCF or serum levels of resistin in both obese and non-obese individuals at the distal timepoints. Moreover, based on the GCF and serum levels of resistin at baseline and the distal follow-up, it was found that obese patients had a higher expression of resistin, indicating an obesity-dominant higher level of pro-inflammatory expression.
Adiponectin, an anti-inflammatory adipokine, and has been shown to be a regulator of macrophage polarization to assist in reducing inflammation [73]. Besides, adiponectin and its agonists are promising candidates for the treatment of periodontitis due to emerging evidence of the link between adiponectin and periodontitis [74]. Based on the results of our systematic review, two studies [35, 42] demonstrated that NSPT leads to an increase in adiponectin levels in non-obese individuals. However, the meta-analysis suggests that NSPT may not have an impact on the serum levels of adiponectin at 3- or 6-months post-treatment in either obese or non-obese subjects. The same situation was observed in the GCF level of adiponectin at the 3-month follow-up in obese patients, but a significant increase in the GCF level of adiponectin was found in non-obese patients 3 months after the therapy, indicating that obesity may reduce the effectiveness of the treatment, while non-obese individuals may be more responsive to NSPT for anti-inflammation. There was no difference between obese and non-obese participants in the baseline serum level of adiponectin, as well as at the 3-month/6-month follow-up for serum adiponectin and at the 3-month follow-up for GCF adiponectin. Adiponectin may be a sensitive biomarker only in non-obese patients for a 3-month follow-up after NSPT to evaluate the treatment's effectiveness.
Leptin is one of the most well-known pro-inflammatory adipokines and is also recognized for its role in appetite regulation. Leptin resistance is considered a major risk factor for obesity [75]. Recent research has shown that leptin can promote the progression of periodontitis by inducing pro-inflammatory M1 macrophage skewing through the leptin/NLRP3 signaling pathway [76]. Our quantitative analysis of serum leptin levels found that NSPT did not have a significant impact on either obese or normal weight individuals at 3-month or 6-month intervals. Additionally, there were no differences in serum leptin levels between the two groups at baseline or at the 3-month follow-up. However, at the 6-month follow-up, serum leptin levels were significantly higher in the obese group compared to the non-obese group. These findings suggest that serum leptin analysis at either 3-month or 6-month intervals following NSPT may not be an accurate marker for treatment effectiveness.
RBP4, an adipokine related to obesity and insulin resistance [50], has been proposed as a potential biomarker of inflammatory activity in obesity and chronic periodontitis [77]. However, due to the limited number of included studies, a subgroup analysis of RBP4 in serum levels was only conducted in obese individuals. The results suggest that NSPT contributed to a decrease in the serum levels of RBP4 at 3 months post-treatment. This decrease in RBP4 levels may be indicative of a reduction in inflammatory activity in obese individuals.
Despite the above-mentioned biomarkers, MMP-8 is another essential mediator in the systemic subclinical inflammatory response in obesity; moreover, previous research has shown that some functional polymorphisms in the MMP genes are associated with the risk of periodontal disease [78, 79]. Meanwhile, many oxidative stress-related metabolites, such as malondialdehyde and 8-hydroxy-deoxyguanosine in GCF, were the most consistently associated with periodontitis [80]. Besides, patients with chronic periodontitis displayed higher levels of vaspin whether with obesity or not, however, the level of vaspin declined after the NSPT. These findings may provide other ideal diagnostic and prognostic indicators of CP for better therapeutic outcome [81].
The effect of obesity, specifically the adipose tissue, on the expression of pro-inflammatory cytokines may limit the effectiveness of NSPT in reducing their levels. Adipose tissue is an endocrine organ that releases various pro-inflammatory cytokines, which may increase the threshold of the NSPT's effect, making it difficult for the gingiva and periodontal bone to relieve the inflammatory state [82]. The relevant indicators suitable for the comorbidity model of obesity and periodontitis have been screened out from a number of pro-inflammatory and anti-inflammatory cytokines, and the results are considerable. However, due to the limitations of current research data, a longitudinal comparison of given changing levels (Δvalues for variation for individual before and after the NSPT) of indicators between obese and non-obese subjects cannot be effectively carried out. It is widely known that periodontitis is a bacterial infectious disease, and many cytokines/adipokines related to inflammation regulate the pathophysiology of periodontitis through interactions between tissue cells and immune cells.
Additionally, the regulatory mechanisms involved in the associations between periodontitis and obesity remain to be fully elucidated. It is important to control for confounding factors by excluding individuals with other metabolic or systemic diseases to minimize selection bias, as obesity is often comorbid with other conditions. Furthermore, follow-up intervals should be standardized and the observation period prolonged to evaluate long-term efficacy. As new adipokines, such as vaspin and chemerin, continue to emerge, more research is needed to establish their relationship with periodontitis and obesity. Inevitably, with the only permission of English-published article, publish bias cannot be avoid and our findings should be interpreted with caution, as most of the published studies were at moderate risk of bias and in several meta-analyses the heterogeneity is very high, basically because of the clinical heterogeneity. These limitations present opportunities for future research in this field.
Conclusions
NSPT can impact the levels of specific pro-inflammatory and anti-inflammatory mediators in biological fluids, both in obese and non-obese individuals, as well as between the two groups. Specifically, NSPT can lead to a decrease in serum and GCF levels of IL-6 and RBP4 in obese individuals after 3 months and an increase in GCF adiponectin levels in normal-weight individuals after 3 months. Besides, for patients with periodontitis, there is no sufficient evidence to prove that obese patients have a statistically significant decrease in the levels of other cytokines compared to patients with normal weight. Our findings implied the potential ideal follow-up intervals and sensitive biomarkers for clinical bioanalysis in personalized decision-making of effect of NSPT due to patients’ BMI value. These findings suggest that the 3-month follow-up interval and the aforementioned biomarkers could be valuable for clinical bioanalysis as an auxiliary chairside tool to evaluate the efficacy of NSPT.
Availability of data and materials
The datasets used and/or analyzed during the study are available from the corresponding author upon reasonable request.
References
Papapanou PN, Sanz M, Buduneli N, Dietrich T, Feres M, Fine DH, Flemmig TF, Garcia R, Giannobile WV, Graziani F, et al. Periodontitis: consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018;45(Suppl 20):S162-s170.
Zhang Y, Zhang Y, Mei Y, Zou R, Niu L, Dong S. Reactive oxygen species enlightened therapeutic strategy for oral and maxillofacial diseases-art of destruction and reconstruction. Biomedicines. 2022;10(11):2905.
Mainas G, Ide M, Rizzo M, Magan-Fernandez A, Mesa F, Nibali L. Managing the systemic impact of periodontitis. Medicina (Kaunas). 2022;58(5):621.
Sabharwal A, Gomes-Filho IS, Stellrecht E, Scannapieco FA. Role of periodontal therapy in management of common complex systemic diseases and conditions: an update. Periodontol 2000. 2018;78(1):212–226.
Sanz M, Marco Del Castillo A, Jepsen S, Gonzalez-Juanatey JR, D’Aiuto F, Bouchard P, Chapple I, Dietrich T, Gotsman I, Graziani F, et al. Periodontitis and cardiovascular diseases: consensus report. J Clin Periodontol. 2020;47(3):268–88.
Romano F, Perotto S, Mohamed SEO, Bernardi S, Giraudi M, Caropreso P, Mengozzi G, Baima G, Citterio F, Berta GN, et al. Bidirectional association between metabolic control in type-2 diabetes mellitus and periodontitis inflammatory burden: a cross-sectional study in an Italian population. J Clin Med. 2021;10(8):1787.
WorldHealthOrganization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i-xii, 1–253.
Haslam DW, James WP. Obesity. Lancet. 2005;366(9492):1197–209.
Tzanavari T, Giannogonas P, Karalis KP. TNF-alpha and obesity. Curr Dir Autoimmun. 2010;11:145–56.
Zhao P, Xu A, Leung WK. Obesity, bone loss, and periodontitis: the interlink. Biomolecules. 2022;12(7):865.
Kirichenko TV, Markina YV, Bogatyreva AI, Tolstik TV, Varaeva YR, Starodubova AV. The role of adipokines in inflammatory mechanisms of obesity. Int J Mol Sci. 2022;23(23):14982.
Suriagandhi V, Nachiappan V. Protective effects of melatonin against obesity-induced by leptin resistance. Behav Brain Res. 2022;417: 113598.
Flores-Cortez YA, Barragán-Bonilla MI, Mendoza-Bello JM, González-Calixto C, Flores-Alfaro E, Espinoza-Rojo M. Interplay of retinol binding protein 4 with obesity and associated chronic alterations (Review). Mol Med Rep. 2022;26(1):244.
Khanna D, Welch BS, Rehman A. Pathophysiology of obesity. In: StatPearls. edn. Treasure Island: StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC.; 2022.
Perlstein MI, Bissada NF. Influence of obesity and hypertension on the severity of periodontitis in rats. Oral Surg Oral Med Oral Pathol. 1977;43(5):707–19.
Pamuk F, Kantarci A. Inflammation as a link between periodontal disease and obesity. Periodontol 2000. 2022;90(1):186–196.
Khan MS, Alasqah M, Alammar LM, Alkhaibari Y. Obesity and periodontal disease: a review. J Fam Med Prim Care. 2020;9(6):2650–3.
Abu-Shawish G, Betsy J, Anil S. Is obesity a risk factor for periodontal disease in adults? A systematic review. Int J Environ Res Public Health. 2022;19(19):12684.
Keller A, Rohde JF, Raymond K, Heitmann BL. Association between periodontal disease and overweight and obesity: a systematic review. J Periodontol. 2015;86(6):766–76.
Martinez-Herrera M, Silvestre-Rangil J, Silvestre FJ. Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med Oral Patol Oral Cir Bucal. 2017;22(6):e708-e715.
Katz J, Bimstein E. Pediatric obesity and periodontal disease: a systematic review of the literature. Quintessence Int. 2011;42(7):595–9.
Sanada T, Sano T, Sotomaru Y, Alshargabi R, Yamawaki Y, Yamashita A, Matsunaga H, Iwashita M, Shinjo T, Kanematsu T, et al. Anti-inflammatory effects of miRNA-146a induced in adipose and periodontal tissues. Biochem Biophys Rep. 2020;22: 100757.
Jepsen S, Suvan J, Deschner J. The association of periodontal diseases with metabolic syndrome and obesity. Periodontol 2000. 2020;83(1):125–153.
Lamster IB, Pagan M. Periodontal disease and the metabolic syndrome. Int Dent J. 2017;67(2):67–77.
Subedi S, Patil SS, Baniya BK, Bista S, Kafle B, Shrestha N. Assessment of attachment level by laser in pocket therapy. J Nepal Health Res Counc. 2022;20(2):436–40.
Tagge DL, O’Leary TJ, El-Kafrawy AH. The clinical and histological response of periodontal pockets to root planing and oral hygiene. J Periodontol. 1975;46(9):527–33.
Oza RR, Sharma V, Multani P, Balsara K, Bajaj P, Dhadse P. Comparing the effectiveness of ultrasonic instruments over manual instruments for scaling and root planing in patients with chronic periodontitis: a systematic review and meta-analysis. Cureus. 2022;14(11): e31463.
Papageorgiou SN, Reichert C, Jäger A, Deschner J. Effect of overweight/obesity on response to periodontal treatment: systematic review and a meta-analysis. J Clin Periodontol. 2015;42(3):247–61.
Suresh S, Mahendra J, Singh G, Pradeep Kumar AR, Thilagar S, Rao N. Effect of nonsurgical periodontal therapy on plasma-reactive oxygen metabolite and gingival crevicular fluid resistin and serum resistin levels in obese and normal weight individuals with chronic periodontitis. J Indian Soc Periodontol. 2018;22(4):310–6.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7): e1000097.
Boudin F, Nie JY, Bartlett JC, Grad R, Pluye P, Dawes M. Combining classifiers for robust PICO element detection. BMC Med Inform Decis Mak. 2010;10:29.
Nishida C, Ko GT, Kumanyika S. Body fat distribution and noncommunicable diseases in populations: overview of the 2008 WHO Expert Consultation on Waist Circumference and Waist-Hip Ratio. Eur J Clin Nutr. 2010;64(1):2–5.
WHO-Expert-Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163.
Zuza EP, Barroso EM, Carrareto AL, Pires JR, Carlos IZ, Theodoro LH, Toledo BE. The role of obesity as a modifying factor in patients undergoing non-surgical periodontal therapy. J Periodontol. 2011;82(5):676–82.
Duzagac E, Cifcibasi E, Erdem MG, Karabey V, Kasali K, Badur S, Cintan S. Is obesity associated with healing after non-surgical periodontal therapy? A local vs. systemic evaluation. J Periodontal Res. 2016;51(5):604–612.
Çetiner D, Uraz A, Öztoprak S, Akça G. The role of visfatin levels in gingival crevicular fluid as a potential biomarker in the relationship between obesity and periodontal disease. J Appl Oral Sci. 2019;27: e20180365.
Zuza EP, Barroso EM, Fabricio M, Carrareto AL, Toledo BE. J RP: Lipid profile and high-sensitivity C-reactive protein levels in obese and non-obese subjects undergoing non-surgical periodontal therapy. J Oral Sci. 2016;58(3):423–30.
Martinez-Herrera M, Silvestre FJ, Silvestre-Rangil J, Lopez-Domenech S, Banuls C, Rocha M. Levels of serum retinol-binding protein 4 before and after non-surgical periodontal treatment in lean and obese subjects: an interventional study. J Clin Periodontol. 2018;45(3):336–44.
Akram Z, Baharuddin NA, Vaithilingam RD, Rahim ZH, Chinna K, Krishna VG, Saub R, Safii SH. Effect of nonsurgical periodontal treatment on clinical periodontal variables and salivary resistin levels in obese Asians. J Oral Sci. 2017;59(1):93–102.
Altay U, Gürgan CA, Ağbaht K. Changes in inflammatory and metabolic parameters after periodontal treatment in patients with and without obesity. J Periodontol. 2013;84(1):13–23.
Suvan J, Masi S, Harrington Z, Santini E, Raggi F, D’Aiuto F, Solini A. Effect of treatment of periodontitis on incretin axis in obese and nonobese individuals: a cohort study. J Clin Endocrinol Metab. 2021;106(1):e74–82.
Gonçalves TE, Zimmermann GS, Figueiredo LC, Souza Mde C, da Cruz DF, Bastos MF, da Silva HD, Duarte PM. Local and serum levels of adipokines in patients with obesity after periodontal therapy: one-year follow-up. J Clin Periodontol. 2015;42(5):431–9.
Martinez-Herrera M, Silvestre FJ, Silvestre-Rangil J, López-Domènech S, Bañuls C, Rocha M. Levels of serum retinol-binding protein 4 before and after non-surgical periodontal treatment in lean and obese subjects: an interventional study. J Clin Periodontol. 2018;45(3):336–44.
Martínez-Herrera M, Abad-Jiménez Z, Silvestre FJ, López-Domènech S, Márquez-Arrico CF, Silvestre-Rangil J, Víctor VM, Rocha M. Effect of non-surgical periodontal treatment on oxidative stress markers in leukocytes and their interaction with the endothelium in obese subjects with periodontitis: a pilot study. J Clin Med. 2020;9(7):2117.
Gonçalves TE, Feres M, Zimmermann GS, Faveri M, Figueiredo LC, Braga PG, Duarte PM. Effects of scaling and root planing on clinical response and serum levels of adipocytokines in patients with obesity and chronic periodontitis. J Periodontol. 2015;86(1):53–61.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355: i4919.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–805.
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1):135.
Ortega-Senovilla H, de Oya M, Garcés C. Relationship of NEFA concentrations to RBP4 and to RBP4/retinol in prepubertal children with and without obesity. J Clin Lipidol. 2019;13(2):301–7.
McGrath S, Zhao X, Steele R, Thombs BD, Benedetti A. Estimating the sample mean and standard deviation from commonly reported quantiles in meta-analysis. Stat Methods Med Res. 2020;29(9):2520–37.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366: l4898.
Al-Hamoudi N, Abduljabbar T, Mirza S, Al-Sowygh ZH, Vohra F, Javed F, Akram Z. Non-surgical periodontal therapy reduces salivary adipocytokines in chronic periodontitis patients with and without obesity. J Investig Clin Dent. 2018;9(2): e12314.
Vohra F, Akram Z, Bukhari IA, Sheikh SA, Javed F. Short-term effects of adjunctive antimicrobial photodynamic therapy in obese patients with chronic periodontitis: a randomized controlled clinical trial. Photodiagnosis Photodyn Ther. 2018;21:10–5.
Md Tahir K, Ab Malek AH, Vaithilingam RD, Saub R, Safii SH, Rahman MT, Abdul Razak F, Alabsi AM, Baharuddin NA. Impact of non-surgical periodontal therapy on serum Resistin and periodontal pathogen in periodontitis patients with obesity. BMC Oral Health. 2020;20(1):52.
Abdellatif HM, Ali D, Divakar DD, BinShabaib MS. SS AL: Periodontal status and whole salivary adipokines after scaling and root planing with and without adjunct antimicrobial photodynamic therapy in obese patients with periodontitis. Photodiagnosis Photodyn Ther. 2022;40: 103112.
Zuza EC, Pires JR, de Almeida AA, Toledo BEC, Guimaraes-Stabili MR, Junior CR, Barroso EM. Evaluation of recurrence of periodontal disease after treatment in obese and normal weight patients: two-year follow-up. J Periodontol. 2020;91(9):1123–31.
Al-Zahrani MS, Alghamdi HS. Effect of periodontal treatment on serum C-reactive protein level in obese and normal-weight women affected with chronic periodontitis. Saudi Med J. 2012;33(3):309–14.
Falagas ME, Kompoti M. Obesity and infection. Lancet Infect Dis. 2006;6(7):438–46.
Fantuzzi G. Adipose tissue, adipokines, and inflammation. J Allergy Clin Immunol. 2005;115(5):911–919; quiz 920.
Brum RS, Duarte PM, Canto GL, Flores-Mir C, Benfatti CAM, Porporatti AL, Zimmermann GS. Biomarkers in biological fluids in adults with periodontitis and/or obesity: a meta-analysis. J Indian Soc Periodontol. 2020;24(3):191–215.
Taylor JJ, Preshaw PM. Gingival crevicular fluid and saliva. Periodontol 2000. 2016;70(1):7–10.
Ghallab NA. Diagnostic potential and future directions of biomarkers in gingival crevicular fluid and saliva of periodontal diseases: review of the current evidence. Arch Oral Biol. 2018;87:115–24.
Zhang A, Sun H, Wang X. Serum metabolomics as a novel diagnostic approach for disease: a systematic review. Anal Bioanal Chem. 2012;404(4):1239–45.
Naruishi K, Nagata T. Biological effects of interleukin-6 on gingival fibroblasts: cytokine regulation in periodontitis. J Cell Physiol. 2018;233(9):6393–400.
Wueest S, Konrad D. The controversial role of IL-6 in adipose tissue on obesity-induced dysregulation of glucose metabolism. Am J Physiol Endocrinol Metab. 2020;319(3):E607-e613.
Esteves Lima RP, Atanazio ARS, Costa FO, Cunha FA, Abreu LG. Impact of non-surgical periodontal treatment on serum TNF-α levels in individuals with type 2 diabetes: a systematic review and meta-analysis. J Evid Based Dent Pract. 2021;21(2): 101546.
Greenfield JR, Campbell LV. Relationship between inflammation, insulin resistance and type 2 diabetes: “cause or effect”? Curr Diabetes Rev. 2006;2(2):195–211.
Ebrahimi M, Heidari-Bakavoli AR, Shoeibi S, Mirhafez SR, Moohebati M, Esmaily H, Ghazavi H, Saberi Karimian M, Parizadeh SM, Mohammadi M, et al. Association of serum hs-CRP levels with the presence of obesity, diabetes mellitus, and other cardiovascular risk factors. J Clin Lab Anal. 2016;30(5):672–6.
Byun JS, Lee HY, Tian J, Moon JS, Choi J, Lee SH, Kim YG, Yi HS. Effect of salivary exosomal miR-25-3p on periodontitis with insulin resistance. Front Immunol. 2021;12: 775046.
Cebeci E, Cakan C, Gursu M, Uzun S, Karadag S, Koldas M, Calhan T, Helvaci SA, Ozturk S. The main determinants of serum resistin level in type 2 diabetic patients are renal function and inflammation not presence of microvascular complication, obesity and insulin resistance. Exp Clin Endocrinol Diabetes. 2019;127(4):189–94.
Devanoorkar A, Kathariya R, Guttiganur N, Gopalakrishnan D, Bagchi P. Resistin: a potential biomarker for periodontitis influenced diabetes mellitus and diabetes induced periodontitis. Dis Markers. 2014;2014: 930206.
Ohashi K, Parker JL, Ouchi N, Higuchi A, Vita JA, Gokce N, Pedersen AA, Kalthoff C, Tullin S, Sams A, et al. Adiponectin promotes macrophage polarization toward an anti-inflammatory phenotype. J Biol Chem. 2010;285(9):6153–60.
Wang Z, Chen Z, Fang F, Qiu W. The role of adiponectin in periodontitis: current state and future prospects. Biomed Pharmacother. 2021;137: 111358.
Morris DL, Rui L. Recent advances in understanding leptin signaling and leptin resistance. Am J Physiol Endocrinol Metab. 2009;297(6):E1247-1259.
Han Y, Huang Y, Gao P, Yang Q, Jia L, Zheng Y, Li W. Leptin aggravates periodontitis by promoting M1 polarization via NLRP3. J Dent Res. 2022;101(6):675–85.
Kanoriya D, Pradeep AR, Mallika A, Singhal S, Garg V. Correlation of crevicular fluid and serum levels of retinol-binding protein 4 and leptin in chronic periodontitis and obesity. Clin Oral Investig. 2017;21(7):2319–25.
Lauhio A, Färkkilä E, Pietiläinen KH, Åström P, Winkelmann A, Tervahartiala T, Pirilä E, Rissanen A, Kaprio J, Sorsa TA, et al. Association of MMP-8 with obesity, smoking and insulin resistance. Eur J Clin Invest. 2016;46(9):757–65.
Belo VA, Souza-Costa DC, Lana CM, Caputo FL, Marcaccini AM, Gerlach RF, Bastos MG, Tanus-Santos JE. Assessment of matrix metalloproteinase (MMP)-2, MMP-8, MMP-9, and their inhibitors, the tissue inhibitors of metalloproteinase (TIMP)-1 and TIMP-2 in obese children and adolescents. Clin Biochem. 2009;42(10–11):984–90.
Baima G, Corana M, Iaderosa G, Romano F, Citterio F, Meoni G, Tenori L, Aimetti M. Metabolomics of gingival crevicular fluid to identify biomarkers for periodontitis: a systematic review with meta-analysis. J Periodontal Res. 2021;56(4):633–45.
Balli U, Bozkurt Dogan S, Ongoz Dede F, Sertoglu E, Keles GC. The levels of visceral adipose tissue-derived serpin, omentin-1 and tumor necrosis factor-α in the gingival crevicular fluid of obese patients following periodontal therapy. J Oral Sci. 2016;58(4):465–73.
Rasouli N, Kern PA. Adipocytokines and the metabolic complications of obesity. J Clin Endocrinol Metab. 2008;93(11 Suppl 1):S64-73.
Acknowledgements
None.
Funding
This work is supported by Fundamental Research Funds of Xi’an Jiaotong University for Free Exploration and Innovation—Project for Teacher (XZY012021069) and Project to Enhance the Base of Innovation Ability of Xi’an City—Medical Research (21YXYJ0123).
Author information
Authors and Affiliations
Contributions
Yuwei Zhang, Ru Jia and Yifei Zhang: Conceptualization; Methodology; Data extraction; Writing original draft; Xuefei Sun and Yukun Mei: Investigation; Data extraction; Editing; Rui Zou: Methodology; Supervision. Lin Niu and Shaojie Dong: Writing draft and editing; Providing projects and funds.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Inclusion and exclusion criteria and studies excluded after full-text analysis and related reasons. Table S2. The detailed effect of NSPT in respect to inflammatory cytokines and adipokines. Table S3. Synthesis of results in subgroup analyses. Table S4. Risk of bias assessment of included studies according to the ROBINS-I tool. Table S5. Risk of bias assessment of the 4 included RCTs with the ROB-2 tool. Figure S1. Subgroup analysis comparing baseline serum levels of IL-6 before non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S2. Subgroup analysis comparing serum levels of IL-6 before and three months after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) group. Figure S3. Comparison of 3-month follow-up of serum levels of IL-6 after non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S4. Subgroup analysis comparing baseline GCF levels of IL-6 before non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S5. Subgroup analysis comparing GCF levels of IL-6 before and three months after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S6. Comparison of 3-month follow-ups of GCF levels of IL-6 after non-surgical periodontal therapy for patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S7. Subgroup analysis comparing GCF levels of IL-6 before and distal follow-up time after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S8. Subgroup analysis comparing GCF levels of IL-6 before and distal follow-up time after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S9. Subgroup analysis comparing baseline serum levels of TNF-a before non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S10. Subgroup analysis comparing serum levels of TNF-a before and three months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S11. Subgroup analysis comparing serum levels of TNF-a before and three months after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S12. Subgroup analysis comparing baseline GCF levels of TNF-a before non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S13. Subgroup analysis comparing GCF levels of TNF-a before and three months after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S14. Comparison of three-month follow-ups of GCF levels of TNF-a after non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S15. Subgroup analysis comparing GCF levels of TNF-a before and distal follow-up time after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S16. Subgroup analysis comparing GCF levels of TNF-a before and distal follow-up time after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S17. Subgroup analysis comparing distal follow-up time GCF levels of TNF-a after non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S18. Subgroup analysis comparing baseline serum levels of CRP/hs-CRP before non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S19. Subgroup analysis comparing serum levels of CRP/hs-CRP before and 3 months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S20. Subgroup analysis comparing serum levels of CRP/hs-CRP before and 3 months after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S21. Subgroup analysis comparing follow-up serum levels of CRP/hs-CRP 3 months after non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S22. Subgroup analysis comparing salivary levels of resistin before and distal time after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S23. Subgroup analysis comparing baseline GCF levels of resistin before non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S24. Subgroup analysis comparing GCF levels of resistin before and distal time after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S25. Subgroup analysis comparing GCF levels of resistin before and distal time after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S26. The comparing distal follow-up time GCF levels of resistin after non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S27. Subgroup analysis comparing baseline serum levels of resistin before non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S28. Subgroup analysis comparing serum levels of resistin before and distal time after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S29. Subgroup analysis comparing serum levels of resistin before and distal time after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S30. Comparison of distal follow-up time serum levels of resistin after non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S31. Subgroup analysis comparing baseline serum levels of adiponectin before non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S32. Subgroup analysis comparing serum levels of adiponectin before and three months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S33. Subgroup analysis comparing serum levels of adiponectin before and three months after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S34. Subgroup analysis comparing 3 months follow-up serum levels of adiponectin after non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S35. Subgroup analysis comparing serum levels of adiponectin before and six months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S36. Subgroup analysis comparing serum levels of adiponectin before and six months after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S37. Subgroup analysis comparing 6 months follow-up serum levels of adiponectin after non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S38. Subgroup analysis comparing baseline GCF levels of adiponectin before non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S39. Subgroup analysis comparing GCF levels of adiponectin before and three months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S40. Subgroup analysis comparing 3 months follow-up GCF levels of adiponectin after non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S41. Subgroup analysis comparing baseline serum levels of leptin before non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S42. Subgroup analysis comparing serum levels of leptin before and three months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S43. Subgroup analysis comparing serum levels of leptin before and three months after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups. Figure S44. Subgroup analysis comparing 3 months follow-up serum levels of leptin after non-surgical periodontal therapy within patients with obesity and periodontitis (OP) and normal-weight patients with periodontitis (NP) groups. Figure S45. Subgroup analysis comparing serum levels of leptin before and six months after non-surgical periodontal therapy in patients with obesity and periodontitis (OP) groups. Figure S46. Subgroup analysis comparing serum levels of leptin before and six months after non-surgical periodontal therapy in normal-weight patients with periodontitis (NP) groups.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, Y., Jia, R., Zhang, Y. et al. Effect of non-surgical periodontal treatment on cytokines/adipocytokines levels among periodontitis patients with or without obesity: a systematic review and meta-analysis. BMC Oral Health 23, 717 (2023). https://doi.org/10.1186/s12903-023-03383-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03383-3