
Abstract
Background
The risk of SARS-COV-2 transmission is relatively high during dental procedures. A study was conducted to investigate the effects of mouthwashes on SARS-COV-2 viral load reduction in the oral cavity.
Methods
A systematic search was performed in PubMed, EMBASE, Scopus, Web of Science, and Cochrane library for relevant studies up to 20 July, 2022. Randomized and non-randomized clinical trial and quasi-experimental studies evaluating patients with Covid-19 infection (patients) who used mouthwashes (intervention) compared to the same patients before using the mouthwash (comparison) for reducing the SARS-COV-2 load or increasing the cycle threshold (Ct) value (outcome) were searched according to PICO components. Three independent reviewers conducted literature screening and data extraction. The Modified Downs and Black checklist was used for quality assessment. A meta-analysis was performed with a random effects model in the Revman 5.4.1software using the mean difference (MD) of cycle threshold (Ct) values.
Results
Of 1653 articles, 9 with a high methodological quality were included. A meta-analysis indicated that 1% Povidone-iodine (PVP-I) was an effective mouthwash for reducing the SARS-COV-2 viral load [MD 3.61 (95% confidence interval 1.03, 6.19)]. Cetylpyridinium chloride (CPC) [MD 0.61 (95% confidence interval -1.03, 2.25)] and Chlorhexidine gluconate (CHX) [MD -0.04 95% confidence interval (-1.20, 1.12)] were not effective against SARS-COV-2.
Conclusion
Using mouthwashes containing PVP-I may be recommended for reducing the SARS-COV-2 viral load in the oral cavity of patients before and during dental procedures, while the evidence is not sufficient for such effects for CPC and CHX-containing mouthwashes.
Similar content being viewed by others

Introduction
SARS-CoV-2, the cause of coronavirus disease 2019 (Covid-19), a Betacoronavirus, belongs to the coronaviride family. It is a single-stranded, positive-sense RNA virus [1]. The main transmission route of SARS-CoV-2 is through respiratory droplets. These droplets cause direct contact infection during coughing, sneezing, and speaking or indirect contact infection via touching infected objects and the environment [2]. This virus shows high transmissibility and binds with the surface angiotensin-converting enzyme-2 (ACE2) receptors of host cells using the S1 subunit of the receptor binding domain in the spike protein. These receptors are expressed in multiple human systems and tissues, such as the lung and salivary glands as well as the epithelial cells of the nasopharynx and oropharynx [1, 3,4,5].
There is evidence that the oral cavity is a SARS-CoV-2 reservoir because ACE2 is highly expressed in the oral non-keratinizing squamous epithelium. Moreover, researchers successfully detected the SARS-CoV-2 RNA in the saliva [6]. Therefore, saliva is a source of SARS-CoV-2 transmission. There is a relatively high risk of virus transmission in dental procedures and oropharyngeal examination because of face-to-face treatments and aerosol-generating equipment [7, 8]. The ultrasonic scalers and high-speed handpieces spray saliva, blood, and fomites resulting in microbial transmission between patients and clinic staff. Viral shedding has been detected in the oral cavity of symptomatic and asymptomatic patients [9].
Prevention of SARS-CoV-2 infection is important in dental clinics; hence, it is critical to break the viral transmission chain between the patients and staff. There are some recommendations for this. The first step is to use personal protective equipment. Patient evaluation and identification of patients with potential Covid-19 infection are very crucial. The use of a non-contact thermometer is recommended for temperature measurement. A questionnaire can screen the patients; it should investigate whether the patient had any Covid-19 infection symptoms, such as fever and respiratory problems, during the past 14 days and if they had a close contact with a confirmed Covid-19 infected patient within the past two weeks [10]. Moreover, postponing the appointment and referring the patients to local health departments is recommended if the patient has a body temperature above 37.3 °C or is suspected as an at-risk case with a positive answer to the Covid-19 infection questionnaire [11].
Despite the application of these health recommendations, because of the presence of asymptomatic patients in to dental clinics, additional protective measures should be considered before and during dental procedures, such as the use of disinfectants and mouthwashes.
Today, a large number of antimicrobial mouthwashes are available on the market that have natural or synthetic antiseptic compounds. Preoperative antisepsis mouthwashes are frequently used in dental offices [12]. Different concentrations of these mouthwashes have antibacterial and antiviral effects [13, 14].
Recent publications have recommended that using antiseptic mouthwashes may control the viral load of SARS-COV-2 in the saliva. However, scientific evidence is lacking/contradictory for the anti-SARS-COV-2 effects. Although researchers have investigated the in-vitro effects of antiseptic mouthwashes on Covid-19 [15,16,17,18,19], limited clinical trial studies have examined the effects of antiseptic mouthwashes on Covid-19 viral load. The present systematic review was performed to answer: What are the effects of mouthwashes on SARS-COV-2 viral load reduction in the oral cavity?
Methods.
We systematically reviewed studies including patients with a SARS-CoV-2 positive test that used a mouthwash for SARS-COV-2 viral load reduction. In this study, we adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 2020 recommendations provided by Liberati [20].
Electronic searches
The PubMed, EMBASE, Scopus, Web of Science and Cochrane Central databases were searched using the MeSH and non-MeSH terms and the keywords. Table 1 presents the search strategy for mentioned databases. Google Scholar, MedRxiv, and clinicaltrials.gov were also searched with similar keywords manually to retrieve the gray literature. The reference lists of the included papers were also searched to find relevant studies.
Eligibility criteria and study selection
The studies that fulfilled the following inclusion criteria according to the PICO acronym were included.
Type of included studies
Randomized clinical trialsnon-randomized clinical trialsquasi-experimental studies
Types of participants: Participants were subjects diagnosed with Covid-19 infection with no age or gender restrictions.
Types of interventions:
-
Interventions: The use of the mouthwash was an intervention for patients infected with Covid-19
-
Comparator: No mouthwash use was the comparison
Types of outcome measures:
-
Primary outcome: change in cycle threshold value.
-
Secondary outcome: change in viral load.
Types of excluded studies:
-
Reviews
-
Letters to the editor
-
Technical notes
-
In vitro studies
-
Animal studies
-
conference papers
-
studies without the evaluation of the SARS-COV2 viral load or Ct values in saliva
Data extraction
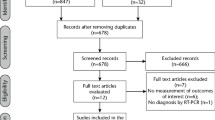
The screening was done independently by T.E, SZ.M, and ARSH. The PRISMA flow diagram was used as a guide to the selection process (Fig. 1). First, duplicate results were identified and excluded. The titles and the abstracts of the papers were screened to exclude the irrelevant studies. Accordingly, the search results were categorized into three categories (included, excluded and unclear). Then, the full texts of the retrieved studies were reviewed for final inclusion. Any disagreement between the three researchers was resolved by discussion. The following data were extracted from eligible articles: study characteristics (study title, authors, date of publication, study design, number of patients); baseline data (kind of mouthwash, type of examination for measuring the viral load, type of analyses of viral load) and clinical outcomes (viral load reduction). The mean and standard deviation of Ct values or mean and standard deviation of viral load before and after the intervention were compared. This review study was conducted from November 2, 2020 to August 15, 2022. The Endnote 20 software was used for organizing the references.

The PRISMA flow diagram of screening and selection process
Assessing the risk of bias
Three reviewers (T.E, S.Z.M, A.SH) independently assessed the risk of bias for the included studies as part of the data extraction procedure. A modified Down and Black (D&B) Risk of Bias checklist [21] was used for assessing the quality of the included studies. Each satisfactory response received a score of 1; otherwise, a score of 0 was assigned. Studies with a modified D&B level ≥ 5 were considered as studies with a low risk of bias. Those with a modified D&B level < 5 points were considered as studies with a high risk of bias (Table 2). GRADE (Grades of Recommendation, Assessment, Development and Evaluation) system was applied to rank the certainty of the scientific evidence [22].
Meta-analysis
Five studies that reported the mean and standard deviation of the Ct value or the value could be calculated from other reported data in the study were included in the meta-analysis. The RevMan 5.4.1 was used for analysis. There was a high level of heterogeneity in the mouthwash type, diagnostic kit, specimen (saliva or nasopharynx or oropharynx swab) and time of experiment (the time between the first RT-PCR test and using the mouthwash) among studies. Random-effects models and subgroup analysis were used to reduce the impact of heterogeneity. The Egger’s and Begg’s tests were used for publication bias assessment.
Ethical consideration
This systematic review and meta-analysis was registered in the PROSPERO database (registration number: CRD42021274832).
Results
In the initial search, 1653 papers were retrieved from the PubMed, EMBASE, Scopus, Web of Science, Cochrane Central, Google Scholar, MedRxiv, and clinicaltrials.gov. After removal of duplicates, 1539 title and abstracts were screened for the eligibility criteria. As for the remaining 18 articles, a paper was excluded if it met other inclusion criteria but did not report the mean and SD of the viral load or an accurate Ct value before and after the intervention. Excluded studies and reasons for exclusion are listed in Table 3. Finally, 9 articles were included in our study (See Fig. 1).
Assessment of methodological quality
As shown in Table 2, according to the modified D&B score, 5 studies obtained a score of 6 [23, 24, 26,27,28], 1 study scored 7 [31], and 3 studies scored 8 [25, 29, 30]. All studies were considered to have a low risk of bias.
There was hetreogenecity in included studies in the type mouthwash (intervention), diagnostic kit, specimen (saliva, nasopharynx, or oropharynx swab) and time of experiment (the time between the first RT-PCR test and using the mouthwash). GRADE system ranked the certainty of the scientific evidence and the strength of the recommendation as moderate for both outcomes (Downgraded for observed heterogeneity) [22].
Study characteristics
In 7 publications, the study population was patients with a positive PCR test for SARS-COV-2 in the hospital [23,24,25, 27,28,29,30]. In one study, the patients were quarantined at home or were admitted to the hospital [26]. The patients were those referred to Dental Clinics of The Ohio State University College of Dentistry and Wexner Medical Center in one study [31].
Six studies had control groups [24, 25, 28,29,30,31]. The other three studies had no control groups and baseline samples were compared with experimental samples [23, 26, 27].
In one study, if patients started one treatment for Covid-19, they were excluded from the study [24]. In two studies, the patients received different treatments for Covid-19 during the experiment such as lopinavir/ritonavir, hydroxychloroquine, antibiotics, or a combination of them [25, 27]. Seven studies did not the use of antiviral or other medications during the study [23, 24, 26, 28,29,30,31].
In one study, 9 out of 10 patients had different underlying diseases such as chronic renal failure, multiple myeloma, and arterial hypertension [23]. In another study, 2 out of 20 subjects had asthma and obesity as comorbidities [24]. A history of non-Hodgkin's lymphoma, diabetes, and ischemic stroke was reported for 2 out of 4 participants in one study [26]. About 30% of all patients had comorbidities in one study [28]. One study reported that a number of symptomatic patients received remdesivir or convalescent plasma but a number or percentage was not mentioned [31]. Another study reported that 21% of the participants had different underlying diseases (diabetes millets, hypertension, and chronic kidney disease) [25]. At least 30% of the participants had hypertension, cardiovascular disease, diabetes, respiratory disease, renal disease, obesity or hypothyroidism in one study [30] In another study, 77.84% of patients had no medical history [29]. One study did not mention any underlying diseases [27].
Descriptive findings of studies
Studies conducted by Gottsauner et al. [23], Mohamed et al. [38], Mukhtar et al. [25], Carrouel et al. [29] and Chaudhary et al. [31] were not included in the meta-analysis. In the study by Gottsauner et al. [23], the envelope (E) gene of SARS-COV-2 was amplified. Four patients showed an increase in the viral load after intervention and 4 patients showed a decrease in the viral load. There was no difference in the viral load between baseline and intervention swab tests in two patients. Therefore, they reported no significant reduction in the intraoral viral load after rinsing with 1% hydrogen peroxide mouthwash (Tables 4, and 5). Mohamed et al. [24] reported the result of swab tests as either negative (no Ct obtained), positive (Ct value ≤ 45 for both assays), or indeterminate(When only one gene assay had Ct < 45) for E gene and RNA-dependent RNA polymerase (RdRp) gene before and after rinsing with PVP-I, Cetylpyridinium chloride (CPC), and tap water. SARS-CoV-2 test was negative in all specimens of PVP-I group on days 4, 6, and 12. In the Listerine group, 4 out of 5 swab tests were negative on subsequent days. Two samples were negative in the tap water group on days 4, 6 and 12. In the control group, one swab sample was negative on days 4 and 12, and there was no negative sample on day 6. In this study, rinsing with 1% PVP-I and Listerine mouthwashes three times a day effectively reduced the SARS-CoV-2 viral load. Writers concluded that rinsing 1% PVP-I and essential oils could be a part of the treatment and management of COVID-19 at early stages (Tables 4, and 5). Mukhtar et al. [25] reported the result of swab tests as either negative and inconclusive (Ct value = 35–40) or positive (Ct value < 34.99) for ORF-1a/b and E-genes after rinsing with a mouthwash containing 6% hydrogen peroxide (HP) mixed with 0.2% chlorhexidine gluconate (CHX). At baseline, Ct values of none of the swab tests were negative in the intervention and control groups (0 out of 46 swab test was negative). After 5 days, 6 out of 45 swab tests were negative in the intervention group while no swab test was negative in the control group. After 15 days, 15 out of 43 swab tests were negative in the intervention group and 9 out of 44 were negative in the control group. They found a significant difference in the PCR results between the two groups that used the mouthwash on day 5, but the difference was not significant on day 15. They concluded that their intervention caused more COVID19-negative PCR by 5 day of treatment, symptoms severity would be improved after 2 days and there would be less intubation and mortality (Tables 4, and 5). Carrouel et al. [29] targeted the RdRp gene. On days 1 and 7 of the experiment, the Ct value changed by 2 points at 1 h, 4 h, and 9 h after using the CDCM mouthwash, indicating that it was effective in reducing the viral load. According to the study by Keyarts et al. a 2-point increase in the Ct value was considered as effective in reducing the viral load [39]. Writers concluded that using CDCM on day 1 reduced the viral load of SARS-COV-2 (Tables 4, and 5). Chaudhary et al. [31] did not mentioned which RNA gene was targeted. Saline, 1% hydrogen peroxide, 0.12% chlorhexidine, and 0.5% povidone-iodine were effective 15 min and 45 min post mouthwash use according to Ct value reports. They concluded that mouthwashes can simply and effectively reduce the risk of transmitting the virus. Other characteristics and results of the 9 included studies are summarized in Tables 4 and 5.
Meta-analysis
According to the mean differences of Ct values, 4 studies were included in meta-analysis [26,27,28, 30]. These studies used mouthwashes containing PVP-I, CHX and CPC. In this meta-analysis, there were 5 subgroups of time for the PVP-I-containing mouthwash: 5 min (min), 1 h (h), 2 h, 3 h, and 6 h after rinsing. The studies conducted by Lamas and Seneviratne [26, 28] were included in the meta-analysis of the effect of PVP-I-containing mouthwash on the Ct value of SARS-COV-2. The MD was 3.61 and 95% confidence interval (CI) was 1.03 to 6.19 for analyzing Ct values before and after rinsing with PVP-I containing mouthwashes. These mouthwashes were found to be effective 5 min, 1 h, 2 h, 3 h and 6 h after rinsing (Fig. 2).

Forest plot of meta-analysis of the effect of PVP-I mouthwash on Cycle threshold value of SARS-COV-2
The meta-analysis of the effect of CHX mouthwash on Ct value of SARS-COV-2, which included studies conducted by Yoon, Seneviratne and Eduardo [27, 28, 30], had 7 time subgroups: 0–5 min, 30 min, 1 h, 2 h, 3 h, 4 h and 6 h after rinsing. MD was -0.04 and 95% CI was -1.20 to 1.12 for analyzing Ct values before and after rinsing with mouthwashes containing CHX; therefore, these mouthrinses were not effective for reducing SARS-COV-2 viral load (Fig. 3).

Forest plot of meta-analysis of the effect of Chlorhexidine gluconate-containing mouthwash on Cycle threshold value of SARS-COV-2
There were five subgroups of time in the meta-analysis of CPC-containing mouthwashes: 0–5 min, 30 min, 1 h, 3 h, 6 h after rinsing according to the studies conducted by Seneviratne and Eduardo [28, 30]. CPC containing mouthwashes were not effective against SARS-COV-2 when analyzing Ct values before and after rinsing mouthwashes containing CPC (MD: 0.61, 95% CI: -1.03 to 2.25) (Fig. 4).

Forest plot of meta-analysis of the effect of CPC-containing mouthwash on Cycle threshold value of SARS-COV-2
The Egger’s and Begg’s tests were used for publication bias assessment (Fig. 5). Although a specific gap cannot be detected, due to the small number of included studies, the evaluation of publication bias is not reliable.

Funnel plots based on Ct value changes. a) PVP mouthwash b) CHX mouthwash C) CPC mouthwash
Discussion
Covid-19 is known to transfer from one person to another through infected droplets and aerosols. Close contact of dentists with patients and aerosol-generating procedures can significantly increase airborne contamination and cross-infection of SARS-CoV-2 in dental clinics.
Antiseptic mouthrinses have been suggested for various prophylactic and therapeutic purposes in dentistry. However, their anti-SARS-CoV-2 effect to control the viral load has not been evaluated systematically.
Mouthwashes should have a high substantivity. It means that they are released slowly, so they show their antimicrobial effects for an extended time; therefore, only mouthrinses with high substantivity may be effective against Covid-19.
In-vitro studies demonstrated that different concentrations of povidone-iodine have antiviral effects against SARSCOV-2 [15,16,17,18]. Some other studies investigated the effects of hydrogen peroxide, cetylpyridinium chloride, ethanol, and essential oil mouthwashes on Covid-19 [15, 19]. An in-vitro study examined the virucidal effects of 8 different oral rinses. In this study, researchers added mouthrinses to viral suspension and a particular substance simulating the oral environment. The results showed that dequalinium chloride, benzalkonium chloride, ethanol, and povidone-iodine had significantly more antiviral effects compared to other compounds. They concluded that commercially available oral rinses inactivated SARS-CoV-2 within a short exposure time [15].
Hydrogen peroxide eliminates microorganisms of the oral cavity by degradation into oxygen and water. Hossainian et al. found that hydrogen peroxide mouthwashes did not consistently control the microbiota of the oral cavity [40]. Despite the safety of hydrogen peroxide in the short time, long-term use might have carcinogenic effects. According to Filho J et al., H2O2 mouthwashes should not be continuously recommended for patients with Covid-19 because there is no approved evidence that H2O2 prevents Covid-19 syndromes or prevents the virus from spreading [41]. However, Peng et al. found that 1% hydrogen peroxide or 0.2% povidone-iodine reduced the microbial and viral load when using a rubber dam was not possible [8]. In the oral cavity, hydrogen peroxide will be inactivated due to the host catalase activity [42].
PVP-I is a water-soluble iodophor composed of iodine and polyvinylpyrrolidone as a water-soluble polymer [43]. The free iodine molecule penetrates the microorganism, oxidizes surface proteins, and disrupts nucleotides and fatty acids, causing cell death [43]. Povidone‐iodine has a broad spectrum of antimicrobial effects against bacteria, fungi and different viruses. In one study, 0.23% povidone-iodine mouthrinse showed a significant reduction in bactericidal activity and inactivated influenza virus and MERS-COV [16]. PVP-I is more effective than other common antimicrobial agents such as chlorhexidine, Octenidine, and polyhexinide [44]. It has been demonstrated that PVP-I had sustained effects for more than 4 h [45]. Oxidation mouthwashes, such as povidone-iodine may reduce the salivary viral load of SARS-COV-2 [46]. A study by Muhamed Khan et al. confirmed that gargling a mouthwash containing 0.5% povidone-iodine was safe for healthcare workers and their patients before oral surgery and ENT examination. No allergy was reported [2]. Parhar et al. found that PVP-I reduced the viral transmission of Covid-19 during upper airway mucosal surgery [47]. There are some contraindication to the use for PVP-I: 1) patients with an allergy to iodine, 2) thyroid disease, 3) pregnancy, 4) treatment with radioactive iodine [48]. Our meta-analysis showed that PVP-I mouthwash could reduce the viral load of SARS-COV-2 in the oral cavity.
CHX is a broad-spectrum antiseptic mouthwash with antibacterial and antiplaque properties [49, 50]. Bernstein et al. reported that CHX has antiviral effects on lipid-enveloped viruses while it has no effects on non-enveloped viruses [51]. In a systematic review by Cavalcante-Leão that included in-vitro studies, the researchers concluded that the use of 1% and 7% PVP-I was more effective than HP and CHX in reducing the viral load of the coronavirus family [52]. Peng et al. also found that CHX was not effective for Covi-19 transmission reduction during dental practices [8]. According to the results of the meta-analysis, it may not be concluded whether CHX or a combination of CHX and HP has antiviral effects against SARS-CoV-2.
Listerine mouthrinses contain four active ingredients (eucalyptol, menthol, methyl salicylate, thymol) as well as inactive constituents such as water, alcohol and benzoic acid. Previous studies demonstrated the effectiveness of Listerine in reducing dental plaque and gingivitis [53]. Moreover, Listerine has a significant efficacy against fungal species. Listerine disrupts the cell walls of microorganisms and inhibits the enzymatic activity of pathogens [54]. In vitro studies have shown that Listerine has virucidal effects. Meiller et al. found that oral rinsing with Listerine for thirty seconds reduced the viral load of HSV-1. They explained that this finding could be extended to other enveloped viruses [55]. Mohamed et al. concluded that Listerine mouthwash was effective against SARS-CoV-2 [38]; however, the study by Mohamed et al. [38] was used for the systematic review but it was not included in the meta-analysis.
CDCM mouthwash contains beta-cyclodextrin and Citrox. A study by Carrouel et al. that evaluated this compound was included in the present systematic review and meta-analysis. Hooper et al. found that 1% CDCM mouthwash significantly inhibited the growth of 14 bacterial and some candida species [56]. It is also effective against Zikavirus [57], enterovirus A71 [58], HIV-1 [59], and influenza A [60]. However, no other published study evaluated the effect of this component on SARS-COV-2 except for the study conducted by Carrouel et al. This study was used for the systematic review but it was not included in the meta-analysis.
CPC is a quaternary ammonium water-soluble compound. CPC can penetrate the cell membrane, raise the endocytic and lysosomal PH, and disrupt the cell activity. In past decades, some clinical trials showed that CPC mouthwashes were effective in gingivitis and plaque control [61]. Gurzawska-Comis et al. found that CPC might have virucidal effects, especially against enveloped viruses [62]. In-vitro studies suggest that CPC disrupts different strains of the influenza virus [63]. Using CPC-containing mouthwashes may not be effective in reducing Covid-19 viral load according to our meta-analysis.
A limited number of clinical trial studies examined the effect of mouthwashes on the viral load of Covid-19 in the saliva. The sample size of some of these experimental studies was small. Therefore, more clinical trial studies with standard sample sizes are required.
Conclusion
Since the oral cavity serves as a reservoir of SARS-CoV-2, using mouthwashes can be effective in Covid-19 patients to prevent the transmission of this virus. PVP-I at 0.5% and 1% concentrations reduced the viral load of SARS-CoV-2 in oropharyngeal, nasopharyngeal, and saliva specimens. Thus, it might be considered as a simple and inexpensive intervention during the Covid-19 pandemic.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- Ct:
-
Cycle threshold
- MD:
-
Mean difference
- PVP-I:
-
Povidone-iodine
- CPC:
-
Cetylpyridinium chloride
- CHX:
-
Chlorhexidine gluconate
- ACE2:
-
Angiotensin-converting enzyme-2
- RdRp:
-
RNA-dependent RNA polymerase
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- D&B checklist:
-
Down and Black checklist
- HP:
-
Hydrogen peroxide
- min:
-
Minutes
- h:
-
Hour
- CI:
-
Confidence Interval
References
Mittal A, Manjunath K, Ranjan RK, Kaushik S, Kumar S, Verma V. COVID-19 pandemic: Insights into structure, function, and hACE2 receptor recognition by SARS-CoV-2. PLoS Pathog. 2020;16(8):e1008762.
Khan MM, Parab SR, Paranjape M. Repurposing 0.5% povidone iodine solution in otorhinolaryngology practice in Covid 19 pandemic. Am J Otolaryngol. 2020;41(5):102618.
Ni W, Yang X, Yang D, Bao J, Li R, Xiao Y, et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit Care. 2020;24(1):422.
Duarte-Neto AN, Monteiro RAA, da Silva LFF, Malheiros D, de Oliveira EP, Theodoro-Filho J, et al. Pulmonary and systemic involvement in COVID-19 patients assessed with ultrasound-guided minimally invasive autopsy. Histopathology. 2020;77(2):186–97.
Hamming I, Timens W, Bulthuis ML, Lely AT, Navis G, van Goor H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol. 2004;203(2):631–7.
Azzi L, Carcano G, Gianfagna F, Grossi P, Gasperina DD, Genoni A, et al. Saliva is a reliable tool to detect SARS-CoV-2. J Infect. 2020;81(1):e45–50.
Zhang XH, Ling JQ. Guidelines on the Prevention and Control of Disease in Dental Practice during the Coronavirus Outbreak. Chin J Dent Res. 2020;23(2):89–94.
Peng X, Xu X, Li Y, Cheng L, Zhou X, Ren B. Transmission routes of 2019-nCoV and controls in dental practice. Int J Oral Sci. 2020;12(1):9.
Ra SH, Lim JS, Kim GU, Kim MJ, Jung J, Kim SH. Upper respiratory viral load in asymptomatic individuals and mildly symptomatic patients with SARS-CoV-2 infection. Thorax. 2021;76(1):61–3.
Gostic K, Gomez AC, Mummah RO, Kucharski AJ, Lloyd-Smith JO. Estimated effectiveness of symptom and risk screening to prevent the spread of COVID-19. Elife. 2020;9.
Siles-Garcia AA, Alzamora-Cepeda AG, Atoche-Socola KJ, Peña-Soto C, Arriola-Guillén LE. Biosafety for Dental Patients During Dentistry Care After COVID-19: A Review of the Literature. Disaster Med Public Health Prep. 2020:1–6.
Carrouel F, Conte MP, Fisher J, Gonçalves LS, Dussart C, Llodra JC, et al. COVID-19: A Recommendation to Examine the Effect of Mouthrinses with β-Cyclodextrin Combined with Citrox in Preventing Infection and Progression. Journal of clinical medicine. 2020;9(4).
Ardizzoni A, Pericolini E, Paulone S, Orsi CF, Castagnoli A, Oliva I, et al. In vitro effects of commercial mouthwashes on several virulence traits of Candida albicans, viridans streptococci and Enterococcus faecalis colonizing the oral cavity. PLoS ONE. 2018;13(11):e0207262.
Fernandez YMM, Exterkate RAM, Buijs MJ, Crielaard W, Zaura E. Effect of mouthwashes on the composition and metabolic activity of oral biofilms grown in vitro. Clin Oral Investig. 2017;21(4):1221–30.
Meister TL, Brüggemann Y, Todt D, Conzelmann C, Müller JA, Groß R, et al. Virucidal Efficacy of Different Oral Rinses Against Severe Acute Respiratory Syndrome Coronavirus 2. J Infect Dis. 2020;222(8):1289–92.
Eggers M, Koburger-Janssen T, Eickmann M, Zorn J. In Vitro Bactericidal and Virucidal Efficacy of Povidone-Iodine Gargle/Mouthwash Against Respiratory and Oral Tract Pathogens. Infect Dis Ther. 2018;7(2):249–59.
Anderson DE, Sivalingam V, Kang AEZ, Ananthanarayanan A, Arumugam H, Jenkins TM, et al. Povidone-Iodine Demonstrates Rapid In Vitro Virucidal Activity Against SARS-CoV-2, The Virus Causing COVID-19 Disease. Infect Dis Ther. 2020;9(3):669–75.
Hassandarvish P, Tiong V, Mohamed NA, Arumugam H, Ananthanarayanan A, Qasuri M, et al. In vitro virucidal activity of povidone iodine gargle and mouthwash against SARS-CoV-2: implications for dental practice. Br Dent J. 2020:1–4.
Bidra AS, Pelletier JS, Westover JB, Frank S, Brown SM, Tessema B. Rapid In-Vitro Inactivation of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Using Povidone-Iodine Oral Antiseptic Rinse. J Prosthodont. 2020;29(6):529–33.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-34.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924.
Gottsauner MJ, Michaelides I, Schmidt B, Scholz KJ, Buchalla W, Widbiller M, et al. A prospective clinical pilot study on the effects of a hydrogen peroxide mouthrinse on the intraoral viral load of SARS-CoV-2. Clin Oral Investig. 2020;24(10):3707–13.
Mohamed NA, Baharom N, Sulaiman WSW, Rashid ZZ, Ken WK, Ali UK, et al. EARLY VIRAL CLEARANCE AMONG COVID-19 PATIENTS WHEN GARGLING WITH POVIDONE-IODINE AND ESSENTIAL OILS – A CLINICAL TRIAL. medRxiv. 2020:2020.09.07.20180448.
Mukhtar K, Qassim S, Al Qahtani SA, Danjuma MI-M, Mohamedali M, Farhan HA, et al. A randomized trial on the regular use of potent mouthwash in COVID-19 treatment. medRxiv. 2021:2020.11.27.20234997.
Martínez Lamas L, Diz Dios P, Pérez Rodríguez MT, Del Campo Pérez V, Cabrera Alvargonzalez JJ, López Domínguez AM, et al. Is povidone iodine mouthwash effective against SARS-CoV-2? First in vivo tests. Oral Dis. 2020.
Yoon JG, Yoon J, Song JY, Yoon SY, Lim CS, Seong H, et al. Clinical Significance of a High SARS-CoV-2 Viral Load in the Saliva. J Korean Med Sci. 2020;35(20):e195.
Seneviratne CJ, Balan P, Ko KKK, Udawatte NS, Lai D, Ng DHL, et al. Efficacy of commercial mouth-rinses on SARS-CoV-2 viral load in saliva: randomized control trial in Singapore. Infection. 2021;49(2):305–11.
Carrouel F, Valette M, Gadea E, Esparcieux A, Illes G, Langlois ME, et al. Use of an antiviral mouthwash as a barrier measure in the SARS-CoV-2 transmission in adults with asymptomatic to mild COVID-19: a multicentre, randomized, double-blind controlled trial. Clin Microbiol Infect. 2021;27(10):1494–501.
Eduardo FP, Corrêa L, Heller D, Daep CA, Benitez C, Malheiros Z, et al. Salivary SARS-CoV-2 load reduction with mouthwash use: A randomized pilot clinical trial. Heliyon. 2021;7(6):e07346.
Chaudhary P, Melkonyan A, Meethil A, Saraswat S, Hall DL, Cottle J, et al. Estimating salivary carriage of severe acute respiratory syndrome coronavirus 2 in nonsymptomatic people and efficacy of mouthrinse in reducing viral load: A randomized controlled trial. J Am Dent Assoc. 2021;152(11):903–8.
Cyril Vitug L, Santiaguel J, Angelica Exconde MA, Ma Teresa Tricia B. Oral Gargle of Ethanol-Based Mouthwash Solution and Its Effects on Adult Patients with Mild Covid-19 Infection: An Open Label-Randomized Controlled Trial: Chest. 2021 Oct;160(4):A2504. doi: https://doi.org/10.1016/j.chest.2021.08.014. Epub 2021 Oct 11.
Anderson ER, Patterson EI, Richards S, Pitol AK, Edwards T, Wooding D, et al. CPC-containing oral rinses inactivate SARS-CoV-2 variants and are active in the presence of human saliva. Journal of medical microbiology. 2022;71(2).
Takeda R, Sawa H, Sasaki M, Orba Y, Maishi N, Tsumita T, et al. Antiviral effect of cetylpyridinium chloride in mouthwash on SARS-CoV-2. Sci Rep. 2022;12(1):14050.
Jain A, Grover V, Singh C, Sharma A, Das DK, Singh P, et al. Chlorhexidine: An effective anticovid mouth rinse. J Indian Soc Periodontol. 2021;25(1):86–8.
Huang YH, Huang JT. Use of chlorhexidine to eradicate oropharyngeal SARS-CoV-2 in COVID-19 patients. J Med Virol. 2021;93(7):4370–3.
Filho JMP, Spanemberg JC, Cardoso JA. Coronavirus pandemic: is H(2)O(2) mouthwash going to overcome the chlorhexidine in dental practices? J Stomatol Oral Maxillofac Surg. 2021;122(5):527–8.
Almanza-Reyes H, Moreno S, Plascencia-López I, Alvarado-Vera M, Patrón-Romero L, Borrego B, Reyes-Escamilla A, Valencia-Manzo D, Brun A, Pestryakov A, Bogdanchikova N. Evaluation of silver nanoparticles for the prevention of SARS-CoV-2 infection in health workers: In vitro and in vivo. PLoS One. 2021;16(8):e0256401.
Keyaerts E, Vijgen L, Maes P, Duson G, Neyts J, Van Ranst M. Viral load quantitation of SARS-coronavirus RNA using a one-step real-time RT-PCR. Int J Infect Dis. 2006;10(1):32–7.
Hossainian N, Slot DE, Afennich F, Van der Weijden GA. The effects of hydrogen peroxide mouthwashes on the prevention of plaque and gingival inflammation: a systematic review. Int J Dent Hyg. 2011;9(3):171–81.
Filho JMP, Spanemberg JC, Cardoso JA. Coronavirus pandemic: is H(2)O(2) mouthwash going to overcome the chlorhexidine in dental practices? J Stomatol Oral Maxillofac Surg. 2020;S2468–7855(20):30267–76.
Kraus FW, Perry WI, Nickerson JF. Salivary catalase and peroxidase values in normal subjects and in persons with periodontal disease. Oral Surg Oral Med Oral Pathol. 1958;11(1):95–102.
Lepelletier D, Maillard JY, Pozzetto B, Simon A. Povidone Iodine: Properties, Mechanisms of Action, and Role in Infection Control and Staphylococcus aureus Decolonization. Antimicrob Agents Chemother. 2020;64(9):e00682-20.
J.M. Lachapelle OC, AF. Casado, B. Leroy, G. Micali, D. Tennstedt, J. Lambert. Antiseptics in the era of bacterial resistance: a focus on povidone iodine. clinical practie. 2013;10(5):579–92.
Domingo MA, Farrales MS, Loya RM, Pura MA, Uy H. The effect of 1% povidone iodine as a pre-procedural mouthrinse in 20 patients with varying degrees of oral hygiene. J Philipp Dent Assoc. 1996;48(2):31–8.
Kurakula M, Rao GSNK. Pharmaceutical assessment of polyvinylpyrrolidone (PVP): As excipient from conventional to controlled delivery systems with a spotlight on COVID-19 inhibition. J Drug Deliv Sci Technol. 2020;60:102046.
Parhar HS, Tasche K, Brody RM, Weinstein GS, O’Malley BW Jr, Shanti RM, et al. Topical preparations to reduce SARS-CoV-2 aerosolization in head and neck mucosal surgery. Head Neck. 2020;42(6):1268–72.
Gray PEA, Katelaris CH, Lipson D. Recurrent anaphylaxis caused by topical povidone-iodine (Betadine). J Paediatr Child Health. 2013;49(6):506–7.
Haydari M, Bardakci AG, Koldsland OC, Aass AM, Sandvik L, Preus HR. Comparing the effect of 0.06% -, 0.12% and 0.2% Chlorhexidine on plaque, bleeding and side effects in an experimental gingivitis model: a parallel group, double masked randomized clinical trial. BMC Oral Health. 2017;17(1):118.
James P, Worthington HV, Parnell C, Harding M, Lamont T, Cheung A, et al. Chlorhexidine mouthrinse as an adjunctive treatment for gingival health. Cochrane Database Syst Rev. 2017;3(3):Cd008676.
Bernstein D, Schiff G, Echler G, Prince A, Feller M, Briner W. In vitro virucidal effectiveness of a 0.12%-chlorhexidine gluconate mouthrinse. J Dent Res. 1990;69(3):874–6.
Cavalcante-Leão BL, de Araujo CM, Basso IB, Schroder AG, Guariza-Filho O, Ravazzi GC, et al. Is there scientific evidence of the mouthwashes effectiveness in reducing viral load in Covid-19? A systematic review. J Clin Exp Dent. 2021;13(2):e179–89.
Alshehri FA. The use of mouthwash containing essential oils (LISTERINE®) to improve oral health: A systematic review. Saudi Dent J. 2018;30(1):2–6.
Chen Y, Wong RW, Seneviratne CJ, Hägg U, McGrath C, Samaranayake LP. Comparison of the antimicrobial activity of Listerine and Corsodyl on orthodontic brackets in vitro. Am J Orthod Dentofacial Orthop. 2011;140(4):537–42.
Meiller TF, Silva A, Ferreira SM, Jabra-Rizk MA, Kelley JI, DePaola LG. Efficacy of Listerine Antiseptic in reducing viral contamination of saliva. J Clin Periodontol. 2005;32(4):341–6.
Hooper SJ, Lewis MA, Wilson MJ, Williams DW. Antimicrobial activity of Citrox bioflavonoid preparations against oral microorganisms. Br Dent J. 2011;210(1):E22.
Zou M, Liu H, Li J, Yao X, Chen Y, Ke C, et al. Structure-activity relationship of flavonoid bifunctional inhibitors against Zika virus infection. Biochem Pharmacol. 2020;177: 113962.
Lalani S, Poh CL. Flavonoids as Antiviral Agents for Enterovirus A71 (EV-A71). Viruses. 2020;12(2).
Li BQ, Fu T, Dongyan Y, Mikovits JA, Ruscetti FW, Wang JM. Flavonoid baicalin inhibits HIV-1 infection at the level of viral entry. Biochem Biophys Res Commun. 2000;276(2):534–8.
Goncharova EP, Kostyro YA, Ivanov AV, Zenkova MA. A Novel Sulfonated Derivative of β-Cyclodextrin Effectively Inhibits Influenza A Virus Infection in vitro and in vivo. Acta Naturae. 2019;11(3):20–30.
Costa X, Laguna E, Herrera D, Serrano J, Alonso B, Sanz M. Efficacy of a new mouth rinse formulation based on 0.07% cetylpyridinium chloride in the control of plaque and gingivitis: a 6-month randomized clinical trial. J Clin Periodontol. 2013;40(11):1007–15.
Gurzawska-Comis K, Becker K, Brunello G, Gurzawska A, Schwarz F. Recommendations for Dental Care during COVID-19 Pandemic. J Clin Med. 2020;9(6):1833.
Popkin DL, Zilka S, Dimaano M, Fujioka H, Rackley C, Salata R, et al. Cetylpyridinium Chloride (CPC) Exhibits Potent, Rapid Activity Against Influenza Viruses in vitro and in vivo. Pathog Immun. 2017;2(2):252–69.
Acknowledgements
Not applicable.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, TE, SZM; Investigation, TE, SZM, ARSH, Data curation and Formal analysis, TE, ARSH; Manuscript drafting TE, SZM, ARSH, MA.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ebrahimi, T., Shamshiri, A.R., Alebouyeh, M. et al. Effectiveness of mouthwashes on reducing SARS-CoV-2 viral load in oral cavity: a systematic review and meta-analysis. BMC Oral Health 23, 443 (2023). https://doi.org/10.1186/s12903-023-03126-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03126-4