
Abstract
Background
The effects of a low concentration of hypochlorous acid (HOCl) mouthwash on salivary bacteria remained unclear. We aimed to evaluate the antibacterial effects of 100 ppm HOCl mouthwash on salivary bacteria, including Staphylococcus aureus (S. aureus), in patients with periodontal disease (PD).
Methods
Patients with PD were randomized into mouthwash-only (MW, n = 26) and mouthwash with periodontal flosser (MWPF, n = 27) groups. Patients without PD were selected for the control group (n = 30). S. aureus culture and saliva samples (before and after the intervention) were collected for bacterial DNA extraction. A real-time polymerase chain reaction assay and serial dilutions of S. aureus culture and saliva samples were used to measure the salivary bacteria total count (SBTC) and confirm the antibacterial effects of the mouthwash using S. aureus.
Results
No significant difference in demographic data was observed among the three groups. Before the intervention, the baseline SBTC of the MW and MWPF groups was significantly higher than that of the control group. After the mouthwash rinses, the SBTC data significantly changed in the MW and MWPF groups only (by 62.4% and 77.4%, respectively). After the base-2 log-transformation of the SBTC data, a similar trend was observed. Linear regression revealed that baseline SBTC and the MWPF intervention significantly affected SBTC reduction percentage by volume. After incubation with 10% (v/v) of mouthwash, the survival rates of 106 and 107 colony-forming units/mL of S. aureus were 0.51% ± 0.06% and 1.42% ± 0.37%, respectively.
Conclusions
These study results indicated that 100 ppm HOCl mouthwash treatment could effectively reduce SBTC in patients with PD and the abundance of S. aureus. It provides that the HOCl mouthwash can be an option for individuals to help control SBTC, especially in patients with PD.
Trial registration
The study protocol was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (KMUHIRB-F(I)-20200042) on 20/03/2020 and retrospectively registered at ClinicalTrial.gov (NCT05372835) on 13/05/2022.
Similar content being viewed by others


Introduction
Periodontal disease (PD) is a common oral disease in adults (individuals aged 30 years or older). The symptoms of PD are inflammation of the gingiva and periodontium [1]. Poor oral hygiene is a risk factor for PD [2]. The accumulation of dental plaque—especially when pathogenic bacteria are dominant—can lead to progressive periodontitis and the loss of teeth [3, 4]. Controlling the bacteria in the mouth is key to maintaining oral health [5]. The use of mouthwash and periodontal flossers can inhibit oral bacterial growth and increase the concentration of beneficial bacteria, thereby promoting dental health and preventing gum problems [6,7,8]. Mouthwash can effectively reduce oral bacterial counts in patients with periodontitis; however, the effects and efficacy of different mouthwash components on periodontitis remain unclear, and few studies have demonstrated the efficacy of such products [9]. Mouthwashes that contain ingredients with antibacterial properties, particularly those that can effectively reduce the number of microorganisms related to PD, have become popular.
Two key concerns regarding the use of mouthwash are its unpleasant taste and its potential to cause tooth staining [1]. Mouthwashes containing chemicals such as chlorhexidine and hypochlorous acid (HOCl) have been used to reduce the accumulation of oral bacteria and pathogens [1, 10, 11]. HOCl is a nonantibiotic antibacterial solution [12]. A stabilized HOCl solution was observed to effectively and rapidly kill most microorganisms it came in contact with in vitro [13, 14]. HOCl has potent anti-inflammatory and cytoprotective effects [13,14,15]. HOCl removes the outer polymer matrix of biofilms formed by microorganisms in a manner akin to physically scraping them off [13]. HOCl consists of a group of reactive oxygen species [16]. It exerts broad antibacterial effects on multiple Gram-positive and Gram-negative bacteria and has few side effects. HOCl does not irritate mucous membranes or result in pigmentation on the surface of teeth or restorations [16]. These studies support that HOCl mouthwash can be effective disinfection in dental care and oral hygiene.
Saliva serves as a reservoir of microorganisms and plays a key role in regulating bacterial colonization in the various oral structures [17]. Mouthwash is already known to contribute to the decrease of oral bacteria numbers and dental plaque accumulation. Previous in vitro studies indicate that HOCl mouthwash at a concentration of 250—500 ppm or lower concentration is an effective antimicrobial agent to reduces the viability of pathogenic bacteria of oral diseases without having the significant side effects [11, 18,19,20]. However, rare in vivo studies report the antibacterial effects of HOCl mouthwash on salivary bacteria in patients with PD, especially in lower concertation of HOCl. Recently, a new mouthwash called Chlogen has recently become available in Taiwan. Chlogen contains HOCl at a concentration of 100 ppm, which is relatively low. Whether Chlogen is effective at controlling salivary bacteria is unclear. A randomized controlled trial was conducted to investigate the antiseptic effects of Chlogen on salivary bacterial total count (SBTC) in patients with PD with and without concurrent use of periodontal flosser. We also evaluated whether the intervention’s effects differed significantly among these three groups. A commercialized bacterial strain (Staphylococcus aureus) with pure culture was used to compare the antiseptic effects of Chlogen.
Materials and methods
Ethics statement
The study protocol was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (KMUHIRB-F(I)-20200042) and retrospectively registered at ClinicalTrial.gov (NCT05372835). The study protocol followed the Declaration of Helsinki. The participation was voluntary and anonymous after the informed consent obtained.
Participants
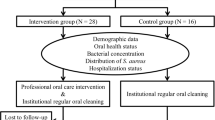
This was a double-blind (participants and lab investigation), randomized, parallel clinical trial enrolled outpatients at a private dental clinic (Fig. 1). Participants were aged between 35 and 70 years and provided written informed consent. Information on health histories and use of dental cleaning tools, such as mouthwash, was collected. Full-mouth dental examination records were checked by the same dentist. Gingivitis was defined as > 10% of tooth sites bleeding upon probing (BOP) and/or gingival bleeding (GI) and without probing pocket depth (PPD) or clinical attachment loss (CAL) > 3 mm. Periodontitis was defined as > 10% of teeth or > 15% of tooth sites with BOP and PPD or CAL ≥ 5 mm [21, 22]. The PDs of intervention were gingivitis and periodontitis. Patients without PD were enrolled into a control group. Patients who did not wish to participate, who had used antibiotics or immunosuppressive drugs within the last 6 months, who were pregnant, who smoked regularly, or who had a history of cancer or systemic disease were not included. Sample size was calculated using the mean difference in SBTC with base 2-log transformed data (effect size (ES) = 0.8, α = 0.05, and power = 0.8). Estimated sample size was 19 for each group. The IRB project was ended on schedule. In total, 53 patients with PD were randomly divided into two groups; one group (n = 26) used mouthwash only (Taiwan Patent No. M616466), and the other group (n = 27) used a mouthwash and periodontal flosser (Taiwan Patent No. M590033). A total of 30 individuals without PD were enrolled into the control group and gargled using 15 mL of pure water.

The CONSORT flowchart
Data collection
Before saliva collection, participants rinsed with 5 mL of water. Before and after the intervention, participants were asked to expectorate for a maximum of 3 min into a 50-mL sterile centrifugation tube (Creative Biotechnology, Taipei, Taiwan). The collected specimens were immediately placed in a portable ice box for storage and sent to a laboratory for same-day bacterial DNA extraction. The volume and weight of each saliva sample were recorded.
SBTC analysis
S. aureus ATCC 29213 was used as a reference strain in all experiments. The protocol for salivary bacterial DNA extraction, RT-PCR reaction, and bacterial growth curve estimation is described in our previous study [23] and ClinicalTrial.gov database ID: NCT05372835. After bacterial DNA extraction, real-time polymerase chain reaction (RT-PCR) was used to quantify the SBTC data (SBTC/mL and SBTC/g) in the samples. The RT-PCR assay of each sample was conducted in triplicate to calculate the SBTC data of each sample by using the equation created in our previous study [23]. Human blood DNA was used as a negative control group. The coefficient of variation of the threshold was between 2 and 11%.
Antibacterial activity of the mouthwash
After serial dilution, S. aureus solutions [0, 101, 102, 103, 104, 105, and 106 colony-forming units (CFU)/mL] were centrifuged at 2000 rpm for 5 min to concentrate the bacteria. The liquid was removed, 180 µL of fresh culture medium was added to resuspend the bacteria, and the cell suspension was aliquoted in 96-well plate. Next, 20 µL of the mouthwash was added to each well. The mixture was incubated at 37 °C for 2 h. Finally, 10 µL of CCK-8 reagent (CCK-8, Omics Bio, New Taipei City, Taiwan) was added and the mixture was agitated. The 96-well plate was incubated at 37 °C for 2 h, and the absorbance optical density (OD) value at 450 nm was measured using an ELISA reader. Each experiment was performed in triplicate. A standard growth curve was established for the measurement of serial dilution of the bacteria in the mixture and the bacterial survival rate.
Statistical analysis
After the data collection and checking were complete, the finalized debugged files were linked as a full dataset for statistical analysis with JMP statistical software (version 11, SAS Institute Inc. Cary, North Carolina, U.S.). Data were presented in frequency distribution tables and as percentages, means, and standard deviations. Considering the distribution of SBTC data, nonparametric statistical methods and base 2–log-transformed data were used to identify differences in the numerical data. Linear regression analysis was conducted to assess the factors contributing to percentage changes in SBTC after the intervention.
Results
A total of 83 participants was recruited into the present study. The mean age of participants was 58.0 ± 13.1 years. No significant differences in age (p = 0.21), man-to-woman ratio (p = 0.056), and collected saliva sample weight (p = 0.17) and volume (p = 0.53) were observed among the MW, MWPF, and control groups (Table 1). The average baseline bacterial counts by saliva volume in the MW, MWPF, and control groups were 2.97 ± 8.73 × 108, 7.99 ± 4.82 × 108, and 2.21 ± 4.26 × 106 CFU/mL, respectively, and the corresponding bacterial counts by saliva weight were 3.40 ± 1.06 × 109, 8.41 ± 3.90 × 109, and 2.29 ± 4.25 × 107 CFU/g, respectively. The baseline SBTC data in the MWPF and MW groups were significantly higher than that in the control group (p < 0.001). However, no significant difference between the MWPF and MW groups was observed. The SBTC data normalized through a log transformation by using base 2, and similar statistical results were obtained.
SBTC before and after the intervention is presented in Table 2. SBTC decreased significantly in the MW and MWPF groups by nonparametric statistics but did not reduce significantly in the control group. The changes in SBTC in the MW and MWPF groups were also significantly larger than those in the control group (p < 0.001), whose SBTC increased. The % decrease in SBTC by volume and by weight was significantly lower after the intervention in the MWPF group (− 77.4% ± 25.7% and − 74.8% ± 32.3%, respectively) (p < 0.001) and MW group (− 62.4% ± 31.9% and − 61.6% ± 33.9%, respectively) (p < 0.001) but higher after the intervention in the control group (259.5% ± 1105.5% and 289.9% ± 137.0%, respectively).
Log-transformed SBTC after the intervention is presented in Table 3. The statistical analysis with log-transformed data were similar to the original data (p < 0.001). The % decrease in SBTCs by volume and by weight were significantly lower after the intervention in the MW group (− 9.7% ± 8.9% and − 9.6% ± 8.9%, respectively) (p < 0.001) and MWPF group (− 13.4% ± 9.6% and − 13.35% ± 10.1%, respectively) (p < 0.001) but not in the control group.
Multivariate linear regression analysis of log-transformed SBTC data (Table 4) revealed that baseline SBTC (β = − 0.02, 95% confidence interval [CI] = − 0.03 to − 0.005 and β = − 0.06, 95% CI = − 0.12 to 0.00, respectively) was significantly correlated with % decreases in SBTC. The MWPF (vs. control: β = − 0.07, 95% CI = − 0.13 to − 0.10) group significantly affected the % decrease in SBTC by volume, but it was a borderline significance to affect the % decrease in SBTC by weight. Other factors, namely MW group (vs. controls: β = − 0.03, 95% CI = − 0.09 to 0.03 and β = − 0.02, 95% CI = − 0.08 to 0.05, respectively), age (β = − 0.0002, 95% CI = − 0.002 to 0.001 and β = − 0.0001, 95% CI = − 0.002 to 0.002, respectively) and sex (β = 0.04, 95% CI = − 0.01 to 0.08 and β = 0.04, 95% CI = − 0.01 to 0.09, respectively) did not significantly affect the % decrease in SBTC data.
A standard curve was established through a CCK-8 assay, and S. aureus growth was described as bacterial count log value = 3.515 + 0.556 × OD value. The survival rates of 106 and 107 CFU/mL of S. aureus were 0.51% ± 0.06% and 1.42% ± 0.37%, respectively.
Discussion
Present study found the SBTC of patients with PD in the MW and MWPF groups was significantly higher than that of the control group before the intervention. After the HOCl mouthwash intervention 5 min, the SBTC data significantly decreased in the MW and MWPF groups. After base-2 log-transformation of the SBTC data, a similar trend was observed. Multivariate linear regression revealed that baseline SBTC and the MWPF intervention significantly affected SBTC reduction percentage by volume. Previous study report that S. aureus is a common pathogenic bacteria found in the oral cavity of patients with PD [24]. Present study showed that 10% (v/v) mouthwash killed more than 98% of S. aureus by an in vitro assay. Although S. aureus used in this study was not identified from the study participants, these study results could partially support that 100 ppm HOCl mouthwash could effectively reduce the salivary bacterial load and S. aureus in patients with PD. However, previous study show that antimicrobial susceptibility of the same disinfection agent to planktonic and sessile cells are different [25]. Further studies are needed to test the antimicrobial effects of HOCl mouthwash on dental biofilm.
Previous studies show that SBTC by volume can be as high as 108 or 109 CFU/mL [26, 27]. SBTC by volume in patients with PD was significantly higher than in individuals with adequate oral health [28]. SBTC by volume decreased by 33% and 58% after participants gargled for 30 s with 500 ppm HOCl and 0.2% chlorohexidine, respectively [29]. In the present study, gargling with 100 ppm HOCl mouthwash for 5 min decreased SBTC by volume by 62.4% and 77.4% in the MW and MWPF groups, respectively. Before the intervention, SBTC by volume was significantly higher in patients with PD than in the control group. In the intervention groups, SBTC by volume was as high as 108 CFU/mL and by weight was as high as 109 CFU/g. Our study results are consistent with those of previous studies [26, 27]. The difference in percent decrease in SBTC by volume can be partially explained by the duration of use and concentration of HOCl.
Multivariate linear regression analysis revealed that the effect sizes of the MW (ES = 0.73) and MWPF (ES =1.05) groups were medium and large by the Cohen classification [30], respectively. In the present study, SBTC by volume in the MW and MWPF groups decreased by 62.4% and 77.4%, respectively, indicating that the antibacterial effect of the mouthwash plus periodontal flosser (MWPF group) higher than that of the mouthwash only (MW group). The decrease in SBTC by volume was 15% larger in the MWPF group than in the MW group but nonsignificant. For the base 2-log-transformed SBTC data, linear regression analysis revealed that the MWPF group (vs. controls) significantly affected the percentage decrease in SBTC by volume. Clinical studies have demonstrated that periodontal flossers facilitate greater contact between mouthwash and oral bacteria, thereby strengthening the antibacterial effects of mouthwash. The use of both a dental flosser and a manual toothbrush is significantly more effective for improving gingival health than a manual toothbrush alone [31]. These findings in combination with our results suggest that a periodontal flosser enhances the antibacterial effects of mouthwash.
PD is caused by an increase in dental plaque and inflammation. Early-stage PD, involving gingivitis, is reversible [32]. When dental plaque accumulates, gingivitis progresses to periodontitis, which is the irreversible destruction of periodontal tissue and alveolar bone [3]. Elevated gingival crevicular fluid miRNA expression is a potential biomarker for periodontitis or periodontal inflammation area [33]. In the present study, HOCl mouthwash effectively and rapidly decreased SBTC. It is possible that the HOCl mouthwash can contribute to the prevention and management of PD. Biomarkers can be used to detect PD at an early stage, thereby weakening the effects of PD on quality of life. These study results suggest that PD can be identified at an early stage by biomarkers and further to be prevented through the effective removal of plaque biofilm by using the mouthwash. Well-designed studies with large samples are required to support our hypotheses.
In one study, HOCl mouthwash had no direct antibacterial effect at 7 h after use, and bacterial count returned to baseline within 1 h of use [29]. Because of the limited observation time, we were unable to determine the duration of the bactericidal or bacteriostatic effects of the mouthwash in the oral cavity. More studies are required to investigate how the mouthwash in the present study can most effectively be used.
During the oral bacterial DNA extraction, some saliva samples were contaminated with small pieces of food residue. The food residue may have increased the variability of the antibacterial effects of mouthwash on SBTC by weight. This may partially explain why the MWPF intervention was not a significant factor in the regression analysis for the reduction in SBTC by weight.
A broad variety of mouthwash is available in the market. The potential unfavorable side-effects of mouthwash are cell cytotoxicity, bacterial resistance, tooth staining, and unpleasant taste [10, 34]. Some of these side-effects can be correlated with the CHX mouthwash [34]. Compared with the usage frequency of mouthwash with CHX, it is not common use of HOCl mouthwash [6]. Previous study indicate that HOCl can be produced from human immune cells and it has no such side-effects on the structure of oral cavity [35]. Present study showed that patients with PD could significantly reduce the SBTC data after the usage of HOCl mouthwash in a short time period. These study results suggest that 100 ppm HOCl mouthwash can be a good alternative option for patients with PD helping to reduce the SBTC.
This study has several limitations. First, data on the effects of durations of use and concentrations of HOCl mouthwash were not collected. Therefore, the most effective method of using the present mouthwash remains unclear. Although 100-ppm HOCl mouthwash is known to be nontoxic to cells in our previous study (data not shown), the antibacterial efficacy of the mouthwash on individual periodontitis-causing bacteria was not investigated in this study. Numerous types of bacteria are present in saliva, and the environment in which bacteria grow can vary depending on bacterial strain; further research is required to determine the antibacterial effects of mouthwash on salivary specific periodontal pathogens.
Conclusions
The baseline SBTC was significantly higher in patients with PD and contributed to the percentage reduction of SBTC data by multivariate regression analysis. The treatment of 100 ppm HOCl mouthwash could effectively decrease the SBTC in patients with PD and the level of S. aureus by an in vitro study, respectively. We suggest that HOCl mouthwash is an option for individuals to help control bacteria in the mouth, especially in patients with PD.
Availability of data and materials
Data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- CFU:
-
Colony-forming unit
- ES:
-
Effect size
- HOCl:
-
Hypochlorous acid
- MW:
-
Mouthwash
- MWPF:
-
Mouthwash and periodontal flosser
- OD:
-
Optical density
- PD:
-
Periodontal disease
- RT-PCR:
-
Real-time polymerase chain reaction
- S. aureus:
-
Staphylococcus aureus
- SBTC:
-
Salivary bacterial total count
References
Rajendiran M, Trivedi HM, Chen D, Gajendrareddy P, Chen L. Recent Development of Active Ingredients in Mouthwashes and Toothpastes for Periodontal Diseases. Molecules. 2021;26:2001.
Lertpimonchai A, Rattanasiri S, Arj-Ong Vallibhakara S, Attia J, Thakkinstian A. The association between oral hygiene and periodontitis: a systematic review and meta-analysis. Int Dent J. 2017;67:332–43.
Lang NP, Schatzle MA, Loe H. Gingivitis as a risk factor in periodontal disease. J Clin Periodontol. 2009;36(Suppl 10):3–8.
Palmer RJ. Oral bacterial biofilms–history in progress. Microbiology. 2009;155:2113–4.
Bowen WH, Burne RA, Wu H, Koo H. Oral Biofilms: Pathogens, Matrix, and Polymicrobial Interactions in Microenvironments. Trends Microbiol. 2018;26:229–42.
Takenaka S, Ohsumi T, Noiri Y. Evidence-based strategy for dental biofilms: Current evidence of mouthwashes on dental biofilm and gingivitis. Jpn Dent Sci Rev. 2019;55:33–40.
Lee PP, Mak WY, Newsome P. The aetiology and treatment of oral halitosis: an update. Hong Kong Med J. 2004;10:414–8.
Furquim Dos Santos Cardoso V, Amaral Roppa RH, Antunes C, Silva Moraes AN, Santi L, Konrath EL. Efficacy of medicinal plant extracts as dental and periodontal antibiofilm agents: A systematic review of randomized clinical trials. J Ethnopharmacol. 2021;281:114541.
Grover V, Mahendra J, Gopalakrishnan D, Jain A. Effect of octenidine mouthwash on plaque, gingivitis, and oral microbial growth: A systematic review. Clin Exp Dent Res. 2021;7:450–64.
Van der Weijden FA, Van der Sluijs E, Ciancio SG, Slot DE. Can Chemical Mouthwash Agents Achieve Plaque/Gingivitis Control? Dent Clin North Am. 2015;59:799–829.
Castillo DM, Castillo Y, Delgadillo NA, Neuta Y, Jola J, Calderon JL, et al. Viability and Effects on Bacterial Proteins by Oral Rinses with Hypochlorous Acid as Active Ingredient. Braz Dent J. 2015;26:519–24.
Levine JM. Dakin’s solution: past, present, and future. Adv Skin Wound Care. 2013;26:410–4.
Sakarya S, Gunay N, Karakulak M, Ozturk B, Ertugrul B. Hypochlorous Acid: an ideal wound care agent with powerful microbicidal, antibiofilm, and wound healing potency. Wounds. 2014;26:342–50.
Totoraitis K, Cohen JL, Friedman A. Topical Approaches to Improve Surgical Outcomes and Wound Healing: A Review of Efficacy and Safety. J Drugs Dermatol. 2017;16:209–12.
Kim C, Cha YN. Taurine chloramine produced from taurine under inflammation provides anti-inflammatory and cytoprotective effects. Amino Acids. 2014;46:89–100.
Green JN, Kettle AJ, Winterbourn CC. Protein chlorination in neutrophil phagosomes and correlation with bacterial killing. Free Radic Biol Med. 2014;77:49–56.
Van der Velden U, Van Winkelhoff AJ, Abbas F, De Graaff J. The habitat of periodontopathic micro-organisms. J Clin Periodontol. 1986;13:243–8.
Tazawa K, Jadhav R, Azuma MM, Fenno JC, McDonald NJ, Sasaki H. Hypochlorous acid inactivates oral pathogens and a SARS-CoV-2-surrogate. BMC Oral Health. 2023;23:111.
Koluman A, Aktas A, Adiloglu S. Antimicrobial activities of Ankaferd BloodStopper, hypochlorous acid, and chlorhexidine against specific organisms. Turk J Med Sci. 2022;52:276–8.
Hsieh YL, Yao JC, Hsieh SC, Teng NC, Chu YT, Yu WX, et al. The In Vivo Toxicity and Antimicrobial Properties for Electrolyzed Oxidizing (EO) Water-Based Mouthwashes. Materials (Basel). 2020;13:4299.
da Silva-Boghossian CM, do Souto RM, Luiz RR, Colombo AP. Association of red complex, A. actinomycetemcomitans and non-oral bacteria with periodontal diseases. Arch Oral Biol. 2011;56:899–906.
Lourenco TGB, de Oliveira AM, Tsute Chen G, Colombo APV. Oral-gut bacterial profiles discriminate between periodontal health and diseases. J Periodontal Res. 2022;57:1227–37.
Chiang TC, Huang MS, Lu PL, Huang ST, Lin YC. The effect of oral care intervention on pneumonia hospitalization, Staphylococcus aureus distribution, and salivary bacterial concentration in Taiwan nursing home residents: a pilot study. BMC Infect Dis. 2020;20:374.
Fritschi BZ, Albert-Kiszely A, Persson GR. Staphylococcus aureus and other bacteria in untreated periodontitis. J Dent Res. 2008;87:589–93.
Al-Ouqaili MTS, Al-Kubaisy SHM, Al-Ani NFI. Biofilm antimicrobial susceptibility pattern for selected antimicrobial agents against planktonic and sessile cells of clinical isolates of staphylococci using MICs, BICs and MBECs. Asian J Pharmaceutics. 2018;12(4):S1375-83.
Marsh P, Martin M. Oral Microbiology 4th ed Butterworth-Heinemann. Oxford, United Kingdom: Lincare House, Jordan Hill; 1999.
Darout IA. Oral bacterial interactions in periodontal health and disease. J Dent Oral Hyg. 2014;6:7.
Uzel NG, Teles FR, Teles RP, Song XQ, Torresyap G, Socransky SS, et al. Microbial shifts during dental biofilm re-development in the absence of oral hygiene in periodontal health and disease. J Clin Periodontol. 2011;38:612–20.
Lafaurie GI, Zaror C, Diaz-Baez D, Castillo DM, De Avila J, Trujillo TG, et al. Evaluation of substantivity of hypochlorous acid as an antiplaque agent: A randomized controlled trial. Int J Dent Hyg. 2018;16:527–34.
Ezzati K, Laakso EL, Salari A, Hasannejad A, Fekrazad R, Aris A. The Beneficial Effects of High-Intensity Laser Therapy and Co-Interventions on Musculoskeletal Pain Management: A Systematic Review. J Lasers Med Sci. 2020;11:81–90.
Goyal CR, Qaqish JG, Schuller R, Lyle DM. Evaluation of the Addition of a Water Flosser to Manual Brushing on Gingival Health. J Clin Dent. 2018;29:81–6.
Page RC. Gingivitis. J Clin Periodontol. 1986;13:345–59.
Isola G, Santonocito S, Distefano A, Polizzi A, Vaccaro M, Raciti G, et al. Impact of periodontitis on gingival crevicular fluid miRNAs profiles associated with cardiovascular disease risk. J Periodontal Res. 2023;58:165–74.
Van Strydonck DA, Slot DE, Van der Velden U, Van der Weijden F. Effect of a chlorhexidine mouthrinse on plaque, gingival inflammation and staining in gingivitis patients: a systematic review. J Clin Periodontol. 2012;39:1042–55.
Block MS, Rowan BG. Hypochlorous Acid: A Review. J Oral Maxillofac Surg. 2020;78:1461–6.
Acknowledgements
We thank all the patients, staff, and the dental hygienist who participated in this study and the fieldworkers who contributed to the data collection process.
Funding
This research was supported through funding from an industry–academia project at Kaohsiung Medical University (S-S108037).
Author information
Authors and Affiliations
Contributions
Y.C. wrote the original draft, completed lab investigation and C.F. prepared mouthwash, invited patients, sample collection, and H.L. prepared table 1-4, project administration. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol followed the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (KMUHIRB-F(I)-20200042) and retrospectively registered at ClinicalTrial.gov (NCT05372835). The participation was voluntary and anonymous after the informed consent obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lin, YC., Tsai, CF. & Huang, HL. Effects of hypochlorous acid mouthwash on salivary bacteria including Staphylococcus aureus in patients with periodontal disease: a randomized controlled trial. BMC Oral Health 23, 698 (2023). https://doi.org/10.1186/s12903-023-03358-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03358-4