
Abstract
Objective
White spot lesions (WSLs), the earliest evidence of enamel demineralization, are considered amenable to intervention to achieve a remineralized or arrested state of caries. The management of WSLs is quite challenging, and there is no definitive cure as yet. We performed a network meta-analysis to assess the efficacy of seven therapies for WSLs and gave a hierarchy of them.
Materials and methods
We systematically searched the PubMed, EMBASE, Cochrane, and Web of Science databases (last search: July 2022) to identify all relevant studies. We limited our search to studies published in English. Randomized controlled designed in vitro/clinical trials related to the efficacy of the seven therapies for WSLs were included. Data extraction was performed independently by two reviewers. The risk of bias (ROB) 2.0 tool from Cochrane and a previous in vitro methodological tool will be used for the quality assessment. Variations in quantitative light-induced fluorescence (QLF), laser fluorescence (LF), and lesions area were the primary outcome measures. Standard mean difference (SMD) was used as the effect size for the Network meta-analysis (NMA). Consistency and inconsistency tests were conducted. The hierarchy of 7 treatment effects was evaluated using surface probabilities under cumulative ranking (SUCRA). Publication bias was evaluated using a bias plot.
Results
Forty-two articles were included in the systematic review. Thirty-one of them, with a total of 1906 participants, were included in the network meta-analysis. The studies owned a low and moderate risk of bias. This analysis does not suffer from significant inconsistency. The difference between 4 groups ‘self-assembled peptide (SAP) P11-4’, ‘P11-4 + Fluoride Varnish (FV)’, ‘Resin Infiltration (RI)’, ‘casein phosphor peptides-amorphous calcium fluoride phosphate (CPP-ACFP)’ and the 'Control' group was found to be statistically significant. Compared to the ‘FV’ and ‘casein phosphor peptides-amorphous calcium phosphate (CPP-ACP)’ groups, the ‘P11-4 + FV” group and ‘RI” group made a significant difference. The hierarchy was evident in the SUCRA values of 7 therapies. P11-4 + FV and RI were considered effective therapies compared to the control group or the FV group (gold standard group).
Conclusions
The available evidence suggests that resin infiltration and P11-4 in combination with fluoride varnish had advantages over gold standard (FV). The effect of tricalcium phosphate-based drugs and fluoride is not very noticeable. Overall, drugs based on P11-4 and resin infiltration will be better therapies. Using more than two drugs in combination also would increase efficacy.
Similar content being viewed by others


Introduction
White spot lesions (WSLs), also known as early caries lesions (ECLs), are the earliest evidence of enamel demineralization and remineralization therapy is a trend in treatment [1,2,3]. WSLs are typically in the international caries detection and assessment system (ICDAS) II 1–2 range [1, 2, 4]. Under physiological conditions, there is a balance between demineralization and remineralization at the enamel surface as a result of altered pH levels [5]. If this balance is disturbed, early caries lesions will appear [3]. It should be mentioned that orthodontic treatments with fixed multibracket appliances hinder the maintenance of oral hygiene, leading to the accumulation of plaque and the progression of dental caries [6,7,8]. WSLs occur precisely in this way. Moreover, WSLs are assumed to correlate with bracket debonding time, raising concerns about orthodontic WSLs. Orthodontic WSLs are considered active until the time of bracket debonding [6, 9, 10]. The management of caries is undergoing a paradigm shift towards the minimally invasive approach, which emphasizes the prevention, reduction, and reversal of caries in incipient lesions [1, 11, 12]. These early lesions are considered amenable to the intervention to achieve a state of remineralization or arrest of caries. If the process of demineralization is not halted, the intact enamel surface will eventually collapse and cavitate [1, 13,14,15].
Fluoride-based strategies are the gold standard for preventing and managing WSLs [2, 16, 17]. Fluoride can interact with saliva at the surface and subsurface of the enamel. And then, it can combine with phosphate and calcium ions to form large new crystals containing more fluoride (Fluor-hydroxyapatite), thus improving remineralization [18]. However, current fluoride therapies have been reported to be flawed, especially caries already manifested as white spots [6, 12, 19, 20]. The casein phosphopeptides (CPP) contain multiple phosphoryl sequences that can stabilize calcium phosphate in nano complexes in solutions like amorphous calcium phosphate (ACP). Through their multiple phosphoryl sequences, the CPP binds to ACP in a metastable solution to prevent the dissolution of the calcium and phosphate ions. The casein phosphor peptides- amorphous calcium phosphate (CPP-ACP) also serves as a reservoir for bioavailable calcium and phosphate, thereby promoting remineralization [18, 21]. But compared to fluoride, the mentioned properties of CPP-ACP do not perform well in the treatment results [22,23,24]. The clinically significant benefit of tricalcium phosphate product over fluoride cannot be performed [6, 25, 26]. The self-assembling peptide P11-4(SAP P11-4) provides a novel opportunity for the remineralization therapy of WSLs through the mechanism of biomimetic mineralization [6, 27,28,29]. The current findings suggest that P11-4 has superior performance in the treatment of WSLs compared to the gold standard fluoride [12, 15, 30, 31]. Resin infiltration (RI) has also emerged as an effective method to treat WSLs by minimally invasive means [32, 33].
There have been many clinical studies exploring the differences between the methods of treating WSLs, but there isn't a broadly accepted conclusion [32, 34,35,36,37]. It is unrealistic to conduct a comparative study of all treatment modalities for WSLs at one time. Traditional meta-analyses have also been performed to compare the differences between two or several treatments [38,39,40,41]. In contrast to traditional meta-analyses, network meta-analyses (NMA) allow for the inclusion of evidence from direct and indirect comparisons across different intervention research networks to create multiple hierarchies of intervention effects, even where two interventions comparisons are lacking [42,43,44]. A comparison of the many treatment options and standard procedures for WSLs is necessary [45]. To date, however, no comparison of WSLs’ therapies has been performed using a network meta-analysis with relatively sufficient evidence. Therefore, this study aimed to perform a systematic review and network meta-analysis to compare the aforementioned therapies for contributing to the establishment of clinical treatment guidelines for WSLs [41].
Methods and analysis
Registration
The systematic review and network meta-analysis are reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [46]. The study protocol was registered (registration number: CRD42022343703) with the International Prospective Register of Systematic Reviews (PROSPERO).
Search strategy
Two researchers (Xie and Yu) independently searched for meta-analysis articles published in the following databases: Web of Science, EMBASE, PubMed, and Cochrane Central Register of Controlled Trials. They used medical topic headings (MeSH) and free-text terms. The search time frame was from January 2007 to June 2022. The search strategies are based on the PICOS principle, which can be found in Supplementary Table.
Selection of researches and eligibility criteria
The two reviewers (Xie and Yu, blinded to each other) independently completed the screening of the studies using a specifically designed data extraction form. The disagreement will be solved by Li using an inner decision system. Trials were considered eligible according to inclusion and exclusion criteria. The following are detailed criteria in Table 1.
In the research, it was necessary to exclude diseases with similar treatment modalities to WSLs, such as deep caries, root caries, and fluorosis [47,48,49,50,51]. Systemic and structural barriers also limit dental health for individuals with special healthcare needs (SHCN) [52]. For intervention, in contrast to resin infiltration, conventional composite resin filling is contrary to the current treatment philosophy of managing WSLs [53, 54]. We also had to confront several studies that explored drug concentrations, frequency of use, and use of novel forms of treatment [55,56,57]. We had difficulty performing a network meta-analysis of these unique forms of intervention. For this research, we tend to analyze measures that have specific values. Visual indicators such as visual analog scale (VAS) may introduce a potential bias, which also questions the accuracy of optical indicators [50, 58]. Conventional fluoride varnish has to be applied repeatedly ranging from once every 2 weeks to four topical applications a year to maintain its effectiveness [31, 59]. It is necessary to set a follow-up time ADDIN EN.CITE. Non-RCT designed and plagiarized articles are not eligible for review.
Data extraction
The following data will be extracted by two blinded reviewers using EXCEL software, Author and journal; Publication year; Study design; Participants and groups; Baseline characters; Intervention; Comparison; Outcome; Results, and Follow-up period. The data will be extracted from the full text or if missing data is present, the author will be contacted via email. The disagreement will be solved by Li using an inner decision system.
Risk of bias in individual studies
For clinical research, the ROB 2.0 tool from Cochrane will be used for the quality assessment [60]. The risk of bias will be assessed based on the following five parts: randomization process, deviations from intended interventions, missing outcome data, measurement, and selection of the reported results. The overall risk of bias was expressed as 'low risk of bias' if all domains were categorized as low risk, 'some concerns' if a certain concern was raised in at least one area but was not classified as high risk in any other area, or ‘high risk of bias’ if at least one domain has been classified as high risk, or if it has multiple domains with certain concerns [60]. The methodological quality assessment tool for included in vitro study was from previous systematic reviews of in vitro studies [61, 62]. The risk of bias in each article was evaluated according to the description of the following parameters: specimen randomization; single-operator protocol implementation; blinding of the testing machine operator; the presence of a control group; standardization of the sample preparation; outcome mode evaluation; use of all materials according to the manufacturer’s instructions; description of the sample size calculation. If the reviewers stated the parameter, the study received a “YES” for that specific parameter. In the case of missing data, the parameter received a “NO.” The risk of bias was classified regarding the sum of “YES” answers received: 1 to 3 indicated a high bias, 4 to 6 medium, and 7 to 8 indicated a low risk of bias. All quality assessment processes are carried out by two blinded researchers (Xie and Yu), with Li responsible for resolving disputes arising from this process.
Data analysis
We performed a network meta-analysis to analyze direct and indirect comparisons of the six different therapies and the control treatment using a multivariable meta-analysis model with the STATA 15.1 statistical software (Stata Corp. College Station, Texas, USA).
The outcome of interest is the variation (from baseline to endpoint) in the absolute value of the lesion metric, such as QLF (quantitative photo-induced fluorescence), LF (DIAGNOdent measurement pen), or lesion area, which is typically measured by image analysis. Where studies did not provide a standard deviation (SD) of the change in outcomes, these values were estimated using a correlation coefficient (r) of 0.5 and the following equation:
According to the Cochrane Handbook guideline [63]. Since these changes were continuous outcomes by various measurements, the effect sizes were calculated as SMDs and 95% confidence intervals (CIs). The difference between the drugs was considered significant when the 95%CI for SMD did not include 0 (equivalent to P < 0.05). We conducted an inconsistency analysis to explore differences between the direct and various indirect effect estimates for the same comparison [42, 64]. Inconsistency between direct and indirect comparisons may indicate transitivity that is not immediately obvious [42, 65]. The side-split test was used to analyze the local inconsistency. After that, a consistency model was used for network meta-analysis. To rank the effects of the treatment regimens, we used surface probabilities under cumulative ranking (SUCRA) [66]. A SUCRA of x% indicates that the intervention achieves x% of the effectiveness of the imaginary intervention; thus, larger SUCRAs indicate more preferable interventions [42]. The forest plot was based on the consistency model. Additionally, publication bias was assessed using a comparison-adjusted funnel plot.
Results
Search results
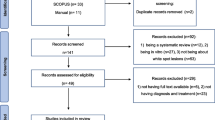
Our search strategy identified 3032 studies from four primary databases. Furthermore, we identified ten additional studies after reviewing the reference lists of all eligible articles and recent systematic reviews. Following the removal of 660 duplicate records removed, 2382 records were evaluated. When 2033 non-RCT records were removed, 349 articles were included in the final eligible assessment. Subsequently, 42 studies fulfilled the requirements of the systematic review [1, 2, 6, 12, 15, 22, 26, 30,31,32, 34, 36, 37, 67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95]. Eleven studies were excluded from the NMA because the format of the results or the quantity of interventions is not appropriate for use in NMA [22, 26, 34, 67, 71,72,73, 76, 81, 83, 86]. Among the 31 studies included in NMA, the following treatment conditions were evaluated: CPP-ACP [10]; CPP-ACFP (6 studies); Control (22 studies); FV (21 studies); P11-4(7 studies); P11-4 + FV (5 studies); RI (5 studies). As 2 studies provided 2 additional outcomes, 33 results from 31 studies were included in the meta-analysis.
The flow chart of the literature retrieval process is shown in Fig. 1.

Flowchart diagram of randomized controlled trials of WSL/ECL’s therapies
Characteristics of the included studies
Data extraction results were displayed in the following Table 2. All articles were RCT-designed research. Articles reporting sex ratios were relatively balanced. For most articles, the participants were in the range of children and adolescents. 29/36 in vivo articles were focused on permanent teeth, while 7/36 in vivo articles focused on primary teeth. Six studies did not provide a detailed message regarding the age of the participants because these were in vitro-engineered lesions. Five articles focused on the different kinds of toothpaste used in daily life, which made them lacking the appropriate interventions and absent in NMA [2, 71, 73, 76, 81]. 2 articles provide additional records for NMA [12, 89]. In 42 studies, 35.7% orthodontics WSLs, 4.8% non-orthodontics WSLs, 16.7% WSLs without special introductions, 7.1% ACLs,19.0% ECLs, 2.4% molar incisor hypo-mineralization (MIH) [75] and 14.3% artificial lesions compose all lesions. But a single ACL study with a description of ICDAS = 2 resulted in its inclusion in NMA [68]. Due to the uncertainty of using fluoride toothpaste in oral education (Some articles have explicit descriptions, others do not), we did not consider the efficacy of fluoride toothpaste in this study. Two studies were on occlusal surface lesions [15, 30], where the outcomes were generally consistent with those of smooth surface lesions. One study studied both occlusal surface and smooth surface [95] with a mild difference observed between them, while the rest of the studies were on smooth surface lesions or smooth surface lesions associated with orthodontic brackets.
Results of ROB assessment
Thirty-six clinical articles were evaluated by ROB 2.0 for the risk of bias. Figure 2 provides details of ROB evaluation in each included clinical study. Overall, 12 articles were judged to be of low ROB, 22 of moderate ROB, and the remaining two were assessed as high ROB. The majority of studies receive a "yellow" rating because there was no information for randomized queue concealment. The other part is that there is no guarantee of the blinded method of the assessor in evaluating the results and whether the procedures were by a pre-specified analysis plan. There are also risks associated with the absence of a specific description of the bias of the outcomes. One of the two high-risk studies was due to the high-risk assessment obtained during the concealment of randomized cohorts, and the other was due to failure to guarantee the impact of loss to follow-up. Table 3 showed the ROB result of the six in vitro studies. Most of the manuscripts involved were counted with a medium or low risk of bias. The sources of risk are from the sample size calculation, single operator, and operator blinded parameters.

Risk of bias for clinical studies. According to the ROB 2 tool, the risk offset evaluation was carried out from five aspects. Green means low risk, yellow means some concern, and red means high risk. In addition, the overall evaluation results and a bar chart are also shown in the graph
Network meta-analysis
This network meta-analysis included a total of 1906 people with 33 outcomes. Figure 3 showed the network map.

Network Map
Network plot
The network of direct treatment comparisons for the changes in absolute values of the outcomes of the WSLs is illustrated in Fig. 3. The sizes of the node reflect the number of matching trials. As shown in the network plot, the ‘FV’ (22 outcomes) and ‘Control’ groups (22 outcomes) were included in the largest number of treatment comparisons, followed by the ‘CPP-ACP’ (10 outcomes) and ‘P11-4’ (7 outcomes), while the ‘CPP-ACFP’ (6 outcomes), ‘RI’ (5 outcomes) and ‘P11 + FV’ (5 outcomes) groups were less. There were 15 direct comparisons. The lines link direct comparisons, and the thickness of the lines represents the number of trials that compare the two therapies. There were 15 pair-to-pair direct comparison groups. The most frequent intercomparison in the included literature was “FV group VS Control group” (12 direct comparisons), followed by the “CPP-ACP group VS Control group” (8 direct comparisons), “CPP-ACFP group VS Control group” (5 direct comparisons), “FV VS P11-4” (5 direct comparisons) and “FV VS P11-4 + FV” (5 direct comparisons). The other specific quantities are also represented in Table 4.
Consistency and inconsistency analysis
We performed an inconsistency analysis to identify potential inconsistencies between direct and indirect comparisons. The results indicated that there were no significant differences between the direct comparison and the indirect comparison (χ2 = 9.05, P = 0.9388). We also performed the local inconsistency test; the results of the side split test in Table 4 showed that there was no significant difference between the indirect comparison and direct comparison in 15 groups(P > 0.05). Six comparisons lack the results of direct comparisons but only indirect comparisons, which can be also shown in Fig. 3.
Forest plot with the result of NMA
Figure 4a shows the NMA forest plot from the consistency model. We used SMD as the effect size. As shown in Fig. 4a, there was a statistically significant difference between 4 groups (P11-4, P11-4 + FV, RI, CPP-ACFP) and the ‘Control’ group (with 95% CI of SMD < 0). Compared to the ‘FV’ and ‘CPP-ACP’ groups, the ‘P11-4 + FV” and ‘RI” groups showed a significant difference (with 95% CI of SMD < 0). No significant differences were found for other comparisons. Visual displays of point estimates and confidence intervals of relative effects of interventions against a common comparator were shown in Fig. 4b [96]. There were no statistically significant differences in direct and indirect comparisons between these interventions and the control group according to inconsistency analysis.

a Forest Plot, b Forest plots for comparison with the control group
SUCRA ranking
Figure 5 showed the SUCRA of seven therapies. The hierarchy of WSLs' treatments and the SUCRA values are shown in Table 5. The higher the SUCRA value, the higher the ranking. The values of SUCRA used in our study indicated the following hierarchy among the seven treatments: 50.5, 24, 3.3, 31.9, 61.9, 89.7, and 88.7% for the CPP-ACFP, CPP-ACP, Control, FV, P11-4, P11-4 + FV, RI treatments. Figure 6 shows the changes in the absolute value of the outcome identified in association with the seven therapies.

Surface probabilities under cumulative ranking (SUCRA) Values of Seven Therapies. The horizontal axis is the rank sequence from 1 to 7. The vertical axis is cumulative probabilities. Intervention is ranked based on SUCRA. The larger the surface area under the curve and the faster the curve rises, the greater the possibility of being the most efficacious treatment. The specific calculated SUCRA values are shown in Table 4. Con: Control group; FV: Fluoride varnish; P11-4: self-assembling peptide 11–4

Outcome absolute value changes identified in association with The 7 Therapies
Publication bias
The funnel plot fitted to the comparison was symmetrical around the zero line, indicating that there was no evidence of publication bias. The publication bias plot is shown in Fig. 7.

publication bias plot
Discussion
We sought to compare the common therapy effects of white spot lesions and searched as much literature as possible for this network meta-analysis. Several valuable findings from this network analysis may inform standardized treatment procedures for the treatment of WSLs. Firstly, the clinical efficacy of conventional fluoride based as well as CPP-ACP-based remineralization strategies is not statistically significant. Secondly, resin infiltration and P11-4-based treatment strategies ranked high. Finally, we have observed that the combination of drugs improves the effectiveness of remineralization therapy in WSLs. In particular, the combination of the self-assembled peptide P11-4 and the fluoride varnish showed the most excellent efficacy.
Based on the SUCRA probabilities, we created an effect size hierarchy for therapeutic effects. The ‘P11-4 + FV’ and ‘resin infiltration’ interventions had more effective outcomes than the other interventions, followed by ‘P11-4’, ‘CPP-ACFP’, ‘FV’, ‘CPP-ACP’, and ‘Control’ interventions. This result suggests that fluorinated varnishes are not clinically effective compared to the control group [ES: -0.25 95%CI (: -0.51,0.02)], even though fluoride strategies are currently the gold standard for managing WSLs [2, 16, 17]. There have been reports of deficiencies in current fluoride therapies, primarily ineffective in caries that have already manifested as white spots [6, 12, 19, 20]. It has already been supposed that the effects restricted to the enamel surface layer led to the shortcomings of fluoride-based strategies [6, 97].
The NMA on the efficacy of CPP-ACP is also under the current clinical status [35, 98,99,100], with no significant differences either compared to FV [ES: 0.07 95%CI (: -0.29,0.44)] or to the control group [ES: -0.18 95%CI (: -49,0.14)]. CPP-ACP allows for the remineralization of deep lesions [101, 102]. The similarity of CPP-ACP to the fluoride strategy suggests that there are other potential reasons for the remineralization effect. Besides, the study found that SAP P11-4, which can form scaffolds on the enamel surface [6, 27,28,29, 103], exhibited superior remineralization properties than the control group [ES: -0.56 95%CI (: -0.96, -0.15)]. The effectiveness of P11-4 in randomized studies, conventional Meta-analysis, and the NWA suggest to us that it is more relevant to establish micro scaffolds suitable for remineralization than to provide the required ions for remineralization [12, 15, 30, 31, 69, 103,104,105].
We need to be more cautious about the effects of resin infiltration therapy, even though it ranks very highly in this analysis [ES: -0.94 95%CI (: -1.46, -0.43) compared to the control group]. Unlike remineralization therapy, resin infiltration, as a minimally invasive etch-adhesive system, can penetrate deep into caries and significantly improve the aesthetic effect of the surface of caries [50, 106, 107]. This means that resin infiltration therapy did not cause regeneration of the enamel, although the effectiveness of resin infiltration has been favored by many clinical studies and meta-analyses [37, 40, 50, 108]. Visual indicators such as visual analog scale (VAS) may introduce a potential bias, which also questions the accuracy of optical indicators [50, 58]. Again, this is the reason we did not include these outcomes in the current study. From the results of this research, CPP-ACFP tended over CPP-ACP, and P11-4 + FV combinations also tended over P11-4 alone. Combination therapy appears to be more appropriate for the treatment of WSLs. The combined application of P11-4 and fluoride varnish holds the highest ranking [ES: -0.96 95%CI (: -1.44, -0.48) compared to the control group], probably due to the formation of precursor scaffolds while providing the ion pool required for remineralization. In summary, the precursor scaffolds and remineralization ion pools together facilitate the management and treatment of WSLs.
We would like to stress here the importance of this study and some methodological necessities. Firstly, there is still no network meta-analysis of WSLs, and in particular, there is a lack of a comprehensive evaluation system for multiple remineralization therapies and resin infiltration therapies. Secondly, there is an urgent need for standardization of current clinical strategies regarding WSLs. Our study will provide an important reference for this. In addition, to match the standardization in the definition of WSLs, we chose 2007 as the starting year for the search. The ICDAS II standards were theoretically discussed in 2005 by the ICDAS work-shop [4, 109, 110]. It’s necessary promoting the changes in caries-related clinical decision-making strategies [111]. It often takes time. It was at the 54th ORCA Congress in 2007 that the ICDAS II criteria became a keyword in the diagnostic section compared to the ICDAS criteria in the 53rd ORCA Congress [112, 113]. Finally, the use of SUCRA alone for comparison of treatment outcomes in NMA is not adequate. Therefore, we used an inconsistency test (Table 4), SUCRA statistic (Table 5 and Fig. 5), and visual displays of point estimates and confidence intervals of relative effects of interventions against a common comparator (Fig. 4b) in this NMA to aid in interpretation [96].
We have equally carefully considered the limitations of this study. Most notably, there remains a paucity of trials in this space that can inform direct comparisons, in particular, the top-ranked interventions. The vast majority of direct comparison studies are relative to FV or control groups. Besides, we did not discuss potential influencing factors for WSL, such as gender, age, follow-up time, outcome measuring tool, etc. This is because the data indicating these contents are difficult to unify. Finally, we also recognize the potential bias that comes from setting language limits. However, there was no regional selection bias in this study. We also compared other systematic reviews that were not included in other languages to identify possible bias [114, 115].
Overall, this systematic review and network meta-analysis points to the clinical advantages of resin infiltration and SAP P11-4 (in combination with fluorinated varnish or as a single agent). This study clarifies the hierarchy of multiple therapies for WSLs and informs clinical strategies for WSLs. We plan to attempt analyses of confounding factors in the future to provide more reference value for the standardization of WSLs treatment.
Conclusions
Our study compared and evaluated the effects of the treatment for WSLs. Both resin infiltration and SAP P11-4 have a positive therapeutic effect on WSLs. The clinical efficacy of both CPP-ACP-based and fluoride-based drugs is not significant. The combination of SAP P11-4 and fluoride varnish is a better strategy for treating WSLs.
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its supplementary information files].
References
Kobeissi R, Badr SB, Osman E. Effectiveness of self-assembling peptide P(11)-4 compared to tricalcium phosphate fluoride varnish in remineralization of white spot lesions: a clinical randomized trial. Int J Clin Pediatr Dent. 2020;13(5):451–6.
Al-Batayneh OB, Bani Hmood EI, Al-Khateeb SN. Assessment of the effects of a fluoride dentifrice and GC Tooth Mousse on early caries lesions in primary anterior teeth using quantitative light-induced fluorescence: a randomised clinical trial. Eur Arch Paediatr Dent. 2020;21(1):85–93.
Gugnani N, Pandit IK, Gupta M, Josan R. Caries infiltration of noncavitated white spot lesions: a novel approach for immediate esthetic improvement. Contemp Clin Dent. 2012;3(Suppl 2):S199-202.
Dikmen B. Icdas II criteria (international caries detection and assessment system). J Istanb Univ Fac Dent. 2015;49(3):63–72.
Burne RA, Marquis RE. Alkali production by oral bacteria and protection against dental caries. FEMS Microbiol Lett. 2000;193(1):1–6.
Welk A, Ratzmann A, Reich M, Krey KF, Schwahn C. Effect of self-assembling peptide P(11)-4 on orthodontic treatment-induced carious lesions. Sci Rep. 2020;10(1):6819.
Staudt CB, Lussi A, Jacquet J, Kiliaridis S. White spot lesions around brackets: in vitro detection by laser fluorescence. Eur J Oral Sci. 2004;112(3):237–43.
Mattousch TJ, van der Veen MH, Zentner A. Caries lesions after orthodontic treatment followed by quantitative light-induced fluorescence: a 2-year follow-up. Eur J Orthod. 2007;29(3):294–8.
Ren Y, Jongsma MA, Mei L, van der Mei HC, Busscher HJ. Orthodontic treatment with fixed appliances and biofilm formation–a potential public health threat? Clin Oral Investig. 2014;18(7):1711–8.
Nyvad B, Baelum V. Nyvad criteria for caries lesion activity and severity assessment: a validated approach for clinical management and research. Caries Res. 2018;52(5):397–405.
Featherstone JDB, Chaffee BW. The evidence for Caries Management by Risk Assessment (CAMBRA®). Adv Dent Res. 2018;29(1):9–14.
Sedlakova Kondelova P, Mannaa A, Bommer C, Abdelaziz M, Daeniker L, di Bella E, et al. Efficacy of P(11)-4 for the treatment of initial buccal caries: a randomized clinical trial. Sci Rep. 2020;10(1):20211.
Young DA, Kutsch VK, Whitehouse J. A clinician's guide to CAMBRA: a simple approach. Compend Contin Educ Dent. 2009;30(2):92–4, 6, 8, passim.
Ismail AI, Sohn W, Tellez M, Amaya A, Sen A, Hasson H, et al. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol. 2007;35(3):170–8.
Doberdoli D, Bommer C, Begzati A, Haliti F, Heinzel-Gutenbrunner M, Juric H. Randomized clinical trial investigating self-assembling peptide P(11)-4 for treatment of early occlusal caries. Sci Rep. 2020;10(1):4195.
Fontana M. Enhancing fluoride: clinical human studies of alternatives or boosters for caries management. Caries Res. 2016;50(Suppl 1):22–37.
Amaechi BT, van Loveren C. Fluorides and non-fluoride remineralization systems. Monogr Oral Sci. 2013;23:15–26.
Lata S, Varghese NO, Varughese JM. Remineralization potential of fluoride and amorphous calcium phosphate-casein phospho peptide on enamel lesions: An in vitro comparative evaluation. J Conserv Dent. 2010;13(1):42–6.
Petersson LG, Twetman S, Pakhomov GN. The efficiency of semiannual silane fluoride varnish applications: a two-year clinical study in preschool children. J Public Health Dent. 1998;58(1):57–60.
Oliveira BH, Salazar M, Carvalho DM, Falcão A, Campos K, Nadanovsky P. Biannual fluoride varnish applications and caries incidence in preschoolers: a 24-month follow-up randomized placebo-controlled clinical trial. Caries Res. 2014;48(3):228–36.
Reynolds EC. Anticariogenic complexes of amorphous calcium phosphate stabilized by casein phosphopeptides: a review. Spec Care Dentist. 1998;18(1):8–16.
Bailey DL, Adams GG, Tsao CE, Hyslop A, Escobar K, Manton DJ, et al. Regression of post-orthodontic lesions by a remineralizing cream. J Dent Res. 2009;88(12):1148–53.
Walker GD, Cai F, Shen P, Bailey DL, Yuan Y, Cochrane NJ, et al. Consumption of milk with added casein phosphopeptide-amorphous calcium phosphate remineralizes enamel subsurface lesions in situ. Aust Dent J. 2009;54(3):245–9.
Pulido MT, Wefel JS, Hernandez MM, Denehy GE, Guzman-Armstrong S, Chalmers JM, et al. The inhibitory effect of MI paste, fluoride and a combination of both on the progression of artificial caries-like lesions in enamel. Oper Dent. 2008;33(5):550–5.
Fernández-Ferrer L, Vicente-Ruíz M, García-Sanz V, Montiel-Company JM, Paredes-Gallardo V, Almerich-Silla JM, et al. Enamel remineralization therapies for treating postorthodontic white-spot lesions: A systematic review. J Am Dent Assoc. 2018;149(9):778-86.e2.
Rechmann P, Bekmezian S, Rechmann BMT, Chaffee BW, Featherstone JDB. MI Varnish and MI Paste Plus in a caries prevention and remineralization study: a randomized controlled trial. Clin Oral Investig. 2018;22(6):2229–39.
Philip N. State of the art enamel remineralization systems: the next frontier in caries management. Caries Res. 2019;53(3):284–95.
Kind L, Stevanovic S, Wuttig S, Wimberger S, Hofer J, Müller B, et al. Biomimetic remineralization of carious lesions by self-assembling peptide. J Dent Res. 2017;96(7):790–7.
Kirkham J, Firth A, Vernals D, Boden N, Robinson C, Shore RC, et al. Self-assembling peptide scaffolds promote enamel remineralization. J Dent Res. 2007;86(5):426–30.
Alkilzy M, Tarabaih A, Santamaria RM, Splieth CH. Self-assembling Peptide P(11)-4 and Fluoride for Regenerating Enamel. J Dent Res. 2018;97(2):148–54.
Lena Sezici Y, Yetkiner E, Aykut Yetkiner A, Eden E, Attin R. Comparative evaluation of fluoride varnishes, self-assembling peptide-based remineralization agent, and enamel matrix protein derivative on artificial enamel remineralization in vitro. Prog Orthod. 2021;22(1):4.
Kannan A, Padmanabhan S. Comparative evaluation of Icon® resin infiltration and Clinpro™ XT varnish on colour and fluorescence changes of white spot lesions: a randomized controlled trial. Prog Orthod. 2019;20(1):23.
Sonesson M, Bergstrand F, Gizani S, Twetman S. Management of post-orthodontic white spot lesions: an updated systematic review. Eur J Orthod. 2017;39(2):116–21.
Yuan H, Li J, Chen L, Cheng L, Cannon RD, Mei L. Esthetic comparison of white-spot lesion treatment modalities using spectrometry and fluorescence. Angle Orthod. 2013;84(2):343–9.
Imani MM, Safaei M, Afnaniesfandabad A, Moradpoor H, Sadeghi M, Golshah A, et al. Efficacy of CPP-ACP and CPP-ACPF for prevention and remineralization of white spot lesions in orthodontic patients: a systematic review of randomized controlled clinical trials. Acta Inform Med. 2019;27(3):199–204.
Gözetici B, Öztürk-Bozkurt F, Toz-Akalın T. Comparative evaluation of resin infiltration and remineralisation of noncavitated smooth surface caries lesions: 6-month results. Oral Health Prev Dent. 2019;17(2):99–106.
Giray FE, Durhan MA, Haznedaroglu E, Durmus B, Kalyoncu IO, Tanboga I. Resin infiltration technique and fluoride varnish on white spot lesions in children: Preliminary findings of a randomized clinical trial. Niger J Clin Pract. 2018;21(12):1564–9.
Tao S, Zhu Y, Yuan H, Tao S, Cheng Y, Li J, et al. Efficacy of fluorides and CPP-ACP vs fluorides monotherapy on early caries lesions: a systematic review and meta-analysis. PLoS One. 2018;13(4): e0196660.
Yengopal V, Mickenautsch S. Caries preventive effect of casein phosphopeptide-amorphous calcium phosphate (CPP-ACP): a meta-analysis. Acta Odontol Scand. 2009;67(6):321–32.
Soveral M, Machado V, Botelho J, Mendes JJ, Manso C. Effect of resin infiltration on enamel: a systematic review and meta-analysis. J Funct Biomater. 2021;12(3).
Singal K, Sharda S, Gupta A, Malik VS, Singh M, Chauhan A, et al. Effectiveness-of calcium phosphate derivative agents on the prevention and remineralization of caries among children- A systematic review & meta-analysis of randomized controlled trials. J Evid Based Dent Pract. 2022;22(3): 101746.
Zhang Y, Liu Y, Su Y, You Y, Ma Y, Yang G, et al. The metabolic side effects of 12 antipsychotic drugs used for the treatment of schizophrenia on glucose: a network meta-analysis. BMC Psychiatry. 2017;17(1):373.
O’Donoghue G, Blake C, Cunningham C, Lennon O, Perrotta C. What exercise prescription is optimal to improve body composition and cardiorespiratory fitness in adults living with obesity? A network meta-analysis. Obes Rev. 2021;22(2): e13137.
Bafeta A, Trinquart L, Seror R, Ravaud P. Reporting of results from network meta-analyses: methodological systematic review. BMJ. 2014;348: g1741.
Lopatiene K, Borisovaite M, Lapenaite E. Prevention and treatment of white spot lesions during and after treatment with fixed orthodontic appliances: a systematic literature review. J Oral Maxillofac Res. 2016;7(2): e1.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71.
Hiraishi N, Sayed M, Takahashi M, Nikaido T, Tagami J. Clinical and primary evidence of silver diamine fluoride on root caries management. Jpn Dent Sci Rev. 2022;58:1–8.
Chen Z, Cao S, Wang H, Li Y, Kishen A, Deng X, et al. Biomimetic remineralization of demineralized dentine using scaffold of CMC/ACP nanocomplexes in an in vitro tooth model of deep caries. PLoS One. 2015;10(1): e0116553.
Mukai Y, Lagerweij MD, ten Cate JM. Effect of a solution with high fluoride concentration on remineralization of shallow and deep root surface caries in vitro. Caries Res. 2001;35(5):317–24.
Bourouni S, Dritsas K, Kloukos D, Wierichs RJ. Efficacy of resin infiltration to mask post-orthodontic or non-post-orthodontic white spot lesions or fluorosis - a systematic review and meta-analysis. Clin Oral Investig. 2021;25(8):4711–9.
Wadia R. Dental fluorosis - bleaching and resin infiltration. Br Dent J. 2020;228(2):82.
Devinsky O, Boyce D, Robbins M, Pressler M. Dental health in persons with disability. Epilepsy Behav. 2020;110: 107174.
Dziaruddin N, Zakaria ASI. Resin infiltration of non-cavitated enamel lesions in paediatric dentistry: a narrative review. Children (Basel). 2022;9(12):1893.
Lin GSS, Chan DZK, Lee HY, Low TT, Laer TS, Pillai MPM, et al. Effectiveness of resin infiltration in caries inhibition and aesthetic appearance improvement of white-spot lesions: an umbrella review. J Evid Based Dent Pract. 2022;22(3): 101723.
Dai Z, Xie X, Zhang N, Li S, Yang K, Zhu M, et al. Novel nanostructured resin infiltrant containing calcium phosphate nanoparticles to prevent enamel white spot lesions. J Mech Behav Biomed Mater. 2022;126: 104990.
Sánchez-Tito M, Tay LY. Antibacterial and white spot lesions preventive effect of an orthodontic resin modified with silver-nanoparticles. J Clin Exp Dent. 2021;13(7):e685–91.
Hosseinpour-Nader A, Karimi N, Ghafari HA. Ex-vivo effects of propolis quantum dots-nisin-nanoquercetin-mediated photodynamic therapy on Streptococcus mutans biofilms and white spot lesions. Photodiagnosis Photodyn Ther. 2022;41: 103255.
Markowitz K, Carey K. Assessing the appearance and fluorescence of resin-infiltrated white spot lesions with caries detection devices. Oper Dent. 2018;43(1):E10–8.
Shah M, Paramshivam G, Mehta A, Singh S, Chugh A, Prashar A, et al. Comparative assessment of conventional and light-curable fluoride varnish in the prevention of enamel demineralization during fixed appliance therapy: a split-mouth randomized controlled trial. Eur J Orthod. 2018;40(2):132–9.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366: l4898.
Hardan L, Devoto W, Bourgi R, Cuevas-Suárez CE, Lukomska-Szymanska M, Fernández-Barrera M, et al. Immediate dentin sealing for adhesive cementation of indirect restorations: a systematic review and meta-analysis. Gels. 2022;8(3).
Bourgi R, Hardan L, Rivera-Gonzaga A, Cuevas SC. Effect of warm-air stream for solvent evaporation on bond strength of adhesive systems: a systematic review and meta-analysis of in vitro studies. Int J Adhes Adhes. 2020;105: 102794.
Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019;10:Ed000142.
Donegan S, Williamson P, D’Alessandro U, Tudur SC. Assessing key assumptions of network meta-analysis: a review of methods. Res Synth Methods. 2013;4(4):291–323.
Song F, Xiong T, Parekh-Bhurke S, Loke YK, Sutton AJ, Eastwood AJ, et al. Inconsistency between direct and indirect comparisons of competing interventions: meta-epidemiological study. BMJ. 2011;343: d4909.
Salanti G, Ades AE, Ioannidis JP. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol. 2011;64(2):163–71.
Vollú AL, Rodrigues GF, Rougemount Teixeira RV, Cruz LR, Dos Santos MG, de Lima Moreira JP, et al. Efficacy of 30% silver diamine fluoride compared to atraumatic restorative treatment on dentine caries arrestment in primary molars of preschool children: A 12-months parallel randomized controlled clinical trial. J Dent. 2019;88: 103165.
Souza BM, Silva MS, Braga AS, Santos D, Carvalho TS, Santos NMD, et al. Acceptability and effect of TiF4 on dental caries: a randomized controlled clinical trial. Braz Oral Res. 2021;35: e121.
Jablonski-Momeni A, Nothelfer R, Morawietz M, Kiesow A, Korbmacher-Steiner H. Impact of self-assembling peptides in remineralisation of artificial early enamel lesions adjacent to orthodontic brackets. Sci Rep. 2020;10(1):15132.
Karabekiroğlu S, Ünlü N, Küçükyilmaz E, Şener S, Botsali MS, Malkoç S. Treatment of post-orthodontic white spot lesions with CPP-ACP paste: A three year follow up study. Dent Mater J. 2017;36(6):791–7.
Yin W, Hu DY, Li X, Fan X, Zhang YP, Pretty IA, et al. The anti-caries efficacy of a dentifrice containing 1.5% arginine and 1450 ppm fluoride as sodium monofluorophosphate assessed using Quantitative Light-induced Fluorescence (QLF). J Dent. 2013;41 Suppl 2:S22–8.
Abdellatif HM, Ali AM, Baghdady SI, ElKateb MA. Caries arrest effectiveness of silver diamine fluoride compared to alternative restorative technique: randomized clinical trial. Eur Arch Paediatr Dent. 2021;22(4):575–85.
Gokce G, Savas S, Kucukyilmaz E, Veli I. Effects of toothpastes on white spot lesions around orthodontic brackets using quantitative light-induced fluorescence (QLF): An in vitro study. J Orofac Orthop. 2017;78(6):480–6.
Bröchner A, Christensen C, Kristensen B, Tranæus S, Karlsson L, Sonnesen L, et al. Treatment of post-orthodontic white spot lesions with casein phosphopeptide-stabilised amorphous calcium phosphate. Clin Oral Investig. 2011;15(3):369–73.
Restrepo M, Jeremias F, Santos-Pinto L, Cordeiro RC, Zuanon AC. Effect of fluoride varnish on enamel remineralization in anterior teeth with molar incisor hypomineralization. J Clin Pediatr Dent. 2016;40(3):207–10.
Esparza-Villalpando V, Fernandez-Hernandez E, Rosales-Berber M, Torre-Delgadillo G, Garrocho-Rangel A, Pozos-Guillén A. Clinical efficacy of two topical agents for the remineralization of enamel white spot lesions in primary teeth. Pediatr Dent. 2021;43(2):95–101.
Güçlü ZA, Alaçam A, Coleman NJ. A 12-week assessment of the treatment of white spot lesions with CPP-ACP paste and/or fluoride varnish. Biomed Res Int. 2016;2016:8357621.
Beerens MW, Ten Cate JM, Buijs MJ, van der Veen MH. Long-term remineralizing effect of MI Paste Plus on regression of early caries after orthodontic fixed appliance treatment: a 12-month follow-up randomized controlled trial. Eur J Orthod. 2018;40(5):457–64.
Beerens MW, van der Veen MH, van Beek H, ten Cate JM. Effects of casein phosphopeptide amorphous calcium fluoride phosphate paste on white spot lesions and dental plaque after orthodontic treatment: a 3-month follow-up. Eur J Oral Sci. 2010;118(6):610–7.
He T, Li X, Dong Y, Zhang N, Zhong Y, Yin W, et al. Comparative assessment of fluoride varnish and fluoride film for remineralization of postorthodontic white spot lesions in adolescents and adults over a 6-month period: A single-center, randomized controlled clinical trial. Am J Orthod Dentofacial Orthop. 2016;149(6):810–9.
Srisilapanan P, Korwanich N, Yin W, Chuensuwonkul C, Mateo LR, Zhang YP, et al. Comparison of the efficacy of a dentifrice containing 1.5% arginine and 1450 ppm fluoride to a dentifrice containing 1450 ppm fluoride alone in the management of early coronal caries as assessed using Quantitative Light-induced Fluorescence. J Dent. 2013;41 Suppl 2:S29–34.
Sitthisettapong T, Doi T, Nishida Y, Kambara M, Phantumvanit P. Effect of CPP-ACP paste on enamel carious lesion of primary upper anterior teeth assessed by Quantitative Light-Induced Fluorescence: A One-Year Clinical Trial. Caries Res. 2015;49(4):434–41.
van der Kaaij NC, van der Veen MH, van der Kaaij MA, ten Cate JM. A prospective, randomized placebo-controlled clinical trial on the effects of a fluoride rinse on white spot lesion development and bleeding in orthodontic patients. Eur J Oral Sci. 2015;123(3):186–93.
Guo X, Li X, Liao C, He K, Zhong Y, He T. Therapeutic effect of a novel bioactive glass-ceramics on early caries lesions: a single-center, randomized controlled clinical trial. Clin Oral Investig. 2022;26(1):217–23.
Singh S, Singh SP, Goyal A, Utreja AK, Jena AK. Effects of various remineralizing agents on the outcome of post-orthodontic white spot lesions (WSLs): a clinical trial. Prog Orthod. 2016;17(1):25.
Turska-Szybka A, Gozdowski D, Mierzwińska-Nastalska E, Olczak-Kowalczyk D. Randomised clinical trial on resin infiltration and fluoride varnish vs fluoride varnish treatment only of smooth-surface early caries lesions in deciduous teeth. Oral Health Prev Dent. 2016;14(6):485–91.
Simon LS, Dash JK, U D, Philip S, Sarangi S. Management of post orthodontic white spot lesions using resin infiltration and CPP-ACP materials- a clinical study. J Clin Pediatr Dent. 2022;46(1):70–4.
Ciftci ZZ, Hanimeli S, Karayilmaz H, Gungor OE. The efficacy of resin infiltrate on the treatment of white spot lesions and developmental opacities. Niger J Clin Pract. 2018;21(11):1444–9.
Bröseler F, Tietmann C, Bommer C, Drechsel T, Heinzel-Gutenbrunner M, Jepsen S. Randomised clinical trial investigating self-assembling peptide P(11)-4 in the treatment of early caries. Clin Oral Investig. 2020;24(1):123–32.
Üstün N, Aktören O. Analysis of efficacy of the self-assembling peptide-based remineralization agent on artificial enamel lesions. Microsc Res Tech. 2019;82(7):1065–72.
Heravi F, Ahrari F, Tanbakuchi B. Effectiveness of MI Paste Plus and Remin Pro on remineralization and color improvement of postorthodontic white spot lesions. Dental Research Journal. 2018;15(2):95–103.
Tomaževič T, Drevenšek M, Kosem R. Evaluation of fluoride varnish treatment of postorthodontic white spot lesions by visual inspection and laser fluorescence-A randomized controlled study. Clin Exp Dent Res. 2022.
Memarpour M, Fakhraei E, Dadaein S, Vossoughi M. Efficacy of fluoride varnish and casein phosphopeptide-amorphous calcium phosphate for remineralization of primary teeth: a randomized clinical trial. Med Princ Pract. 2015;24(3):231–7.
Mehta R, Nandlal B, Prashanth S. Comparative evaluation of remineralization potential of casein phosphopeptide-amorphous calcium phosphate and casein phosphopeptide-amorphous calcium phosphate fluoride on artificial enamel white spot lesion: an in vitro light fluorescence study. Indian J Dent Res. 2013;24(6):681–9.
Llena C, Leyda AM, Forner L. CPP-ACP and CPP-ACFP versus fluoride varnish in remineralisation of early caries lesions. A prospective study. Eur J Paediatr Dent. 2015;16(3):181–6.
Mbuagbaw L, Rochwerg B, Jaeschke R, Heels-Andsell D, Alhazzani W, Thabane L, et al. Approaches to interpreting and choosing the best treatments in network meta-analyses. Syst Rev. 2017;6(1):79.
Müller F, Zeitz C, Mantz H, Ehses KH, Soldera F, Schmauch J, et al. Elemental depth profiling of fluoridated hydroxyapatite: saving your dentition by the skin of your teeth? Langmuir. 2010;26(24):18750–9.
Indrapriyadharshini K, Madan Kumar PD, Sharma K, Iyer K. Remineralizing potential of CPP-ACP in white spot lesions - A systematic review. Indian J Dent Res. 2018;29(4):487–96.
Oliveira GM, Ritter AV, Heymann HO, Swift E Jr, Donovan T, Brock G, et al. Remineralization effect of CPP-ACP and fluoride for white spot lesions in vitro. J Dent. 2014;42(12):1592–602.
Pithon MM, Baião FS, Sant’Anna LID, Tanaka OM, Cople-Maia L. Effectiveness of casein phosphopeptide-amorphous calcium phosphate-containing products in the prevention and treatment of white spot lesions in orthodontic patients: A systematic review. J Investig Clin Dent. 2019;10(2): e12391.
Reynolds EC. Remineralization of enamel subsurface lesions by casein phosphopeptide-stabilized calcium phosphate solutions. J Dent Res. 1997;76(9):1587–95.
Cai F, Shen P, Morgan MV, Reynolds EC. Remineralization of enamel subsurface lesions in situ by sugar-free lozenges containing casein phosphopeptide-amorphous calcium phosphate. Aust Dent J. 2003;48(4):240–3.
Kamal D, Hassanein H, Elkassas D, Hamza H. Comparative evaluation of remineralizing efficacy of biomimetic self-assembling peptide on artificially induced enamel lesions: An in vitro study. J Conserv Dent. 2018;21(5):536–41.
B KA, R Y, Puranik MP. Remineralization of early enamel caries lesions using self-assembling peptides P(11)-4: systematic review and meta-analysis. J Oral Biol Craniofac Res. 2022;12(3):324–31.
Mohamed RN, Basha S, Al-Thomali Y, Saleh Alshamrani A, Salem Alzahrani F, Tawfik EE. Self-assembling peptide P(11)-4 in remineralization of enamel caries - a systematic review of in-vitro studies. Acta Odontol Scand. 2021;79(2):139–46.
Meyer-Lueckel H, Paris S. Improved resin infiltration of natural caries lesions. J Dent Res. 2008;87(12):1112–6.
Kobbe C, Fritz U, Wierichs RJ, Meyer-Lueckel H. Evaluation of the value of re-wetting prior to resin infiltration of post-orthodontic caries lesions. J Dent. 2019;91: 103243.
Nogueira VKC, Mendes Soares IP, Fragelli CMB, Boldieri T, Manton DJ, Bussaneli DG, et al. Structural integrity of MIH-affected teeth after treatment with fluoride varnish or resin infiltration: An 18-Month randomized clinical trial. J Dent. 2021;105: 103570.
Ekstrand KR, Martignon S, Ricketts DJ, Qvist V. Detection and activity assessment of primary coronal caries lesions: a methodologic study. Oper Dent. 2007;32(3):225–35.
Ismail A. Rationale and Evidence for the International Caries Detection and Assessment System (ICDAS II). 2005.
Baelum V. Caries management: technical solutions to biological problems or evidence-based care? J Oral Rehabil. 2008;35(2):135–51.
54th ORCA Congress. July 4–7, 2007, Helsingør, Denmark. pp. 268–294. Caries Research. 2007;41(4):268–94.
53rd ORCA Congress. Caries Research. 2006;40(4):303–58.
McNulty KL, Elliott-Sale KJ, Dolan E, Swinton PA, Ansdell P, Goodall S, et al. The Effects of Menstrual Cycle Phase on Exercise Performance in Eumenorrheic Women: A Systematic Review and Meta-Analysis. Sports Med. 2020;50(10):1813–27.
Lopez P, Radaelli R, Taaffe DR, Newton RU, Galvão DA, Trajano GS, et al. Resistance training load effects on muscle hypertrophy and strength gain: systematic review and network meta-analysis. Med Sci Sports Exerc. 2021;53(6):1206–16.
Acknowledgements
Not applicable
Funding
The funding source of this research is all from Zunxuan Xie's postgraduate research fund of Jilin University, and there is no other funding source.
Author information
Authors and Affiliations
Contributions
Zunxuan Xie: Literature selection, Data extraction, Data analysis, Risk of bias assess, Essay Writing. Lei Yu: Literature selection, Data extraction, Data analysis, Risk of bias assess, Essay Writing. Sining Li: Resolving Disputes, Essay Writing. Jianing Li: Essay Writing, English Consultant. Yuyan Liu: Guidance, English Consultant. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
An ethics statement is not applicable because this study is based exclusively on published literature.
Consent for publication
Not applicable.
Competing interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xie, Z., Yu, L., Li, S. et al. Comparison of therapies of white spot lesions: a systematic review and network meta-analysis. BMC Oral Health 23, 346 (2023). https://doi.org/10.1186/s12903-023-03076-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03076-x