
Abstract
Background
Promoting prevalence of metabolic syndrome (MetS) in Rheumatoid arthritis (RA) patients might occur secondary to RA therapy as well as sedentary life style. However, conflicting observations have been reported on the correlation between MetS and RA. This study aimed to determine the frequency of MetS and association of its components in RA.
Methods
In this study, 500 RA patients and 500 age- and gender-matched healthy controls were enrolled. MetS was fulfilled through the International Diabetes Federation (IDF) criteria. A multivariate regression model was used to control for variables independently associated with the risk of MetS in RA patients.
Results
The prevalence of MetS was 58.8% on IDF criteria in RA patients that was higher than controls (20.4%). Higher incidence of cardiovascular disease (CVD), the familial history of CVD, hypertension, type 2 diabetes mellitus (T2DM), smoking, dyslipidemia, and higher levels of body mass index (BMI), waist circumference (WC), total cholesterol level, fasting blood sugar (FBS), triglyceride (TG) level, low-density lipoprotein (LDL) level, while lower levels of high-density lipoprotein (HDL) were associated with an increased risk of MetS in RA patients. Multivariate regression analysis indicated that age, WC, dyslipidemia, LDL, and DAS28 were independent predictors of MetS in the RA patients.
Conclusions
The prevalence of MetS is higher in RA patients. Our findings suggest an association between cardiovascular risk factors and the increased prevalence of MetS in RA patients.
Similar content being viewed by others

Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease that involves the joints and can affect most of the body’s vital organs, including the heart, kidneys, skin, and other organs [1]. Inflammation of the joints may be transient but is usually chronic and leads to joint damage [2]. Even in the general population, cardiovascular disease remains the primary cause of mortality; nevertheless, RA is associated with an approximately two-fold greater risk of acquiring cardiovascular disease (CVD) [3, 4]. Risk factors for cardiovascular disease in the patients include diabetes mellitus, hyperlipidemia, family history of cardiovascular disease, and elevated body mass index (BMI) [5]. Several studies have shown that factors associated with RA (traditional risk factors such as hypertension, dyslipidemia, diabetes mellitus, and obesity), especially inflammation, are also associated with an increased risk of cardiovascular disease in these patients [6, 7].
Metabolic syndrome (MetS) is a set of the most important risk factors for cardiovascular disease, characterized by abdominal obesity, insulin resistance, dyslipidemia, and hypertension [8]. In several studies, MetS has been seen in a large number of patients with RA [9]. Insulin resistance is one of the most important factors in increasing the incidence of cardiovascular disease in individuals with MetS [10, 11]. In addition, increasing these inflammatory markers increases the risk of atherosclerosis. Elevated blood pressure (BP), which is one of the diagnostic criteria for MetS, has a prevalence ranging from 3.8 to 73% in different populations with RA [12, 13]. Numerous factors, including inflammation, lack of physical activity, and medications, increase BP in patients with RA [14, 15]. Studies show that medications used for symptom relief in RA, including non-steroidal anti-inflammatory drugs (NSAIDs) and glucocorticoids, can increase the risk of high blood pressure. Additionally, certain disease-modifying antirheumatic drugs (DMARDs), such as leflunomide, may also contribute to elevated blood pressure, although this is not common among most other sDMARDs and bDMARDs [16, 17]. Furthermore, obesity is known as the most important factor in the pathogenesis of inflammation [18]. With increasing BMI, the level of circulating inflammatory proteins increase. All of these factors are produced by adipocytes, which play an important role in causing inflammation [19].
Due to the increasing prevalence and cardiovascular complications in patients with MetS, this disorder has become a pandemic and a global concern. Therefore, according to the results of previous studies and the importance of the relationship between MetS and RA (as two effective and consistent factors to increase the risk of cardiovascular complications), the present study was performed to investigate the frequency of MetS and its associated factors, such as Fasting blood sugar) FBS, Triglyceride (TG), total cholesterol, High-density lipoprotein (HDL), BP, waist circumference (WC), in RA patients.
Materials and methods
Study participants
Our case-control study enrolled 500 RA patients referred to the outpatient Rheumatology clinic of the Ali-Ebne-Abitaleb Hospital, Rafsanjan, Iran, who fulfilled the American College of Rheumatology (ACR) criteria [20], and 500 healthy persons matched based on age, gender and ethnicity with the patients. The healthy controls were selected from volunteers among hospital personnel and individuals accompanying patients in emergency or other hospital departments. These individuals had no clinical history of chronic inflammatory or autoimmune diseases. Also, exclusion criteria in both groups were infectious diseases, malignancy, pregnancy and breastfeeding. All individuals voluntarily sign a written consent to participate in the study, which was approved by the Ethics Committee of Rafsanjan University of Medical Sciences.
MetS diagnosis criteria
International Diabetes Federation (IDF) criteria was used to diagnose MetS. IDF defines MetS as central obesity, which is defined as a waist circumference of less than 90 cm for males and 80 cm for women, with ethnicity-specific values assumed if body mass index (BMI) is greater than 30 kg/m2 combined with any two of the following four characteristics makes a person have MetS: raised TG (≥ 150 mg/dL) or treatment specifically for this lipid abnormality; reduced HDL cholesterol (< 40 mg/dL in men, < 50 mg/dL in women); elevated blood pressure (≥ 130/85 mm Hg) or treatment specifically for this lipid abnormality; and elevated FBS (≥ 100 mg/dL) or previously identified T2DM it is known as MetS.
Clinical measurements
Systolic and diastolic BP (mmHg) were measured twice by a standard mercury sphygmomanometer after resting seated for 5 min. BP ≥ 130 mmHg for systolic pressure or ≥ 85 mmHg for diastolic pressure or current hypertension treatment was described as hypertension. WC (cm) was measured on a horizontal plane at the midpoint between the lower rib margin and the iliac crest. According to the IDF, a WC less than 80 cm suggests a reduced risk of T2DM, hypertension or coronary heart disease [21]. Weight (kg) was measured with the subjects dressed in light clothing and barefoot after overnight fasting with a standard scale. In addition, standing height measurement was conducted with a calibrated standard wall-mounted stadiometer, following the recommendations of the World Health Organization (WHO) [22]. BMI was calculated by weight (kg) divided by height squared (m2). According to the WHO criteria, BMI value ≤ 18.5 kg/m2 was considered underweight, 18.5–24.9 kg/m2 as normal, 25–29.9 kg/m2 as overweight and ≥ 30 indicated obesity [22].
Laboratory measurements
For each participant, serum concentrations of FBS, TG, total cholesterol, low-density lipoprotein (LDL) and high-density lipoprotein (HDL) were determined using the clinical biochemistry autoanalyzer (BT3000 Plus, Biotecnica Instruments SPA, Italy) via commercial reagents (Pars Azmoon, Iran), after an overnight fasting. ESR was measured using the automated kineticphotometric method by the Automatic ESR analyzer XC-A30 (Caretium Medical Instruments, China). In addition, CRP, anti-cyclic citrullinated peptide (anti-CCP), and Rheumatoid factor (RF) were measured by the nephelometric method.
Assessment of RA disease activity
RA activity was measured using the Disease Activity Score including 28 joints (DAS28). A score of DAS28 ≤ 2.6 indicates remission, ≤ 3.2 low disease activity, 3.3–5.1 moderate and > 5.1 high disease activity [23]. To evaluate functional disability, the Health Assessment Questionnaire (HAQ) was used. The HAQ score can range from 0 for no disability to 3 for greatest possible disability [24]. Also, to measure the patients’ general health a visual analogic scale (VAS) was used.
Statistical analysis
The SPSS software version 22 (SPSS, Chicago, IL, USA) was used for data analysis. The Kolmogorov–Smirnov test was applied to evaluate the normality of scale variables. The normally distributed variables were expressed as mean ± SD, and analyzed by independent sample t-test. The non-normally distributed variables were analyzed via the Mann–Whitney U test. Multivariate logistic regression analysis was conducted to measure the odds ratios (OR) and 95% confidence intervals (CI) and estimate the independence of the predictors of RA parameters associated with MetS. P values ≤ 0.05 were considered as statistically significant.
Results
Characteristics of patients and controls
The clinical presentations and demographic data of the RA patients and healthy controls are demonstrated in Table 1. Among the important specifications, hypertension was detected in 215 (43%) of RA patients and 105 (21%) healthy controls (P < 0.0001). The ESR level was higher in RA patients than controls (21.3 ± 14.9 mm/h vs.4.7 ± 2.1; P < 0.0001). History of CVD was higher in RA patients 49 (9.8%) than controls 23 (4.6%; P = 0.0019). Familial history of CVD was seen in 53 (10.6%) RA patients and 24 (4.8%) controls (P = 0.0032). BMI was higher in RA patients than controls (28.3 ± 4.9 kg/m2 vs. 24.8 ± 2.9 kg/m2, P = 0.024). WC was higher in RA patients than controls in males (106.4 ± 9.1 cm vs. 96.2 ± 7.9 cm; P < 0.001) and females (95.4 ± 8.9 cm vs. 85.6 ± 7.7 cm; P < 0.001). Total cholesterol level was higher in patients than controls (195.8 ± 41.8 mg/dl vs. 165.6 ± 38.4 mg/dl; P = 0.001). It was seen that FBS level was higher in RA patients (94.3 ± 34.2 mg/dl) than healthy controls (86.4 ± 21.8 mg/dl; P = 0.011). The TG level was higher in RA patients than controls (154.9 ± 62.5 mg/dl vs. 134.8 ± 41.3 mg/d; P = 0.048). Also, HDL level was lower in RA patients than controls. Finally, the frequency of MetS was higher in RA patients than healthy controls (294 (58.8%) vs. 102 (20.4%); P < 0.0001).
Characteristics of RA patients with and without MetS
Table 2 shows the specifications of RA patients with and without MetS based on IDF criteria to diagnose MetS. In the RA patient group, 294 subjects had MetS and 206 cases had no MetS. In patients with MetS, there were 80 (27.3%) males and 214 (72.7%) females, while in patients without MetS there was 55 (26.7%) males and 151 (73.3%) females.
Considering the RA disease severity indexes, the 28Tender Joint Count was higher significantly (P = 0.009) in patients with MetS (3.84 ± 2.58) than subjects without MetS (2.18 ± 1.7). Additionally, 28Swollen Joint Count was higher significantly (P = 0.011) in patients with MetS (2.92 ± 2.45) than cases without MetS (2.56 ± 1.63). It was seen that DAS28 score was higher significantly (P = 0.004) in patients with MetS (4.01 ± 1.88) than patients without MetS (2.75 ± 0.84).
Regarding inflammatory factors, CRP level was significantly (P = 0.001) increased in patients with MetS (36.9 ± 12.1) than patients without MetS (32.2 ± 11.1). Moreover, ESR level was significantly higher (P = 0.001) in patients with MetS (22.9 ± 13.3) than subjects without MetS (19.1 ± 12.5). RF level was higher significantly (P = 0.001) in RA patients with MetS (33.4 ± 10.2) in comparison to patients without MetS (31.6 ± 9.1). The anti-CCP level was significantly higher (P = 0.004) in RA patients with MetS (39.8 ± 12.7) compared to patients without MetS (34.8 ± 10.9).
History of CVD was higher (P = 0.014) in patients with MetS (12.5%) than RA patients without MetS (3.5%). Additionally, the familial history of CVD was seen in RA patients (13.9%) with MetS and in 12 (4.3%) RA patients without MetS (P < 0.001). Regarding the cardiovascular risk factors, hypertension was seen in 51.2% patients with MetS and in 30.03% patients without MetS (P = 0.025). T2DM was seen in 20.4% patients with MetS and in 14.0% cases without MetS (P = 0.03). WC of RA patients with MetS (109.9 ± 9.4) (IDF) in men (109.9 ± 9.4) and women (98.4 ± 8.9) were significantly higher (P = 0.004) than male (99.8 ± 8.1) and female (88.6 ± 7.7) patients without MetS. Dyslipidemia was significantly higher (P < 0.001) in patients with MetS (54.7%) than patients without MetS (25.7%). Total cholesterol level was significantly higher (P = 0.012) in RA patients with MetS (203.8 ± 52.6) than patients without MetS (191.8 ± 46.7). FBS level was significant higher (P = 0.047) in RA patients with MetS (95.7 ± 35.2) compared to those without MetS (89.8 ± 25.8). It was seen that LDL level was significantly higher (P = 0.032) in RA patients with MetS (139.7 ± 33.7) compared to those without MetS (135.9 ± 34.6). However, the HDL level was significantly lower (P = 0.034) in RA male (45.9 ± 13.4) and female (45.8 ± 12.2) patients with MetS compared to male (51.5 ± 11.9) and female (49.9 ± 13.1) patients without MetS.
Independent association of the variables with MetS in RA patients
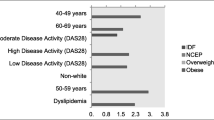
According to the multivariate regression analysis (results shown as forest plot in Fig. 1), it was revealed that the variables below were independent predictors of MetS in the RA patients; age (OR = 1.10, 95%CI: 1.04 to 1.65, P = 0.004), WC (OR = 1.87, 95%CI: 1.17 to 2.31, P = 0.014), dyslipidemia (OR = 1.93, 95%CI: 1.40 to 2.77, P = 0.003), LDL (OR = 1.65, 95%CI: 1.13 to 2.10, P = 0.019), and DAS28 (OR = 2.12, 95%CI: 1.88 to 3.23, P = 0.031).

Forrest plot to show multivariate regression model results for the variables independently associated with the risk of Mets in the RA patients
Discussion
Given the increasing prevalence of MetS and its cardiovascular complications, this study aimed to assess MetS frequency and identify risk factors in RA patients from Rafsanjan City, where previous studies indicated associations with other conditions [25,26,27]. The research provides insights into MetS characteristics and determinants in this specific region, suggesting potential targeted intervention and management strategies for individuals facing both RA and MetS.
In our study, the prevalence of MetS was 58.8% based on IDF criteria in RA patients that was higher significantly than controls (20.4%). This discrepancy in MetS prevalence among RA patients is not unique to our study, as global variations have been documented, ranging from 12.1 to 53.4%. These disparities are likely attributed to differences in population demographics and the criteria used for diagnosing patients within various regions [28,29,30]. A comprehensive meta-analysis, incorporating data from four cross-sectional controlled studies and eight case-control studies involving 2283 RA patients and 4403 controls, unveiled a significant association between RA and the risk of MetS. The overall OR calculated from this analysis was 1.24, affirming a substantial correlation between RA and the likelihood of developing MetS [28]. These findings underscore the global relevance of understanding the intricate relationship between RA and MetS, emphasizing the need for consistent diagnostic criteria and heightened awareness of this association for effective management and preventive measures across diverse populations.
A meta-analysis of 14 studies on the prevalence of MetS in Iranian healthy subjects indicated that prevalence of MetS for subjects with 20 years and older was 23.8% and in individuals with less than 20 years was 10.98%. Additionally, MetS was more frequent in women (25.5%) compared to men (17.16%) and the prevalence was increased in accordance to aging. This analysis indicated that the most frequent element of MetS was low HDL (59.7%) and then hypertriglyceridemia (39.5%) [31]. In a meta-analysis in 2019, it was detected that the overall prevalence of MetS was 30.4%. Moreover, MetS had high prevalent in women (34.8%) than men (25.7%). Additionally, and increasing trend was seen in different ages, as MetS increased from 12.1% in 20–29 years-old age group to 51.7% in the over 60 years-old age group. However, a study in 2016 in Iranian adolescents, it was revealed that the prevalence of the MetS was 10.1% among Iranian adolescents (boys: 10.3%, girls: 9.9%). This study concluded that the prevalence of MetS was high in Iranian overweight adolescents [32]. Our study also indicated that the prevalence of MetS was 20.4% based on IDF criteria in healthy individuals.
Another study is Iranian population, it was seen that prednisolone dosage, age, and Vitamin D serum levels were significant predictors of MetS occurrence in RA patients. It was shown that Vitamin D was a protective factor against MetS. It was also shown that there was a negative correlation between BMI and Vitamin D serum levels. This study indicated that Vitamin D plays a protective role against MetS in RA patients [33]. Our investigation demonstrated that history of CVD, the familial history of CVD, hypertension, T2DM, smoking, BMI, WC, dyslipidemia, total cholesterol level, FBS, TG level, LDL level was significantly higher in RA patients with MetS compared to RA patients without MetS. However, the HDL level was significantly lower in RA patients with MetS compared to those without MetS. By the multivariate regression analysis, we observed that age (OR = 1.12), WC (OR = 1.84), dyslipidemia (OR = 1.94), LDL (OR = 1.05), and DAS28 (OR = 2.10) were independent predictors of MetS in the RA patients and were associated with increased risk of MetS in these patients. It should be noted that RA is already associated with chronic systemic inflammation, and MetS adds to this inflammatory burden [34, 35]. Low HDL levels can worsen inflammation because HDL has anti-inflammatory properties. The combination of RA, MetS, and low HDL can lead to a vicious cycle where inflammation further lowers HDL, and reduced HDL fails to counteract inflammation effectively.
Our study found a significant association between elevated ESR and CRP levels and the presence of MetS in RA patients, supporting the role of chronic inflammation in developing insulin resistance. This aligns with existing literature, highlighting the association between inflammatory processes and metabolic dysregulation in RA [36]. The reciprocal relationship between inflammation and MetS suggests that chronic inflammation characteristic of RA contributes to insulin resistance and other MetS components [37]. However, the cross-sectional design of our study limits the ability to establish causality. Longitudinal studies are needed to clarify whether chronic inflammation precedes MetS development or vice versa. Future research should also explore the molecular mechanisms linking inflammation to insulin resistance in RA and MetS, which could inform targeted interventions to improve outcomes for RA patients at risk of MetS.
A bulk of investigations has assessed an association between MetS and RA activity exerting DAS28 solely [38,39,40]. Our findings are in line with these reports, through which RA patients with MetS tended to have a significantly higher DAS28 scores in comparison to those without MetS. On the other hand, a number of studies also indicated no association between presence of MetS and increased DAS28 in RA population [41,42,43,44]. A limited number of reports has focused on further indices other than DAS28, such as Simplified Disease Activity Index (SDAI), and Clinical Disease Activity Index (CDAI) to evaluated RA disease activity in subjects with MetS. These reports indicated a significant association between the presence of MetS and higher RA disease activity, represented by DAS28, SDAI, and CDAI [45, 46]. In our investigation, other than DAS28, 28Tender Joint Count and 28Swollen Joint Count were associated with the presence of MetS in RA patients. In line with these observations, we observed increased levels of RF and anti-CCP in RA cases with MetS compared to those without MetS. This suggests a potential connection between the severity of RA, as indicated by increased levels of RF and anti-CCP, and the presence of MetS. The observed correlation implies that the immunological and inflammatory components reflected by these RA disease markers may contribute to the development or exacerbation of metabolic disturbances in RA patients.
Acknowledging the limitations inherent in our current study is crucial for a nuanced interpretation of our findings. Our study’s cross-sectional design and small sample size limit the ability to establish causality and discern the sequence of events. The sample, drawn exclusively from a single tertiary care facility specializing in severe and active diseases, may overrepresent advanced disease states, affecting the generalizability of our findings. Future research with larger, more diverse cohorts and longitudinal designs is needed to better understand the relationship between rheumatoid arthritis and MetS and provide a more robust interpretation of the associations observed.
In conclusion, this study highlights the significantly elevated prevalence of MetS among RA patients compared to the healthy population, underscoring the need for targeted interventions and increased awareness. Key risk factors identified include a history of CVD, familial predisposition to CVD, hypertension, T2DM, smoking, elevated BMI, WC, dyslipidemia, total cholesterol levels, FBS, TG, and LDL levels. Reduced HDL levels were also associated with increased MetS risk. Independent predictors of MetS in RA patients were age, WC, dyslipidemia, LDL levels, and DAS28. Future research should focus on longitudinal studies with larger, more diverse cohorts to clarify causative mechanisms and validate predictors. Additionally, examining therapeutic interventions and lifestyle modifications could inform preventive strategies and optimize care. Integrating genetic factors and novel biomarkers may further advance personalized medicine and tailored treatment for this vulnerable population.
Data availability
The datasets analyzed and generated during the study are available from the corresponding author on reasonable request.
References
Khurana R, Berney SM. Clinical aspects of rheumatoid arthritis. Pathophysiology. 2005;12(3):153–65.
Ehrlich GE. Kelley’s Textbook of Rheumatology. JAMA. 2009;302(8):900–4.
Radner H, Lesperance T, Accortt NA, Solomon DH. Incidence and prevalence of cardiovascular risk factors among patients with rheumatoid arthritis, psoriasis, or psoriatic arthritis. Arthritis Care Res. 2017;69(10):1510–8.
Pujades-Rodriguez M, Duyx B, Thomas SL, Stogiannis D, Rahman A, Smeeth L, et al. Rheumatoid arthritis and incidence of twelve initial presentations of cardiovascular disease: a population record-linkage cohort study in England. PLoS ONE. 2016;11(3):e0151245.
Del Rincón I, Williams K, Stern MP, Freeman GL, Escalante A. High incidence of cardiovascular events in a rheumatoid arthritis cohort not explained by traditional cardiac risk factors. Arthritis Rheumatism: Official J Am Coll Rheumatol. 2001;44(12):2737–45.
Zhang J, Chen L, Delzell E, Muntner P, Hillegass WB, Safford MM, et al. The association between inflammatory markers, serum lipids and the risk of cardiovascular events in patients with rheumatoid arthritis. Ann Rheum Dis. 2014;73(7):1301–8.
Arts EE, Fransen J, Den Broeder AA, van Riel PL, Popa CD. Low disease activity (DAS28 ≤ 3.2) reduces the risk of first cardiovascular event in rheumatoid arthritis: a time-dependent Cox regression analysis in a large cohort study. Ann Rheum Dis. 2017;76(10):1693–9.
Mottillo S, Filion KB, Genest J, Joseph L, Pilote L, Poirier P, et al. The metabolic syndrome and cardiovascular risk: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;56(14):1113–32.
Hallajzadeh J, Safiri S, Mansournia MA, Khoramdad M, Izadi N, Almasi-Hashiani A, et al. Metabolic syndrome and its components among rheumatoid arthritis patients: a comprehensive updated systematic review and meta-analysis. PLoS ONE. 2017;12(3):e0170361.
Hanley AJ, Williams K, Stern MP, Haffner SM. Homeostasis model assessment of insulin resistance in relation to the incidence of cardiovascular disease: the San Antonio Heart Study. Diabetes Care. 2002;25(7):1177–84.
Luo P, Xu W, Ye D, Chen W, Ying J, Liu B, et al. Metabolic syndrome is Associated with an increased risk of rheumatoid arthritis: a prospective cohort study including 369,065 participants. J Rhuematol. 2024;51(4):360–7.
Banerjee S, George MD, Singh S, Tchervenkov J, Van Heusen A, Tageldin M, et al. Patient perception of Cardiovascular Risk in Rheumatoid Arthritis. ACR Open Rheumatol. 2020;2(5):255–60.
Agca R, Hopman LH, Laan KJ, van Halm VP, Peters MJ, Smulders YM, et al. Cardiovascular event risk in rheumatoid arthritis compared with type 2 diabetes: a 15-year longitudinal study. J Rhuematol. 2020;47(3):316–24.
Anyfanti P, Gkaliagkousi E, Triantafyllou A, Koletsos N, Gavriilaki E, Galanopoulou V et al. Hypertension in rheumatic diseases: prevalence, awareness, treatment, and control rates according to current hypertension guidelines. J Hum Hypertens. 2020:1–9.
Wei T, Yang B, Liu H, Xin F, Fu L. Development and validation of a nomogram to predict coronary heart disease in patients with rheumatoid arthritis in northern China. Aging. 2020;12(4):3190.
Houpt JB, Pritzker KP, Gahunia HK. Pharmacologic agents for knee articular cartilage Injury and Disease. Articular Cartilage of the Knee: Springer; 2020. pp. 253–65.
Mebrahtu TF, Morgan AW, West RM, Stewart PM, Pujades-Rodriguez M. Oral glucocorticoids and incidence of hypertension in people with chronic inflammatory diseases: a population-based cohort study. CMAJ. 2020;192(12):E295–301.
Linauskas A, Overvad K, Symmons D, Johansen MB, Stengaard-Pedersen K, de Thurah A. Body fat percentage, waist circumference, and obesity as risk factors for rheumatoid arthritis: a Danish cohort study. Arthritis Care Res. 2019;71(6):777–86.
Ouchi N, Parker JL, Lugus JJ, Walsh K. Adipokines in inflammation and metabolic disease. Nat Rev Immunol. 2011;11(2):85–97.
Britsemmer K, Ursum J, Gerritsen M, van Tuyl L, van Schaardenburg D. Validation of the 2010 ACR/EULAR classification criteria for rheumatoid arthritis: slight improvement over the 1987 ACR criteria. Ann Rheum Dis. 2011;70(8):1468–70.
Alberti KGMM, Zimmet P, Shaw J. Metabolic syndrome—a new world-wide definition. A consensus statement from the international diabetes federation. Diabet Med. 2006;23(5):469–80.
Committee WE. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:1–452.
Prevoo M, Van’ Hof T, Kuper MA, Van Leeuwen H, Van De Putte M, Van Riel L. Modified disease activity scores that include twenty-eight‐joint counts development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheumatism: Official J Am Coll Rheumatol. 1995;38(1):44–8.
Ferraz M, Oliveira LM, Araujo P, Atra E, Tugwell P. Crosscultural reliability of the physical ability dimension of the health assessment questionnaire. J Rhuematol. 1990;17(6):813.
Bagheri-Hosseinabadi Z, Moadab F, Amiri A, Abbasifard M. The prevalence and contributing risk factors of coronavirus disease 2019 infection in patients with metabolic syndrome. BMC Endocr Disorders. 2023;23(1):100.
Bagheri-Hosseinabadi Z, Khalili P, Hakimi H, Jalali N, Abbasifard M. Evaluation of the relationship between opioid addiction and metabolic syndrome and its components in the adult population from Rafsanjan city; a cohort study. Inflammopharmacology. 2022;30(6):2107–16.
Bazmandegan G, Abbasifard M, Nadimi AE, Alinejad H, Kamiab Z. Cardiovascular risk factors in diabetic patients with and without metabolic syndrome: a study based on the Rafsanjan cohort study. Sci Rep. 2023;13(1):559.
Zhang J, Fu L, Shi J, Chen X, Li Y, Ma B, et al. The risk of metabolic syndrome in patients with rheumatoid arthritis: a meta-analysis of observational studies. PLoS ONE. 2013;8(10):e78151.
de Oliveira BMGB, das, Chagas Medeiros MM, de Cerqueira JVM, de Souza Quixada RT, de Oliveira ÍMAX. Metabolic syndrome in patients with rheumatoid arthritis followed at a University Hospital in Northeastern Brazil. Revista Brasileira de Reumatologia (English Edition). 2016;56(2):117 – 25.
Chung CP, Oeser A, Solus JF, Avalos I, Gebretsadik T, Shintani A, et al. Prevalence of the metabolic syndrome is increased in rheumatoid arthritis and is associated with coronary atherosclerosis. Atherosclerosis. 2008;196(2):756–63.
Mazloomzadeh S, Khazaghi ZR, Mousavinasab N. The prevalence of metabolic syndrome in Iran: a systematic review and meta-analysis. Iran J Public Health. 2018;47(4):473.
Esmaillzadeh A, Mirmiran P, Azadbakht L, Etemadi A, Azizi F. High prevalence of the metabolic syndrome in Iranian adolescents. Obesity. 2006;14(3):377–82.
Goshayeshi L, Saber H, Sahebari M, Rezaieyazdi Z, Rafatpanah H, Esmaily H, et al. Association between metabolic syndrome, BMI, and serum vitamin D concentrations in rheumatoid arthritis. Clin Rheumatol. 2012;31(8):1197–203.
González-Gay MA, González-Juanatey C. Inflammation and lipid profile in rheumatoid arthritis: bridging an apparent paradox. BMJ Publishing Group Ltd; 2014. pp. 1281–3.
Giraud C, Tournadre A, Pereira B, Dutheil F, Soubrier M, Lhomme M, et al. Alterations of HDL particle phospholipid composition and role of inflammation in rheumatoid arthritis. J Physiol Biochem. 2019;75:453–62.
Chen L, Chen R, Wang H, Liang F. Mechanisms linking inflammation to insulin resistance. International journal of endocrinology. 2015;2015.
Nicolau J, Lequerré T, Bacquet H, Vittecoq O. Rheumatoid arthritis, insulin resistance, and diabetes. Joint Bone Spine. 2017;84(4):411–6.
Gaafar A, Aly HM, Amer A. Metabolic syndrome, hematological markers of inflammation and disease activity in rheumatoid arthritis. Int J Clin Rheumatol. 2021;16(2):052–8.
Pandey PK, Swami A, Biswas TK, Thakuria R. Prevalence of metabolic syndrome in treatment naïve rheumatoid arthritis and correlation with disease parameters. Archives Rheumatol. 2017;32(1):46.
Dao H-H, Do Q-T, Sakamoto J. Increased frequency of metabolic syndrome among Vietnamese women with early rheumatoid arthritis: a cross-sectional study. Arthritis Res Therapy. 2010;12(6):1–10.
García-Chagollán M, Hernández‐Martínez SE, Rojas‐Romero AE, Muñoz‐Valle JF, Sigala‐Arellano R, Cerpa‐Cruz S, et al. Metabolic syndrome in rheumatoid arthritis patients: relationship among its clinical components. J Clin Lab Anal. 2021;35(3):e23666.
Slimani S, Abbas A, Ammar AB, Rahal F, Khider I, Khelif K et al. Prevalence of metabolic syndrome in Algerian rheumatoid arthritis patients. Correlation with disease activity and functional status. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2017;11:S425-S7.
Kononoff A, Vuolteenaho K, Hämäläinen M, Kautiainen H, Elfving P, Savolainen E, et al. Metabolic syndrome, disease activity, and adipokines in patients with newly diagnosed inflammatory joint diseases. JCR: J Clin Rheumatol. 2021;27(8):e349–56.
Šalamon L, Morović-Vergles J, Marasović-Krstulović D, Kehler T, Šakić D, Badovinac O, et al. Differences in the prevalence and characteristics of metabolic syndrome in rheumatoid arthritis and osteoarthritis: a multicentric study. Rheumatol Int. 2015;35:2047–57.
Grzechnik K, Targońska-Stępniak B. Metabolic syndrome and rheumatoid arthritis activity: an analysis of Clinical, Laboratory, and Ultrasound parameters. Nutrients. 2023;15(22).
Gomes KWP, Luz AJP, Felipe MRB, Beltrão LA, Sampaio AXC, Rodrigues CEM. Prevalence of metabolic syndrome in rheumatoid arthritis patients from northeastern Brazil: Association with disease activity. Mod Rheumatol. 2018;28(2):258–63.
Acknowledgements
The authors are grateful of the patients and the healthy individuals for their participation in the study.
Funding
This study was financially supported by the Rafsanjan University of Medical Sciences, Rafsanjan, Iran.
Author information
Authors and Affiliations
Contributions
ZBH; Performed the statistical analysis, participated in manuscript preparation, and read the manuscript critically. FM; Contributed in statistical analysis, participated in manuscript preparation and read the manuscript critically. MA; Developed the main idea, examined the patients, participated in manuscript preparation and read the manuscript critically.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved from the local Ethical Review committee located in Rafsanjan University of Medical Sciences (IR.RUMS.REC.1399.113) and written informed consent form was taken by all subjects. All methods were carried out in accordance with relevant guidelines and regulations provided by Rafsanjan University of Medical Sciences.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Bagheri-Hosseinabadi, Z., Moadab, F. & Abbasifard, M. Prevalence and contributing factors of metabolic syndrome in rheumatoid arthritis patients. BMC Endocr Disord 24, 140 (2024). https://doi.org/10.1186/s12902-024-01675-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-024-01675-5