
Abstract
Background
The prevalence of Early Childhood Caries (ECC) in South Africa was last determined in 2002 in a national survey. Since then only few scattered studies were conducted across pocketed communities in the country. There appears to be an increasing trend in dental caries prevalence in South Africa. Since South Africa has one of the highest burden of HIV in the world, less focus was spent on Non-Communicable Diseases (NCDs), it was only when HIV patients developed NCD’s did the government start evaluating NCDs. However, oral health is still not given enough attention within the health sphere. It is the hope of this systematic review to showcase the extent of dental caries amongst the future leaders of our country.
Objectives
The systematic review presents the prevalence and severity of early childhood caries between age groups and provinces in South Africa from 1975 to 2014.
Design
A systematic review of prevalence was performed. Settings and participants: All studies performed on children under the age of six who lived in South Africa were eligible to be included.
Primary and Secondary outcome measures
The prevalence of ECC and the dmft scores were the primary and secondary outcome measures.
Results
Twenty-one studies were included in the present review. The overall prevalence was 44.94% (95% confidence interval (C.I.) 39.73–50.15%) and the overall dmft score was 2.422 (95% C.I. 2.148–2.696).
Conclusions
The dmft score was the lowest in the Limpopo Province and highest in the Eastern Cape. ECC prevalence increased post-apartheid possibly on account of lifestyle changes due to the exodus from rural to urban and peri-urban areas.
Registration The protocol of this systematic review was registered with PROSPERO, CRD42018112161, in November 2018.
Similar content being viewed by others


Introduction
Dental caries is the progressive damage to the enamel caused by commensal bacteria in the mouth. External pathogens have not been shown to cause dental caries. However, a change in the homeostasis between normal commensals in the mouth and the surrounding tissues and structures has been shown to lead to dental caries causation [1]. Bacterial concentrations increase when there is inadequate removal of plaque and increased dietary sugar [2]. If untreated, dental caries can lead to pain and early loss of teeth, resulting in disfigurement and affect the oral health-related quality of life [3]. Early childhood caries (ECC) is defined as the presence of one or more cavitated or non-cavitated, decayed, missing (due to caries), or filled tooth in any primary (deciduous) tooth in a child aged under six years [4].
In 2017, the incidence of oral health conditions was ranked third-highest among all health problems and consisted of 3,6 billion cases, and approximately 530 million children suffer from deciduous caries globally [5]. The prevalence of ECC varies both across countries [6,7,8] and within the same country [7]. Similarly, the prevalence of ECC in South Africa (SA) differs between provinces. In 2004, the national prevalence of the disorder was 60.3% for 6 year olds [9]. No current national prevalence data for ECC in South Africa is available. However, Smit et al. [10] documented a significantly higher prevalence (84%) in the Western Cape than described by van Wyk et al. in 2004 [9].
The severity of the dental disease is expressed as the decayed, missing and filled tooth score and measured as the decayed, missing and filled tooth (dmft) index. International figures for the dmft indices vary: in Qatar it was reported as 7.6 [11], 3.65 in China [12], and 2.46 in Palestine [13]. In South Africa, the national dmft score was 2.4 [9], and 6.2 in the Western Cape [10].
South Africa is a densely populated developing country. It is listed as an upper- to middle-income country with 59.62 million inhabitants, of which children under the age of five constitute almost 10% or 5.7 million [14]. Historically, South Africa was immersed in political and racial division. Since the freedom charter was introduced in 2004, every South African is considered equal. Globally, South Africa has the highest income disparity within its constituents, with a Gini index of 63.0 in 2014 [15]. The Gini index determines the measure of inequality within a country. An index of 100 represents perfect inequality, and a measure of 0 means that the population is equal (all individuals have the same income) [16]. The country’s economic inequalities have resulted in an association between the prevalence of dental caries and unmet treatment needs [17].
Early Childhood Caries (ECC) has a significant burden in South Africa, particularly in the Western Cape Province. A few published studies report ECC’s prevalence in children under six years of age and under living in South Africa. To effectively prevent and manage ECC in South Africa, it is essential to know the disease prevalence and severity within this population. Therefore, the present study aimed to determine the prevalence and severity of ECC in South Africa.
Materials and methods
This study was conducted according to the Meta-Analysis of Observational Studies in Epidemiology (MOOSE) guidelines [18], Additional file 1: Table S1. The protocol of this systematic review was registered with PROSPERO, CRD42018112161, in November 2018. The protocol paper was published in JMIR Research Protocols in 2021 [19]. Ethics approval was not required as the present investigation was not a primary study involving participants.
A comprehensive search strategy was first developed by a research team comprising experts in paediatric dentistry, epidemiology, biostatistics, and librarian studies. There was no limit to the language of publication. Although all the studies were performed in South Africa, the studies were all published in English. The first and last authors (FKD and TR) independently conducted a pilot study to test the strategy, following which the authors confirmed the final search strategy. Peer-reviewed articles were searched in the following databases until the end of November 2020, MEDLINE; ERIC via EBSCOhost; Scopus; CINAHL via EBSCO (1900 to present); Dentistry and Oral Sciences Sources via EBSCOhost; Academic Search Complete via EBSCOhost; E-Journals via EBSCOhost; Health Source: Nursing Academic Edition via EBSCOhost and Cochrane Library. Using the key terms: (a) "early childhood caries" OR "caries" OR "decay" OR "dmft" OR "dental" OR "oral" OR "PUFA" (b) "prevalence" and (c) "children" OR "peri-natal" OR "paediatric" OR "pediatric" OR "neonatal" OR "infant" and (d) "South Africa". The keywords were used in the following combinations: a + b + c + d. Hand searching of included articles was performed. All eligible studies downloaded from the databases were uploaded into Rayyan [20], where duplicates were removed.
Screening and selection criteria
Studies were included if they were conducted in South Africa; they were based on children six years and under from the general population, if they reported sufficient information on the prevalence of ECC (sample size, prevalence of disease, mean of dmft, standard deviation of dmft) (Additional file 2: Table S2). Articles were excluded if they were abstracts, commentaries, review articles, or intervention studies. Dissertations, conference proceedings, commentaries/letters and other grey literature were also excluded from this review. Cross-sectional and cohort studies were eligible for inclusion. The inclusion and exclusion of articles were performed in Rayyan [21]. Any disagreements in the screening of articles were clarified with all the authors (Additional file 2: Table S2).
Data extraction
Two authors independently screened (FKD and TR) and extracted data from the included articles into Excel. If there was any disagreement between the authors, a consensus was reached through discussion with all the authors. If possible and required, the corresponding authors were contacted to provide the additional or missing information. In instances where articles failed to reflect the data collection date and were too old, or the authors could not be contacted, a consensus was reached among the present study’s authors to impute a suitable missing year of data collection; usually, 3–5 years before the study was published.
The following information was extracted from each eligible study: author, year of publication, study design, location and period, sampling technique, sample size, number of cases, diagnostic criteria, type of examiners, number decayed, missing, and filled teeth (dmft). Where possible, each category was sub-grouped according to the year of publication, age, urban/rural area, and Province. If it was unclear whether the area was urban or rural, the information was designated to an “urban/rural” category.
Critical appraisal
The studies’ quality was assessed by two independent authors (FK and TR) using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Studies Reporting Prevalence Data [22, 23]. The specific JBI Critical Appraisal tool contained nine explicit criteria, and a maximum score of nine indicated the lowest risk of bias, Table 1. The process was repeated twice by the same authors. Any inconsistencies which arose between the two authors were resolved by consulting with the remaining authors. Two independent authors (FK and TR) judged the scoring, and a final decision was reached by consensus with all the authors.
Data synthesis
Meta-analyses were conducted using StataCorp. 2019. STATA Statistical Software: Release 17, College Station, TX: StataCorp LLC. The pooled estimates and 95% confidence intervals for each indicator were calculated by combining each study’s data. Q-test and I2-statistical analysis were used to determine statistical heterogeneity. A random-effects model was adopted because of significant heterogeneity (I2 > 50%); Subgroup analysis was conducted to explore possible factors, including urban and rural status, age distribution and Province.
To reflect ECC’s spatial distribution, pooled prevalence estimates for ECC in all children under six years in each Province during 1975–2014 were entered into the QGIS software 3.8.3 (2019) to form a prevalence map.
Patient and public involvement statement
Neither patients nor the public was involved in the design, conduct, reporting, or dissemination of research plans.
Results
Search and selection results
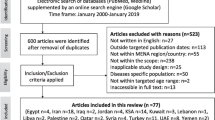
A total of 2441 publications were identified in the search strategy, and a further seven were identified through other sources. After 194 articles were removed due to duplication, 2254 articles were analysed.
After reading the titles and abstracts of the remaining articles, 2201 were excluded, and two authors independently evaluated the remaining 53 full-text articles for eligibility. After the full-text analysis, 24 were excluded because they did not meet the inclusion criteria, and 29 were included in the meta-analysis (Fig. 1, Table 2). Thus, the total sample size was 29,477 individuals. The characteristics of the 29 studies are summarised in Table 1. Sixteen articles had information on the dmft score, and 26 had information on prevalence. The overall prevalence was 44.94% (Table 3), and the overall dmft score was 2.422 (Table 4). Of these, 28 studies used diagnostic criteria established by the World Health Organization (WHO) Oral Basic Surveys Methods 2,3 and 4. In 12 studies, dentists examined the participants (Table 5). Characteristics of included studies can be found in Table 5.

Flow chart of literature search and selection
Prevalence of ECC in South Africa
The pooled overall prevalence of ECC was 44.94% (95% C.I. 39.73–50.15%). The prevalence for 4- and 5- year-olds were reported in 14 studies. ECC’s overall prevalence ranged from 57.37% between 1975 and 1979 to 61.75% between 2010 and 2014, indicating a U-shaped trend over time. The rural prevalence was higher than the urban prevalence of ECC.
The overall prevalence of dental caries by Province is illustrated in Fig. 2. The prevalence of dental caries decreased from 1975 to 1994 but showed an increase from 1995 to the present, Table 1.

Spatial Distribution of ECC prevalence and dmft scores in South Africa
The dmft per Province was 3.850, 3.000, 2.370, 2.442 and 0.330 in Eastern Cape, Kwazulu Natal, Western Cape, Gauteng, and Limpopo Provinces, respectively (Fig. 3).

Prevalence of ECC in South Africa by Year
Publication bias
Funnel plots and Begg’s test assessed potential publication bias; the result was significant if p ≤ 0.05.
Duval and Tweedie’s "Trim and Fill" method was used to assess publication bias for the prevalence and dmft scores. Under the random-effects model, the point estimate for prevalence and 95% confidence interval for the pooled was 45.7% (44.8–46.7%). Using Trim and Fill, the imputed point estimate was the same. The method suggests a total of 0 studies missing from this review for the prevalence estimate.
In addition, there were no missing studies for the dmft score as the pooled point estimate was 2.307 (2.236–2.378) and using Trim and Fill, these values remain unchanged. Egger's test results were significant for both dmft, p < 0.001 (Fig. 4) and prevalence, p = 0.0031 (Fig. 5). These results suggest that there was publication bias.

Publication bias dmft score

Publication bias prevalence estimate
Discussion
Summary of main findings
The oral and dental health of individuals are essential to general health, and even more so in children. The current investigation is the first systematic review on the prevalence and severity of ECC in South Africa. The results summarise the last 30 years of prevalence studies among children under 71 months in South Africa.
Agreements and disagreements with previous studies
The meta-analyses of the observational data collected from the eligible studies in the current study have provided a summary estimate of ECC’s prevalence in South Africa. The overall pooled prevalence of ECC was 44.94% and 51.72% for 5-year-old children. The figures are much lower than other middle to upper-income countries, including Albania, 84.0% [73], American Samoa 87.0% [74], Argentina, 80.4% [75], and Turkey, 70.5% [76]. However, they are much higher than that of Namibia [77], which has a prevalence of 31.69%.
The prevalence of dental caries increased as age increased. This corroboratesthe findings from a systematic review of the prevalence of early childhood caries in China [78]. Caries prevalence seems to have decreased from the 1970’s till the early 1990’s, Table 1. Thereafter, the prevalence of caries in children under 6 appears to increase over time. After 1994, the South African government aimed to improve the living standards by providing the poor with housing rather than providing the poor with higher incomes [79]. There was thus an increase in housing and infrastructure but, no change in employment [79]. Furthermore, there has also been an increase in urbanisation. The majority of the population in South Africa is Black, and under the apartheid regime, they were restricted in their mobility [ability to move to urban areas for work]. After the apartheid laws were revoked in June 1991 there was an increase in mobility towards the cities. Post-Apartheid urbanisation has resulted in greater access to sugar and junk food compared to rural areas [80]. This may have resulted in the higher caries prevalence noted post-apartheid.
Of interest was the declining trend in the prevalence of caries prevalence as one moved to the north of the country. The National Children's Oral Health Survey, 2001–2002, indicated that the Limpopo Province had the lowest rate of dental caries in children: 31.30% of 4–5-year-olds and 30.80% in 6-year-old children [9]. The Limpopo Province is one of the poorest regions of South Africa, with a large disparity between poor and affluent residents, especially in the rural areas [81]. Limpopo Province is an arid land, and 75.00% of the population is dependent on groundwater. The Limpopo and North-West provinces have been identified as having high fluoride levels, up to 30 mg/l [82] and they also present with the lowest prevalence of dental caries at 37.36% and 41.02%, respectively.
A challenge or limitation of the current review is that most of the studies were conducted in the Western Cape and Gauteng Provinces. The authors strongly suggest that examiners are thoroughly trained and that test–retest validity is conducted in all future prevalence studies in South Africa. It would also be favourable that a single tool (standardised) be used to examine dental prevalence. The choice of dental disease tool should be based on the exact outcome of the study performed. While the dmft score is sufficient for a dental prevalence and severity study, pulpal involvement, ulceration, fistula and abscess (pufa) score is better suited to determine the severity of clinical outcomes related to the dental treatment needs of the study under investigation.
Caution should be exercised when evaluating the current study results as there is a high heterogeneity among the included studies; this is not uncommon when evaluating systematic reviews of this nature.
Availability of data and materials
The datasets generated and/or analysed during the current study are available from the kikapu repository, https://doi.org/10.25379/uwc.14873340.v1.
Abbreviations
- ECC:
-
Early childhood caries
- NCDs:
-
Non communicable diseases
- dmft:
-
decayed, missing, and filled teeth
- JBI:
-
Joanna Briggs Institute
- MOOSE:
-
Meta-analysis of Observational Studies in Epidemiology
References
Valm AM. The structure of dental plaque microbial communities in the transition from health to dental caries and periodontal disease. J Mol Biol. 2019;431(16):2957–69. https://doi.org/10.1016/j.jmb.2019.05.016.
Jain M, Namdev R, Bodh M, Dutta S, Singhal P, Kumar A. Social and behavioral determinants for early childhood caries among preschool children in India. J Dent Res Dent Clin Dent Prospects. 2015;9(2):115–20. https://doi.org/10.15171/joddd.2014.023.
Ferreira MC, Ramos-Jorge ML, Marques LS, Ferreira FO. Dental caries and quality of life of preschool children: discriminant validity of the ECOHIS. Braz Oral Res. 2017. https://doi.org/10.1590/1807-3107bor-2017.vol31.0024.
Council R. Policy on early childhood caries (ECC): classifications, consequences, and preventive strategies. Am Acad Pediatr Dent. 2016;40(6):59–61.
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet (London, England). 2018;392(10159):1789–858. https://doi.org/10.1016/S0140-6736(18)32279-7.
Al-Jewair TS, Leake JL. The prevalence and risks of early childhood caries (ECC) in Toronto, Canada. J Contemp Dent Pract. 2010;11(5):1–8. https://doi.org/10.1016/j.jgyn.2007.10.005.
Chen KJ, Gao SS, Duangthip D, Lo ECM. Prevalence of early childhood caries among 5-year-old children: a systematic review. J Investig Clin Dent. 2019. https://doi.org/10.1111/jicd.12376.
El Nadeef MAI, Hassab H, Al-Hosani E. National survey of the oral health of 5-year-old children in the United Arab Emirates. East Mediterr Health J. 2010;16(1):51–5.
van Wyk PJ, Louw AJ, du Plessis JB. Caries status and treatment needs in South Africa: report of the 1999–2002 National Children’s Oral Health Survey. SADJ J S Afr Dent Assoc. 2004;59(6):238.
Smit D, Barrie RB, Louw AJ. The burden of dental caries in the Western Cape and a recommended turn-around strategy. S Afr Dent J. 2017;72(8):360–5.
Alkhtib A, Ghanim A, Temple-smith M, Messer LB, Pirotta M, Morgan M. Prevalence of early childhood caries and enamel defects in four and five-year old Qatari preschool children. BMC Oral Health. 2016. https://doi.org/10.1186/s12903-016-0267-z.
Zhou Y, Lin H, Lo E, Wong M. Risk indicators for early childhood caries in 2-year-old children in southern China. Aust Dent J. 2011;56:33–9. https://doi.org/10.1111/j.1834-7819.2010.01280.x.
Azizi Z. The prevalence of dental caries in primary dentition in 4- to 5-year-old preschool children in Northern Palestine. Int J Dent. 2014;2014:1–5. https://doi.org/10.1155/2014/839419.
STATSSA. Mid-year population statistics 2020. 2020. http://www.statssa.gov.za/publications/P0302/P03022020.pdf. Accessed 14 Oct 2020.
The World Bank. Gini index (World Bank estimate)—South Africa. 2020. https://data.worldbank.org/indicator/SI.POV.GINI?locations=ZA&most_recent_value_desc=false. Accessed 11 Nov 2020.
Investopaedia. Gini index. https://www.investopedia.com/terms/g/gini-index.asp. Accessed 14 Nov 2020.
Celeste RK, Fritzell J, Nadanovsky P. The relationship between levels of income inequality and dental caries and periodontal diseases. Cad Saude Publica. 2011;27(6):1111–20. https://doi.org/10.1590/s0102-311x2011000600008.
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. 2000;283:2008–12.
Kimmie-Dhansay F, Barrie R, Naidoo S, Roberts TS. Prevalence of early childhood caries in South Africa: protocol for a systematic review. JMIR Res Protoc. 2021;10(8):e25795. https://doi.org/10.2196/25795. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8371478/.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016. https://doi.org/10.1186/s13643-016-0384-4.
Booyens SJ, van Rooy HK, van der Merwe CA. Caries experience and treatment needs of five-year-old caucasian nursery school children in Pretoria. J Dent Assoc S Afr. 1991;46(4):213–6.
Brindle R, Wilkinson D, Harrison A, Connolly C, Cleaton-Jones P. Oral health in Hlabisa, KwaZulu/Natal–a rural school and community based survey. Int Dent J. 2000;50(1):13–20. https://doi.org/10.1111/j.1875-595x.2000.tb00541.x.
Joanna Briggs Institute. Joanna Briggs Institute critical appraisal checklist for prevalence Studies. n.d.. https://joannabriggs.org/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Prevalence_Studies2017_0.pdf. Accessed 14 Nov 2020.
Chosack A, Cleaton-Jones P, Woods A, Matejka J. Caries prevalence and severity in the primary dentition and Streptococcus mutans levels in the saliva of preschoolchildren in South Africa. Commun Dent Oral Epidemiol. 1988;16(5):289–91. https://doi.org/10.1111/j.1600-0528.1988.tb01777.x.
Chosack A, Cleaton-Jones P, Matejka J, Fatti P. Social class, parents’ education and dental caries in 3- to 5-year-old children. J Dent Assoc S Afr. 1990;45(1):5–7.
Cleaton-Jones P, Richardson BD, Sinwel R, Rantsho J, Granath L. Dental caries, sucrose intake and oral hygiene in 5-year-old South African Indian children. Caries Res. 1984;18(5):472–7. https://doi.org/10.1159/000260805.
Cleaton-Jones P, Richardson BD, McInnes PM, Fatti LP. Dental caries in South African white children aged 1–5 years. Commun Dent Oral Epidemiol. 1978;6(2):78–81. https://doi.org/10.1111/j.1600-0528.1978.tb01125.x.
Cleaton-Jones P, Richardson BD, Rantsho JM. Dental caries in rural and urban black preschoolchildren. Commun Dent Oral Epidemiol. 1978;6(3):135–8. https://doi.org/10.1111/j.1600-0528.1978.tb01137.x.
Cleaton-Jones P, Richardson BD, McInnes PM. Dental caries in coloured and Indian children aged 1–5 years. J Dent Assoc S Afr. 1981;36(2):61–4.
Cleaton-Jones PE, Hargreaves JA, Roberts G, Williams SD, Leidal TI. The dmfs and dmft of young South African children. Community Dent Oral Epidemiol. 1989;17(1):38–40. https://doi.org/10.1111/j.1600-0528.1989.tb01824.x.
Cleaton-Jones P, Williams S, Fatti P. Surveillance of primary dentition caries in Germiston, South Africa, 1981–97. Community Dent Oral Epidemiol. 2000;28(4):267–73. https://doi.org/10.1034/j.1600-0528.2000.280404.x.
Cleaton-Jones P, Williams S, Green C, Fatti P. Dental caries rates in primary teeth in 2002, and caries surveillance trends 1981–2002, in a South African city. Community Dent Health. 2008;25(2):79–83.
du Plessis JB. The effect of socio-economic status on dental caries experience in 6, 12 and 15 year-old school children in Port Elizabeth and Despatch. J Dent Assoc S Afr. 1997;52(7):483–6.
Gordon Y, Reddy J. Prevalence of dental caries, patterns of sugar consumption and oral hygiene practices in infancy in S. Africa. Community Dent Oral Epidemiol. 1985;13(6):310–4. https://doi.org/10.1111/j.1600-0528.1985.tb00462.x.
Gordon N. Oral health care for children attending a malnutrition clinic in South Africa. Int J Dent Hyg. 2007;5(3):180–6. https://doi.org/10.1111/j.1601-5037.2007.00261.x.
Granath L, Cleaton-Jones P, Fatti P, Grossman E. Correlations between caries prevalence and potential etiologic factors in large samples of 4–5-yr-old children. Community Dent Oral Epidemiol. 1991;19(5):257–60. https://doi.org/10.1111/j.1600-0528.1991.tb00162.x.
Granath L, Cleaton-Jones P, Fatti LP, Grossman ES. Prevalence of dental caries in 4- to 5-year-old children partly explained by presence of salivary mutans streptococci. J Clin Microbiol. 1993;31(1):66–70. https://doi.org/10.1128/jcm.31.1.66-70.1993.
Khan MN, Cleaton-Jones PE. Dental caries in African preschool children: social factors as disease markers. J Public Health Dent. 1998;58(1):7–11. https://doi.org/10.1111/j.1752-7325.1998.tb02984.x.
McInnes PM, Vieira E. Dental caries status of Chinese children in Johannesburg, South Africa. Community Dent Oral Epidemiol. 1979;7(3):170–3. https://doi.org/10.1111/j.1600-0528.1979.tb01209.x.
Mndzebele SL. Prevalence and causes of early childhood caries in children less than 6 years old at Tembisa Hospital, South Africa: dental public health. Afr J Phys Health Educ Recreat Dance. 2014;20(sup-1):396–408.
Mohamed N, Barnes JM. Early childhood caries and dental treatment need in low socio-economic communities in Cape Town, South Africa. Health SA SA Gesondheid. 2018;23:1039. https://doi.org/10.4102/hsag.v23i0.1039.
Mothupi KA, Nqcobo CB, Yengopal V. Prevalence of early childhood caries among preschool children in Johannesburg, South Africa. J Dent Child (Chicago, Ill). 2016;83(2):83–7.
Ntombela DE, Mndzebele SL. Parents’ influence on early childhood caries among their children at a community health centre in Gauteng Province, South Africa: public health intervention for maternal and child health. Afr J Phys Health Educ Recreat Dance. 2015;21(sup-2):50–60.
Richardson BD, Cleaton-Jones P, McInnes PM, Rantsho JM, Pieters L. Total sucrose intake and dental caries in black and white South African children of 1–6 years. Part II: dental caries and sucrose intake. J Dent Assoc S Afr. 1978;33(10):539–44.
Roberts GJ, Cleaton-Jones PE, Fatti LP, Richardson BD, Sinwel RE, Hargreaves JA, Williams S. Patterns of breast and bottle feeding and their association with dental caries in 1- to 4-year-old South African children. 1. Dental caries prevalence and experience. Community Dent Health. 1993;10(4):405–13.
Thekiso M, Yengopal V, Rudolph MJ, Bhayat A. Caries status among children in the West Rand District of Gauteng Province, South Africa. SADJ J S Afr Dent Assoc. 2012;67(7):318–20.
Toi CS, Cleaton-Jones PE, Daya NP. Mutans streptococci and other caries-associated acidogenic bacteria in five-year-old children in South Africa. Oral Microbiol Immunol. 1999;14(4):238–43. https://doi.org/10.1034/j.1399-302x.1999.140407.x.
Wanjau J, du Plessis JB. Prevalence of early childhood caries in 3- to 5-year-old children in Philadelphia district, Mpumalanga Province. SADJ J S Afr Dent Assoc. 2006;61(9):390–4.
Williams SD, Cleaton-Jones PE, Richardson BD, Smith C. Dental caries and dental treatment in the primary dentition in an industrialized South African community. Community Dent Oral Epidemiol. 1985;13(3):173–5. https://doi.org/10.1111/j.1600-0528.1985.tb00437.xz.
Richardson BD, Rantsho JM. Caries and dental hygiene. S Afr Med J. 1976;50(40):1536.
MacKeown JM, Cleaton-Jones PE, Fatti P. Caries and micronutrient intake among urban South African children: a cohort study. Commun Dent Oral Epidemiol. 2003;31(3):213–20. https://doi.org/10.1034/j.1600-0528.2003.00042.x.
Matejka J, Sinwell R, Cleaton-Jones P, Williams S, Hargreaves JA, Fatti LP, Docrat M. Dental caries at five and twelve years in a South African Indian community: a longitudinal study. Int J Epidemiol. 1989;18(2):423–6. https://doi.org/10.1093/ije/18.2.423.
Solanki GC, Myburgh N, Moola MH. Dental caries in black preschool children in Cape Town. Community Dent Oral Epidemiol. 1991;19(3):178–9. https://doi.org/10.1111/j.1600-0528.1991.tb00138.x.
MacIntyre UE, du Plessis JB. Dietary intakes and caries experience in children in Limpopo Province, South Africa. SADJ J S Afr Dent Assoc. 2006;61(2):058–63.
Thema LK, Singh S. Epidemiological profile of patients utilising public oral health services in Limpopo province, South Africa. Afr J Prim Health Care Fam Med. 2017;9(1):e1–5. https://doi.org/10.4102/phcfm.v9i1.1206.
Coetzee CE, Wiltshire WA. Occlusal and oral health status of a group of 3–8-year-old South African black children. SADJ J S Afr Dent Assoc. 2000;55(5):252–8.
Rudolph MJ, Gilbert L. Oral health status, knowledge, attitude and behaviour of Riverlea Primary School children. J Dent Assoc S Afr. 1986;41(11):737–40.
van Wyk PJ, van Wyk C. Oral health in South Africa. Int Dent J. 2004;54(6 Suppl 1):373–7. https://doi.org/10.1111/j.1875-595x.2004.tb00014.x.
Roberts GJ, Cleaton-Jones PE, Fatti LP, Richardson BD, Sinwel RE, Hargreaves JA, Williams S, Lucas VS. Patterns of breast and bottle feeding and their association with dental caries in 1- to 4-year-old South African children. 2. A case control study of children with nursing caries. Community Dent Health. 1994;11(1):38–41.
du Plessis JB. Prevalence of dental caries in !Kung Bushmen of Bushmanland. J Dent Assoc S Afr. 1986;41(8):535–7.
Moola MH, Vergotine RJ. Prevalence of dental caries in preschool and primary school children in Mamre. S Afr Med J. 1988;74(7):344–6.
Jinabhai CC, Supersad V, Desai BN. Priority health problems of children in an urban community. S Afr Med J. 1983;64(24):929–33.
Postma TC, Ayo-Yusuf OA, van Wyk PJ. Socio-demographic correlates of early childhood caries prevalence and severity in a developing country–South Africa. Int Dent J. 2008;58(2):91–7. https://doi.org/10.1111/j.1875-595x.2008.tb00182.x.
Byarugaba J. The impact of urbanisation on the health, of black pre-school children in the Umtata district, Transkei, 1990. S Afr Med J. 1991;79(4):444–8.
Bernitz H, Ligthelm AJ. The prevalence of oral pathoses in a private dental practice: a 30 month survey. SADJ J S Afr Dent Assoc. 1998;53(12):531–4.
Cleaton-Jones P, Richardson BD, Sreebny LM, Fatti P, Walker AR. The relationship between the intake frequency and the total consumption of sucrose among four South African ethnic groups. ASDC J Dent Child. 1987;54(4):251–4.
van Wyk C, van Wyk PJ. Trends in dental caries prevalence, severity and unmet treatment need levels in South Africa between 1983 and 2002. SADJ J S Afr Dent Assoc. 2010;65(7):310–4.
Richardson BD, Cleaton-Jones PE, Sinwel RE, Rantsho JM. Trends in sugar intake: do these parallel changes in caries prevalence among S. African preschoolchildren? Community Dent Oral Epidemiol. 1984;12(2):140–4. https://doi.org/10.1111/j.1600-0528.1984.tb01427.x.
MacKeown JM, Faber M. Urbanisation and cariogenic food habits among 4–24-month-old black South African children in rural and urban areas. Public Health Nutr. 2002;5(6):719–26. https://doi.org/10.1079/PHN2002358.
Bajomo AS, Rudolph MJ, Ogunbodede EO. Dental caries in six, 12 and 15 year old Venda children in South Africa. East Afr Med J. 2004;81(5):236–43. https://doi.org/10.4314/eamj.v81i5.9166.
Carstens IL, Louw AJ, Kruger E. Dental status of rural school children in a sub-optimal fluoride area. J Dent Assoc S Afr. 1995;50(9):405–11.
du Plessis JB. The oral health status in Mahonisi: a community with very low levels of dental caries. SADJ J S Afr Dent Assoc. 2000;55(6):308–12.
Hysi D, Caglar E, Droboniku E, Toti C, Kuscu O. Dental caries experience among Albanian pre-school children: a national survey. Community Dent Health. 2017;34(July 2016):46–9. https://doi.org/10.1922/CDH.
Quartey J. Prevalence of early childhood caries among Head Start children in American Samoa. The 128th Annual Meeting of APHA. 2000. https://aphanew.confex.com/apha/128am/techprogram/paper_13727.htm. Accessed 14 Nov 2020.
Fernández CN, Squassi A, Bordoni N. Dental status and dental treatment demands in preschoolers from urban and underprivileged urban areas in Mendoza city, Argentina. Acta Odontol Latinoam. 2015;28(1):13–21. https://doi.org/10.1590/S1852-48342015000100002.
Ölmez S, Uzamiş M, Erdem G. Association between early childhood caries and clinical, microbiological, oral hygiene and dietary variables in rural Turkish children. Turk J Pediatr. 2003;45(3):231–6.
Thopil A. Risk factors associated with early chilhood caries: an epidemiological survey in mariental, Namibia (Issue March). 2013.
Zhang X, Yang S, Liao Z, Xu L, Li C, Zeng H, Song J, Zhang L. Prevalence and care index of early childhood caries in mainland China: evidence from epidemiological surveys during 1987–2013. Sci Rep. 2016;6:18897. https://doi.org/10.1038/srep18897.
Makgetla NS. The post-apartheid economy. Rev Afr Political Econ. 2004;31(100):263–81. https://doi.org/10.1080/0305624042000262284.
de Bruin S, Dengerink J, van Vliet J. Urbanisation as driver of food system transformation and opportunities for rural livelihoods. Food Secur. 2021. https://doi.org/10.1007/s12571-021-01182-8.
Pauw K. A profile of the limpopo province: demographics, poverty, inequality, and unemployment. AgEcon Search. 2005. https://ageconsearch.umn.edu/record/15607/. Accessed 14 Nov 2020.
Gupta AK, Ayoob S. Fluoride in drinking water: status, issues and solutions. Boca Raton: Taylor and Francis Group; 2015. p. 19.
Acknowledgements
To the late Mr Fareed Davids and Mr Eric Abrahams for their librarian skills.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
FKD, RB, TR and SN: Substantial contributions to the conception, design of the study, data acquisition, interpretation of the data, drafting the manuscript, critically revising the manuscript and final approval of the version to be published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
This project was registered with the Biomedical Science Research Ethics Committee of the University of the Western Cape, BM19/4/9. No participants consent was required or requested. Patients or the public WERE NOT involved in the design, or conduct, or reporting, or dissemination plans of our research.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
This is the completed MOOSE Checklist for Meta-analyses of Observational Studies completed for this paper.
Additional file 2:
Characteristics of included studies consisting of the raw data such author, sample size and mean and SD of dmft.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kimmie-Dhansay, F., Barrie, R., Naidoo, S. et al. Prevalence of early childhood caries in South Africa: a systematic review. BMC Oral Health 22, 32 (2022). https://doi.org/10.1186/s12903-021-01982-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-021-01982-6