
Abstract
Background
This study aimed to evaluate the effect of virtual cement space and restorative materials on the fit of computer-aided design and computer-aided manufacturing (CAD-CAM) endocrowns.
Methods
A mandibular first molar tooth model received a butt joint margin endocrown preparation with a 2-mm occlusal thickness. Then, using a 3D-printing system, 120 copies of this prepared die were printed and assigned equally to three groups with different cement space settings (30, 60, and 120 μm) during the chairside CAD design. In the milling process, CAD-based models with a particular space setting were subdivided into four groups (n = 10) and fabricated from different CAD-CAM materials: Vita Suprinity (VS), Celtra Duo (CD), Lava Ultimate (LU), and Grandio blocs (GR). Finally, the endocrowns were stabilized over their corresponding models with siloxane and subjected to micro-computed tomography to measure the fit.
Results
The cement space that was predesigned at 30 μm generated the largest marginal discrepancy (from 144.68 ± 22.43 μm to 174.36 ± 22.78 μm), which was significantly different from those at 60 μm and 120 μm (p < 0.001). The combination of VS or CD with a pre-setting cement space of 60 μm and the combination of LU or GR with a cement space of 120 μm showed better agreement between the predesigned and actual measured marginal gap widths. For internal adaptation, only the cement space set to 30 μm exceeded the clinically acceptable threshold (200 μm).
Conclusions
The setting of the cement space and restorative material significantly affected the marginal adaptation of CAD-CAM endocrown restorations. Considering the discrepancy between design and reality, different virtual cement spaces should be applied to ceramic and resin composite materials.
Similar content being viewed by others

Background
Proper fit of crowns and abutments, presented by internal and marginal gaps, affects the long-term success of dental restorations [1]. The internal gap is measured as the perpendicular distance from the internal surface of the restoration to the axial wall of the preparation, and the marginal gap is the perpendicular distance at the cavosurface margin [2]. Poor marginal adaptation causes the dissolution of the cement layer, resulting in secondary caries and periodontal disease, eventually leading to clinical failure [3, 4]. An inappropriate internal gap can increase the thickness of the cement, decrease the adhesive strength at the adhesive interface, and reduce the resistance to fracture of the restoration [1, 5, 6]. Marginal gaps of ≤ 120 μm and internal gaps of ≤ 200 μm have traditionally been considered clinically acceptable [7,8,9].
Computer-aided design and computer-aided manufacturing (CAD-CAM) dentistry has been widely applied to enhance the effectiveness and accuracy of treatment procedures and outcomes. By chairside designation and production, endocrown restoration has achieved excellent esthetics and favorable biomechanical behavior and has become the preferred choice for many clinicians to restore severely damaged teeth after endodontic treatment [10,11,12]. In a systematic review, CAD-CAM endocrowns obtained clinical success rates ranging from 94 to 100% [13]. Secondary caries and loss of retention, which are closely related to the dissolution of the luting cement and deficiencies in marginal and internal adaptation, were the main causes of failure in the long-term follow-up of CAD-CAM endocrowns [14]. Therefore, it is essential to better understand the factors affecting the fit of CAD-CAM endocrowns.
The CAD-CAM system setting allows the adjustment of different parameters, including the virtual cement space (CS), during the virtual 3-dimensional (3D) design of the restoration [15]. Setting a certain CS width around the fabricated CAD-CAM restoration is important for proper adaptation between the restoration and the prepared abutments, and for a good distribution of the luting agents [16,17,18,19]. Studies have shown that the CS value significantly affects the marginal and internal fit of CAD-CAM crowns [20,21,22]. Whether CS settings have a similar effect on endocrown restoration requires further investigation. According to previous studies, variations in the setting values of CS around CAD-CAM endocrowns ranging from 40 to 120 μm yield different margins and internal adaptations [4, 6, 7]. Therefore, a detailed study of how the CS setting affects the marginal and internal fit of CAD-CAM endocrowns is important.
In addition to the CS setting, the choice of restorative material also influences the final fit of the restoration. With improvements and innovations in CAD-CAM technology, various materials with different compositions and physical properties have become available as CAD-CAM materials [23, 24]. Ceramic materials are popular because of their high esthetics, biocompatibility, and durability; composite resins possess biomimetic properties close to those of human teeth and are more resistant to higher occlusal forces [7, 25]. However, investigations of the effects of different materials on restoration adaptation have reported conflicting findings. Some studies reported that restorations with ceramic materials provide a more favorable marginal and internal fit than composite resins [7, 26], while others showed opposite results [4, 27,28,29].
Despite the widespread use of endocrowns, studies focusing on milling parameters for the ideal fit of manufactured pieces are lacking. The choice of setting values for virtual CS and the type of restorative materials remains unclear. Therefore, this study aimed to combine the parameters of virtual CS and restorative materials and evaluate the fit of CAD-CAM endocrown restorations to determine the best combination. The null hypothesis was that neither the CS nor the type of restorative material would influence the marginal and internal adaptation of endocrowns.
Methods
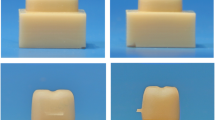
A typodont mandibular first molar (A20A-200; NISSIN Dental Products, Inc., Kyoto, Japan) was prepared for a flat butt joint margin endocrown with a 2-mm occlusal reduction and 2-mm pulp chamber extension with an internal taper of 8° of the axial walls [30, 31]. The endocrown preparation margin was located on the enamel. Then, using a 3D-printing system (DLP1080E, HAN’S LASER, Shenzhen, China) and resin material (T-MRD-521, HAN’S LASER, Shenzhen, China), the prepared molar was replicated into 40 resin blocks, each containing 3 copies (Fig. 1), 120 specimens were produced.

Standardized identical dies of endocrown prepared mandibular molar fabricated by using a 3D-printing system
For all specimens, digital optical impressions were performed with an intraoral scanner, and thus 120 standard tessellation language (STL) files were acquired and imported into the CAD software (CEREC AC, Dentsply Sirona, York, PA, USA), ready to design the endocrown. According to the subsequent settings of the virtual CS (30, 60, and 120 μm), the STL files were randomly distributed into three groups (n = 40). The design parameters of the marginal adhesive gap were set to 30, 60, or 120 μm, in the CAD software (Fig. 2). All endocrowns were designed with identical external contours. In the milling process, using CAM software, these three groups were further divided into subgroups based on different CAD-CAM materials: Vita Suprinity (VS; VITA Zahnfabrik), Celtra Duo (CD; Dentsply Sirona), Lava Ultimate (LU; 3 M ESPE), and Grandio blocs (GR; VOCO). The characteristic features of the tested materials are listed in Table 1 [25, 32,33,34]. Ten endocrowns of each material were fabricated for each STL file with a specific CS setting.

The cement space settings used in each experimental group
The stabilization of the fabricated endocrown to the corresponding models was performed using a siloxane material (GC Fit Checker Advanced, GC Dental Industrial Corp, Tokyo, Japan) under a constant load of 9.8 N for 10 min [35]. Thereafter, the marginal and internal gaps of all specimens were analyzed using high-resolution micro-computed tomography (micro-CT) images (ZKKS-MCT-Sharp, Zhongke Kaisheng Medical Technology Company, Guangzhou, China). Each sample in the scanning tube was placed perpendicular to the X-ray beam for scanning, by setting the following scanning parameters [29]: accelerating voltage of 70 kV, current of 100 μA, exposure time of 79 ms per frame, Al + Cu filter, and rotation step of 0.6° for a 180° rotation. The pixel size of each image was 15 μm. Approximately 1200 cross-sections were obtained from each sample.
After loading the acquired projection images, the software (NRecon v1.6.9, Bruker Micro-CT, Billerica, MA, USA) automatically assimilated the images into a 3D reconstruction. Three vertical sections were selected from the core region of each specimen in the buccolingual (BL) and mesiodistal (MD) directions (Fig. 3A). Seven points (N1-N7) were selected on each of the BL and MD sections (Fig. 4) to analyze the internal fit. N1, N2, N6, and N7 were measured on the cervical seat, and N3, N4, and N5 were measured on the pulpal floor. A total of 42 measurements were taken for each specimen to analyze the internal fit. The same cross-sections used in internal adaptation were used to measure marginal fitness. In addition, two cross sections connecting the endocrown corners were added. A total of 16 points (Fig. 3B), including three points on each of the four sides, buccal (B1, B2, and B3), lingual (L1, L2, and L3), mesial (M1, M2, and M3), distal (D1, D2, and D3), and one point in each of the four corners (C1, C2, C3, and C4) of each specimen, were selected for marginal adaptation measurements [36]. The gap between the restoration and tooth at the selected points was measured in micrometers (µm).

Micro-CT scan image (horizontal cut). A Selected sections in buccolingual and mesiodistal directions for internal and marginal adaptation. B Additional sections (C1-C4) for marginal adaptation

Micro-CT scan image (vertical sections). Schematic representation of measurement positions for internal adaptation. N1, N2, N6, and N7 were measured as the cervical seat, and N3, N4, and N5 were measured as pulpal floor
Statistical analyses were performed using IBM SPSS Statistics, v23 (IBM Corp, Armonk, NY, USA). The normality assumption of the data and the homogeneity of the variances were checked using the Shapiro–Wilk and Levene’s tests, respectively. Because the data were normally distributed, 2-way analysis of variance (ANOVA) and Tukey’s honestly significant difference test were used (α = 0.05).
Results
Regarding the variable CS settings, data analysis showed a statistically significant effect of CS settings on the marginal and internal discrepancy values of tested endocrowns (p < 0.001). For the marginal discrepancy, the highest values were recorded in group CS-30 (144.68–174.36 μm), followed by group CS-120 (81.74–105.35 μm), while the lowest values were recorded in group CS-60 (52.37–82.73 μm). Group CS-60 was statistically significantly different from the CS-30 or CS-120 groups (p < 0.001) (Table 2). All measured margin gap values were within the clinically acceptable range for CAD-CAM restorations, except for group CS-30. For the internal gap (Table 3), the CS-30 group showed significantly higher values (274.48–307.91 μm), in which all measurements exceeded the maximum clinically accepted value of 200 μm. When the CS was designed to be 60 or 120 μm, the internal gap values were within the acceptable range, and no statistically significant difference was found between these two groups (p > 0.05).
Regarding the variable materials, all the tested groups displayed statistically significant differences in marginal fit (p < 0.001). Group VS and CD had a narrower marginal gap than the LU and GR groups (p < 0.001) (Table 2). No statistically significant differences were observed between the LU and GR groups or the VS and CD groups (p > 0.05). For the internal adaptation, no significant differences were observed between the four materials (p > 0.05) (Table 3).
To determine the effect of regions on the internal adaptations, the measurements of the internal gap were compared between the pulpal floor and cervical seat. In the space for all groups, the pulpal floor showed a significantly higher value than the cervical region (p < 0.05) (Table 4).
Discussion
Ensuring that the gap between endocrowns and their abutments is within acceptable marginal and internal values is critical for a positive long-term outcome. This study evaluated the marginal and internal fit of CAD-CAM endocrowns fabricated using four materials (VS, CD, LU, and GR) and three CS settings (30, 60, and 120 μm). The results showed that differences in the CS settings significantly affected the marginal and internal adaptation of the endocrown, while the types of restorative materials only affected the marginal adaptation but not the internal fit. Therefore, the null hypothesis was partially rejected.
Adaptation can be achieved using various methods, including micro-CT imaging. It can provide accurate, 2D, or 3D high-quality images to show the restoration in any direction and orientation without invasion or destruction of the subject being investigated [4, 22, 37, 38]. In addition, precise visualization of the entire cement layer, as well as segmentation and quantification of different areas and materials, can be achieved [37]. Moreover, the selection of measurement points is crucial. Studies have recommended that at least 10 points be randomly selected to measure the adaptation of the restoration and that measurements should be performed throughout the restoration [36, 39]. In addition to the conventional margin measurement points in the six sections used in the previous study, the present study used another two cross-sections joining the endocrown corners for measurement, which enabled the higher reliability of our results.
The CAD-CAM fabricated endocrown has shown significant advantages in clinical practice, but some basic information still needs to be clarified through further investigations, including the optimal CS setting. Theoretically, there is a dilemma in CS designation. A narrow CS can achieve the best fitness of the fabricated restoration and abutment, but such a luting space would be difficult to manage in practice. A wide CS provides more luting space but might cause more microleakage and restoration detachment [15]. The lowest CS value of the CAD-CAM crown was suggested to be set at 50 μm, of which 30 μm was for the space of cement and avoidance of friction, and the remaining 20 μm was for possible deterioration during production [6, 22, 40]. However, discrepancies in placement were not considered in this study. In addition, this proposal has not been supported by experiments or clinical trials.
In this study, three scales of CS values were chosen based on previous reports [4, 6, 7, 21], in which 30 and 120 μm were the lowest and highest acceptable values, respectively; 60 μm was the median of 30 and 120, and, arguably, 60 μm was slightly larger than the suggested 50 μm. Unexpectedly, the CS-30 group showed the highest mean gap width, while the CS-60 group generated the smallest marginal and internal gaps. The relationship between the CS setting in software and the marginal discrepancy in restored teeth has recently attracted attention, and previous reports mentioned that the marginal gap increased with a decrease in the CS setting values [18, 21]. A smaller CS prevents the restoration of complete seating, thus exacerbating the marginal gap. In addition, a negative correlation between the CS setting value and the time for manual crown adjustment was reported [41], indicating that a larger CS value is a possible strategy to improve adaptation and reduce internal adjustments. However, when the CS was designed to be even wider, reaching the maximum threshold recommended by the manufacturer (120 μm), the marginal fit of the restorations worsened, although the actual gap width measurements were still within the acceptable range. The discrepancy between the designation and reality may be due to errors in restoration production, placement inaccuracies, and difficulties in expressing excess cement.
Due to the variable elasticity modulus and milling properties, different CS designations may be preferred to improve CAD-CAM restoration fitness when utilizing different materials [23, 25, 26]. Four products composed of ceramic materials (VS and CD) or resin composites (LU and GR) were used in this study. The possibility of a role for materials in adaptation was verified in the present study. When the CS was set to 60 μm in the software, the VS and CD materials generated an actual marginal gap width close to the predesigned 60 μm, which was better than that of the LU and GR materials. When the CS was set at 120 μm, the actual width of the gap was close to 120 μm in the restorations made of LU and GR. Ceramics have a higher modulus of elasticity and can be more accurately milled and hardly deformable during production [7, 26]. On the contrary, resin composites have better machinability and adaptation [4, 29]; therefore, less precision in milling and more deformation might occur during late processing. In practice, a high agreement between the designation and reality is always preferred. Our results indicate that the settings of CS must be changed according to the material used.
In this study, the effect of crystallization on the fit of VS versus CD endocrowns was investigated. Compared with the fully crystallized ceramic block (CD), VS is a partially crystallized ceramic block that requires post-milling crystallization to achieve its maximum mechanical and optical properties. During the crystallization process, the lithium silicate and meta-silicate crystals become smaller, and densification increases with a reduction in particle size for a close-packed arrangement [42]. Previous studies reported that densification shrinkage during the crystallization process affects the adaptation of ZLS crowns [8, 24]. However, our study found no significant differences between VS and CD. This difference can be attributed to the preparation design. The risk of causing a marginal discrepancy is lower in endocrowns with a flat butt upper gingival shoulder, as used in this study, than that in other restoration designs. Therefore, post-sintering shrinkage of the ZLS material did not significantly affect the maintenance of a “good fit”.
To analyze the internal fit in more detail, we divided the measurements of the internal gap into two different areas for accurate comparisons: the cervical seat and the pulpal floor (Table 4). Consistent with the present study, the internal gap in the pulp chamber has been reported to be the worst-fitting area [4, 7, 36]. This may be due to the narrow and complex structure of the pulpal chamber, and the limited optical depth of the scanner, resulting in blurred images of the pulpal area [4, 7, 36, 43].
This study focused on the influence of CS setting and restorative material factors on the adaptation of a CAD-CAM endocrown. The results showed that a CS setting of 30 μm would generate poor fitness, while a setting of 60 μm or 120 μm would be acceptable. Moreover, considering the need for a strong correlation between design and reality, a space setting of 60 μm would be better for ceramic materials, and 120 μm would be better for resin composites. Further detailed experimental studies and clinical trials are required in the future. To the best of our knowledge, this is the first relevant study on CS designation according to different materials.
Our study has several limitations. As an in vitro experiment, this could not include in vivo factors, such as patient cooperation and contamination with saliva and blood during scanning processing. In addition, a single-tooth model and one scanning and milling system during the design and fabrication of CAD-CAM endocrowns eliminate inconsistencies but overlook diversity in the real world [9, 44]. Further studies are required to understand the influence of clinical oral conditions and the diversity of the CAD-CAM system on the adaptation of endocrowns.
Conclusion
Within the limitations of this in vitro study, the following conclusions were drawn:
-
1.
The setting of virtual CS had a significant effect on the adaptation of CAD-CAM endocrown restoration. Setting at 30 μm would generate poor fitness, while 60 μm or 120 μm would be acceptable.
-
2.
When considering the high coincidence between design and reality, a space setting at 60 μm would be better for ceramic material and at 120 μm would be better for resin composite.
Availability of data and material
All data generated or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CS:
-
Cement space
- VS:
-
Vita suprinity
- CD:
-
Celtra duo
- LU:
-
Lava ultimate
- GR:
-
Grandio blocs
- CAD-CAM:
-
Computer-aided design and computer-aided manufacturing
- 3D:
-
3-Dimensional
- STL:
-
Standard tessellation language
- BL:
-
Buccolingual
- MD:
-
Mesiodistal
References
Goujat A, Abouelleil H, Colon P, Jeannin C, Pradelle N, Seux D, Grosgogeat B. Marginal and internal fit of CAD-CAM inlay/onlay restorations: a systematic review of in vitro studies. J Prosthet Dent. 2019;121(4):590-597 e593.
Holmes JR, Bayne SC, Holland GA, Sulik WD. Considerations in measurement of marginal fit. J Prosthet Dent. 1989;62(4):405–8.
He Y, Li M, Tong G, Meng Y, Hao S, Hu S, Yan W, Yang D. hPTH(3–34)(29–34) selectively activated PKC and mimicked osteoanabolic effects of hPTH(1–34). Bone. 2020;135:115326.
Zimmermann M, Valcanaia A, Neiva G, Mehl A, Fasbinder D. Three-dimensional digital evaluation of the fit of endocrowns fabricated from different CAD/CAM materials. J Prosthodont. 2019;28(2):e504–9.
Zhang Y, Kim JW, Bhowmick S, Thompson VP, Rekow ED. Competition of fracture mechanisms in monolithic dental ceramics: flat model systems. J Biomed Mater Res B Appl Biomater. 2009;88(2):402–11.
Uzgur R, Ercan E, Uzgur Z, Colak H, Yalcin M, Ozcan M. Cement thickness of inlay restorations made of lithium disilicate, polymer-infiltrated ceramic and nano-ceramic CAD/CAM materials evaluated using 3D X-ray micro-computed tomography. J Prosthodont. 2018;27(5):456–60.
El Ghoul WA, Ozcan M, Ounsi H, Tohme H, Salameh Z. Effect of different CAD-CAM materials on the marginal and internal adaptation of endocrown restorations: an in vitro study. J Prosthet Dent. 2020;123(1):128–34.
El-Ashkar A, Taymour M, El-Tannir A. Evaluation of the marginal and internal gaps of partially crystallized versus fully crystallized zirconia-reinforced lithium silicate CAD-CAM crowns: an in vitro comparison of the silicone replica technique, direct view, and 3-dimensional superimposition analysis. J Prosthet Dent. 2021. https://doi.org/10.1016/j.prosdent.2021.07.024.
Ferrairo BM, Piras FF, Lima FF, Honorio HM, Duarte MAH, Borges AFS, Rubo JH. Comparison of marginal adaptation and internal fit of monolithic lithium disilicate crowns produced by 4 different CAD/CAM systems. Clin Oral Investig. 2021;25(4):2029–36.
Naumann M, Schmitter M, Frankenberger R, Krastl G. “Ferrule comes first. Post is second!” fake news and alternative facts? a systematic review. J Endod. 2018;44(2):212–9.
Govare N, Contrepois M. Endocrowns: a systematic review. J Prosthet Dent. 2020;123(3):411-418 e419.
Al-Dabbagh RA. Survival and success of endocrowns: a systematic review and meta-analysis. J Prosthet Dent. 2021;125(3):415 e411-415 e419.
Sedrez-Porto JA, Rosa WL, da Silva AF, Munchow EA, Pereira-Cenci T. Endocrown restorations: a systematic review and meta-analysis. J Dent. 2016;52:8–14.
Belleflamme MM, Geerts SO, Louwette MM, Grenade CF, Vanheusden AJ, Mainjot AK. No post-no core approach to restore severely damaged posterior teeth: an up to 10-year retrospective study of documented endocrown cases. J Dent. 2017;63:1–7.
de Tabata Lucas F, de Lima Silva Taiana A, de Paula Silveira Alessandra C, Ribeiro Ana Paula D. Marginal and internal fit of CAD-CAM composite resin and ceramic crowns before and after internal adjustment. J Prosthet Dent. 2020;123(3):500–5.
Wang CJ, Millstein PL, Nathanson D. Effects of cement, cement space, marginal design, seating aid materials, and seating force on crown cementation. J Prosthet Dent. 1992;67(6):786–90.
Dauti R, Lilaj B, Heimel P, Moritz A, Schedle A, Cvikl B. Influence of two different cement space settings and three different cement types on the fit of polymer-infiltrated ceramic network material crowns manufactured using a complete digital workflow. Clin Oral Investig. 2020;24(6):1929–38.
Elbadawy AA, Elaziz MHA, Alnazzawi AA, Borzangy SS. Effect of various digital cement space settings on the adaptation of CAD/CAM occlusal veneer “micro-ct evaluation.” Dent Mater J. 2021;40(3):625–30.
Iwai T, Komine F, Kobayashi K, Saito A, Matsumura H. Influence of convergence angle and cement space on adaptation of zirconium dioxide ceramic copings. Acta Odontol Scand. 2008;66(4):214–8.
Rinke S, Fornefett D, Gersdorff N, Lange K, Roediger M. Multifactorial analysis of the impact of different manufacturing processes on the marginal fit of zirconia copings. Dent Mater J. 2012;31(4):601–9.
Kale E, Seker E, Yilmaz B, Ozcelik TB. Effect of cement space on the marginal fit of CAD-CAM-fabricated monolithic zirconia crowns. J Prosthet Dent. 2016;116(6):890–5.
Suzuki S, Katsuta Y, Ueda K, Watanabe F. Marginal and internal fit of three-unit zirconia fixed dental prostheses: effects of prosthesis design, cement space, and zirconia type. J Prosthodont Res. 2020;64(4):460–7.
Spitznagel FA, Boldt J, Gierthmuehlen PC. CAD/CAM ceramic restorative materials for natural teeth. J Dent Res. 2018;97(10):1082–91.
Kim JH, Oh S, Uhm SH. Effect of the crystallization process on the marginal and internal gaps of lithium disilicate CAD/CAM crowns. Biomed Res Int. 2016;2016:8635483.
Lawson NC, Bansal R, Burgess JO. Wear, strength, modulus and hardness of CAD/CAM restorative materials. Dent Mater. 2016;32(11):e275–83.
Goujat A, Abouelleil H, Colon P, Jeannin C, Pradelle N, Seux D, Grosgogeat B. Mechanical properties and internal fit of 4 CAD-CAM block materials. J Prosthet Dent. 2018;119(3):384–9.
Azarbal A, Azarbal M, Engelmeier RL, Kunkel TC. Marginal fit comparison of CAD/CAM crowns milled from two different materials. J Prosthodont. 2018;27(5):421–8.
Chavali R, Nejat AH, Lawson NC. Machinability of CAD-CAM materials. J Prosthet Dent. 2017;118(2):194–9.
Yildirim G, Uzun IH, Keles A. Evaluation of marginal and internal adaptation of hybrid and nanoceramic systems with microcomputed tomography: an in vitro study. J Prosthet Dent. 2017;118(2):200–7.
Wang J, Ling Z, Zheng Z, Zheng C, Gai Y, Zeng Y, Zhu X, Chen L, Wu B, Yan W. Clinical efficacy of ceramic versus resin-based composite endocrowns in Chinese adults: study protocol for a randomized controlled trial. Trials. 2020;21(1):559.
Sun J, Ruan W, He J, Lin X, Ci B, Yin S, Yan W. Clinical efficacy of different marginal forms of endocrowns: study protocol for a randomized controlled trial. Trials. 2019. https://doi.org/10.1186/s13063-019-3530-1.
Zheng Z, He Y, Ruan W, Ling Z, Zheng C, Gai Y, Yan W. Biomechanical behavior of endocrown restorations with different CAD-CAM materials: a 3D finite element and in vitro analysis. J Prosthet Dent. 2021;125(6):890–9.
Wendler M, Belli R, Petschelt A, Mevec D, Harrer W, Lube T, Danzer R, Lohbauer U. Chairside CAD/CAM materials. Part 2: flexural strength testing. Dent Mater. 2017;33(1):99–109.
Lambert H, Durand JC, Jacquot B, Fages M. Dental biomaterials for chairside CAD/CAM: state of the art. J Adv Prosthodont. 2017;9(6):486–95.
de Paula Silveira AC, Chaves SB, Hilgert LA, Ribeiro AP. Marginal and internal fit of CAD-CAM-fabricated composite resin and ceramic crowns scanned by 2 intraoral cameras. J Prosthet Dent. 2017;117(3):386–92.
Topkara C, Keles A. Examining the adaptation of modified endocrowns prepared with CAD-CAM in maxillary and mandibular molars: A microcomputed tomography study. J Prosthet Dent. 2022;127(5):744–49.
Dauti R, Cvikl B, Lilaj B, Heimel P, Moritz A, Schedle A. Micro-CT evaluation of marginal and internal fit of cemented polymer infiltrated ceramic network material crowns manufactured after conventional and digital impressions. J Prosthodont Res. 2019;63(1):40–6.
Peng CC, Chung KH, Ramos V. Assessment of the adaptation of interim crowns using different measurement techniques. J Prosthodont. 2020;29(1):87–93.
Gassino G, Barone Monfrin S, Scanu M, Spina G, Preti G. Marginal adaptation of fixed prosthodontics: a new in vitro 360-degree external examination procedure. Int J Prosthodont. 2004;17(2):218–23.
Grajower R, Lewinstein I. A mathematical treatise on the fit of crown castings. J Prosthet Dent. 1983;49(5):663–74.
Wilson PR. Effect of increasing cement space on cementation of artificial crowns. J Prosthet Dent. 1994;71(6):560–4.
Gold SA, Ferracane JL, da Costa J. Effect of crystallization firing on marginal gap of CAD/CAM fabricated lithium disilicate crowns. J Prosthodont. 2018;27(1):63–6.
Kokubo Y, Nagayama Y, Tsumita M, Ohkubo C, Fukushima S, Vult von Steyern P. Clinical marginal and internal gaps of In-Ceram crowns fabricated using the GN-I system. J Oral Rehabil. 2005;32(10):753–8.
Ha SJ, Cho JH. Comparison of the fit accuracy of zirconia-based prostheses generated by two CAD/CAM systems. J Adv Prosthodont. 2016;8(6):439–48.
Acknowledgements
Not applicable.
Funding
This study was supported in part by grants from Natural Science Foundation of Guangdong Province, 2018A0303130213; Clinical Research Startup Program of Southern Medical University by High-level University Construction Funding of Guangdong Provincial Department of Education, LC2016PY023; Clinical Research Program of Nanfang Hospital Southern Medical University, 2018CR018.
Author information
Authors and Affiliations
Contributions
Conceptualization: ZTZ, HBW, and WJY; methodology: HBW, ZTL, and JYM; software: JYM, YTZ, YXZ, and JLW; writing original draft preparation: ZTZ; writing and review and editing: ZTZ, HBW, and WJY. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This article does not contain any studies with human participants or animals performed by any of the authors.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zheng, Z., Wang, H., Mo, J. et al. Effect of virtual cement space and restorative materials on the adaptation of CAD-CAM endocrowns. BMC Oral Health 22, 580 (2022). https://doi.org/10.1186/s12903-022-02598-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-022-02598-0