
Abstract
Background
Globally, dental caries appears a major public health problem and a widespread non -communicable disease. It is more prevalent among children school-age children (6–12 years), However, there are few studies that correlate dental caries with nutritional status. Thus, this study aims to determine the relation of dental caries with nutritional status among school-age children at resource limited setting of southern Ethiopia.
Methodology
A community-based cross sectional study was employed on randomly selected 761 school-age children of Areka town. Data were collected by face-to-face interviewer-administered questionnaire and clinical assessment of dental caries. After that, the collected data were entered into Epi data 3.2.1 and exported to SPSS 20 for further analysis. On the other hand, bivariate and multiple logistic regression analyses were used to identify the association of dependent and independent variables. p Value < 0.05 was considered to declare a result as statistically significant.
Results
Prevalence of dental caries among school-age children was 15.6% (95% CI 13.0–18.5). In technical senses, 4.3% (95% CI 2.9–5.8%) of children were underweight and 14.2% (95% CI 11.7–16.6%) were overweight. However, it has been unfolded that the relationship between dental caries and nutritional status was not statistically significant with a p value (p = 0.32). Factors associated with dental caries were educational status of a mother AOR 3.14, (95% CI 1.03–9.56), not cleaning teeth AOR 7.70, (95% CI 4.00–14.85), sugared coffee drinking AOR 3.22, (95% CI 1.68–6.18.0), sweet food consumption AOR 4.19, (95% CI 1.76–9.96) and non-consuming milk AOR 5.66 ( 95% CI 1.49–21.49).
Conclusion and recommendation
Dental caries at south Ethiopia were low compared to WHO’s reports on oral health on school-age children. Tooth cleaning habit, parental education, sweet food consumption and milk consumption are associated factors. Therefore, behavioral intervention on dental hygiene and dietary practices are mandatory for school-age children.
Similar content being viewed by others

Introduction
Oral health, as defined by the World Health Organization (WHO), is a state of being free of mouth and facial pain, oral infection and sores, periodontal (gum) disease, tooth decay, tooth loss, and other diseases and disorders that limit an individual's capacity for biting/chewing, smiling, speaking, and psychosocial wellbeing [1]. According to the 2017 Global Burden of Disease study, dental caries of the primary teeth affect more than 530 million children worldwide [2]. Consequently, dental caries is a major public health problem globally, and is the most widespread non-communicable disease (NCD) among school-age children. The study of the Global Burden of Disease during the year 2016 has ranked decay of permanent teeth in the first place among half of the world’s population (3.58 billion people), and deciduous teeth was ranked 12th position (560 million children) [3].
Most of the dental caries were untreated with considerable impacts on general health, quality of life, productivity, development, and educational performance [4]. By far, it has been proven that having good oral health enables individuals to communicate effectively, to enjoy food, to speak well, to enjoy a higher quality of life, and to have both higher self-esteem and social confidence. Tooth infection causes pain and restlessness to children resulting in decreased growth hormone and increased metabolic rate so malnutrition in children can occur [5]. More specifically, School-age children (6–12 yrs) are a top priority in oral health programs because of the high prevalence of dental caries and the development of permanent teeth in this age group [6].
The burden of dental caries in children is high. Dental caries will progress into tooth pulp and a dental abscess will result, if untreated, to loss of teeth. In advanced cases, it may interfere with dietary habits as a result affect nutritional status as well as affect sleep, work activities, and school attendance [7, 8].
Dental illnesses, particularly dental caries, cost $298 billion of the global economy in direct treatment costs, accounting for 4.6 percent of global health expenditures [9, 10]. Besides, It spends 5–10% of healthcare budgets in developed countries, and is one of the leading causes of child hospitalization in various high-income countries. It comes as no surpise that it is neglected in developing countries for, it is one of the most expensive diseases to treat [11].
Oral tissues require nourishment for development, growth, and maintenance, and oral problems can influence food choices and, ultimately, nutritional status. Prior to tooth eruption, nutritional deficiencies can affect enamel maturation and composition as well as tooth morphology and size [12,13,14]. Under-nutrition in children not only delays teeth development but also results a high number of carious primary teeth and exacerbates the carcinogenicity of dietary sugars. All in all, it is far beyond clear that tooth decay and early loss of teeth lead to under-nutrition [15].
The WHO set a universal goal for developing countries which should have been achieved by the year 2020. It stated that about 50% of 6 year-old children should be free of decayed teeth and the average DMFT (Decayed Missed Filled teeth) score should not be more than 3 at the age of 12 years [1]. Although dental caries and nutritional status affect one another among school-age children. There are few studies the relation to dental caries with nutritional status among school-age children. Therefore, this study was carried out to assess the prevalence of dental caries in relation to nutritional status among school-age children.
Methods and materials
Study setting, design and period
The sections following were conducted according to standard guidelines and procedures of observational methods. A community-based cross- sectional study design was conducted in February 2020 in Areka Town, Woliata zone, Southern Nations Nationality People’s Region (SNNPR), Ethiopia. Areka town is located in the northern part of Wolaita Zone, and is found 299 km South of Addis Ababa, 178 km from the city of Hawassa, and 29 km from Sodo (zonal capital). The town is divided into 4 kebeles with 29 urban and 18 rural villages. According to Areka town’s health office 62,254 total populations and 12,805 households and 20,083 school-age children were calculated by an indicator given from Federal ministry of Health (FMOH) for each region (32.26%) for Southern Nations Nationality Peoples’ Region (SNNPR) in 2010 [16].
Source population and study population
The source population for this study were all school-age children (6–12 years old) living in Areka town from February–February, 2020.
Inclusion and exclusion criteria
All school-age children permanently residing in the selected household for at least 6 months and their caregivers were included. On the other hand, severe medically ill, long-term medication, and undergoing orthodontic treatment school-age children were excluded.
Determination of sample size
Sample size was calculated by single population proportion formula with an assumption of the prevalence of dental caries of 36.3% [17] at Gonder town. Other assumptions were 95% Confidence interval, 5% margin of error, 2 design effect, and 10% non-response rate. The total sample was 783 school-age children.
where Z1-α/2 = 95% Confidence interval (CI), P = proportion to be used (36.3%), d = margin of error (5%).
Sampling procedure
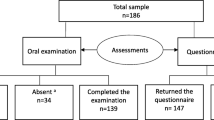
A Systematic random sampling was employed on each kebeles of Areka town. In that regard, the sample size was proportionally allocated among all kebeles depending on their number of households. The sampling frame of households with school-age children was prepared from health posts family folder. Finally, a systematic random sampling method with k is 6th interval was applied to select the households with school-age children. The first households were selected from each kebeles randomly. If the selected the households had more than one eligible school-age child in the house, lottery method was used to select one eligible. In some scenarios, when the child was not present at home, 3 visits were made and after 3 visits, they were recorded as ‘non-response’ (Fig. 1).

Sampling Schematic diagram showing sampling procedure for Areka town, 2020
Data collection tool and procedures
The data used for this study were collected using interviewer administered questionnaire adopted from a review of literatures [17,18,19,20]. School-age children with caregivers were interviewed from the selected household. Ten BSc. graduate nurses were made to be data collectors, and two individuals with a master’s degree were made to be supervisors. Both the data collectors and supervisors were able to speak the local language. Apart from that, training was given for two days on how to collect data and supervise the data collectors. Besides, the supervisors were given additional training on oral examination of children. Besides the principal investigator was supervising during data collection.
Dental caries were assessed by clinical assessment of the oral. It was done by supervisors and the principal investigator. Dental caries was measured by the sum of Decayed, Missing and Filled Teeth (DMFT). DMFT is a tool used for measuring the prevalence of dental caries. The “D” component means Decayed tooth, “M” component is the Missing tooth, “F” component is the Filled tooth and “T” is the Tooth involved. A DMFT score above 0 indicates the presence of caries, whereas a null score indicates the absence of caries. The severity of dental caries were classified based on WHO using DMFT values, values between 0.0–1.1 very low; 1.2–2.6 low; 2.7–4.4 moderate; 4.5–6.5 high; values exceeding 6.6 will be very high [3].
The status of nutrition among children was assessed by measuring height and weight. Height was recorded with the help of a height board. Weight was measured using a Seca digital weighing scale after calibration is done. In that regard, height and weight were measured three times and took the average for further analysis. BMI score was compared to the WHO’sreference 2007 chart for age 5–18 years and assessed by using age and gender specific criteria. The following were assessed using BAZ Underweight as BAZ < − 2SD, normal ≥ − 2SD to ≤ + 1SD and overweight/ obesity as BAZ > + 1SD [21].
Food consumption patterns were assessed using an unquantified interviewer-administered food frequency questionnaire. It was investigated by seven-day food frequency questionnaire (FFQ) consisting of 12 listed food items which are commonly used by the study population and are rich with micronutrients of interest (Calcium, Vitamin C & D), were read to the respondents who were to state the number of times they had consumed the foods in the past 7 days of the data collection period.
Study variables
Dependent variable
Dental caries: It was measured based on DMFT score above 0 indicates active caries and 0 indicates caries free.
Independent variables
-
Nutritional status: underweight, normal, overweight and obesity.
-
Socio economic and demographic variables: age, sex, residence, grade level, parent’s education, monthly income of the family and exposure to mainstream media.
-
Dietary habits of children: sweet consumption, meal frequency, fruit consumption and diary product consumption.
-
Oral health related behaviors: teeth brushing, mouth rinsing, dental plaque, toothache, dental clinic visit and flossing habit.
Operational definitions
-
DMFT: Decayed (D), presence of a lesion in a pit or fissure or on smooth tooth surface had a detectable softened floor, destabilized enamel or softened wall. Missing (M), a person gives a history of pain and/or presence of cavity prior to extraction because of caries,. Filled (F) presence of one or more restorations.
-
Dental caries: A DMFT score above 0 indicates the presence of caries, whereas a null score indicates the absence of caries.
-
Regular tooth brushing- reported of brushing tooth with toothbrush and fluoride toothpaste twice a day or after every meal for about two minutes.
-
Flossing habit- is removing of food and dental plaque from space between two teeth areas a toothbrush is unable to reach.
Data quality assurance
The Questionnaire was first prepared by English language. Then, it was translated to local language Wolayitatoo by local and English language experts. After that, it was translated back to English by different language experts to maintain its consistency. Pre-test was conducted by taking 5% of the sample which is 39 school-age children in Bombe town outside the study area after training given. This verified the clarity of instruments and helped to familiarize data collectors to the instrument and necessary correction was made accordingly. The supervisors and the principal investigator made daily checkup on the data collection process to ensure the completeness and consistency. Any error found during the process was corrected immediately.
Data management and analysis procedures
Data were entered into Epi data version 3.2.1 after ensuring completeness of each questionnaire. After that, it was exported to SPSS version 20 for further analyses. Descriptive statistics was conducted to determine the frequencies and percentages of different variables. Bivariate and multiple logistic regression analyses were done to identify variables that were associated with the dependent variables. Independent variables having P value less than 0.25 on bivariate analysis were nominated for multiple logistic regression analysis for further confounding effect control [22]. Hosmer and Lemeshow goodness of fit test was used to assess the fitness of the model during multiple logistic regression analyses. Normality was checked by Kolmogorov smirnov test of normality.
Crude and adjusted odds ratios together with their corresponding 95% confidence intervals were computed and interpreted accordingly. P value < 0.05 was considered to declare a result as statistically significant. A correlational statistical test was used to determine the relation between nutritional status and caries occurrence. BMI- for-age (BAZ) was used to assess each child's nutritional status. BMI- for-age (BAZ) score parameter was calculated using WHO anthroplus 2007 version 3.2.2 software.
Result
Socio demographic characteristics of respondents
A total of 761 participants were included in the analysis, resulting in a response rate of 97.2%. Out of these, three hundred thirty-one (43.5%) school-aged children were between the ages of 6 and 8 years, with a median age of 9.0 years and an interquartile range (IQR) of 4, and 54 percent of them were girls. Most of the respondents, 723 (95%) were urban residents. Five hundred twelve (67.3%) of them were attending class at governmental school, and they were 0–4 class students. On the other side, two hundred forty-four (32.1%) mothers or caregivers had no formal education, but 308(40.5%) of fathers were college graduates. Above half of (52.7%) the mothers’ or caregivers’ occupation was housewife, and 296 (38.9%) fathers were government employees. It has been seen that the majority of the households 505 (66.4%) had exposure to the mainstream meadia (TV) (Table 1).
Oral health-related behaviors of children
It has been found that the majority of the children, (72.5%), never clean their teeth; of those who do, 416 (75.3%) clean their teeth once or less than once a day, while just 136 (24.7%) clean them on a regular basis. Two hundred and forty-nine children (45.1%) used mouthwash/rinse with water, whereas 209 people (37.9%) used paste-based toothbrushes. Almost half 288 (52.2%) clean their teeth in the morning before breakfast. On the other hand, two hundred seventeen (39.3%) children spent only one minute on teeth cleaning. Almost all 372 (96.1%) of the children who had a flossing habit used a conventional tool, and 193 (49.9%) flossed when something entered their teeth. The majority of the participant 467(61.4%) don’t know when to renew toothbrush. The majority of them (92.6%) have never visited a dental clinic, and of those who have, the majority went for emergency dental pain treatment 52 (41.4%) and extraction 5 (8.6%) (Table 2).
Dietary habits of children
More than three forth of the children 590 (77.5%) drink tea with an added sugar. And two hundred twenty-one (29%) of the children drink coffee with an added sugar. Besides, three hundred nineteen (41%) of the children are found to drink soft drinks and two third of the children 553 (70%) consume sweets. Among these sweet food consumers, 272 (51.0%) consume less than once per week and 141(26.5%) consume on a daily basis. Five hundred sixty-five (74.2%) of the children consume milk less than once per week (Table 3).
Consumption frequency of selected foods and beverages in the past 7 days
The highest percentage among leafy green vegetables, banana, wheat, and maize to be taken at least once in the last seven days with a frequency rate of 759 (99.7%), 756 (99.3%), 31 (96.1%), and 727 (95.5%) respectively. It shows abundant consumption of vitamin C whereas fish and fish oil, meat and orange had been consumed at least once by 24 (3.2%), 370 (40.9%) and 460 (60.4%) respectively, and these are the lowest percentage observed and shows lacks calcium and vitamin D (Table 4).
Nutritional status and prevalence of dental caries
The median height and weight were 130.00 cm with IQR 16.00 and 29.00 kg with IQR 9 respectively. Among all children, 33 (4.3%) were underweight based on BAZ (< − 2 SD) with (95% CI 2.9–5.8), 620 (81.5%) were within the normal range (≥ − 2 SD and ≤ + 1 SD) with (95% CI 78.7–84.4) and 108 (14.2%) were overweight/obese (> + 1 SD) with (95% CI 11.7.0–16.6). The median score of BAZ was 0.37 with an IQR of 1.14.
The prevalence of dental caries was 119 (15.6%) with (95% CI 13.0–18.5). The prevalence is almost equally distributed among males 53 (15.1%) and females 66 (16.1%). The score of DMFT ranged from 0 to 8 and the mean DMFT was 0.27 (± 0.75). The prevalence of dental caries was higher among children who were underweight and overweight.21.2% and 18.5% respectively. On the other hand, it decreased among children with normal weight 14.8%; it was checked by the chi-square test, and was statistically not significant (Table 5).
Relationship of dental caries with nutritional status
The relationship between dental caries and nutritional status was not statistically significant with a P value (P = 0.32). The DMFT score was positively correlated to BAZ score, but the relationship did not show strong relationship with correlation coefficient value (r = 0.011).
Factors associated with dental caries
Place of residence, school type, educational status of the mother, exposure to the media, cleaning teeth, consumption of sugared coffee, sweet foods consumption, and milk consumption were candidate variables for multiple logistic analysis at P value < 0.25. In that regard, the multiple logistic regression analysis revealed the educational status of the mother, habit of cleaning teeth, consumption of sugared coffee, sweet foods consumption, and milk consumption had a statistical association.
Children whose mothers were not educated were 3.14 times (95% CI 1.03–9.56) at risk as compared to those whose mothers are educated. Besides, children who did not clean their teeth were 7.70 times more likely to have caries as compared to those who had cleaned their teeth (AOR = 7.70, 95% CI 4.00–14.85). On the other hand, children who had not consumed sugared coffee were 3.22 times reduced risk to have caries as compared to those who consume sugared coffee (AOR = 3.22, 95% CI 1.68–6.18). Meanwhile, children who had consumed sweet foods were 4.19 times at high risk as compared to those who had not consumed sweet foods (AOR = 4.19, 95% CI 1.76–9.96). Children who had not to consumed milk were 5.66 times more likely to have dental caries than those who had consume milk usually (AOR = 5.66, 95% CI 1.49–21.49). There was no statistically significant association between dental caries and nutritional status of the children (Table 6).
Discussion
The prevalence of dental caries was found 15.6% in line with the study conducted in Bahir Dar city, Ethiopia (21.8%) [18], Tanzania (17.6%) [23], and Nigeria (21.7%)[24]. However, it was lower than studies carried out in other parts of Ethiopia (36.3–48.5%) [17,18,19,20], Eritrea (78%) [25], and India (76.25%) [26]. It was also much lower than the figures reported by the WHO on oral health among of school children (60–90%) [7]. These figures could be due to socio-demographic and economic characteristics, and dietary behaviors. This might be due to the fact that 95% of the study participants were from urban residences.
Dental caries, on the other hand, was associated with the educational status of the mother, cleaning teeth, sugared coffee consumption, sweet consumption, and milk consumption. Educational status of the children’s mothers was found to be significantly associated with dental caries. Hence, there follows a simple logic here: as the education level of the mother increases, the probability of dental caries getting reduces. This was supported by similar findings from other parts of Ethiopia [17, 19]. It might be the fact that mothers who were educated are more likely to gain knowledge about dental health. It also gives an opportunity to have increased access to information from different media.
Dental caries development and teeth brushing practices had an inverse relationship. This goes in line with the study conducted in different parts of Ethiopia; Bahir Dar, Gonder, Adiss Abeba, and Finote Selam [17,18,19,20]. This finding is also in line with the study conducted in Tamil Nadu India [27]. It is generally true that cleaning teeth will remove away the food debris from the oral cavity. Therefore, Streptococcus mutans cannot get enough nutrients and time for growth, and there will be no acid production that causes dental caries development.
In this study, those children who had consumed sugared coffee do have an increased the chance of developing caries than those who had not consumed. Sweet consumption was also significantly associated with dental caries. Children who consumed more sweet foods frequently had a higher chance of developing dental caries than those who consumed sweet foods rarely. This is supported by a study done in Adiss Abeba, Finote Selam, and Harar town [19, 20, 28]. It is also in line with a study done in Mbeya City, Tanzania [23]. This might be related to much acid production by microorganisms like bacteria to teeth because of fermentation of the sweet foods. Gradually, the enamel of the tooth goes into dental caries [29].
Children who consume milk on a regular basis were 5.66 times safer than those children not consuming milk. It might be Cow milk had small amount of fluoride concentration and was similar to other studies [30].
Nutritional status (BAZ) and dental caries development was not significantly associated. This is in line with a study done in India (14). Dental caries is a multifactorial disease with several identified risk factors however the correlation between dental caries and nutritional status is not well understood, and requires further experimental research.
Difficulties in using radiological examination at the field level might reduce the actual magnitude of dental caries was the limitation of the study. All limitation of cross-sectional design was the limitations of this study.
Conclusion and recommendations
The prevalence of dental caries was found to be low compared to the WHO’s report on oral health among school children. The educational status of mothers, habit of cleaning teeth, consumption of sugared coffee, consumption sweet food, and milk consumption were the associated factors for dental caries. There was no significant association between dental caries and nutritional status. Behavioral intervention on dental hygiene and dietary habits should be given to children and parents. Moreover, further studies using all methods of diagnosis of dental caries and assessment of knowledge, attitude, and practices of children and their parents on dental hygiene should be recommended.
Availability of data and materials
The datasets during and/or analyzed during the current study is available from the corresponding author on reasonable request.
Abbreviations
- AOR:
-
Adjusted odds ratio
- BAZ:
-
BMI for age Z score
- BMI:
-
Body Mass Index
- CI:
-
Confidence interval
- COR:
-
Crude odds ratio
- DMFT:
-
Decayed missed filled teeth
- IQR:
-
Interquartile range
- GBD:
-
Global burden of disease
- NCD:
-
Non communicable disease
- SD:
-
Standard deviation
- SNNPR:
-
Southern Nations Nationality People Region
- WHO:
-
World Health Organization
References
Organization WH. Promoting Oral Health in Africa: Prevention and control of oral diseases and noma as part of essential noncommunicable disease interventions. 2016.
Organization WH. Ending childhood dental caries: WHO Implementation Manual. 2019.
Organization WH. Oral health surveys: basic methods: World Health Organization. 2013.
Monse B, Heinrich-Weltzien R, Benzian H, Holmgren C, van Palenstein HW. PUFA-an index of clinical consequences of untreated dental caries. Commun Dent Oral Epidemiol. 2010;38(1):77–82.
Mouradian WE, Slayton RL, Maas WR, Kleinman DV, Slavkin H, DePaola D, et al. Progress in children’s oral health since the surgeon general’s report on oral health. Acad Pediatr. 2009;9(6):374–9.
Organization WH. Health system profile. Regional Health Systems Observatory, WHO Eastern Mediterranean Regional Office: Islamic Republic of Iran; 2006.
Pitts NB, Zero DT, Marsh PD, Ekstrand K, Weintraub JA, Ramos-Gomez F, et al. Dental caries. Nat Rev Dis Primers. 2017;3(1):1–16.
Li M, Zhi Q, Zhou Y, Qiu R, Lin H. Impact of early childhood caries on oral health-related quality of life of preschool children. Eur J Paediatr Dent. 2015;16(1):65–72.
Arora A, Scott JA, Bhole S, Do L, Schwarz E, Blinkhorn AS. Early childhood feeding practices and dental caries in preschool children: a multi-centre birth cohort study. BMC Public Health. 2011;11(1):1–7.
Listl S, Galloway J, Mossey P, Marcenes W. Global economic impact of dental diseases. J Dent Res. 2015;94(10):1355–61.
Petersen PE. World Health Organization global policy for improvement of oral health-World Health Assembly 2007. Int Dent J. 2008;58(3):115–21.
Reddy KV, Thakur AS, Moon N, Reddy KE, Chandrakala S, Saxena S. Association between overweight and dental caries among 8–13 year old school children in central India. J Indian Assoc Public Health Dent. 2018;16(1):22.
Folayan MO, Adeniyi AA, Chukwumah NM, Onyejaka N, Esan AO, Sofola OO, et al. Programme guidelines for promoting good oral health for children in Nigeria: a position paper. BMC Oral Health. 2014;14(1):1–8.
Kumar S, Kroon J, Lalloo R, Kulkarni S, Johnson NW. Relationship between body mass index and dental caries in children, and the influence of socio-economic status. Int Dent J. 2017;67(2):91–7.
Bagramian RA, Garcia-Godoy F, Volpe AR. The global increase in dental caries. A pending public health crisis. Am J Dent. 2009;22(1):3–8.
Office ATH. Anual Plan Of Areka Town Health Office. Areka, South Ethiopia.: Areka Health office 2018.
Ayele FA, Taye BW, Ayele TA, Gelaye KA. Predictors of dental caries among children 7–14 years old in Northwest Ethiopia: a community based cross-sectional study. BMC Oral Health. 2013;13(1):1–6.
Mulu W, Demilie T, Yimer M, Meshesha K, Abera B. Dental caries and associated factors among primary school children in Bahir Dar city: a cross-sectional study. BMC Res Notes. 2014;7(1):1–7.
Berhane HY, Worku A. Oral health of young adolescents in Addis Ababa—A community-based study. Open J Prevent Med. 2014;2014.
Teshome A, Yitayeh A, Gizachew M. Prevalence of dental caries and associated factors among Finote Selam primary school students aged 12–20 years, Finote Selam town. Ethiopia Age. 2016;12(14):15–7.
Onis Md, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World health Organization. 2007;85:660–7.
Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3(1):1–8.
Mwakayoka H, Masalu JR, Kikwilu EN. Dental caries and associated factors in children aged 2–4 years old in Mbeya City, Tanzania. J Dent. 2017;18(2):104.
Adeniyi AA, Oyapero OA, Ekekezie OO, Braimoh MO. Dental Caries and Nutritional Status of School Children in Lagos, Nigeria - A Preliminary Survey. J West Afr Coll Surg. 2016;6(3):15–38.
Andegiorgish AK, Weldemariam BW, Kifle MM, Mebrahtu FG, Zewde HK, Tewelde MG, et al. Prevalence of dental caries and associated factors among 12 years old students in Eritrea. BMC Oral Health. 2017;17(1):1–6.
Ingle NA, Dubey HV, Kaur N, Gupta R. Prevalence of dental caries among school children of Bharatpur city, India. J Int Soc Prevent Commu Dent. 2014;4(1):52.
Parasuraman G, Krishna Y, Kaviya M, Jain N, Rajendiran P, Dutta R. A study on the prevalence of dental caries among the school going children in Tamil Nadu. Int J Commu Med Public Health. 2017;10:3582–9.
Ademe D, Admassu D, Balakrishnan S. Analysis of salivary level Lactobacillus spp. and associated factors as determinants of dental caries amongst primary school children in Harar town, eastern Ethiopia. BMC Pediatr. 2020;20(1):1–9.
Elangovan A, Mungara J, Joseph E. Exploring the relation between body mass index, diet, and dental caries among 6–12-year-old children. J Indian Soc Pedodont Prevent Dent. 2012;30(4):293.
Larsen M, Senderovitz F, Kirkegaard E, Poulsen S, Fejerskov O. Dental fluorosis in the primary and the permanent dentition in fluoridated areas with consumption of either powdered milk or natural cow’s milk. J Dent Res. 1988;67(5):822–5.
Acknowledgements
We would like to acknowledge Wolaita Sodo University for providing materials used for the work. Our deepest gratitude goes to the data collectors, kebeles leaders and Areka town’ health officers for their cooperation through the entire data collection time. Last but not least, we owe the respondents a heartfelt credit for their cooperation.
Funding
Wolaita Sodo University under NORAD project was funded the research. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript."
Author information
Authors and Affiliations
Contributions
SB: Initiated the research; wrote the research proposal; conducted the research, worked on data entry and analysis, and wrote the manuscript. SBW: Involved in the write up of methodology of proposal and research work, analysis and manuscript write up. YK: Contributed in the write up of proposal and write up of the manuscript. DW: participated in the write up of methodology of proposal, research work and write up of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
All methods were conducted in accordance with relevant guidelines and regulations of observational studies. Ethical clearance was obtained from the Wolaita Sodo University, Institutional Review Committee of the College of health sciences and Medicine. An official letter of cooperation was given to Areka town Health Office. Data collectors had explained the objective, benefit and risks of the study to get informed written consent for mothers or caregivers of the children. Moreover, Data collectors were give advice mothers or caregivers of the undernourished child to provide additional balanced diets for their children and to visit the nearby health facility. The right of the respondent to withdraw from the interview or not to participate was respected. Besides, identification of an informant was possible only through specific identification numbers.
Consent for publication
Not applicable.
Competing interests
The authors declared that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bassa, S., Workie, S.B., Kassa, Y. et al. Prevalence of dental caries and relation with nutritional status among school-age children in resource limited setting of southern Ethiopia. BMC Oral Health 23, 84 (2023). https://doi.org/10.1186/s12903-023-02786-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-02786-6