
Abstract
Background
Sugar-sweetened drinks (SSDs) are known to be cariogenic, but this association has not been well investigated in population-based repeated cross-sectional studies in recent years. Therefore, this study examined whether SSD intake is associated with higher caries experience in 10- and 15-year-olds.
Methods
The study sample included participants from the Munich study centre of two birth cohorts with data on non-cavitated caries lesions (NCCL/S), caries experience (DMF/S index), overall caries burden (DMF + NCCL/S) and SSD intake. In total, 915 and 996 children were included from the 10- and 15-year follow-ups, respectively. Intake (g/day) of SSDs, comprising cola, lemonade, ice-tea, sport/energy drinks, fruit squashes and nectars, was calculated from food frequency questionnaires. For analyses, the SSD intake was converted into portions (250 ml/day). Multiple logistic regression and prospective analysis models were performed to test associations between SSD intake and various definitions of caries, adjusting for sex, parental education, body mass index (BMI) categories, study cohort, plaque-affected sextants, mode of SSD consumption, energy content of SSDs, and total energy intake.
Results
The mean overall caries burden at 10 and 15 years of age was 1.81 (SD: 2.71) and 6.04 (SD: 8.13), respectively. The average consumption of SSDs at the 10- and 15-year follow-ups was 0.48 (SD: 0.85) and 0.83 (SD 1.40) portions/day, respectively. After adjusting for confounders, in 10-year-olds, SSD intake was significantly associated with higher caries experience based on the indices DMF/S (adjusted odds ratio: 1.29; 95% CI: 1.06–1.57), NCCL/S (1.24; 1.03–1.49) and DMF + NCCL/S (1.27; 1.05–1.55). At the 15-year follow-up, SSD consumption was significantly associated with increased DMF/S index (1.12; 1.01–1.25) only. Prospective model associating 10-year SSD intake with 15-year caries experience was not significant.
Conclusions
SSD intake significantly increases the caries burden in 10-year-olds, with attenuated effects in 15-year-olds. To prevent caries, SSD consumption should be reduced, especially in children and adolescents.
Similar content being viewed by others


Background
Dental caries remain among the most prevalent oral diseases in children and adolescents [1]. The aetiology of caries is multi-factorial [2]; among these factors, sugar intake is associated with an increased risk of caries [3, 4]. Fermentable dietary sugars constitute bacteria’s primary energy source, which then produce acids, such as lactic acid, which lowers the pH and leads to demineralization of the dental hard tissue [2]. Therefore, a diet rich in mono- and disaccharides might be a relevant caries risk factor. Previously, it was believed that sticky foods such as chocolates, cookies and cakes have a strong tendency of getting lodged into the pits and fissures of the teeth, thus increasing the risk of the development of caries [5]; however, the influence of sugar in liquid form might be increasingly impactful and has thus far not been fully considered. Along with current lifestyle changes, the consumption of sugar-sweetened drinks (SSDs) seems to have increased [6,7,8]. In addition to the excessive sugar load, these beverages are acidic in nature, which instantly reduces the oral pH. Although this effect can be initially neutralized by the buffering capacity of saliva [9], caries development may increase with greater frequency and extent of SSD exposure. However, it could be observed that individuals, particularly growing children, are replacing drinking water with SSDs. Such long-term exposure to SSDs is detrimental to dental health and poses a potential risk of the development of caries. Although clinical studies suggest a causal relationship between SSDs and caries, confirmatory evidence through population-based studies is scarce [10]. Some larger studies have been performed in children of younger ages [11, 12], but longitudinal evidence from population-based studies in adolescents is rare. Adolescence is a life stage during which dietary and other lifestyle changes begin to appear [13]. Therefore, this study aimed to analyse the association of SSD consumption on the caries experience of adolescents at 10- and 15-year follow-ups, adjusting for the relevant confounders. The tested null hypothesis was that SSD intake does not affect caries experience at both follow-up time points.
Methods
The study protocols of the two birth cohorts were approved by the regional ethics committee, and written consent for the physical and dental examinations was obtained from all participating children and their guardians. The recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies were applied for reporting [14].
Study population
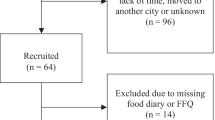
The study sample was derived from two German prospective birth cohorts German Infant Nutritional Intervention programme plus (GINIplus) and Lifestyle-related factors, Immune System and the development of Allergies in East and West Germany plus (LISAplus). The present study used a cross-sectional design performed at two time points, when the same participants were followed-up at 10 and 15 years of age. Children born in the Munich centre who had available dental examination data and dietary information were included in this study. Details concerning the study’s background, representative recruitment strategy, inclusion and exclusion criteria have been described elsewhere [15,16,17]. In this study, a total of 915 (GINIplus: 557; LISAplus: 358) and 996 (GINIplus: 652; LISAplus: 344) participants were included from the 10- and 15-year follow-ups, respectively.
Questionnaire
Before examinations at the study centre, a structured questionnaire and a food frequency questionnaire (FFQ) were sent to the subjects through post. Information on food intake over the past 12 months was obtained at each follow-up. The FFQs were filled predominantly by the parents at 10-year follow-up, and by the subjects with the help of parent at 15-year follow-up [18]. After quality control, the collected data were classified into 17 major food groups or 41 subgroups. Intake in g/day was calculated from the reported frequency of intake and estimated portion sizes Details on the quality control procedure and grouping can be found in a previously published article [18]. The SSD subgroup included colas, lemonades, ice-tea, sport/energy drinks, fruit squashes and nectars. For analysis purposes, SSD intake was converted into portions of 250 ml per day. In addition to SSD intake, parental education, defined as the highest level of either maternal or paternal education, was obtained from questionnaire administered to the parents.
Clinical examination
On the day of clinical examination, study nurses welcomed the subjects and recorded their body weight (kg) and body height (cm). Following this, dental examination was performed by calibrated dentists at both the 10- and 15-year follow-ups [15, 17]. In brief, the oral cavity was illuminated using a halogen lamp (Ri-Magic, Rudolf Riester GmbH, Jungingen, Germany). The surfaces of the teeth were dried with cotton rolls to improve visibility. Caries experience was measured at both surface and tooth level using the DMF/S index according to WHO standards [19]. Non-cavitated carious lesions (NCCL/S) only in the permanent dentition were scored using criteria defined by the International Caries Detection and Assessment System (ICDAS) [20]. Using these indices, overall caries burden (DMF + NCCL/S) was calculated. Furthermore, the extent of plaque was measured visually, and binary decisions were made for each sextant for the presence of plaque. The number of plaque-affected sextants was summed from 0 (no sextant affected) to 6 (all sextants affected).
Statistical analyses
All analyses were performed using R, version 3.3.2 (R Core Team 2016, Vienna, Austria). The intake of SSDs in portions of 250 ml per day among patients 10 and 15 years of age was defined as the exposure variable. The outcome variables were recoded binomially per surface, indicating if caries was present (0: healthy; 1: caries) at the 10- and 15-year follow-ups according to three indices: 1) DMF/S, 2) NCCL/S, and 3) DMF + NCCL/S. Parental education was classified into high (> 10 years), medium (=10 years) or low (< 10 years). Body mass index (BMI) was defined as weight in kilograms divided by height in meters squared. Following the recommendations of the working group on obesity in children and adolescents [21, 22], we classified BMI according to German age- and sex-specific percentile cut-offs for 10 and 15 year olds: (severely) underweight (<3rd percentile), normal weight (≥10th to <90th percentile); and overweight/obese (≥90th percentile). Although Kromeyer-Hauschild et al. classified BMI among children and adolescents into 5 categories, we merged them into 3 groups as the prevalence of severely underweight (<3rd percentile) and obese (>97th percentile) participants were very low in our study sample. The mode of SSD consumption was classified as not consumed, consumed with food, consumed exclusively without food, or consumed in a combination of with and without food. The energy content of SSDs was defined as diet/light/zero, normal or mixed (combination of diet/light/zero and normal). The total energy intake (kcal/day) was calculated as a continuous variable for each individual.
Simple and multiple logistic regression models were performed cross-sectionally at the 10- and 15-year follow-ups (N = 915 and N = 996, respectively), to assess the association between SSD intake and the various outcome variables. All models were adjusted for sex, parental education, age−/sex-standardized BMI categories, study cohort, plaque-affected sextants, mode of SSD consumption, energy content of SSDs, and total energy intake. As a part of sensitivity analysis, a prospective analysis was performed in which SSD intake at the 10-year follow-up was regressed on caries presence at the 15-year follow-up on all the subjects present in both follow-ups (N = 487). In addition to the previously adjusted covariates, prospective models were additionally adjusted for caries experience under the corresponding definition at 10 years of age. All the participants were around the same age during each follow-up; therefore, there was no variance accounted for by this variable, and the models were not adjusted for age. The adjusted odds ratios (aORs), their corresponding 95% confidence intervals (95% CIs), and p-values were calculated.
Results
The mean age of the participants was 10.2 years (SD: 0.2) and 15.3 years (SD: 0.3) at the 10- and 15-year follow-ups, respectively. The study had an approximately 1:1 male-to-female ratio (Table 1). Descriptively, the overall caries burden (DMF + NCCL/S) increased from 1.81 (SD: 2.71) at the 10-year follow-up to 6.04 (SD: 8.13) at the 15-year follow-up (Table 2). During the study period, the proportion of participants affected with caries increased as well: DMF/S > 0: 15.6 to 36.1%; NCCL/S > 0: 47.9 to 66.2%; and DMF + NCCL/S > 0: 53.2 to 73.3% (Table 3). Similarly, the average SSD consumption in this study increased from 0.48 (SD: 0.85; range: 0–7.66) portions per day at the 10-year follow-up to 0.83 (SD: 1.40; range: 0–15.43) portions per day at the 15-year follow-up (Table 3). Caries-affected children tended to consume marginally more SSDs per day than caries-free children. Caries were also more frequent among males than among females.
Table 4 shows the results from the multiple logistic regression analyses performed for various definitions of caries at the 10- and 15-year follow-ups and the prospective analysis, respectively. At the 10-year follow-up, SSD intake was significantly associated with higher caries experience under DMF/S (aOR: 1.24; 95% CI: (1.04–1.48)), NCCL/S (1.33 (1.13–1.58)) and DMF + NCCL/S (1.36 (1.1–1.63)) criteria. After adjusting for all the covariates, DMF/S (1.29 (1.06–1.57)), NCCL/S (1.24 (1.03–1.49)) and DMF + NCCL/S (1.27 (1.05–1.55)) remained significantly associated with SSDs. In the 15-year follow-up, only DMF/S was found to be significantly associated with SSDs both before (1.15 (1.05–1.26)) and after (1.12 (1.01–1.25)) adjusting for the covariates. In the prospective analysis, the subset of participants for whom data were available from both follow-up time points was included (N = 487). There was no significant association between 10-year SSD intake and 15-year caries experience (Additional file 1: Table S1 and S2).
Discussion
This study assessed the potential associations between SSD consumption and caries experience among children from two German birth cohorts who were followed-up at 10 and 15 years of age. An association between SSD consumption and caries experience was observed at the 10-year follow-up under DMF/S, NCCL/S and DMF + NCCL/S definitions; however, in the 15-year follow-up, the association was attenuated and significant only under DMF/S criteria.
Carbohydrates on the whole [5] or SSDs [23,24,25] are known to be linked to the development of caries. In our study, the children in the 10-year follow-up had a low overall caries burden of 1.81. A reason for this is that the caries information was obtained only from the permanent dentition. Despite this, SSD intake in 10-year olds was found to be significantly associated with increased caries experience. Some cross-sectional studies have found associations between SSDs and caries experience in the adolescent age group [26,27,28,29,30]; however, most of these studies did not include NCCL/S. Although some studies reported longitudinal associations in younger children with a follow-up time ranging between 4 and 36 months [31,32,33,34], such studies were not available in an adolescent age group.
We observed a weaker association between SSDs and caries at the 15-year follow-up. The main possible explanations for this reduced association might be underreporting of SSD consumption at 15-year follow-up and improved oral hygiene habits in this age group, such as the increased use of fluoride toothpastes and mouth rinses. It has been reported that in spite of consuming more SSDs, a decrease in caries could be observed in some industrialized nations [35], which could be credited to the use of fluorides and other preventive measures [36,37,38]. On the other hand, the prevalence of caries still remains high in some industrialized nations [39]. Fluorides might have increased the threshold of sugar consumption to an extent [37, 40]. Another factor that might have influenced this lack of association is the effect of positive sampling that might have occurred, in which the “average” population becomes more concentrated from the loss of participants on both sides of the distribution due to a lack of interest or compliance in the research setting. Some participants might have exhibited the “Hawthorne effect”, i.e., reducing the intake of SSD consumption to fare well during the study period; alternatively, some might have underreported their SSD consumption. Although fewer participants in this study consumed a higher number of portions of SSDs, it could be seen that the caries experience was high among this population sample, which indicates a dose-response relationship, as observed in other studies [10,11,12]. We cannot completely rule out that a minor proportion of well-made tooth-coloured restorations might have gone undetected in the 15-year follow-up.
The main strength of the present exploratory study is that we assessed a sample size of over 900 children at both follow-up time points, ages 10 and 15 years. Our study benefitted from extensive dental data in terms of surface-level caries information and sextant-level plaque data; general health estimators, such as parental education and BMI; and dietary intake through validated FFQs. We identified some commonly observed covariates and adjusted the models for these factors. The mode of SSD consumption, the energy content of SSDs, or the total energy intake were included in the models to further reduce the influence of confounders; the inclusions of these variables did not nullify the observed associations. Considering the low proportion of remaining primary teeth in 10-year follow-up, we did not include dmf/s as one of the outcomes in our analyses. We also observed that considering only DMF/S as an index to report caries would underestimate the caries experience. In the 15-year follow-up, the mean DMF/S was only 1.24, but the mean overall caries burden was 6.04. The major component of the caries burden was contributed by the NCCL/S. Thereby; we emphasize the inclusion of NCCL/S in studies in order to estimate more accurate caries severity among populations. One main limitation we could expect in this study was the possibility of the presence of information bias, as the dietary information was obtained through questionnaires. As commonly observed in such study designs, participants may want to perform better in the study and tend to underreport some of the diet-related variables. It might be argued that adjusting for plaque-affected sextants might lead to over-adjustment and reduce the effects shown by SSDs. However, it must be noted that the extent of plaque is one of the most important aspects in the caries causal pathway, and its inclusion in the models is justified. Although the collection of dietary information in children is challenging by itself, FFQs provide a practical means of dietary assessment in large population studies, as they are associated with low participant burden and ease in data processing [41]. It might be possible that the influence of free-sugar might have influenced the results in this study; unfortunately, this information was not obtained in our study. Therefore, there might be some confounding arising from non-inclusion of this variable. However, we had adjusted for the total energy intake, which might largely counteract the effect caused by non-inclusion of free-sugar intake. Our study population was rather homogenous in terms of town of origin, age and socioeconomic status; therefore, the results from our study might not be entirely representative of children of low socioeconomic status or from other towns.
Conclusion
The results of the present study indicate a significant positive association between SSD intake and caries, especially in 10-year-olds. The SSD consumption of 15-year-olds was significantly associated with DMF/S only. On the other hand, there was no association between SSD intake among 10-year-olds and caries incidence. The consumption and frequency of SSD intake should be reduced to a minimum or ideally avoided, especially in patients with any caries experience.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- aOR:
-
Adjusted odds ratio
- BMI:
-
Body mass index
- CI:
-
95% Confidence interval
- dmf/ DMF:
-
Decayed/ missed/ filled teeth or surfaces per individuum (DMF index, WHO 1997)
- FFQ:
-
Food frequency questionnaire
- GINIplus:
-
German Infant Nutritional Intervention programme plus study
- ICDAS:
-
International Caries Detection and Assessment System
- LISAplus:
-
Lifestyle-related factors, Immune System and the development of Allergies in East and West Germany plus Study
- NCCL:
-
Non-cavitated caries lesions
- OR:
-
Odds ratio
- SD:
-
Standard deviation
- SSDs:
-
Sugar-sweetened drinks
References
Petersen PE. The world Oral health report 2003: continuous improvement of oral health in the 21st century--the approach of the WHO global Oral health Programme. Community Dent Oral Epidemiol. 2003;31:3–23.
Marsh PD. Microbial ecology of dental plaque and its significance in health and disease. Adv Dent Res. 1994;8:263–71.
Ruottinen S, Karjalainen S, Pienihäkkinen K, Lagström H, Niinikoski H, Salminen M, Rönnemaa T, Simell O. Sucrose intake since infancy and dental health in 10-year-old children. Caries Res. 2004;38:142–8.
Sheiham A, James WP. Diet and dental caries: the pivotal role of free sugars reemphasized. J Dent Res. 2015;94:1341–7.
Gustafsson BE, Quensel CE, Lanke LS, Lundqvist C, Grahnen H, Bonow BE, Krasse B. The Vipeholm dental caries study; the effect of different levels of carbohydrate intake on caries activity in 436 individuals observed for five years. Acta Odontol Scand. 1954;11:232–64.
Han E, Powell LM. Consumption patterns of sugar sweetened beverages in the United States. J Acad Nutr Diet. 2013;113:43–53.
Bleich SN, Wang YC, Wang Y, Gortmaker SL. Increasing consumption of sugar-sweetened beverages among US adults: 1988-1994 to 1999-2004. Am J Clin Nutr. 2009;89:372–81.
Wang YC, Bleich SN, Gortmaker SL. Increasing caloric contribution from sugar-sweetened beverages and 100% fruit juices among US children and adolescents, 1988-2004. Pediatrics. 2008;121:e1604–14.
Bardow A, Lagerlöf F, Nauntofte B, Tenuvuo J: Dental caries. The disease and its clinical management. In Dental caries. 2 edn. Fejerskov O, Kidd EAM. Oxford: Blackwell Publishing Ltd.; 2008: 189–208.
Burt BA, Kolker JL, Sandretto AM, Yuan Y, Sohn W, Ismail AI. Dietary patterns related to caries in a low-income adult population. Caries Res. 2006;40:473–80.
Levy SM, Warren JJ, Broffitt B, Hillis SL, Kanellis MJ. Fluoride, beverages and dental caries in the primary dentition. Caries Res. 2003;37:157–65.
Marshall TA, Levy SM, Broffitt B, Warren JJ, Eichenberger-Gilmore JM, Burns TL, Stumbo PJ. Dental caries and beverage consumption in young children. Pediatrics. 2003;112:e184–e91.
Lytle LA. Nutritional issues for adolescents. J Am Diet Assoc. 2002;102:S8–S12.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12:1495–9.
Heitmüller D, Thiering E, Hoffmann U, Heinrich J, Manton D, Kühnisch J, Neumann C, Bauer CP, Heinrich-Weltzien R, Hickel R. Is there a positive relationship between molar incisor hypomineralisations and the presence of dental caries? Int J Paediatr Dent. 2013;23:116–24.
Pitchika V, Thiering E, Metz I, Rothmaier K, Willenberg A, Hickel R, Standl M, Kocher T, Heinrich J, Kühnisch J. Gingivitis and lifestyle influences on high-sensitivity C-reactive protein and interleukin 6 in adolescents. J Clin Periodontol. 2017;44:372–81.
Kühnisch J, Kabary L, Malyk Y, Rothmaier K, Metz I, Hickel R, Heinrich J, Manton D, Standl M. Relationship between caries experience and demarcated hypomineralised lesions (including MIH) in the permanent dentition of 15-year-olds. Clin Oral Investig. 2018;22:2013–9.
Harris C, Flexeder C, Thiering E, Buyken A, Berdel D, Koletzko S, Bauer CP, Brüske I, Koletzko B, Standl M. GINIplus study group: changes in dietary intake during puberty and their determinants: results from the GINIplus birth cohort study. BMC Public Health. 2015;15:841.
WHO. Oral health surveys. Basic methods. 4th ed. Geneva: World Health Organization; 1997.
Pitts N. Detection, assessment, diagnosis and monitoring of caries. Basel: Karger; 2009.
Kromeyer-Hauschild K, Wabitsch M, Kunze D, Geller F, Geiß CH, Hesse V, von Hippel A, Jaeger U, Johnsen D, Korte W, et al. Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben [Percentiles of body mass index in children and adolescents evaluated from different regional German studies] (article in German). Monatsschrift Kinderheilkunde. 2001;149:807–18.
Arbeitsgemeinschaft Adipositas im Kindes- und Jugendalter (AGA), 2009. BMI-Referenz [BMI reference], 2009. [http://www.a-g-a.de/].
Tahmassebi JF, Duggal MS, Malik-Kotru G, Curzon ME. Soft drinks and dental health: a review of the current literature. J Dent. 2006;34:2–11.
Fidler Mis N, Braegger C, Bronsky J, Campoy C, Domellöf M, Embleton ND, Hojsak I, Hulst J, Indrio F, Lapillonne A, et al. Sugar in infants, children and adolescents: a position paper of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2017;65:681–96.
Bleich SN, Vercammen KA. The negative impact of sugar-sweetened beverages on children's health: an update of the literature. BMC Obes. 2018;5:6.
Armfield JM, Spencer AJ, Roberts-Thomson KF, Plastow K. Water fluoridation and the association of sugar-sweetened beverage consumption and dental caries in Australian children. Am J Public Health. 2013;103:494–500.
Guido JA, Martinez Mier EA, Soto A, Eggertsson H, Sanders BJ, Jones JE, Weddell JA, Villanueva Cruz I. Anton de la concha JL: caries prevalence and its association with brushing habits, water availability, and the intake of sugared beverages. Int J Paediatr Dent. 2011;21:432–40.
Lee JG, Messer LB. Intake of sweet drinks and sweet treats versus reported and observed caries experience. Eur Arch Paediatr Dent. 2010;11:5–17.
Skinner J, Byun R, Blinkhorn A, Johnson G. Sugary drink consumption and dental caries in New South Wales teenagers. Aust Dent J. 2015;60:169–75.
Wilder JR, Kaste LM, Handler A, Chapple-McGruder T, Rankin KM. The association between sugar-sweetened beverages and dental caries among third-grade students in Georgia. J Public Health Dent. 2016;76:76–84.
Warren JJ, Blanchette D, Dawson DV, Marshall TA, Phipps KR, Starr D, Drake DR. Factors associated with dental caries in a group of American Indian children at age 36 months. Community Dent Oral Epidemiol. 2016;44:154–61.
Lim S, Sohn W, Burt BA, Sandretto AM, Kolker JL, Marshall TA, Ismail AI. Cariogenicity of soft drinks, milk and fruit juice in low-income african-american children: a longitudinal study. J Am Dent Assoc. 2008;139:959–67.
Watanabe M, Wang DH, Ijichi A, Shirai C, Zou Y, Kubo M, Takemoto K, Masatomi C, Ogino K. The influence of lifestyle on the incidence of dental caries among 3-year-old Japanese children. Int J Environ Res Public Health. 2014;11:12611–22.
Wigen TI, Wang NJ. Does early establishment of favorable oral health behavior influence caries experience at age 5 years? Acta Odontol Scand. 2015;73:182–7.
Zero DT, Moynihan P, Lingström P, Birkhed D. The role of dietary control. In: Fejerskov O, Kidd E, editors. Dental caries: the disease and its clinical management. 2nd ed. Oxford: Blackwell; 2008. p. 330–49.
Duggal MS, Toumba KJ, Amaechi BT, Kowash MB, Higham SM. Enamel demineralization in situ with various frequencies of carbohydrate consumption with and without fluoride toothpaste. J Dent Res. 2001;80:1721–4.
Zero DT. Sugars - the arch criminal? Caries Res. 2004;38:277–85.
Marinho VC, Higgins JP, Sheiham A, Logan S. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003:CD002278.
Petersen PE. World Health Organization global policy for improvement of oral health--world health assembly 2007. Int Dent J. 2008;58:115–21.
Moynihan PJ, Kelly SA. Effect on caries of restricting sugars intake: systematic review to inform WHO guidelines. J Dent Res. 2014;93:8–18.
Stiegler P, Sausenthaler S, Buyken AE, Rzehak P, Czech D, Linseisen J, Kroke A, Gedrich K, Robertson C, Heinrich J. A new FFQ designed to measure the intake of fatty acids and antioxidants in children. Public Health Nutr. 2010;13:38–46.
Acknowledgements
The GABA GmbH, Lörrach, Germany, supported this study by providing oral health care packages for all participating children as incentives. The authors thank all the children and their guardians who participated in this investigation, as well the GINIplus and LISAplus study groups for their on-going support.
Funding
The Munich arm of the GINIplus/LISAplus studies was primarily supported by grants from the Federal Ministry for Education, Science, Research and Technology and from Helmholtz Zentrum Munich (formerly GSF). The dental investigations were funded by grants from the German Research Foundation (Deutsche Forschungsgemeinschaft, FKZ KU-2518/1–1, KU-2518/1–2, HE-3294/7–1 and HE-3294/7–2). The funding institutions did not influence the design of the study, the collection, analysis, and interpretation of data and writing of the manuscript.
Author information
Authors and Affiliations
Contributions
ViP undertook the statistical analyses, developed the first draft and made necessary changes after the internal review of the manuscript. MS, CH and ET checked the analyses, provided critical inputs and advised at all stages of the manuscript. RH, JH and JK conceived the study, provided critical inputs and advised at all stages of the manuscript. All authors approved the final draft.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The present study protocol was approved by the ethics committee of the Bavarian Board of Physicians (No. 10090 for GINIplus and No. 12067 for LISAplus). Written consent for the physical and dental examinations was obtained from all participating children and their guardians.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Table S1.
Descriptive statistics for caries experience among 10- and 15-year-olds (prospective data) under various definitions of caries and relevant risk factors. Table S2. Crude associations between consumption of sugar-sweetened drinks (SSDs) and caries development under various definitions in the sub-sample present at both 10- and 15-year follow-ups (prospective data). SSD consumption at 10-year vs. caries experience at 10- and 15-year follow-up.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pitchika, V., Standl, M., Harris, C. et al. Association of sugar-sweetened drinks with caries in 10- and 15-year-olds. BMC Oral Health 20, 81 (2020). https://doi.org/10.1186/s12903-020-01068-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-020-01068-9