
Abstract
Background
This study aimed to compare the effect of Clinpro™ White varnish containing 5% sodium fluoride (NaF) and functionalized tricalcium phosphate, MI varnish containing 5% NaF and casein phosphopeptide-amorphous calcium phosphate (CPP-ACP), and 38% Silver diamine fluoride (SDF) in preventing demineralization of treated white spot lesions (WSLs) in enamel of primary teeth.
Methods
Forty-eight primary molars with artificial WSLs were allocated into four groups as follows: Group 1: Clinpro white varnish, Group 2: MI varnish, Group 3: SDF, and Group 4: control (no treatment). The three surface treatments were applied for 24 h and then enamel specimens were subjected to pH cycling. Thereafter, the mineral content of specimens was evaluated by Energy Dispersive X-ray Spectrometer and the lesion depth was assessed via Polarized Light Microscope. One-way ANOVA followed by Tukey’s post hoc test were used at p ≤ 0.05 to identify significant differences.
Results
Insignificant difference in mineral content was observed among treatment groups. Treatment groups exhibited significantly higher mineral content compared to control except for Fluoride (F). MI varnish showed the highest mean calcium (Ca) ion content (66.57 ± 0.63), and Ca/P (2.19 ± 0.11), followed by Clinpro white varnish, and SDF. MI varnish also displayed the highest phosphate (P) ion content (31.46 ± 0.56), followed by SDF (30.93 ± 1.02), and Clinpro white varnish (30.53 ± 2.19). Fluoride content was highest in SDF (0.93 ± 1.18), followed by MI (0.89 ± 0.34) and Clinpro (0.66 ± 0.68) varnishes. Significant difference in lesion depth was observed among all groups (p < 0.001). The lowest mean lesion depth (µm) was found in MI varnish (226.23 ± 44.25) which was significantly lower than Clinpro white varnish (285.43 ± 44.70), SDF (293.32 ± 46.82), and control (576.69 ± 42.66). Insignificant difference in lesion depth was found between SDF and Clinpro varnish.
Conclusions
In primary teeth, WSLs treated with MI varnish displayed better resistance to demineralization compared to WSLs treated with Clinpro white varnish and SDF.
Similar content being viewed by others

Background
White spot lesion (WSL) is considered the first sign of dental caries. It clinically appears as a chalky white opacity and is considered the earliest macroscopic evidence of enamel caries. WSLs are characterized by a porous subsurface enamel while the outermost enamel layer covering the lesion remains relatively intact and appears radiopaque. Control of WSLs includes prevention of demineralization and enhancement of remineralization to arrest lesion activity and improve esthetics [1].
Fluoride varnish is one important WSLs’ management strategy, especially in children, due to their safety and ease of application. Fluoride varnishes promote the growth of calcium fluoride on tooth surfaces which acts as an intraoral fluoride reservoir releasing calcium and fluoride ions when the oral pH drops [2]. To increase the effectiveness of fluoride varnishes, some manufacturers have added calcium (Ca) and inorganic phosphate (P) ions to enhance the precipitation of fluoro-hydroxyapatite by increasing its constituting ions bioavailability [3].
Clinpro white varnish (3 M Espe, USA) combines 5% NaF with a unique functionalized tricalcium phosphate (fTCP). In Clinpro white varnish, TCP is combined with fumaric acid producing free phosphate and fumaric acid-protected calcium oxide. The calcium protected with fumaric acid does not react with fluoride (F) till varnish application. When the varnish is applied on the teeth surfaces, it slowly dissolves releasing Ca, P and F ions for up to 24 h [4].
MI varnish (GC, Tockyo, Japan) is a one fluoride varnish product that contains 5% NaF and 2% RECALDENT™ [casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) nanocomplexes]. CPP-ACP is an amorphous form of calcium phosphate (ACP) stabilized by a casein phosphopeptide (CPP) derived from milk casein. The varnish sets when it contacts saliva and slowly releases F and CPP-ACP. This increases the bioavailability of F, Ca and P ions enhancing remineralization [5]. According to the manufacturer, the size of CPP-ACFP nanocomplexes are less than 2 nm enhancing penetration into biofilm, enamel, and dentinal tubules [6].
The use of silver diamine fluoride (SDF) has increased in recent years as a minimally invasive approach for caries management. Its high F content (44,800 ppm) enhances remineralization, while its silver content kills cariogenic bacteria and thus lesion arrest is promoted [7]. When applied on carious enamel lesions, SDF interacts with hydroxyapatite in the tooth structure to generate calcium fluoride and silver phosphate which improves the mineral density of enamel, increases the hardness of hydroxyapatite crystals, and reduces the depth of the carious lesion [7, 8]. Moreover, further mineral loss from demineralized tooth structures was found to decrease following SDF application, possibly due to incorporation of silver nanoparticles into treated hydroxyapatite [9]. Like fluoride varnish, SDF’s ease of use and effectiveness have made SDF application a popular treatment in pediatric dentistry.
Despite the availability of different remineralizing agents, there is inconclusive evidence about the superiority of a specific agent specifically in primary teeth. Moreover, studies reporting on the effectiveness of SDF in comparison to fluoride varnishes containing different sources of calcium phosphate are scarce. Only one in-vitro study investigated those products, however on bovine dentin [4].
Therefore, the aim of the present study was to compare the mineral content and lesion depth of artificial enamel caries in primary teeth treated with Clinpro white varnish, MI varnish and 38% SDF after being subjected to pH cycling. The null hypothesis was that there would be no difference in the remineralization potential among treatment groups.
Methods
Sample size estimation
Based on the null hypothesis and by adopting an alpha level of 5%, a beta level of 20% i.e. power = 80% as well as an effect size of 0.60 based on the results of a previous study [10]; the predicted sample size (n) was 48.
Enamel specimens’ preparation
Forty-eight sound primary molars, that were freshly extracted for orthodontic reasons or naturally exfoliating, were included. Teeth were cleaned, polished with a non-fluoride containing polishing paste and examined under a stereomicroscope to exclude teeth with developmental defects, cracks, or enamel demineralization in the buccal surface. Teeth were stored in distilled water until use [11, 12]. A 4 × 4 mm2 square adhesive tape was placed on the center of the buccal surface of each tooth. The entire tooth was then coated with an acid resistant nail varnish (Amanda A.R.E). A 4 × 4 mm2 enamel window was created by removing the adhesive paper [12].
Subsurface enamel lesions were created by submerging each tooth in 10 ml of a demineralizing solution (pH 4.4) for 4 days inside a light resistant container [11] until a distinct visual change in enamel in both dry and wet conditions was evident (ICDAS score 2) [13].
Treatment protocols and pH cycling
After induction of WSLs, each tooth was rinsed with 10 ml deionized water and dried with a stream of compressed air. Teeth were randomly divided into four groups by a study independent operator as follows:
-
Group 1 In which a thin coating of Clinpro white varnish was applied to exposed enamel using a micro-brush.
-
Group 2 In which a thin coating of MI varnish was applied to exposed enamel using a micro-brush.
In groups 1 and 2, teeth were allowed to air dry for 5 min before being placed in artificial saliva for 24 h [12]. Varnishes were carefully removed from all specimens using a cotton swab dipped in acetone to avoid harming the enamel surface. Teeth were then rinsed with deionized water for 1 min before being subjected to pH cycling [11].
-
Group 3 In which 38% SDF was applied with a micro-brush to exposed enamel for two minutes. Teeth were washed with 10 ml deionized water for 30 s, dried with compressed air and stored in artificial saliva for 24 h. Thereafter, teeth were rinsed with deionized water for 1 min before pH cycling [12].
-
Group 4 (Control group) After creating WSLs, teeth were left untreated and were stored in artificial saliva for 24 h. Teeth were rinsed with deionized water for 1 min before pH cycling.
pH cycling
All specimens were subjected to 9 days of pH cycling (8 days de/remineralization + 1-day remineralization). Demineralization/Remineralization cycles consisted of teeth immersion in 60 ml of demineralizing solution for 4 h followed by immersion in 60 ml of remineralizing solution for 20 h. This cycle was repeated for 8 days consecutively, and new solutions were used daily. After each cycle, specimens were washed with deionized water before progressing to the next cycle. On day 9, the specimens were immersed in the remineralization solution for 24 h [11, 14]. Details of materials used in the study are listed in Table 1.
Mineral content measurement
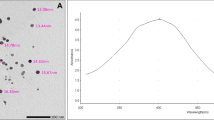
After pH cycling, teeth were washed with deionized water and prepared for quantitative elemental analysis using energy dispersive X-ray spectrometer (EDX) (Inspect S Manufacturer, FEI Company, Netherlands) with an accelerating voltage of 30 kV, magnification up to 106 and a 1 nm gun’s resolution. Specimens were fixed with a double adhesive tape to a sample holder so that the enamel window was facing upward. Three different readings were obtained from the center of each enamel window and an average was calculated for each specimen. The weight percent of calcium (Ca), fluoride (F) and phosphorus (P) in enamel surface was assessed as well as the Ca/P ratio [12, 15].
Lesion depth measurement
After EDX assessment, teeth were qualitatively assessed for lesion depth with a polarized light microscope (PLM) (PRIOR scientific, PriorLux POLTM) at a magnification of × 100. Using a slow-speed diamond saw and ample water spray, teeth were longitudinally sliced into mesial and distal halves from the center of the 4 × 4 mm2 window. For each tooth, one tooth half was selected using a toss of a coin. Tooth halves were then reduced to a thickness of 100–150 µm using wet 150 grit silicon carbide papers [11, 14]. Image J analysis software (Java-based image processing program) was used to measure the depth of demineralized zones. In each specimen, the deepest area of enamel demineralization was selected, and the lesion depth was measured in (µm) via drawing 3 perpendicular lines to the outer enamel surface at three distinct places (at the center of the deepest area of the lesion and at the peripheries of this area). The mean was determined and recorded as the specimen's lesion depth [11, 14].
Statistical analysis
Data were analyzed using one-way ANOVA followed by Tukey’s post hoc test. The significance level was set at p ≤ 0.05 within all tests. Statistical analysis was performed with R statistical analysis software version 4.1.2 for Windows.Footnote 1
Results
I-EDX analysis
Mean and standard deviation (SD) values of weight percentage (%) for different elements are presented in Table 2. Mineral content analysis showed the following:
-
Ca weight % The highest value was found in MI varnish (66.57 ± 0.63), followed by Clinpro white varnish (66.23 ± 0.51), then SDF (64.51 ± 0.52), while the lowest value was found in the control group (34.68 ± 3.29). Insignificant difference was found among the treatment groups, yet the control group differed significantly with all other groups (p < 0.001).
-
P weight % The highest value was found in MI varnish (31.46 ± 0.56), followed by SDF (30.93 ± 1.02), then Clinpro white varnish (30.53 ± 2.19), while the lowest value was found in the control group (18.33 ± 1.90). Post hoc pairwise comparisons showed the control group to have a significantly lower value than other groups (p < 0.001), while insignificant difference was found among the treatment groups.
-
Ca/P The highest value was found in MI varnish (2.19 ± 0.18), followed by Clinpro white varnish (2.11 ± 0.05), then SDF (2.09 ± 0.06), while the lowest value was found in the control group (1.90 ± 0.18). Post hoc pairwise comparisons showed the control group to have a significantly lower value than other groups (p = 0.003), while insignificant difference was found among the treatment groups.
-
F weight % The highest value was found in SDF (0.93 ± 1.18), followed by MI varnish (0.89 ± 0.34), then Clinpro white varnish (0.66 ± 0.68), while the lowest value was found in the control group (0.54 ± 0.52). Non-significant difference was found among all groups.
Table 2 EDX analysis
II- lesion depth
Mean and SD values of lesion depth (µm) for different groups are presented in Table 3. Representative PLM images for all groups are presented in Figs. 1, 2, 3 and 4. A significant difference was evident among groups (p < 0.001). The highest value for lesion depth was found in the control group (576.69 ± 42.66), followed by SDF (293.32 ± 46.82), then Clinpro white varnish (285.43 ± 44.70), while the lowest value was found in MI varnish (226.23 ± 44.25). SDF and Clinpro white varnish had significantly higher lesion depth values than MI varnish (p < 0.001).

PLM image of a representative lesion from group 1 (clinpro™ white) showing lesion depth at 3 different areas

PLM image of a representative lesion from group 2 (MI varnish) showing lesion depth at 3 different areas

PLM image of a representative lesion from group 3 (SDF) showing lesion depth at 3 different areas

PLM image of a representative lesion from group 4 (control) showing lesion depth at 3 different areas
Discussion
In early enamel lesions, both fluoride varnish and SDF have been suggested as treatment strategies, especially in young children, due to their ease of application and safety [3, 12, 16, 17]. The effect of SDF compared to NaF varnish on enamel remineralization was previously investigated [12, 18]. Yet, up to our knowledge, our study is the first to compare the effect of SDF and fluoride varnishes containing calcium-phosphate on WSLs in primary teeth.
Our results demonstrated that the three investigated topical treatments were able to remineralize demineralized enamel of primary teeth. MI varnish followed by Clinpro white varnish were better than SDF in terms of Ca and P content, Ca/P ratio, as well as lesion depth. Although EDX analysis revealed insignificant differences in Ca, P, and F ions content as well as Ca/P among all treatment groups, yet Ca content and Ca/P were higher in MI varnish followed by Clinpro white varnish. On the other hand, the control group showed significantly lower values for all variables except for F ion content. This indicates that the three topical agents exerted considerable remineralization of the WSLs, thus increasing their resistance to further demineralization when exposed to a subsequent acidic challenge. Thus, the null hypothesis is not rejected. The F content in the 3 agents could have contributed to the remineralization process by enhancing precipitation of minerals into the decalcified lesions [19]. Although F content in SDF is much higher than MI and Clinpro white varnishes, yet the adhesiveness of varnishes that allows prolonged contact with enamel as well as the availability and sustained release of F and other minerals may have contributed to the higher Ca and P content as well as Ca/P in MI varnish and Clinpro white groups. In agreement with the present findings, the effectiveness of MI varnish compared to other fluoride and calcium phosphate containing varnishes was reported in many studies [11, 20,21,22,23,24]. One study disclosed that MI varnish had a significantly higher capacity to remineralize decalcified enamel in terms of microhardness and mineral content compared to Clinpro white varnish [23]. Shen, et al. [24] reported that sound primary teeth enamel previously treated with MI varnish was more resistant to acid demineralization than specimens treated with Clinpro white varnish or a 5% NaF varnish where the % of inhibition of demineralization was significantly highest in MI varnish while lesion depth was significantly lowest compared to other groups. Shen, et al. [24] also reported that MI varnish exhibited the highest Ca, P, and F ions release compared to Clinpro white varnish as well as other calcium phosphate and fluoride containing varnishes.
Abufarwa, et al. [14] disclosed that MI varnish application could prevent enamel demineralization for up to 4 weeks. Cochrane et al. [25], also found that MI varnish significantly released higher F, Ca and P compared to Clinpro white varnish. The authors suggested that the low ion release of Clinpro white may be due to the low concentration of added fTCP or the low solubility of TCP.
CPP in MI varnish may have also contributed to a better remineralization by stabilizing CPP-ACFP nanoclusters preventing them from growing to the threshold size for phase transitions, thus keeping Ca and P ions freely accessible to diffuse into mineral-deficient lesions [26, 27]. Furthermore, casein contains amino acids that may have acted as acid buffers, thus provided treated specimens a better resistance to demineralization [21]. Another positive characteristic of MI varnish is that the CPP-ACFP nanocomplexes are electroneutral ion clusters thus they can rapidly diffuse out of the varnish and into subsurface lesions through intra-prismatic spaces [28].
Opposite to our findings, one study reported that a 5% NaF containing varnish and Clinpro white varnish achieved significantly better remineralization of demineralized enamel compared to MI varnish. However, in this study, varnishes were applied for only 6 h before treated specimens were subjected to pH cycling [29].
In the present study, Clinpro white varnish exhibited more Ca and Ca/P ratio compared to SDF which may be related to the TCP content of Clinpro white as well as its manufacturing process where fTCP is produced by functionalizing TCP with silica which promotes linking with hard tissue defects in acidic conditions [29, 30]. Other studies also confirmed that addition of TCP to fluoridated products achieved better remineralization than products containing fluoride only [11, 24, 31].
Nevertheless, a systematic review concluded that the potential of fluoride varnishes to arrest dental caries is not satisfactory, and that topical products with higher fluoride concentrations may be more effective [32]. The potential of SDF to remineralize and arrest enamel and dentin caries is well documented where a Ca and P rich layer was found on the surface of caries arrested lesions [9, 16]. Although most of the evidence pertaining to SDF comes from studies concerned with arresting dentin caries, its effectiveness in remineralizing initial enamel lesions was also reported [17]. Eventually, a systematic review and meta-analysis indicated that SDF application to decayed primary teeth can effectively prevent dental caries in the entire dentition compared to fluoride varnish [33].
Our findings showed SDF-treated specimens to have the highest F content. This finding might be attributable to the flowability of the SDF solution which makes complete contact with the enamel surface and thus delivers a high amount of F to demineralized enamel in a short period of time. It could also be due to the SDF’s high F content which is nearly double that of Clinpro white and MI varnishes [12]. It has been demonstrated that SDF can penetrate decalcified enamel, thereby, it acts as a fluoride reservoir enhancing remineralization and preventing further demineralization [34].
The cariostatic effect of SDF is not yet fully understood. It is suggested to be a result of antibacterial and remineralizing effects. Given that no bacterial biofilm was used in the present study, the noted SDF effect is therefore related to its remineralizing effect. It is suggested that an insoluble layer is formed after SDF application which consists of calcium fluoride, silver phosphate, silver chloride, and fluorapatite. This layer protects against further demineralization and prevents lesion progression. Yet this layer can also hinder minerals deposition inside the body of the lesion [12, 17]. This may explain the higher lesion depth of SDF group in the present study compared to MI and Clinpro white varnishes.
Opposite to our results, Yu et al. [12] demonstrated that lesion depth was lower in SDF treated subsurface enamel lesions compared to a 5% NaF varnish. However, in the latter study, fluoride varnish was applied for only 60 min. Additionally, the bioavailability of Ca and P in varnishes used in the current study may account for this inconsistency. Notably, Yu et al. [12] also pointed out that insoluble silver chloride was formed on the lesion surface, and this may be responsible for the increased hardness of WSLs. The authors also reported that silver nanoparticles were incorporated into the hydroxyapatite crystal in SDF-treated teeth which in turn can suppress bacterial adhesion thus preventing lesion progression [12].
Thus, although results of our study indicated that SDF showed lower Ca and Ca/P as well as deeper lesions than the tested varnishes, its clinical application to WSLs may increase resistance to bacterial induced demineralization more than the investigated varnishes. Thus, SDF may be of benefit in non-compliant patients. This also highlights the need to investigate SDF and fluoride varnishes in the presence of bacteria to mimic the oral environment.
Previously, Romão, et al. [17] suggested that SDF can be used for communities with limited financial resources, high caries risk individuals or those with poor compliance because SDF can immediately release all its fluoride content thus achieving more rapid arrest compared to fluoride varnishes.
A limitation of the present study is that in-vitro remineralization may be quite different when compared to the dynamic complex biological systems that occur in the oral cavity. Additionally, the antibacterial effect of the three tested agents was not taken into consideration where the clinical remineralization of carious lesions may be enhanced through availability of free mineral ions as well as the antimicrobial action of the used agents. Therefore, due to the evident limitations of in-vitro investigations, caution must be taken when making direct interpretations to clinical circumstances. Another limitation was that lesion depth of the treatment groups was not measured directly after demineralization and later compared to the post-treatment and pH cycling scores. Instead, demineralization was confirmed visually using the ICDAS-II relying on the significantly strong positive correlation that ICDAS has with histological lesion depth, where score 2 indicates a demineralized enamel that extends beyond half the enamel thickness [35]. Thereafter, post-treatment and pH cycling scores were compared to a control group that received no treatment as in some previous studies [11, 14, 17].
Conclusion
Within the limitation of the present study, the investigated remineralizing agents were all found to have a positive impact on prevention of enamel demineralization of treated WSLs in primary teeth. Fluoride varnish containing CPP-ACP (MI varnish) was the most effective in enhancing acid resistance. Yet, clinical trials are still required to verify the data obtained from this in-vitro investigation.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the first author upon request.
Notes
R Core Team (2022). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.
References
Tufekci E, Dixon JS, Gunsolley JC, Lindauer SJ. Prevalence of white spot lesions during orthodontic treatment with fixed appliances. Angle Orthod. 2011;81(2):206–10. https://doi.org/10.2319/051710-262.1.
Xin W, Leung KC, Lo EC, Mok MY, Leung MH. A randomized, double-blind, placebo-controlled clinical trial of fluoride varnish in preventing dental caries of Sjögren's syndrome patients. BMC Oral Health. 2016;16(1):102. https://doi.org/10.1186/s12903-016-0296-7. Erratum in: BMC Oral Health. 2017; 17 (1):63.
Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochr Database Syst Rev. 2013;7:CD002279. https://doi.org/10.1002/14651858.CD002279.
Wierichs RJ, Stausberg S, Lausch J, Meyer-Lueckel H, Esteves-Oliveira M. Caries-preventive effect of NaF, NaF plus TCP, NaF plus CPP-ACP, and SDF varnishes on sound dentin and artificial dentin caries in vitro. Caries Res. 2018;52(3):199–211. https://doi.org/10.1159/000484483.
Cross KJ, Huq NL, Reynolds EC. Casein phosphopeptide-amorphous calcium phosphate nanocomplexes: a structural model. Biochemistry. 2016;55(31):4316–25. https://doi.org/10.1021/acs.biochem.6b00522.
https://www.gcaustralasia.com/Upload/product/pdf/95/GC3347-MIV-Brochure-update-FA-(secure).pdf. Accessed December 20, 2022.
Chibinski AC, Wambier LM, Feltrin J, Loguercio AD, Wambier DS, Reis A. Silver diamine fluoride has efficacy in controlling caries progression in primary teeth: a systematic review and meta-analysis. Caries Res. 2017;51(5):527–41. https://doi.org/10.1159/000478668.
Mei ML, Ito L, Cao Y, Lo EC, Li QL, Chu CH. An ex vivo study of arrested primary teeth caries with silver diamine fluoride therapy. J Dent. 2014;42(4):395–402. https://doi.org/10.1016/j.jdent.2013.12.007.
Zhao IS, Gao SS, Hiraishi N, Burrow MF, Duangthip D, Mei ML, Lo EC, Chu CH. Mechanisms of silver diamine fluoride on arresting caries: a literature review. Int Dent J. 2018;68(2):67–76. https://doi.org/10.1111/idj.12320.
Nehal RS, Magda ME, Niveen SB, Samia S. Remineralization effect of fluoride varnish containing casein phosphopeptide amorphous calcium phosphate on caries-like lesions in primary teeth (in vitro study). Alex Dent J. 2019;44(1):13–6. https://doi.org/10.21608/ADJALEXU.2019.57568.
Tuloglu N, Bayrak S, Tunc ES, Ozer F. Effect of fluoride varnish with added casein phosphopeptide-amorphous calcium phosphate on the acid resistance of the primary enamel. BMC Oral Health. 2016;16(1):103. https://doi.org/10.1186/s12903-016-0299-4.
Yu OY, Mei ML, Zhao IS, Li QL, Lo EC, Chu CH. Remineralisation of enamel with silver diamine fluoride and sodium fluoride. Dent Mater. 2018;34(12):e344–52. https://doi.org/10.1016/j.dental.2018.10.007.
Abrams SH, Sivagurunathan KS, Silvertown JD, Wong B, Hellen A, Mandelis A, Hellen WMP, Elman GI, Mathew SM, Mensinkai PK, Amaechi BT. Correlation with caries lesion depth of the canary system, DIAGNOdent and ICDAS II. Open Dent J. 2017;29(11):679–89. https://doi.org/10.2174/1874210601711010679.
Abufarwa M, Noureldin A, Campbell PM, Buschang PH. The longevity of casein phosphopeptide-amorphous calcium phosphate fluoride varnish’s preventative effects: assessment of white spot lesion formation. Angle Orthod. 2019;89(1):10–5. https://doi.org/10.2319/021718-127.1.
Hegde MN, Moany A. Remineralization of enamel subsurface lesions with casein phosphopeptide-amorphous calcium phosphate: a quantitative energy dispersive X-ray analysis using scanning electron microscopy: an in vitro study. J Conserv Dent. 2012;15(1):61–7. https://doi.org/10.4103/0972-0707.92609.
Punhagui MF, Jussiani EI, Andrello AC, Favaro JC, Guiraldo RD, Lopes MB, Berger SB. Effect of application time and concentration of silver diamine fluoride on the enamel remineralization. J Clin Exp Dent. 2021;13(7):e653–8. https://doi.org/10.4317/jced.58318.
Romão DA, Fernández CE, de Melo SL. Commercial silver diamine fluoride (SDF) products on caries lesion progression in primary enamel: an in vitro study. Oral Health Prev Dent. 2020;18(1):1025–9. https://doi.org/10.3290/j.ohpd.b871057.
Phonghanyudh A, Duangthip D, Mabangkhru S, Jirarattanasopha V. Is silver diamine fluoride effective in arresting enamel caries? A randomized clinical trial. Int J Environ Res Public Health. 2022;19(15):8992. https://doi.org/10.3390/ijerph19158992.
Hicks J, Garcia-Godoy F, Flaitz C. Biological factors in dental caries: role of remineralization and fluoride in the dynamic process of demineralization and remineralization (part 3). J Clin Pediatr Dent. 2004;28(3):203–14. https://doi.org/10.17796/jcpd.28.3.w0610427l746j34n.
Varma V, Hegde KS, Bhat SS, Sargod SS, Rao HA. Comparative evaluation of remineralization potential of two varnishes containing CPP-ACP and tricalcium phosphate: an in vitro study. Int J Clin Pediatr Dent. 2019;12(3):233–6. https://doi.org/10.5005/jp-journals-10005-1629.
Rani KB, Ramanna PK, Mailankote S, Joy AK, Thomas AA, Baby M. Evaluation of anticaries efficacy of various fluoride varnishes on artificial enamel lesion: an in vitro study. J Contemp Dent Pract. 2021;22(7):774–7.
Savas S, Kavrìk F, Kucukyìlmaz E. Evaluation of the remineralization capacity of CPP-ACP containing fluoride varnish by different quantitative methods. J Appl Oral Sci. 2016;24(3):198–203. https://doi.org/10.1590/1678-775720150583.
Salinovic I, Schauperl Z, Marcius M, Miletic I. The Effects of three remineralizing agents on the microhardness and chemical composition of demineralized enamel. Materials. 2021;14(20):6051. https://doi.org/10.3390/ma14206051.
Shen P, Bagheri R, Walker GD, Yuan Y, Stanton DP, Reynolds C, Reynolds EC. Effect of calcium phosphate addition to fluoride containing dental varnishes on enamel demineralization. Aust Dent J. 2016;61(3):357–65. https://doi.org/10.1111/adj.12385.
Cochrane NJ, Shen P, Yuan Y, Reynolds EC. Ion release from calcium and fluoride containing dental varnishes. Aust Dent J. 2014;59(1):100–5. https://doi.org/10.1111/adj.12144.
Soares R, De-Ataide IN, Fernandes M, Lambor R. Assessment of enamel remineralisation after treatment with four different remineralising agents: a scanning electron microscopy (SEM) study. J Clin Diagn Res. 2017;11(4):ZC136–41. https://doi.org/10.7860/JCDR/2017/23594.9758.
Jayarajan J, Janardhanam P, Jayakumar P, Deepika A. Efficacy of CPP-ACP and CPP-ACPF on enamel remineralization: an in vitro study using scanning electron microscope and DIAGNO dent. Indian J Dent Res. 2011;22(1):77–82. https://doi.org/10.4103/0970-9290.80001.
Cochrane NJ, Cai F, Huq NL, Burrow MF, Reynolds EC. New approaches to enhanced remineralization of tooth enamel. J Dent Res. 2010;89(11):1187–97. https://doi.org/10.1177/0022034510376046.
Mohd Said SN, Ekambaram M, Yiu CK. Effect of different fluoride varnishes on remineralization of artificial enamel carious lesions. Int J Paediatr Dent. 2017;27(3):163–73. https://doi.org/10.1111/ipd.12243.
Elkassas D, Arafa A. Remineralizing efficacy of different calcium-phosphate and fluoride based delivery vehicles on artificial caries like enamel lesions. J Dent. 2014;42(4):466–74. https://doi.org/10.1016/j.jdent.2013.12.017.
Karlinsey RL, Mackey AC, Walker TJ, Frederick KE, Blanken DD, Flaig SM, Walker ER. In vitro remineralization of human and bovine white-spot enamel lesions by NaF dentifrices: a pilot study. J Dent Oral Hyg. 2011;3(2):22–9.
Gao SS, Zhang S, Mei ML, Lo EC, Chu CH. Caries remineralisation and arresting effect in children by professionally applied fluoride treatment - a systematic review. BMC Oral Health. 2016;1(16):12. https://doi.org/10.1186/s12903-016-0171-6.
Oliveira BH, Rajendra A, Veitz-Keenan A, Niederman R. The effect of silver diamine fluoride in preventing caries in the primary dentition: a systematic review and meta-analysis. Caries Res. 2019;53(1):24–32. https://doi.org/10.1159/000488686.
Idoraşi L, Crăciunescu EL, Stan AT, Sinescu C, Chiş AC, Onchiş-Moacă D, Romînu M, Negruţiu ML. Morphological aspects in remineralizing potential of Silver Diamine Fluoride. Rom J Morphol Embryol. 2021;62(2):537–43. https://doi.org/10.47162/RJME.62.2.20.
Jablonski-Momeni A, Ricketts DN, Rolfsen S, Stoll R, Heinzel-Gutenbrunner M, Stachniss V, Pieper K. Performance of laser fluorescence at tooth surface and histological section. Lasers Med Sci. 2011;26(2):171–8. https://doi.org/10.1007/s10103-010-0768-y.
Acknowledgements
Not applicable.
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
All authors participated in study conception and design. Teeth collection, preparation, and treatment were performed by AM. Data analysis was done by AM, GA, and MW. AM wrote the first draft of the manuscript. GA and MW revised and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The research was reviewed by the research ethics committee of the Faculty of Dentistry, Ain Shams University with reference number (FDASU-RecEM121910). All methods were performed according to the ethical principles of Declaration of Helsinki. Parents gave their informed consent to use their children’s teeth for research purpose orally which was previously approved by the research ethics committee.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mashhour, A., Allam, G. & Wassel, M. Comparative evaluation of prevention of demineralization of artificial enamel caries treated with two fluoride varnishes and 38% SDF in primary teeth: an in vitro study. BMC Oral Health 23, 110 (2023). https://doi.org/10.1186/s12903-023-02799-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-02799-1