
Abstract
Background
Digital workflow is showing an increasing tendency in everyday dentistry. Accuracy is essential during digital dental workflows for all indication areas. The present study aimed to evaluate the effect of software updates on the accuracy of intraoral scanner (IOS) devices.
Methods
3Shape Trios 3 Pod with software versions 18.1.2. (TRI3_1) and 20.1.2. (TRI3_2); 3Shape Trios 4 Move, version 19.2.2. (TRI4_1); and 3Shape Trios 4 Pod, version 20.1.1. (TRI4_2) were used to take direct optical impressions from a polymethyl methacrylate (PMMA) full arch reference model with prepared teeth (FDI 11,14,17 for crowns and FDI 26 for onlay) and an edentulous region (between FDI 14 and 17). The scanners were used eight times; STL files were imported into Geomagic Control X for accuracy assessment by comparing them to a reference data set created by an industrial high-precision scanner (AICON SmartScan-3D C5). The average deviation of the surface points was calculated in three locations: across a full arch (Parameter 1), the region of a four-unit bridge (Parameter 2), and a single prepared abutment (Parameter 3).
Results
In parameter 1 and 2, the newest model with the latest software (TRI4_2) reached the highest accuracy (31.06 ± 5.24 µm and 21.69 ± 7.50 µm). In parameter 3, an older generation scanner running legacy software produced the highest accuracy: TRI4_1, 11.75 ± 0.35 µm.
Conclusion
Appropriate software updates can significantly increase the trueness and precision of intraoral scanner devices. With updated software, the older generation can match the accuracy level of latest equipment.
Similar content being viewed by others


Background
Digital workflow is showing an increasing tendency in everyday dentistry. The beginning of digital dentistry can be placed in the early’80 s [1]. From that point on, digitalization has constantly been present and evolving in the dental field. By now, intraoral scanners easily exceed the accuracy of conventional impressions up to 4–5-unit bridges. Therefore, more and more dental offices invest to intraoral scanners (IOSs) [2]. Accuracy is essential during digital dental workflows for all indication areas. According to ISO 5725, accuracy comprises precision and trueness [3]. Accuracy means the difference between the quantitative values obtained from the measurement and the actual spatial values of the measured object [4]. Precision is the difference between the repeated measurements on a given target, and trueness expresses how close a measurement’s results are to the actual values of the measured object [5]. Crowns’ and bridges’ marginal and internal fit is the most important criteria for clinically acceptable prosthetic restorations [6]. Clinically acceptable accuracy can be placed between 50 and 120 μm (or less) according to the literature [5,6,7,8,9,10]. Previous studies show that digital workflow is clinically acceptable for solo restorations and short-span bridges [11, 12]. The accuracy of digital impressions decreases as more teeth are scanned [13, 14]. Most intraoral scanners create the 3D virtual model by capturing 2D images and stitching them together with some overlaps. Stitching errors add up to a greater inaccuracy along the full arch [15]. The challenge areas of digital intraoral scanning include implant-supported restorations, full-house bridges and edentulous ridges [16, 17]. Based on the literature, the scanning strategy (the order in which teeth surfaces are to be digitalized) determines the accuracy of digital impressions [18,19,20]. Mennito et al. [21] established that the scanning path influences the accuracy when larger areas are scanned, such as full arch scans. Moreover, Ender et al. [22] found that while the scanning strategy does not affect the accuracy on short-span segments, it has an impact on full arch. Another important aspect is the IOS’s calibration, which can significantly impact accuracy [23]. An additional factor of essence is the lightning conditions, which also affect accuracy [24]. Furthermore, the proficiency of the person who is scanning and the patient’s individual characteristics (such as arch width, extent of mouth opening) can influence the quality of digital impressions [25, 26]. It is well-known that the digital impression-taking has a learning curve; the operator must practice intraoral scanning before confidence in everyday clinical application is achieved [27,28,29].
There is less information in literature about the impact of the hardware and software components on IOS performance [2, 30]. The manufacturer companies continuously develop new generations of intraoral scanners (new hardware and software versions) and software updates (same generations of IOSs with new software version). The updates aim to improve the IOS’s overall performance and capability to capture the intraoral situation more reliably, stably, and rapidly – making digitizing easier for the operator a more comfortable for the patient.
Numerous studies examined the accuracy of intraoral scanners, but only a few attempted to evaluate the effect of software updates on accuracy [2, 30]. Trios 3 and Trios 4 were evaluated in our study since the 3Shape Trios scanners proved to have the high accuracy in the literature, and therefore they are an often used IOS [31, 32].
The present study aimed to investigate the effect of software updates on trueness and precision in case of two different generations of intraoral scanners with four different software versions. The null hypothesis was that there is no association between the software version of the IOSs and the accuracy of digital impressions. The alternative hypothesis was that the newer software version of the IOSs generates a more accurate digital impression.
Methods
Our study examined two generations of intraoral scanners with four different software versions (Table 1). The tested intraoral scanners included the 3Shape Trios 3 (2015) with the 18.1.2. software version introduced to the dental market in 2018 (TRI3_1) and with the 20.1.2. software version introduced in 2020 (TRI3_2), the 3Shape Trios 4 (2019) with the 19.2.2. software version presented in 2019 (TRI4_1), and the 3Shape Trios 4 (2019) with the 20.1.1. software version released to market in 2020 (TRI4_2). The investigated IOSs in the order of software release were the following: TRI3_1 (3Shape Trios 3 18.1.2.), TRI4_1 (3Shape Trios 4 19.2.2.), TRI4_2 (3Shape Trios 4 20.1.1.) and TRI3_2 (3Shape Trios 3 20.1.2.). Trios intraoral scanners use confocal laser scanning technology to capture the virtual model [29]. As a reference, a polymethyl methacrylate (PMMA) model was used (Fig. 1). Supragingival prepared teeth (FDI World Dental Federation) included numbers 11, 14, and 17 for a crown and 26 for an inlay; teeth 15 and 16 were missing.

Reference polymethyl methacrylate model
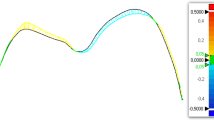
The reference model was scanned by a highly accurate industrial scanner (AICON SmartScan-3D C5; AICON 3D Systems GmbH, Braunschweig, Germany). According to the user guide, the reference scanner’s accuracy was a maximal 8-μm feature accuracy (and a 2-μm resolution limit) [33]. An experienced operator familiar with Trios IOSs made all the digital impressions. The manufacturer-recommended scanning strategy was followed during the process. Scanning was started from the occlusal surface of the left prepared first molar. After capturing the occlusal surface, the tip of the scanner was rotated by 45º, and first the buccal surface then the palatal surface was scanned. Each intraoral scanner device made eight digital impressions, resulting in 8 STL files for the comparison procedure under standard lighting conditions. STL files were imported into the Geomagic Control X program and were compared to the reference model by superimposition. In Geomagic Control X, all STL files were cropped by the same examiner to eliminate any unnecessary parts such as the palatal soft tissue and tuber maxillae. First, an initial alignment was performed, which matched the coordinate system of scan data to the nominal data; then, the best-fit alignment function was used to find the best overall alignment. After superimposition, 3D comparison (gap distance assessment of available surface points) between the reference STL files and files produced by the tested intraoral scanner devices was performed. The measured parameters were the following (Fig. 2):
-
Surface deviation of the full-arch scan: Variation between the digital impressions made by the examined IOSs and the reference dataset. It represents the global accuracy of the full arch. (Parameter 1).
-
Surface deviation of the abutment teeth 14 and 17 and the alveolar ridge between them (four-unit bridge): It presents the distortion effect of the edentulous ridge. (Parameter 2).
-
Surface deviation of the prepared incisor [11]: this parameter indicates a single tooth impression capability – the best accuracy of the IOS (Parameter 3).

Measured parameters: full arch (Parameter 1), the region of a four-unit bridge (Parameter 2), and a single prepared abutment (Parameter 3)
The 3D analysis software exported the root mean square (RMS) values of spatial deviations for use in a statistical software package. The arithmetic means of the RMS values were used to indicate the trueness, and their standard deviation (SD) parameters were used to indicate the precision of the investigated scanner based on an article by Renne, Mennito and Vág in 2021 [30].
Eight individual RMS data points were available for each of the three Parameters described above and each IOS, resulting in a dataset of 96 observations. Scanner performance was described in terms of mean ± SD of RMS. Device versions were compared pairwise using Student's two-sample t-test (if normality assumptions were satisfied) or Wilcoxon's rank-sum test (otherwise). The statistical package Stata was used for data handling and analysis.
Results
Significant differences were found between the generations and between the software versions. The differences in tendencies were not linear, so we cannot state that newer generations and newer software always reproduce the geometry of the oral cavity in a more accurate fashion. The final result depends also on the region under investigation (Table 2, Fig. 3).

Boxplot diagrams of the results. The intraoral scanners are ordered according to the software release date
Accuracy results of parameter 1 (average surface deviation across a full-arch digital impression)
In the case of full-arch digital impressions the accuracy results from lowest to highest accuracy are the following: TRI3_1 (90.24 ± 15.35 µm), TRI4_1 (52.91 ± 7.44 µm), TRI3_2 (47.44 ± 9.17 µm), and TRI4_2 (31.06 ± 5.24 µm). The newest software version with the older hardware cannot reach the accuracy level of the newer hardware with the second-latest software. The updated software reached significantly better accuracy in both generations. We did not find a significant difference in accuracy between TRI4_1 and TRI3_2, which suggests that with the proper software update, the older generation could perform similarly to new equipment in terms of accuracy.
Accuracy results of parameter 2 (average surface deviation across a four-unit bridge)
The observed data showed a decrease in the deviation from perfect trueness and precision as hardware and software evolved.
The accuracy results of teeth 14 and 17 and the edentulous ridge in decreasing order of deviation were the following: TRI3_1 (117.35 ± 20.11 µm), TRI3_2 (45.86 ± 14.84 µm), TRI4_1 (41.04 ± 16.48 µm), and TRI4_2 (21.69 ± 7.50 µm). We found statistically significant differences between the hardware generations and between the majority of software versions, indicating that the newer versions could create more accurate digital impressions, and the distortion effect of the alveolar ridge is getting reduced – the stitching mechanism of the updated software algorithm seems to work better. Although TRI3_2 and TRI4_1 did not have significant accuracy differences between them it can be seen again that the old generation with newer software can reach the accuracy level of the new IOS models.
Accuracy results of parameter 3 (surface of the prepared incisor – 11)
The accuracy results of the prepared tooth 11 in decreasing order of deviation were the following: TRI3_2 (14.45 ± 0.36 µm), TRI3_1 (13.26 ± 0.94 µm), TRI4_2 (12.21 ± 0.71 µm) and TRI4_1 (11.75 ± 0.35 µm). We found a significant difference between TRI3_1 and TRI3_2, but no significance was shown between TRI4_1 and TRI4_2. With this parameter, the latest software produced lower accuracy. The lack-of-precision assessment of the TRI4_2 also produced a greater value. All deviations from perfect trueness were below 20 µm, which is comfortably within the clinically acceptable range.
Discussion
Numerous studies investigated the different properties of IOS: scanning speed, ergonomic properties, special features, accuracy [8, 25, 34,35,36,37]. In this in vitro study the accuracy of intraoral scanners were measured. Accuracy can be measured with different methods. Most studies use special software to compare STL files to a reference data set [7]. The most widely used method is the best-fit alignment. Another possibility is linear distance measurement when gaps between pairs of points are measured [19, 38, 39]. Accuracy has been assessed in many cases by examining prosthetic workflows [7, 40, 41].
In our present study, best-fit alignment was performed. Two different generations of intraoral scanners were used: 3Shape Trios 3 and 3Shape Trios 4. A generation change means, that the manufacturing company upgrades an already existing intraoral scanner (previous generation) in terms of both hardware and software, creating a new version (new generation model) [35]. A software update means a series of changes to fix or improve the program run by the computer. In the literature, limited information is available about the impact of software updates on intraoral scanners performance [30].
This study investigated the effect of software updates on the accuracy of IOS devices. Two different generations of 3Shape Trios intraoral scanners (Trios 3 and Trios 4) and four different software versions were evaluated for their accuracy (trueness and precision). For accuracy, in the literature, the clinically acceptable range for the marginal fit of a restoration is 50 to 120 μm [9, 10]. Examining the accuracy of the full arch is essential because situations when a longer-span or full-house bridge needs to be fabricated occur commonly. Investigating the accuracy of the deviation between two abutments is relevant because of the edentulous region, which can affect the accuracy. The accuracy of a prepared tooth 11 for a crown is vital for examining chairside systems when the indication is a short-span fixed dental prothesis (FPD).
The null hypothesis was rejected on analysis of full arch and bridge scan data: an association between the recency of the software version of the IOSs and a greater accuracy of digital impressions was found.
In case of parameter 1, there was a significant improvement in trueness and precision. The Trios 3, with the latest software version (TRI3_2) was more accurate than the Trios 4 Move with the previous software version (TRI4_1), which is the latest generation of the 3Shape company’s IOS devices. Furthermore, the accuracy of the software updated Trios 4 Pod intraoral scanner (TRI4_2) was better than that of the mentioned Trios 3 (TRI3_2). The latest generation of 3Shape products (Trios 4 Pod) with the updated software (TRI4_2) produced the best accuracy result in our study, except in case of parameter 3, where the Trios 4 Pod with the older software (TRI4_1) proved to have the highest trueness. It is important to highlight that the software run by the Trios 4 Pod was not the latest software version in the dental market. Based on the result, it could be hypothesised that the hardware version of the IOS could impact the accuracy. Ender et. al. [22] in 2019 investigated the full arch and posterior region with two software versions of the CEREC Omnicam. The updated software version produced better accuracy in both parameters.
In the case of parameter 2 significant differences could be seen between the results of the oldest (TRI3_1) and the latest (TRI3_2) software versions of Trios 3 intraoral scanners. The measured data of parameter 2 showed an increasing tendency in trueness and precision compared to parameter 3 (surface deviation of the prepared incisor). It has been stated in previous studies that longer captured distances result in less accurate digital impressions [13].
An edentulous ridge between teeth 14 and 17 is an important part of our measurement because most scanners capture the surfaces with increased inaccuracy across edentulous ridges. Edentulous regions contain less information than tooth surfaces [14, 42]; therefore, it is more difficult for the IOS to stitch the images together. In addition, the size of the edentulous region can affect the recognition of the overlaps, thereby the accuracy [38]. Kim et al. [43] in 2017 investigated the accuracy of IOS on the edentulous region using a 3Shape Trios 3 intraoral scanner device. The average accuracy of the examined IOS (3Shape Trios 3) was 36.1 ± 13.0 µm. In our research, Trios 4 with software version 19.2.2. (TRI4_1) produced almost the same accuracy (41.04 ± 16.48 µm). Furthermore, the Trios 4 with updated software (TRI4_2) provided better accuracy results in the case of trueness and precision (21.69 ± 7.50 µm). The examined edentulous space in our study was shorter than in the mentioned article, which may have caused differences between the results.
In the case of parameter 3, negative impact of software updates on trueness was found. The range of variation across scanner configurations was less than 5 µm, so the difference's clinical impact is negligible. In our research more accurate data were obtained than in the literature: Park et al. [44] examined the accuracy of the 3Shape Trios 3 intraoral scanner in 2016. The accuracy of the examined parameter (solo crown – first incisor) was 49.7 ± 13.0 µm, which is less accurate than our results: TRI3_2, 14.45 ± 0.36 µm and TRI3_1, 13.26 ± 0.94 µm. In our research, two software versions were evaluated in Trios 3: 18.1.2. and 20.1.2. Version 18.1.2. was released in 2018 and 20.1.2. was introduced to the dental market in 2020. The previous research by Park et al. was conducted in 2016. Accordingly, their Trios 3 intraoral scanner was running an earlier software version, which may explain the differences between the results. Another research by Zimmerman et al. [45] examined the accuracy of prepared teeth for solo restorations using the CEREC Omnicam with two different software versions (version 4.6.1 and version 5.0.0). The results showed no significant difference between the two versions in accuracy (v. 4.6.1: 36.7 µm; v. 5.0.0: 40.5 µm). Based on our results, IOSs with legacy software produced almost the same results as IOSs running updated software versions. The difference from the data in the literature may also be due to the shape of the prepared abutment, the distance from the neighbouring teeth as they affect the IOS’s field of vision and thus its accuracy. All measured object has a different geometry making the results not completely comparable [46, 47].
Few studies in the literature evaluate the effect of software updates on the accuracy of intraoral scanners [30]. In further studies, it would be necessary to describe the software version of the IOS and not only the hardware type.
There are some limitations to this study. Our results are based on model scanning procedures (in vitro study); it could be interesting to measure these parameters in clinical circumstances. In clinical situations, numerous factors can impact the accuracy of IOS, such as the saliva flow rate in the oral cavity, the individual characteristics of the patient, and the operator's skills in digital impression-taking. Moreover, our study used only two scanners from the same manufacturer. They use confocal laser technology, and the method of recording data is a video sequence [48]. Many types of intraoral scanners with different data capture modes can produce different results. It would also be interesting to investigate additional intraoral devices for the effects of software updates.
Conclusion
Based on our results the null hypothesis was rejected. Within the current study's limitations, we conclude that new generations of intraoral scanner hardware and software can significantly increase the trueness and precision of the devices when it comes to full-arch scanning. The presence of an edentulous region may still adversely affect the accuracy of the results; however, software updates seem to achieve more accurate STL files. All versions create a clinically acceptable digital impression of a single abutment.
Availability of data and materials
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
References
Miyazaki T, Hotta Y, Kunii J, Kuriyama S, Tamaki Y. A review of dental CAD/CAM: Current status and future perspectives from 20 years of experience. Dent Mater J. 2009;28(1):44–56. https://doi.org/10.4012/dmj.28.44. (PMID: 19280967).
Schmidt A, Klussmann L, Wöstmann B, Schlenz MA. Accuracy of digital and conventional full-arch impressions in patients: An update. J Clin Med. 2020;9(3):688. https://doi.org/10.3390/jcm9030688.PMID:32143433;PMCID:PMC7141355.
Richert R, Goujat A, Venet L, Viguie G, Viennot S, Robinson P, et al. Intraoral Scanner Technologies: A Review to Make a Successful Impression. Journal of Healthcare Engineering. 2017;2017. :8427595. doi: https://doi.org/10.1155/2017/8427595. Epub 2017 Sep 5. PMID: 29065652; PMCID: PMC5605789
De Bièvre P. The 2012 International Vocabulary of Metrology: “VIM.” Accred Qual Assur. 2012;17(2):231–2.
Menditto A, Patriarca M, Magnusson B. Understanding the meaning of accuracy, trueness and precision. Accred Qual Assur. 2007;12(1):45–7. https://doi.org/10.1007/s00769-006-0191.
Pera P, Gilodi S, Bassi F, Carossa S. In vitro marginal adaptation of alumina porcelain ceramic crowns. The Journal of Prosthetic Dentistry [Internet]. 1994 Dec 1 [cited 2019 Jul 9];72(6):585–90. Available from: https://www.sciencedirect.com/science/article/abs/pii/0022391394902895
Nedelcu R, Olsson P, Nyström I, Thor A. Finish line distinctness and accuracy in 7 intraoral scanners versus conventional impression: An in vitro descriptive comparison. BMC Oral Health. 2018;18(1):27. https://doi.org/10.1186/s12903-018-0489-3.PMID:29471825;PMCID:PMC5824445.
Goujat A, Abouelleil H, Colon P, Jeannin C, Pradelle N, Seux D, et al. Marginal and internal fit of CAD-CAM inlay/onlay restorations: A systematic review of in vitro studies. J Prosthet Dent. 2019;121(4):590-597.e3. https://doi.org/10.1016/j.prosdent.2018.06.006. (Epub 2018 Dec 1 PMID: 30509548).
Materials D. Revised American National Standards Institute/American Dental Association Specification No. 8 for Zinc Phosphate Cement. J Am Dent Assoc. 1978;96(1):121–3. https://doi.org/10.14219/jada.archive.1978.0032.
Afify A, Haney S, Verrett R, Mansueto M, Cray J, Johnson R. Marginal discrepancy of noble metal-ceramic fixed dental prosthesis frameworks fabricated by conventional and digital technologies. J Prosthet Dent. 2018;119(2):307.e1-307.e7. https://doi.org/10.1016/j.prosdent.2017.08.012. (Epub 2017 Nov 15 PMID: 29153748).
Ahlholm P, Sipilä K, Vallittu P, Jakonen M, Kotiranta U. Digital Versus Conventional Impressions in Fixed Prosthodontics: A Review. J Prosthodont. 2018;27(1):35–41. https://doi.org/10.1111/jopr.12527. (Epub 2016 Aug 2 PMID: 27483210).
Blatz MB, Conejo J. The Curre nt State o f Chairside Digital Dentistry and Materials. Dental Clinics of NA [Internet]. 2022;63(2):175–97. Available from: https://doi.org/10.1016/j.cden.2018.11.002
Ender A, Attin T, Mehl A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. The Journal of Prosthetic Dentistry [Internet]. 2016 Mar 1 [cited 2019 Jul 5];115(3):313–20. Available from: https://www.sciencedirect.com/science/article/abs/pii/S002239131500551X
Boeddinghaus M, Breloer ES, Rehmann P, Wöstmann B. Accuracy of single-tooth restorations based on intraoral digital and conventional impressions in patients. Clinical Oral Investigations [Internet]. 2015;19(8):2027–34. Available from: https://doi.org/10.1007/s00784-015-1430-7
Park GH, Son KB Da, Lee KB. Feasibility of using an intraoral scanner for a complete-arch digital scan. Journal of Prosthetic Dentistry [Internet]. 2019;121(5):803–10. Available from: https://doi.org/10.1016/j.prosdent.2018.07.014
Hayama H, Fueki K, Wadachi J, Wakabayashi N. Trueness and precision of digital impressions obtained using an intraoral scanner with different head size in the partially edentulous mandible. Journal of Prosthodontic Research [Internet]. 2018;62(3):347–52. Available from: https://doi.org/10.1016/j.jpor.2018.01.003
Andriessen FS, Rijkens DR, van der Meer WJ, Wismeijer DW. Applicability and accuracy of an intraoral scanner for scanning multiple implants in edentulous mandibles: a pilot study. J Prosthet Dent. 2014;111(3):186–94. https://doi.org/10.1016/j.prosdent.2013.07.010. (Epub 2013 Nov 8 PMID: 24210732).
Medina-Sotomayor P, Agustín Pascual M, Isabel Camps A. Accuracy of four digital scanners according to scanning strategy in complete-arch impressions. PLoS ONE. 2018;13(9). e0202916. doi: https://doi.org/10.1371/journal.pone.0202916. Erratum in: PLoS One. 2018 Dec 20;13(12):e0209883. PMID: 30212498; PMCID: PMC6136706.
Vág J, Nagy Z, Simon B, Mikolicz Á, Kövér E, Mennito A, et al. A novel method for complex three-dimensional evaluation of intraoral scanner accuracy. Int J Comput Dent. 2019;22(3):239–49 (PMID: 31463488).
Anh J-W, Park J-M, Chun Y-S, Kim M, Kim M. A comparison of the precision of three-dimensional images acquired by 2 digital intraoral scanners: effects of tooth irregularity and scanning direction. Korean journal of orthodontics. 2016 Jan;46(1):3–12. doi: https://doi.org/10.4041/kjod.2016.46.1.3. Epub 2016 Jan 25. PMID: 26877977; PMCID: PMC4751299.
Mennito AS, Evans ZP, Lauer AW, Patel RB, Ludlow ME, Renne WG. Evaluation of the effect scan pattern has on the trueness and precision of six intraoral digital impression systems. J Esthet Restor Dent. 2018;30(2):113–8. https://doi.org/10.1111/jerd.12371. (Epub 2018 Feb 24 PMID: 29476599).
Ender A, Zimmermann M, Mehl A. Accuracy of complete- and partial-arch impressions of actual intraoral scanning systems in vitro. International journal of computerized dentistry [Internet]. 2019;22(1):11–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30848250
Rehmann P, Sichwardt V, Wöstmann B. Intraoral Scanning Systems: Need for Maintenance. Int J Prosthodont. 2017;30(1):27–9. https://doi.org/10.11607/ijp.4976. (PMID: 28085974).
Revilla-León M, Jiang P, Sadeghpour M, Piedra-Cascón W, Zandinejad A, Özcan M, et al. Intraoral digital scans: Part 2-influence of ambient scanning light conditions on the mesh quality of different intraoral scanners. J Prosthet Dent. 2020;124(5):575–80. https://doi.org/10.1016/j.prosdent.2019.06.004. (Epub 2019 Dec 20 PMID: 31870612).
Abduo J, Elseyoufi M. Accuracy of Intraoral Scanners: A Systematic Review of Influencing Factors. Eur J Prosthodont Restor Dent. 2018;26(3):101–21. https://doi.org/10.1922/EJPRD_01752Abduo21. (PMID: 29989757).
Patzelt SBM, Emmanouilidi A, Stampf S, Strub JR, Att W. Accuracy of full-arch scans using intraoral scanners. Clin Oral Invest. 2014;18(6):1687–94. https://doi.org/10.1007/s00784-013-1132-y. (Epub 2013 Nov 17 PMID: 24240949).
Róth I, Czigola A, Joós-Kovács GL, Dalos M, Hermann P, Borbély J. Learning curve of digital intraoral scanning – an in vivo study. BMC Oral Health. 2020;20(1):1–7. https://doi.org/10.1186/s12903-020-01278-1.PMID:33076894;PMCID:PMC7574448.
Al Hamad KQ. Learning curve of intraoral scanning by prosthodontic residents. Journal of Prosthetic Dentistry [Internet]. 2020;123(2):277–83. Available from: https://doi.org/10.1016/j.prosdent.2019.04.003
Kim J, Park J-M, Kim M, Heo S-J, Shin IH, Kim M. Comparison of experience curves between two 3-dimensional intraoral scanners. J Prosthet Dent. 2016;116(2):221–30. https://doi.org/10.1016/j.prosdent.2015.12.018. (Epub 2016 Apr 7 PMID: 27061634).
Vág J, Renne W, Revell G, Ludlow M, Mennito A, Teich ST, et al. The effect of software updates on the trueness and precision of intraoral scanners. Quintessence international (Berlin, Germany : 1985). 2021 Jun;52(7):636–44. doi: https://doi.org/10.3290/j.qi.b1098315. PMID: 33749223.
Treesh JC, Liacouras PC, Taft RM, Brooks DI, Raiciulescu S, Ellert DO, et al. Complete-arch accuracy of intraoral scanners. J Prosthet Dent. 2018;120(3):382–8. https://doi.org/10.1016/j.prosdent.2018.01.005. (Epub 2018 Apr 30 PMID: 29724554).
Hack GD, Patzelt SBM. Evaluation of the Accuracy of Six Intraoral Scanning. American Dental Association. 2015;10(4):1–5.
Hexagon ADSG‐Po. stereoSCAN neo R16 — 16 0 Megapixel [Official Page]. https://www.creativeinfocom. com/pdfs/stereoscan‐neo‐specification‐r16.pdf.]. stereo SCAN neo. p. 6–7.
Róth I, Czigola A, Fehér D, Vitai V, Levente G, Kovács J, et al. Digital intraoral scanner devices : a validation study based on common evaluation criteria. BMC Oral Health [Internet]. 2022;1–17. Available from: https://doi.org/10.1186/s12903-022-02176-4
Mangano F, Gandolfi A, Luongo G, Logozzo S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health. 2017;17(1):1–11. https://doi.org/10.1186/s12903-017-0442-x.PMID:29233132;PMCID:PMC5727697.
Siqueira R, Galli M, Chen Z, Mendonça G, Meirelles L, Wang HL, et al. Intraoral scanning reduces procedure time and improves patient comfort in fixed prosthodontics and implant dentistry: a systematic review. Clin Oral Invest. 2021;25(12):6517–31. https://doi.org/10.1007/s00784-021-04157-3PMCID:OMC8475874. (PMID: 34658955).
Giachetti L, Sarti C, Cinelli F, Russo DS. Accuracy of Digital Impressions in Fixed Prosthodontics: A Systematic Review of Clinical Studies. Int J Prosthodont. 2020;33(2):192–201. https://doi.org/10.11607/ijp.6468. (PMID: 32069344).
Vecsei B, Joós-Kovács G, Borbély J, Hermann P. Comparison of the accuracy of direct and indirect three-dimensional digitizing processes for CAD/CAM systems – An in vitro study. J Prosthodont Res. 2017;61(2):177–84. https://doi.org/10.1016/j.jpor.2016.07.001. (Epub 2016 Jul 25 PMID: 27461088).
Lee SJ, Betensky RA, Gianneschi GE, Gallucci GO. Accuracy of digital versus conventional implant impressions. Clinical oral implants research. 2015 Jun;26(6):715–9. doi: https://doi.org/10.1111/clr.12375. Epub 2014 Apr 10. PMID: 24720423; PMCID: PMC4428303.
Ferrini F, Sannino G, Chiola C, Capparé P, Gastaldi G, Gherlone EF. Influence of intra-oral scanner (I.O.S.) on the marginal accuracy of CAD/CAM single crowns. International Journal of Environmental Research and Public Health. 2019;16(4):1–9. doi: https://doi.org/10.3390/ijerph16040544. PMID: 30769768; PMCID: PMC6406818.
Bindl A, Mörmann WH. Marginal and internal fit of all-ceramic CAD/CAM crown-copings on chamfer preparations. J Oral Rehabil. 2005;32(6):441–7. https://doi.org/10.1111/j.1365-2842.2005.01446.x. (PMID: 15899023).
Imburgia M, Logozzo S, Hauschild U, Veronesi G, Mangano C, Mangano FG. Accuracy of four intraoral scanners in oral implantology: a comparative in vitro study. BMC Oral Health [Internet]. 2017;17(1):92. Available from: https://doi.org/10.1186/s12903-017-0383-4
Kim JE, Amelya A, Shin Y, Shim JS. Accuracy of intraoral digital impressions using an artificial landmark. J Prosthet Dent. 2017;117(6):755–61. https://doi.org/10.1016/j.prosdent.2016.09.016. (Epub 2016 Nov 15 PMID: 27863856).
Park JM. Comparative analysis on reproducibility among 5 intraoral scanners: Sectional analysis according to restoration type and preparation outline form. Journal of Advanced Prosthodontics. 2016;8(5):354–62. doi: https://doi.org/10.4047/jap.2016.8.5.354. Epub 2016 Oct 21. PMID: 27826385; PMCID: PMC5099127.
Zimmermann M, Ender A, Mehl A. Local accuracy of actual intraoral scanning systems for single-tooth preparations in vitro. J Am Dent Assoc. 2020;151(2):127–35. https://doi.org/10.1016/j.adaj.2019.10.022. (Epub 2019 Dec 26 PMID: 31883705).
Huang MY, Son KB Da, Lee KB. Effect of distance between the abutment and the adjacent teeth on intraoral scanning: An in vitro study. Journal of Prosthetic Dentistry [Internet]. 2021;125(6):911–7. Available from: https://doi.org/10.1016/j.prosdent.2020.02.034
Carbajal Mejía JB, Wakabayashi K, Nakamura T, Yatani H. Influence of abutment tooth geometry on the accuracy of conventional and digital methods of obtaining dental impressions. J Prosthet Dent. 2017;118(3):392–9. https://doi.org/10.1016/j.prosdent.2016.10.021. (Epub 2017 Feb 17 PMID: 28222873).
Güth JF, Keul C, Stimmelmayr M, Beuer F, Edelhoff D. Accuracy of digital models obtained by direct and indirect data capturing. Clin Oral Invest. 2013;17(4):1201–8. https://doi.org/10.1007/s00784-012-0795-0. (Epub 2012 Jul 31 PMID: 22847854).
Acknowledgements
Special thanks to 4iD Nyrt. for the helpful contribution and Dr. Laszlo Kardos for the statistical analysis and language editing.
Funding
Open access funding provided by Semmelweis University. The publication of this article was funded by the Department of Prosthodontics, Semmelweis University, Budapest, Hungary.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to the present study. RI, SJ and VB participated in digital impression taking as supervisor, performed the documentation. SJ was a major contributor in writing the manuscript. VB acquired and analyzed the data. BJ and HP revised the manuscript before submission. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not Applicable.
Consent for publication
Not Applicable.
Competing interests
The authors declare there is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schmalzl, J., Róth, I., Borbély, J. et al. The impact of software updates on accuracy of intraoral scanners. BMC Oral Health 23, 219 (2023). https://doi.org/10.1186/s12903-023-02926-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-02926-y