
Abstract
Background
The aim of this study was to evaluate the possibility of breath testing as a method of cancer detection in patients with oral squamous cell carcinoma (OSCC).
Methods
Breath analysis was performed in 35 OSCC patients prior to surgery. In 22 patients, a subsequent breath test was carried out after surgery. Fifty healthy subjects were evaluated in the control group. Breath sampling was standardized regarding location and patient preparation. All analyses were performed using gas chromatography coupled with ion mobility spectrometry and machine learning.
Results
Differences in imaging as well as in pre- and postoperative findings of OSCC patients and healthy participants were observed. Specific volatile organic compound signatures were found in OSCC patients. Samples from patients and healthy individuals could be correctly assigned using machine learning with an average accuracy of 86–90%.
Conclusions
Breath analysis to determine OSCC in patients is promising, and the identification of patterns and the implementation of machine learning require further assessment and optimization. Larger prospective studies are required to use the full potential of machine learning to identify disease signatures in breath volatiles.
Similar content being viewed by others


Background
Approximately 354,864 new cases of oral cancer are diagnosed annually, and the number, which was associated with 177,384 deaths in 2018, is steadily increasing [1]. About 90% of oral cancers diagnosed are oral squamous cell carcinomas (OSCCs), which result in malignancies in men at least twice as often as women [2]. In Germany, the 5-year survival rate of patients diagnosed with OSCC varies between 63% (female) and 47% (male) [3]. Mortality is associated with the high recurrence rate and metastases of OSCC, and the delayed diagnosis of the disease [4, 5]. Only one-third of OSCC are discovered at an early stage (0–I) [6, 7]. Therefore, the development of tests that enhance our capacity to screen high-risk (e.g. heavy tobacco and alcohol abuse) [8] and post-therapy patients is of great interest.
Breath analysis is not burdensome to patients, and is a rapid, non-invasive and inexpensive cancer screening tool. Its use has already been determined to be a promising approach to detect and differentiate various diseases, gastrointestinal conditions, and cancer types, such as lung, breast, colorectal cancer [9,10,11,12]. In every exhaled human breath, specific volatile organic compounds (VOC) that are byproducts of normal cell metabolism can be identified. These compounds are also present in biofluids such as blood, saliva, urine and feces [13, 14]. The concentrations and types of VOCs present in the exhaled breath of cancer patients compared to healthy individuals may differ based on differences in levels of oxidative stress, which are enhanced in tumor tissues [15, 16]. Gas chromatography coupled with mass spectrometry (GC–MS) is considered the gold standard for VOC screening. However, the E-nose technique, which is based on breath analysis, has produced promising results in OSCC patients as well [17,18,19]. Schmutzhard et al. [20] showed that a significant difference between VOC data from cancer patients relative to the two control groups could be detected using proton transfer-reaction-mass spectrometry (PTR-MS). A study published by Hakim et al. [21] revealed that data produced via GC–MS could be used to detect statistically significant differences between the breath compositions of three evaluated groups (OSCC/lung cancer/control). Further, the authors were able to distinguish groups using a Nanoscale Artificial Nose. Gruber et al. [22] published a feasibility study comparing OSCC patients, benign tumor patients and healthy controls that identified three potential biomarkers of OSCC using GC–MS. Bouza et al. [23] concluded that aldehyde compounds had the capacity to function as OSCC biomarkers when detected using solid-phase micro extraction followed by GC–MS. Further, Hartwig et al. [24] published a pilot study that revealed the absence of three specific VOCs after curative surgery for OSCC when compared to a patient’s initial GC–MS spectrum, which indicated a correlation between OSCC and the specific VOCs identified.
Machine learning is a computational branch that emulates human intelligence by learning from big data, and is applied in various fields, such as finances, entertainment or biological and medical applications to detect patterns which are hard or impossible to see for the human eye [25]. During the last years, a wide range of machine learning approaches were developed for the early diagnosis of different kinds of cancer from images. These include breast cancer detection by analyzing digitized images of fine needle aspirates of breast masses [26], lung cancer prediction from computed tomography images [27, 28] and brain cancer detection using magnetic resonance imaging [29]. Recent developments even include mobile applications for the detection of skin diseases via user-provided images, which are widely applicable and easy to use [30].
The aim of this study was to evaluate breath samples before and after surgery in a larger cohort using machine learning to compare OSCC patients with healthy smokers to optimize the identification of signatures of OSCC using a recently introduced gas chromatography–ion mobility spectrometry (GC–IMS)-based method. Further, we aim to enhance the applicability of the test by improving the detection of OSCC specific IMS signals that may be used to determine a VOC signature in future studies.
Patients and methods
Study population
In this prospective controlled study we collected breath samples from 55 patients with potential OSCC, as well as 50 breath samples from healthy controls. The Ethics committee of the University formally approved the study (EA1/203/19). Written informed consent for study participation was obtained from study participants. All methods were carried out in accordance with relevant guidelines and regulations.
Patients between the age of 18 and 85 with OSCC in the oral cavity and oropharynx with surgical therapy pending were included in the study. Exclusion criteria included a diagnosis of other severe internal accompanying diseases, HIV infection and a Karnofsky performance status scale of less than 50%. All participants in the control group were required to be daily smokers, at least 18 years old and lack known malignant pre-existing conditions.
Sampling
Standardization of sampling in terms of location and patient instruction was known to be crucial from the literature and our pre-tests. Patients were instructed to fast at least 6 h before sampling and refrain from cleaning their teeth with toothpaste or mouthwash. Samples were also taken in a healthy control group under the same conditions and instructions. Patients were instructed to breathe a few times through the slightly opened mouth. Air from each participant’s breath was collected using a 5 mL Luer syringe directly from the mouth. During transport, each syringe was closed with a stopper to prevent contamination. The procedure was repeated twice. All samples were analyzed within 20 min. Additionally, two syringes filled with room air were analyzed.
If analysis within 20 min was not possible (n = 2), the sample was transferred to a single use mylar bag (QuinTron, Milwaukee, WI, USA), stored at room temperature and analyzed within 24 h [31]. During analysis we made sure that these samples did not differ significantly from the other samples. Sampling always took place the morning before surgery or panendoscopy.
Gas chromatography/ion mass spectrometry (GC/IMS)
Breath sample analysis was executed using BreathSpec® (GAS Dortmund, Germany). The device facilitated two-fold separation via GC combined with IMS to detect gaseous compounds in a mixture of analytes. VOCs were pre-separated based on their retention times via GC and detected using an IMS electrometer based on specific drift times needed to travel a fixed distance (drift tube) in a defined electric field.
Samples were injected using a 5 mL-Luer-syringe via a Luer-Lock-Adapter into the BreathSpec® (GAS Dortmund, Germany). Samples were heated to 60 °C while passing through the first transfer line and were pumped into the sample loop (40 °C). A carrier gas transported the sample gas in the loop to the GC column (60 °C). During the first separation, different VOCs pass through the GC capillary column (30 m × 0.53 mm, 0.5 μm) at various speeds due to their different retention times. Next, when passing through the second transfer line (60 °C), separated compounds consecutively are fed into the IMS ionization chamber (45 °C). The first separation reduces levels of competition between analytes for reactant ions and enhances the sensitivity of IMS detection. VOCs are softly chemical-ionized initiated by a low-radiation tritium (H3) source. The collision between fast electrons emitted from the β-radiator (H3) with an inserted reagent gas, which is followed by a cascade of reactions, generates reactant ions. This forms the so-called reaction ion peak (RIP), which represents the number of ions available. The chemical ionization of analytes by reactant ions creates specific analyte ions, as long as the affinity of the analyte to the reactant ion is greater than its affinity to water, which is typical for all heteroatom-organic compounds. Specific analyte ions travel at atmospheric pressure versus a flow of inert drift gas in the drift tube, and the resulting ion current is measured using an electrometer (drift length: 98 mm, electrical field strength: 500 V/cm). IMS measurements are extremely fast (30 ms/spectrum). The mass and geometric structure of an ion determines the drift time of each substance. Therefore, IMS can differentiate isomeric molecules.
To perform analyses, two breath samples and two room air samples were taken from each participant. One sample of the patient’s breath and one of the surrounding air was analyzed using the positive drift voltage IMS mode and one of each of the breath and air samples were assessed using the negative drift voltage mode. The total processing time for one sample was 10 min.
VOC analysis
For visualization and analysis of data, a software provided by the manufacturer was used (VOCal, Dortmund, Germany). GC separation of VOCs divided compounds based on their retention times in the capillary, which resulted in an offset feed into IMS and generated coordinates on the y-axis of the pictorial representation. IMS was used to separate compounds according to their specific drift times in an electric field, which have been displayed as coordinates on the x-axis. These data produce a two-dimensional visualization scheme. The quantification of compounds was performed down to the low parts per billion (ppb) level, and data were used to create a z-axis in the software. Signal intensity was correlated with the analyte concentration of a sample. For analysis, individual signals were marked manually, and signal intensity changes and the presence of recurring patterns were identified using tools in the software.
Machine learning
To work with the 2-dimensional images, which were produced using the manufacturer’s software, they were first transformed into integer arrays. To achieve this, the “Image module” from the Python library pillow (https://pillow.readthedocs.io/en/stable/reference/Image.html) was used to load the images. After successfully transferring the images into the Python script, they were subsequently converted to numpy arrays (https://numpy.org/), using the function “asarray”. The resulting array consists of integer values specifying the color of each pixel in RGB format (https://htmlcolorcodes.com/), so for each pixel in the original image, three color values are produced that represent its respective amount of red, green and blue. Furthermore, to assure all images were of the same size, all images were reshaped to a standard format of 200 × 200 pixels using the numpy function “resize”, since even a difference in size by one pixel could potentially influence the results. As a last step, to ensure an equal importance of each feature, the multidimensional array representing the color values was collapsed into a 1-dimensional array using the numpy function “ravel”.
To identify the best performing classifier, a number of different models were evaluated, including random forest [32], logistic regression [33], K nearest neighbors [34], and linear discriminant analysis [35]. All methods are implemented in the Python library Scikit-Learn (https://scikit-learn.org/stable/), and used with the respective recommended initial parameters. To build each model, depending on the comparison in question, the images were separated into the two categories of “true” and “false” respectively. To train and evaluate the performance of each model, the data was split into training and test set. The training set was used as input for the machine learning model, while the test set was hold back so it remained completely unknown to the machine learning model. After finishing the training, each image in the test set was then predicted by the machine learning model to be “true” or “false” and it was assessed if the model did the correct prediction. The prediction accuracy of each model was analyzed multiple times with varying sizes of training and test set. Initially, a tenfold cross-validation was performed [36], where the data set is split into 10 equally sized parts. Each of the 10 subsets is then used once as test set, with the remaining 9 parts being the training set for this specific case.
Additionally, the recall was evaluated using the leave-one-out methodology [37]. In this case, the test set consists only of a single data sample, while all remaining samples were used as a training set to build the model. Here, each image was used once as a test sample and therefore left out while training the model. Subsequently, the left-out test sample was predicted and the prediction was determined to be either true or false.
Results
Manual VOC evaluation
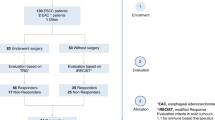
The study population consisted of 55 patients with suspected OSCC before surgery and 50 healthy control subjects. After applying exclusion criteria, some patients could not be included in the final data analysis (Fig. 1).

CONSORT flow diagram
The preoperative analysis consisted of 35 patients (24 men and 11 women) with an average age of 67.2 years. According to their medical history, 21 participants were smokers (60%), four were former smokers, ten were non-smokers (28.6%) (Tables 1 and 2).
Postoperative sampling was carried out in 22 patients (some were lost during follow-up, Fig. 1). Breath samples were taken approximately 12 days after surgery. The control group included 50 healthy smokers (25 men and 25 women), with an average age of 55 years.
To compare the occurrence of different VOC areas in the population and between preoperative and postoperative patients, signals in the visual representation that corresponded to substances in analyzed air were manually marked in all measurements. Data from one patient were placed in chronological order and compared using marked signal areas. It was revealed that certain substances occurred in almost all patients (areas 1, 2, 5, 9), while others appeared regularly, but not in every sample. Others were found very sporadically (areas 6, 12, 14, 17, 20) and some areas were exclusively present in pre- or postoperative samples (areas 24, 25). (Fig. 2, Table 3). Some areas were overlapped by VOCs of disinfectants (e.g. ethanol) and were therefore excluded from further analysis.

Comparison of pre- and postoperative measurements. The heat map shows 25 areas of interest revealed using 44 measurements of 22 patients before and after surgery in negative drift mode. Certain VOCs are present in all samples (areas 1, 2, 5, 9), and display different signal intensity (concentration), others are inconsistently observed (e.g. areas 6, 12, 14, 17, 20), and some VOCs are present in exclusively pre- or postoperative samples (e.g. areas 24 and 25)
Signal intensity changes were also assessed. Many signals differed in intensity depending on whether the analysis was preoperative or postoperative, and an increased intensity was associated with an elevated concentration of the respective substance in a sample. In general, signals detected within postoperative samples tended to be elevated relative to preoperative samples. A comparison of OSCC patients and the control group showed that the number and intensity of signals in healthy participants was elevated relative to OSCC patients (Fig. 3). In some cases, the precise evaluation of the control group was difficult due to the presence of overlap between strongly pronounced signals.

Comparison of preoperative OSCC patients with healthy controls. The heat map shows 25 areas of interest in 10 patients with OSCC (a), 10 healthy controls (c) and correlations with the room air of OSCC patients (b) in positive drift mode. Area 6 is significantly more pronounced in OSCC patients than room air, therefore, the endogenous origin of analytes can be assumed and may be associated with OSCC. In contrast, the signal observed in Area 8 is significantly increased in room air samples, an external origin of analytes is likely. The greatest signal intensity within Area 13 was observed for samples taken from the healthy control group
Machine learning
In the tenfold cross-validation process, pre- and postoperative samples in positive drift mode could only be distinguished with a highest average accuracy of 0.65 (Fig. 4a). For samples in negative drift mode, however, a highest average accuracy of 0.89 was obtained (Fig. 4b). Additionally, differentiating between preoperative tumor samples and healthy smoker samples using positive and negative drift mode could be done with a highest average accuracy of 0.90 and 0.86, respectively (Fig. 4c, d).

Comparison of the prediction accuracy of different machine learning models using tenfold cross-validation. a Pre- and post-operative samples in positive drift mode, b pre- and post-operative samples in negative drift mode, c pre-operative tumor samples and healthy smokers in positive drift mode, d pre-operative tumor samples and healthy smokers in negative drift mode are compared. LR logistic regression, LDA linear discriminant analysis, KNN k-nearest neighbors, DT decision tree, GNB gaussian naive bayes, SVM support vector machine, RF random forest
The estimated accuracy of the models was further confirmed using leave-one-out cross-validation, where logistic regression was determined to be the best performing method overall. For pre- and postoperative samples assessed in positive drift mode, 35 of 61 images (57%) were classified correctly (Additional file 1: Table S1). For samples assessed using negative drift mode this ratio improved to 43 of 58 (74%, Additional file 1: Table S2). Samples collected from preoperative tumor patients and healthy smokers were better differentiated. In samples assessed using positive drift mode, 60 of 72 samples (83%) were classified correctly (Additional file 1: Table S3), and in negative drift mode, 61 of 72 (85%) were predicted correctly (Additional file 1: Table S4). Additionally, we created sub-groups matching patients with either T1/2 (18 of 23) or T3/4 (28 of 33) tumors, female or male patients (16 of 35) and smoker or non-smoker (24/31) resulting in lower accuracies.
Discussion and conclusion
This study showed that sampling exhaled air from the oral cavity using disposable syringes and subsequent processing is possible by following a standardized protocol. This eliminates the time-consuming intermediate step of storing samples before analyzing that has been used frequently to date [9, 38]. Sampling was a quick procedure that was easy to carry out and to learn for the practitioner. Since it is a non-invasive method, patient acceptance was very high. In this study, no patient refused to participate. Data analysis, however, was more complicated and required a trained user with current knowledge of the method. The targeted, pre-selection of relevant substances and automated analysis of specific patterns is needed to make breath testing user-friendly, error-free and widely applied in the future. A critical point in the study design was to define the healthy volunteers as smokers. The design aimed to make sure that signals from smoking habits would not mislead to the conclusion that by-products, from smoking are associated with OSCC, as also low-nicotine cigarettes lead to distortions in exhaled breath [39]. As some OSCC patients were self-reported non-smokers or former smokers, a control group should have been divided into smokers and non-smokers.
Various factors significantly influence the measurement data including food supply, oral hygiene, oral flora, the existence of other severe pre-existing malignant conditions, and the composition of air within the room [40,41,42]. To minimize these factors, samples from OSCC patients were consistently taken in the morning to observe a sobriety phase of at least 6 h. In addition, patients were asked to refrain from cleaning their teeth with toothpaste or mouthwash before sampling. Other pre-existing malignant conditions were an exclusion criterion for study participation. Even with these precautions, substances were present that were believed to be caused by food and oral hygiene products. A longer fasting episode may be necessary for completely eliminating these types of by-products. Two breath samples had to be stored in Mylar bags according to a widely accepted standard and we double-checked these samples prior to analysis, but ome compounds/signals may have been not stable until GC/IMS [31, 43]. It was difficult to ensure the sobriety of participants in the control group and prevent their use of oral hygiene products. This may have explained the enhanced intensity of signals observed for the group [44]. Also, substances from inhaled room air were recognizable in breath samples. Since these were hospital rooms, specific substances such as disinfectants were present in high quantities.
A comparison between OSCC patients and healthy smokers showed that certain substances were more prevalent in OSCC patients than healthy smokers (Fig. 3). For example, area 11 was significantly more pronounced in healthy participants than OSCC patients. Since area 11 was present in the lowest quantities in room air, it seems to be an endogenous human substance, which may be reduced as a result of OSCC. The structure of the compound should be evaluated in subsequent studies. A comparison between pre- and postoperative data revealed some substances that showed similar changes, e.g. the IMS signals of areas 4, 11, 13, 15, and 16 decreased postoperatively (Fig. 2, Table 3).
Our results showed that a detailed breakdown of single substances within samples is complex, and that patient compliance with detailed instructions is extremely important. The identification of purely endogenous substances associated with OSCC is difficult [45]. An increased intensity of signals in postoperative samples may be explained by worsened oral hygiene after surgery as a result of intraoral wounds [46].
Machine learning was able to distinguish between the OSCC patients and healthy volunteers. With an increased amount of data, the differentiation between pre- and postoperative patients might be possible as well to find out signals that may be emitted exclusively by tumor tissues. This is supported by the encouraging tenfold cross-validation result for samples in negative drift mode, where an average accuracy of 0.89 could be attained. This accuracy needs to be further evaluated with a larger patient cohort. In a larger cohort, a sub-group analysis of different tumor sizes, sex and smoking status will be interesting as well. Furthermore, it has to be noted, that the models are currently optimized to achieve an optimal overall accuracy.
At this stage, the testing of high-risk patients for OSCC is not yet feasible. Further studies focussing on (1) pattern recognition using machine learning in a larger cohort and (2) in vitro studies of tumor tissues using GC/MS to find out about specific VOCs with the help of libraries [47] must be carried out. The present study showed that breath sampling using GC/IMS was user-friendly and revealed results for the determination of OSCC in breath samples using machine learning with the highest achieved average accuracy of 86–90% when compared to healthy individuals. It also showed that breath sampling remains prone to interferences by by-products, so that further studies with much larger cohorts are necessary to remove interferences before going on with the development of an e-Nose that may be usable for early detection of OSCC.
Availability of data and materials
The datasets used are available from the corresponding author on reasonable request.
Abbreviations
- OSCC:
-
Oral squamous cell carcinoma
- GC–IMS:
-
Gas chromatography coupled with ion mobility spectrometry
- VOC:
-
Volatile organic compounds
- GC–MS:
-
Gas chromatography coupled with mass spectrometry
- ppb:
-
Parts per billion
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
Lippman SM, Spitz M, Trizna Z, Benner SE, Hong WK. Epidemiology, biology, and chemoprevention of aerodigestive cancer. Cancer. 1994;74(9 Suppl):2719–25.
Fakhry C, Westra WH, Wang SJ, van Zante A, Zhang Y, Rettig E, Yin LX, Ryan WR, Ha PK, Wentz A, et al. The prognostic role of sex, race, and human papillomavirus in oropharyngeal and nonoropharyngeal head and neck squamous cell cancer. Cancer. 2017;123(9):1566–75.
Denaro N, Merlano MC, Russi EG. Follow-up in head and neck cancer: Do more does it mean do better? A systematic review and our proposal based on our experience. Clin Exp Otorhinolaryngol. 2016;9(4):287–97.
Gigliotti J, Madathil S, Makhoul N. Delays in oral cavity cancer. Int J Oral Maxillofac Surg. 2019;48(9):1131–7.
Jones TM, Hargrove O, Lancaster J, Fenton J, Shenoy A, Roland NJ. Waiting times during the management of head and neck tumours. J Laryngol Otol. 2002;116(4):275–9.
Pitiphat W, Diehl SR, Laskaris G, Cartsos V, Douglass CW, Zavras AI. Factors associated with delay in the diagnosis of oral cancer. J Dent Res. 2002;81(3):192–7.
Petti S. Lifestyle risk factors for oral cancer. Oral Oncol. 2009;45(4–5):340–50.
Finamore P, Scarlata S, Incalzi RA. Breath analysis in respiratory diseases: state-of-the-art and future perspectives. Expert Rev Mol Diagn. 2019;19(1):47–61.
Oakley-Girvan I, Davis SW. Breath based volatile organic compounds in the detection of breast, lung, and colorectal cancers: a systematic review. Cancer Biomark. 2017;21(1):29–39.
Rondanelli M, Perdoni F, Infantino V, Faliva MA, Peroni G, Iannello G, Nichetti M, Alalwan TA, Perna S, Cocuzza C. Volatile organic compounds as biomarkers of gastrointestinal diseases and nutritional status. J Anal Methods Chem. 2019;2019:7247802.
Saktiawati AMI, Putera DD, Setyawan A, Mahendradhata Y, van der Werf TS. Diagnosis of tuberculosis through breath test: a systematic review. EBioMedicine. 2019;46:202–14.
Chandran D, Ooi EH, Watson DI, Kholmurodova F, Jaenisch S, Yazbeck R. The use of selected ion flow tube-mass spectrometry technology to identify breath volatile organic compounds for the detection of head and neck squamous cell carcinoma: a pilot study. Medicina (Kaunas). 2019;55(6):306.
Amann A, Costello Bde L, Miekisch W, Schubert J, Buszewski B, Pleil J, Ratcliffe N, Risby T. The human volatilome: volatile organic compounds (VOCs) in exhaled breath, skin emanations, urine, feces and saliva. J Breath Res. 2014;8(3):034001.
Halliwell B. Oxidative stress and cancer: have we moved forward? Biochem J. 2007;401(1):1–11.
Buljubasic F, Buchbauer G. The scent of human diseases: a review on specific volatile organic compounds as diagnostic biomarkers. Flavour Fragr J. 2015;30(1):5–25.
Leunis N, Boumans ML, Kremer B, Din S, Stobberingh E, Kessels AG, Kross KW. Application of an electronic nose in the diagnosis of head and neck cancer. Laryngoscope. 2014;124(6):1377–81.
van de Goor R, Hardy JCA, van Hooren MRA, Kremer B, Kross KW. Detecting recurrent head and neck cancer using electronic nose technology: a feasibility study. Head Neck. 2019;41(9):2983–90.
van Hooren MR, Leunis N, Brandsma DS, Dingemans AC, Kremer B, Kross KW. Differentiating head and neck carcinoma from lung carcinoma with an electronic nose: a proof of concept study. Eur Arch Otorhinolaryngol. 2016;273(11):3897–903.
Schmutzhard J, Rieder J, Deibl M, Schwentner IM, Schmid S, Lirk P, Abraham I, Gunkel AR. Pilot study: volatile organic compounds as a diagnostic marker for head and neck tumors. Head Neck. 2008;30(6):743–9.
Hakim M, Billan S, Tisch U, Peng G, Dvrokind I, Marom O, Abdah-Bortnyak R, Kuten A, Haick H. Diagnosis of head-and-neck cancer from exhaled breath. Br J Cancer. 2011;104(10):1649–55.
Gruber M, Tisch U, Jeries R, Amal H, Hakim M, Ronen O, Marshak T, Zimmerman D, Israel O, Amiga E, et al. Analysis of exhaled breath for diagnosing head and neck squamous cell carcinoma: a feasibility study. Br J Cancer. 2014;111(4):790–8.
Bouza M, Gonzalez-Soto J, Pereiro R, de Vicente JC, Sanz-Medel A. Exhaled breath and oral cavity VOCs as potential biomarkers in oral cancer patients. J Breath Res. 2017;11(1):016015.
Hartwig S, Raguse JD, Pfitzner D, Preissner R, Paris S, Preissner S. Volatile organic compounds in the breath of oral squamous cell carcinoma patients: a pilot study. Otolaryngol Head Neck Surg. 2017;157(6):981–7.
Bi Q, Goodman KE, Kaminsky J, Lessler J. What is machine learning? A primer for the epidemiologist. Am J Epidemiol. 2019;188(12):2222–39.
Turkki R, Byckhov D, Lundin M, Isola J, Nordling S, Kovanen PE, Verrill C, von Smitten K, Joensuu H, Lundin J, et al. Breast cancer outcome prediction with tumour tissue images and machine learning. Breast Cancer Res Treat. 2019;177(1):41–52.
Ardila D, Kiraly AP, Bharadwaj S, Choi B, Reicher JJ, Peng L, Tse D, Etemadi M, Ye W, Corrado G, et al. End-to-end lung cancer screening with three-dimensional deep learning on low-dose chest computed tomography. Nat Med. 2019;25(6):954–61.
Thawani R, McLane M, Beig N, Ghose S, Prasanna P, Velcheti V, Madabhushi A. Radiomics and radiogenomics in lung cancer: a review for the clinician. Lung Cancer. 2018;115:34–41.
Brunese L, Mercaldo F, Reginelli A, Santone A. An ensemble learning approach for brain cancer detection exploiting radiomic features. Comput Methods Programs Biomed. 2020;185:105134.
Pangti R, Mathur J, Chouhan V, Kumar S, Rajput L, Shah S, Gupta A, Dixit A, Dholakia D, Gupta S, et al. A machine learning-based, decision support, mobile phone application for diagnosis of common dermatological diseases. J Eur Acad Dermatol Venereol. 2021;35(2):536–45.
Le HV, Sivret EC, Parcsi G, Stuetz RM. Impact of storage conditions on the stability of volatile sulfur compounds in sampling bags. J Environ Qual. 2015;44(5):1523–9.
Svetnik V, Liaw A, Tong C, Culberson JC, Sheridan RP, Feuston BP. Random forest: a classification and regression tool for compound classification and QSAR modeling. J Chem Inf Comput Sci. 2003;43(6):1947–58.
Wright RE. Logistic regression. In: Grimm LG, Yarnold PR, editors. Reading and understanding multivariate statistics. Washington: American Psychological Association; 1995. p. 217–44.
Zhang Z. Introduction to machine learning: k-nearest neighbors. Ann Transl Med. 2016;4(11):218.
Izenman AJ. Linear discriminant analysis. In: Izenman AJ, editor. Modern multivariate statistical techniques: regression, classification, and manifold learning. New York: Springer; 2008. p. 237–80.
Geisser S. The predictive sample reuse method with applications. J Am Stat Assoc. 1975;70(350):320–8.
Stone M. Cross-validatory choice and assessment of statistical predictions. J R Stat Soc Ser B (Methodol). 1974;36(2):111–47.
Kim YH, Kim KH. Experimental approach to assess sorptive loss properties of volatile organic compounds in the sampling bag system. J Sep Sci. 2012;35(21):2914–21.
Pauwels C, Hintzen KFH, Talhout R, Cremers H, Pennings JLA, Smolinska A, Opperhuizen A, Van Schooten FJ, Boots AW. Smoking regular and low-nicotine cigarettes results in comparable levels of volatile organic compounds in blood and exhaled breath. J Breath Res. 2020;15(1):016010.
Krilaviciute A, Leja M, Kopp-Schneider A, Barash O, Khatib S, Amal H, Broza YY, Polaka I, Parshutin S, Rudule A, et al. Associations of diet and lifestyle factors with common volatile organic compounds in exhaled breath of average-risk individuals. J Breath Res. 2019;13(2):026006.
Blanchet L, Smolinska A, Baranska A, Tigchelaar E, Swertz M, Zhernakova A, Dallinga JW, Wijmenga C, van Schooten FJ. Factors that influence the volatile organic compound content in human breath. J Breath Res. 2017;11(1):016013.
Phillips M, Herrera J, Krishnan S, Zain M, Greenberg J, Cataneo RN. Variation in volatile organic compounds in the breath of normal humans. J Chromatogr B Biomed Sci Appl. 1999;729(1–2):75–88.
Le H, Sivret EC, Parcsi G, Stuetz RM. Stability of volatile sulfur compounds (VSCs) in sampling bags—impact of temperature. Water Sci Technol. 2013;68(8):1880–7.
Beauchamp J. Inhaled today, not gone tomorrow: pharmacokinetics and environmental exposure of volatiles in exhaled breath. J Breath Res. 2011;5(3):037103.
Pleil JD, Stiegel MA, Risby TH. Clinical breath analysis: discriminating between human endogenous compounds and exogenous (environmental) chemical confounders. J Breath Res. 2013;7(1):017107.
Ratiu IA, Ligor T, Bocos-Bintintan V, Szeliga J, Machala K, Jackowski M, Buszewski B. GC-MS application in determination of volatile profiles emitted by infected and uninfected human tissue. J Breath Res. 2019;13(2):026003.
Lemfack MC, Gohlke BO, Toguem SMT, Preissner S, Piechulla B, Preissner R. mVOC 2.0: a database of microbial volatiles. Nucleic Acids Res. 2018;46(D1):D1261–5.
Acknowledgements
The authors would like to thank Dr. Anna Voge for her help in patient recruitment.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work was funded by the German Research Foundation (DFG: PR 1562/1-1).
Author information
Authors and Affiliations
Contributions
SM was involved in breath sampling, breath analysis, later analyzed and interpreted data, wrote the first version of the manuscript, designed Figures. KG analyzed and interpreted data, developed machine learning approach. OW was involved in breath sampling, preliminary breath analysis. RP was involved in interpretation of the machine learning data. SN analyzed and interpreted data. MH analyzed and interpreted data. SP conceived the study, performed the analysis, wrote the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethical Review Committee of Charité − University Medicine Berlin approved the retrospective analysis of our patient data (EA1/203/19). Written informed consent for study participation was obtained from study participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Tables S1–4 provide details of the machine learning results.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mentel, S., Gallo, K., Wagendorf, O. et al. Prediction of oral squamous cell carcinoma based on machine learning of breath samples: a prospective controlled study. BMC Oral Health 21, 500 (2021). https://doi.org/10.1186/s12903-021-01862-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-021-01862-z