
Abstract
Background
Type 1 diabetes (T1D) in youth is becoming a public health problem in Sub-Saharan Africa, including Burkina Faso. However, little is known about the level of knowledge of these patients on T1D. This study aimed to evaluate the knowledge of diabetes in adolescents and young adults about the disease, and identify the factors associated in Burkina Faso.
Methods
A cross-sectional survey was conducted from April to June 2020 among youth with T1D, aged 10 to 30 years, and regularly followed in the internal medicine department of Yalgado Ouedraogo University Hospital of Ouagadougou, Burkina Faso. Data were collected using the French AJD (Aide aux Jeunes Diabétiques) validated diabetes knowledge and skills (DKS) questionnaire designed to test participants’ accuracy in knowledge about six different themes of T1D, as generalities of diabetes, hypoglycemia and hyperglycemia, management of insulin treatment, and self-monitoring blood glucose (SMBG). DKS level was determined by calculating the scores, and univariate and multivariate logistic regression were used to explore factors influencing DKS scores. This level was classified as insufficient or low ≤ 25/50, regular 26–39/50, and adequate or good ≥ 40/50.
Results
Sixty-three participants with a mean age of 19.05 years and a sex ratio (W/M) of 1.17 were included in our study. The mean HbA1c level was 9.79%, and 43 (68.23%) patients had an insufficient DKS level. The mean global DKS score of correct answers was 23.63/50. The percentage of correct answers was respectively 50% for the item “generalities of diabetes”, 32.4% for the item “hypoglycemia and hyperglycemia”, 67.72% for the item “diet”, 37.34% for the item “management of insulin treatment” and 44.97% for the item “SMBG”. In univariate analysis, a better patient DKS level was associated with university education and long duration of diabetes care follow-up (> 10 years, p < 0.05). Only increasing age remain associated with a better knowledge score (p < 0.05) in multivariate analysis.
Conclusion
This study is an important first step in identifying areas for intervention efforts about therapeutic education for youth with type I diabetes in Burkina Faso.
Similar content being viewed by others

Background
Type 1 diabetes (T1D) is the most frequently type of diabetes in youth, characterized by chronic immune-mediated destruction of pancreatic β-cells, usually leading to absolute insulin deficiency [1]. Achieving target glucose levels assessed through monitoring blood glucose levels and glycated hemoglobin is essential to minimize the detrimental effects of hypoglycemia and hyperglycemia [2]. Most of youth with T1D from sub-Saharan African do not meet recommended glycemic targets [3].
The Diabetes Control and Complications Trial and its follow-up study, the Epidemiology of Diabetes Interventions and Complications study, confirmed that an improvement in long-term glucose control by intensified insulin therapy and extensive support and education, can reduce the incidence of complications and delay the progression of existing complications in T1D, in adolescents and adults [4].
Since the implementation of the Life for a Child (LFAC) program [5] in Burkina Faso, prevalence of people with T1D < 25 years rose from 0.14/100,000 in 2013 from 1.36/100,000 by 2021 [6].
In Burkina Faso, because of limited access to insulin and high prices, most of young people with TID benefit from LFAC at the internal medicine department (the main referral center for diabetes in the country) of Yalgado Ouedraogo Teaching Hospital (CHU YO) in Ouagadougou. This program commenced an intervention to provide care for all young people < 26 years of age with diabetes in Burkina Faso in 2013, donating insulin and glucose-monitoring supplies. The internal medicine department of the CHU YO also usually follows people with T1D over the age of 25 years who previously benefit from the LFAC program. These young people followed in the CHU YO have been seen as routine visit every three or four months. They come from all regions of the country except western and south-western regions where there is another hospital with the LFAC support. As of April 1, 2020, out of 143 patients aged 25 and under were followed in Burkina Faso throughout LFAC support, 108 (75.52%) were followed at CHUYO center.
The insulin donated by LFAC was mostly premixed 70/30 insulin formulation, so patients were mainly given fixed doses. All participants routinely test their blood glucose at home two times per day but only those on multiple daily injection insulin therapy were encouraged to adjust their insulin dose at home with meals, exercise, or blood glucose readings. For those on fixed doses, they were encouraged to adjust only in case of recurrent hypoglycemia. Glycemic control in children and adolescents with T1D in this center is very poor [7].
As part of insulin treatment, achieving good glycemic target requires a comprehensive diabetes education [8]. Therapeutic patient education (TPE) allows patients to improve their knowledge and skills both on their chronic disorder and their treatment [9]. In sub Saharan Africa, TPE on diabetes is limited among children with diabetes [10]. Consultation times are short, resulting in little or no time for patient education [11].
All young people followed in the CHU YO center benefit sometimes from therapeutic education for diabetes monitoring, which had remained mainly individual during their routine visits, with a few group sessions on diet since the end of 2018. Educative tools used were those of the French educative program published as “Les Cahiers de l’AJD” (Aide aux Jeunes Diabétiques, help to young diabetics) [12].
In Africa, several studies assessed diabetes knowledge in adults’ patients with type 2 and type 1 diabetes [13,14,15,16,17,18], showing the insufficient level of knowledge (≤ 50% of correct answers through submitted questionnaires). But very few addressed to young people with T1D [19, 20]. In Burkina Faso there is only one study on this topic for type 2 diabetes (T2D) [21] but none for young people with T1D, and the TPE program conducted in the CHUYO center was still not evaluated.
To fill this gap, we aimed to assess T1D knowledge in adolescents and young adults about the disease, and identify the factors associated in the CHUYO center.
Methods
This was a single center cross-sectional survey study conducted from April 1st to June 30th, 2020. The study population included adolescents and young adults with T1D, aged 10 to 30 years, and regularly followed in the internal medicine department of CHUYO for at least one year. As diabetes autoantibodies and C-peptide assays are not available in Burkina Faso, T1D was diagnosed according to standard World Health Organization criteria [22]. Such criteria included age, presentation, the abrupt onset of symptomatic hyperglycemia, need for insulin replacement therapy from diagnosis, and no suggestion of T2D or another type of diabetes being responsible.
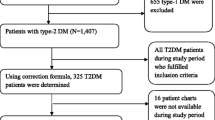
People with another type of diabetes, and those with mental ill-health were excluded. The study was performed during regular outpatient consultations or hospitalizations in this center. All consecutive patients who met the inclusion criteria and seen during the study period have been included. Among them, 6 were aged < 10 years and 9 had less than 1 year history of diabetes and were excluded to the study. All included patients were diagnosed before the age of 25years, as they were all previously followed up in our Life For A Child cohort patients.
We used the AJD (Aide aux Jeunes Diabétiques) diabetes knowledge and skills (DKS) adapted French questionnaire for children and adolescents with T1D [23]. This questionnaire is composed of 50 true-false questions designed to test participants’ accuracy in knowledge about six different themes of T1D: 6 questions on the generalities of diabetes, 12 on hypoglycemia and hyperglycemia, 9 on diet, 17 on the management of insulin treatment and 6 about self-monitoring blood glucose (SMBG). The process of developing the questionnaire was designed based on 310 true-false questions elaborated from a program aimed at initial education of T1D, “les Cahiers de l’AJD”, with the participation of 1576 10–20 years old T1D adolescents, 466 parents, 33 pediatric centers and eight AJD diabetes camps. Answers were analyzed by linkage studies (Ward’s minimum variance method) to guide the Educative Committee in selecting one-third of the questions; the 105 remaining questions were retested in a single series by 564 T1D adolescents, while a test-retest was also performed by 77 adolescents or parents, to select 67 questions, before a last test by 200 adolescents for the final selection of the 50 questions we used [23].
The AJD DKS questionnaire was completed by the patients. In case of French language obstacle, the questionnaire was administered by the interviewer (doctor) with translation of the questionnaire into the two most national languages speaking (“Dioula” and “Mooré”). It was the same interviewer for all patients. To minimize alteration of the questions, we first tested them to some patients who spoke both French and one or the other of the 2 translation languages to ensure that the understanding was the same.
Each correct answer was scored as “1” and each incorrect answer scored as “0”. We associated the choice answer option “I don’t know” to optimize the rate of correct answers. For the analysis we made a two-stage model where the first part was the variables that predict thinking that patient know the answer (yes = 1 and no = 0) to assess only the response of “I do not know”. The second part of the model was the variables that predict the answer they give conditional on thinking that they know (correct answer = 1, incorrect answer = 0).
The score of DKS was evaluated by the number of correct answers to the AJD questionnaire. The level of diabetes knowledge was empirically classified according to total number of correct answers, insufficient or low ≤ 25/50 (≤ 50% of correct answers), regular 26–39/50 (51–79%), and adequate or good ≥ 40/50 (≥ 80%).
For each patient, the consulting physician completed a file to collect the following data: date of first insulin injection, number of daily injections, times of injections (breakfast, lunch, afternoon snack, dinner, and bedtime) and types of insulin (fast-acting, long-lasting, and premixed).
Descriptive analyses are presented as mean (± SD) for quantitative variables and as frequencies and percentage for qualitative variables. Correlation analyses between DKS total score and factors included in the analysis were performed using Chi-square test (or Fisher’s test if appropriate), with a significance level of 0.05. In the multivariate analysis, we included variables that are known to affect knowledge from literature even if they may not have been significant in the univariate analysis, such are sex, age, schooling, living or not with parents, follow up duration and HbA1c. Analyses were made with the IBM SPSS Statistics 26 software, 2018.
Information collected about patients was treated confidentially.
Informed written consent from the youth included, or from their parents or guardians for young people under 18, was obtained before their inclusion in the study. We also sought assent from the children aged 10–17 yrs. The patient’s refusal to participate in this study in no way prevented his treatment and follow-up in the center. The National ethic committee (Comité d’Ethique pour la Recherche en Santé) provided the approval for the study with the registration No 2020-8-146.
Results
Sixty-three participants with a mean age of 19.05 years and a sex ratio (F/M) of 1.17 were included in our study. Female represented 53.97% of participants.
Thirty-eight (60.32%) participants had primary or intermediate school level of education and 8 (12.7%) had high school level. Fifty (78.24%) participants lived in urban areas and 40 (63.5%) lived with both their two parents. More than 20 km separated the home from the monitoring center for 33.33% of youth.
The mean age at the discovery of diabetes was 14.88 years and the circumstance of discovery was ketoacidosis in 50% of cases. The mean duration of diabetes was 3.47 ± 2.51 years. In 68.3% of cases, the duration of diabetes was less than 5years.
Fifty-three participants (84.12%) had fixed doses of insulin. After the initial hospitalization, 26 (41.27%) of patients were re-hospitalized at least once for a total of 31 acute complications, including 9 cases (34.61%) of severe hypoglycemia and 22 cases (84.61%) of ketoacidosis.
The mean HbA1c level at the last contact was 9.79% with an average insulin dose of 0.78 IU/kg/day.
Regarding the TPE, 32 patients (67%), felt well to very well educated.
DKS level
The mean global score of correct answers was 23.63/50. Forty-three (68.23%) patients had an insufficient level of knowledge on their illness and their treatment.
About the sections of the DKS questionnaire, the percentage of correct answers of each theme was respectively 50% for the item “generalities of diabetes”, 32.4% for the item “hypoglycemia and hyperglycemia”, 67.72% for the item “diet”, 37.34% for the item “management of insulin treatment” and 44.97% for the item “SMBG” (Table 1).
In univariate analysis (Table 2), a better DKS score was associated with university education and long duration (> 10 years) of follow-up (p < 0.05). There was no significant difference in score according to sex, age, urban or rural origin, parental situation, feeling of being well educated or having a good glycemic control, DKA episodes and age at T1D diagnosis (p > 0.05).
In multivariate analysis (Table 3), only age was associated with a better knowledge score (p < 0.05). There was no difference in score between patients according to their glycemic control, sex, and family status.
Discussion
With a rate of 47.26% of correct answers, the level of knowledge of adolescents and young adults with diabetes was insufficient. This level of knowledge is also found insufficient in another sub-Saharan African country like Malawi [19]. Our rate is near to the same of 48.2% found in Saoudi Arabia (63.8% of the child used insulin two times a day) [24] but less than the 86% found in one study in the USA [25]. These studies in Malawi, Saoudi Arabia and USA used the Michigan Diabetes Knowledge Test [26], which looked at general knowledge on diabetes, complications and self-care practices. We used the same questionnaire as in France where the level of knowledge is 75% [27]. The better level of DKS in these countries could be explained as their clinics usually offer comprehensive diabetes education by certified diabetes educators and a registered dietitian [23, 25, 27].
Nevertheless, in multivariate analysis, we only found age as the factor associated with the DKS. Age is also described as an associated factor in other studies [19, 27]. The study in Malawi shown association between age and DKS but regarding that 63% of participants had at least 5 years duration of diabetes, it is possible that duration powered the role of age. Other social and demographic factors associated are urban residency [28] and socioeconomic status [25]. Considering that 87.3% of our sample not having a university education and lived in urban areas, the lack of knowledge could be explained by the lack of TPE and the low level of school education.
There is a significant relationship between education level and diabetes knowledge [19, 27, 28], as we found in our study.
Glycemic control was not correlated with knowledge of diabetes as it is shown in another study in Brazil [29] where they also found a significant correlations between HbA1c and resilience, anxiety and depression. However, studies in the USA and France found that better diabetes knowledge is associated with glycemic control [25, 27], which may suggest the involvement of others factors like socioeconomic status or illness perception for example. Moreover, we think if our study was powered, some factors that have been associated with DKS score like glycemic control would have turned out significant. It was described in South Africa that adolescents with at-risk glycemic control believed that T1D is difficult to manage, leading to a largely negative perception of the disease [30].
Among the subsections of the DKS questionnaire, there was an average level of knowledge for the item “generalities” and a weak level for the other items (hypoglycemia, hyperglycemia, insulin treatment, SMBG). These findings are in agreement with the findings in Malawi [19], which contributes to poor glycemic control. As most of our patients had fixed doses of insulin and were not encouraged to adjust their insulin dose at home with meals, exercise, or blood glucose readings, this would impact their knowledge in these subsections of the DKS. It is recommended that SMBG is essential for diabetes management for all children and adolescents with diabetes and an inability to articulate symptoms of hypoglycemia impose to set higher HbA1c goal [2]. Moreover, management of insulin must be supported by comprehensive education, whatever insulin regimen is chosen [31].
There was a good knowledge for the item “diet”, which item is already found to be associated with a better diabetes knowledge in youth with T1D and their caregivers [25]. This good knowledge in our study could also be explained by the group’s education sessions focused on diet we started in the clinic since 2018.
Some limitations of this study may be sources of biases. First our study was limited to the single center of the CHU YO, not considering patients from the western and south-western regions of the country. The translation of the questionnaire from French into the national languages "Dioula” and “Mooré” for its administration to young people who did not understand French language could be the source of misunderstandings. At last, in our analysis we did not do a distinction on the origin of young people between rural and urban areas.
Nevertheless, the CHU YO being the center receiving most people T1D in the country, the results of this study could be able to guide the initiation of therapeutic education programs for the benefit of all people with T1D.
Conclusion
The DKS was insufficient. This research is an important first step in identifying a significant need to develop relevant TPE on diabetes for children, adolescents, and their parents within Burkina Faso to help them manage the condition hence averting long term complications.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AJD:
-
Aide aux Jeunes Diabétiques
- CHU YO:
-
Yalgado Ouedraogo Teaching Hospital
- DKS:
-
diabetes knowledge and skills
- HbA1c:
-
glycated hemoglobin
- LFAC:
-
Life for a Child
- T1D:
-
type 1 diabetes
- T2D:
-
type 2 diabetes
- TPE:
-
therapeutic patient education
- F/M:
-
female/male
References
Libman I, Haynes A, Lyons S, et al. Clinical practice Consensus Guidelines 2022: definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr Diabetes. 2022;23:1160–74.
De Bock M, Codner E, Craig ME, et al. Clinical practice Consensus Guidelines 2022: glycemic targets and glucose monitoring for children, adolescents, and young people with diabetes. Pediatr Diabetes. 2022;23:1270–6.
Katte JC, McDonald TJ, Sobngwi E, Jones AG. The phenotype of type 1 diabetes in sub-saharan Africa. Front Public Health. 2023;11:1014626.
The Diabetes Control and Complications Trial Research Group. Effect of intensive diabetes treatment on the development and progression of long-term complications in adolescents with insulin-dependent diabetes mellitus: Diabetes Control and Complications Trial. J Pediatr. 1994;125:177–88.
Life For A. Child. https://lifeforachild.org/ (20 May 2023, date last accessed).
Sagna Y, Bagbila WPAH, Zoungrana L, et al. P263. Incidence and prevalence of type 1 diabetes in children and young adults in Burkina Faso. Pediatr Diabetes. 2022;23:171–2.
Sagna Y, Bagbila WPAH, Bognounou R, et al. Comparison of regular with NPH insulin vs. premix insulin in children and adolescents with type 1 diabetes in a resources-limited setting: a retrospective data analysis. J Pediatr Endocrinol Metab. 2023;36:447–50.
Lindholm Olinder A, DeAbreu M, Greene S, et al. ISPAD Clinical Practice Consensus Guidelines 2022: diabetes education in children and adolescents. Pediatr Diabetes. 2022;23:1229–42.
World Health Organization. Therapeutic Patient Education: Continuing Education Programmes for Health Care Providers in the Field of Prevention of Chronic Diseases: Report of a WHO Working Group; WHO Regional Office for Europe: Geneva, Switzerland. https://apps.who.int/iris/handle/10665/108151 (23 July 2023, date last accessed).
Hapunda G, Pouwer F. Diabetes in sub-saharan african children: risks, Care, and Challenges. In: Abubakar A, Van De Vijver FJR, editors. Handbook of Applied Developmental Science in Sub-Saharan Africa. New York, NY: Springer New York; 2017. pp. 157–72.
Mbanya J-C, Ramiaya K. Diabetes Mellitus. In: Jamison DT, Feachem RG, Makgoba MW, et al. editors. Disease and Mortality in Sub-Saharan Africa. 2nd ed. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2006.
Commission Pédagogique de l’AJD. Les Cahiers de l’AJD: Education des nouveaux diabétiques. Paris; 2013.
Alaofè H, Hounkpatin WA, Djrolo F, Ehiri J, Rosales C. Knowledge, attitude, practice and associated factors among patients with type 2 diabetes in Cotonou, Southern Benin. BMC Public Health. 2021;21:339.
Mufunda E, Wikby K, Björn A, Hjelm K. Level and determinants of diabetes knowledge in patients with diabetes in Zimbabwe: a cross-sectional study. Pan Afr Med J. 2012;13:78.
Sidibe M, Sidibe AT, Traore AK, Traore FD. Niveau de connaissance des diabétiques sur leur maladie en milieu hospitalier dans un pays d’Afrique subsaharienne cas du Mali. Ann Endocrinol. 2015;76:564.
Yazidi M, Chihaoui M, Chaker F, Rjeb O, Slimane H. Factors Predicting Glycemic Control in Type 1 Diabetic patient. Open Med J. 2016;3:153–8.
Mukeshimana MM, Nkosi ZZ. Communities’ knowledge and perceptions of type two diabetes mellitus in Rwanda: a questionnaire survey. J Clin Nurs. 2014;23:541–9.
Moodley L, Rambiritch V. An assessment of the level of knowledge about diabetes mellitus among diabetic patients in a primary healthcare setting. South Afr Fam Pract. 2007;49:16–16d.
Phiri EC, Msiska G, Kululanga LI, Mbakaya BC. Patient’s Knowledge Assessment on Diabetes and SelfCare Practices among older adolescents with type 1 diabetes Mellitus in Malawi. Eur Sci J ESJ. 2017;13:429.
Okoh B, Jaja T. Knowledge and awareness of diabetes among adolescents in Port Harcourt, Nigeria. Afr J Diabetes Med. 2014;22:18–20.
Yaméogo TM, Kyelem CG, Guira O, et al. Audit of diabetes knowledge among adults with diabetes in Bobo-Dioulasso (Burkina Faso): a cross-sectional study prior to intervention strategy. Open J Intern Med. 2018;08:10–7.
World Health Organization. Definition and diagnosis of diabetes mellitus and intermediate hyperglycaemia: report of a WHO/IDF consultation. Switzerland, 2006.
Martin D, Dossier C, Godot C, et al. Questionnaire de connaissance de l’AJD pour les enfants et les adolescents ayant un diabète de type 1. Educ Thérapeutique Patient - Ther Patient Educ. 2016;8:10106.
Moawad S. Assessment of Knowledge among Saudi Diabetic Children/ adolescent at Riyadh City. Am J Nurs Sci. 2014;3:5.
Moskovitz A, Alex Knee M, Frydman E, Allen H, Tonyushkina K. Diabetes knowledge in Youth with T1DM and their Caregivers-A cross-sectional study. J Diabetes Clin Pract 2018; 1.
Fitzgerald JT, Funnell MM, Anderson RM, Nwankwo R, Stansfield RB, Piatt GA. Validation of the revised brief diabetes knowledge test (DKT2). Diabetes Educ. 2016;42:178–87.
Martin D, Elie C, Dossier C, et al. Diabetes knowledge in adolescents with type 1 diabetes and their parents and glycemic control. Pediatr Diabetes. 2017;18:559–65.
Mangla P, Chopra A, Sudhanshu S, et al. Validation of a diabetes knowledge test for indian children, adolescents and young adults with type 1 diabetes mellitus. Prim Care Diabetes. 2019;13:283–7.
Santos FRM, Bernardo V, Gabbay MAL, Dib SA, Sigulem D. The impact of knowledge about diabetes, resilience and depression on glycemic control: a cross-sectional study among adolescents and young adults with type 1 diabetes. Diabetol Metab Syndr. 2013;5:55.
Lesage S, Deacon E, Van Rensburg E, Segal D. ‘It kinda sucks’: illness perception of a group of south african adolescents with type 1 diabetes mellitus. Afr J Prim Health Care Fam Med 2021; 13.
Danne T, Phillip M, Buckingham BA, et al. ISPAD Clinical Practice Consensus Guidelines 2018: insulin treatment in children and adolescents with diabetes. Pediatr Diabetes. 2018;19:115–35.
Acknowledgements
We are thanks to the patients who participated in the study.
Funding
This study was not supported by any sources of funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, OG; validation, TMY, SAK, and OG; formal analysis, DZ, YS; investigation, DZ, DPS, ST, and YS; data curation, DZ; writing—original draft preparation, DZ; writing—review and editing, YS; supervision, TMY, SAK, and OG. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was performed in accordance with the principles of the Declaration of Helsinki. The study was approved by the National ethic committee of Burkina Faso (Comité d’Ethique pour la Recherche en Santé) and registered under the No 2020-8-146. Informed consent was obtained from all subjects and their legal guardians before inclusion in the study.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zemba, D., Sagna, Y., Traore, S. et al. Diabetes knowledge and associated factors in adolescents and young adults with type 1 diabetes in Ouagadougou (Burkina Faso). BMC Endocr Disord 23, 210 (2023). https://doi.org/10.1186/s12902-023-01469-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-023-01469-1