
Abstract
Background
Gallbladder stone diseases (GSD) is a main risk factor of gallbladder cancer (GBC). This study aimed to reveal their bridge to metabolic syndrome.
Material/method
The clinical and experimental data of 2210 GBC patients, from 3524 Chinese patients, in our hospital from Jan. 2009 to Dec. 2020 were summarized. The metabolic syndrome indexes, influencing factors for both GBC and GSD, were analyzed by unconditional logistic regression in this case–control study.
Result
There were significantly higher morbidity of GBC in the overall, GSD and non-GSD with hypertriglyceridemia patients versus non-hypertriglyceridemia ones (P < 0.001, all). In GSD patients, univariate regression showed a significantly positive correlation between serum triglyceride (TG), low density lipoprotein cholesterol (LDL-c), fasting insulin (FINS) levels, Homeostasis model assessment-insulin resistance (HOMA-IR), female being, body mass index, hypertriglyceridemia and hazard of GBC with GSD (P < 0.001, all), and a significantly negative correlation to systolic pressure (SBP), diastolic pressure (DBP), hypertension and high-density lipoprotein cholesterol (HDL-c), fasting blood glucose (FBG) (P < 0.05, all); multivariate regression showed that serum triglyceride was the most significantly positive factor associated to GBC (P < 0.001, all) among the hazard factors including serum TG, LDL-c levels, HOMA-IR. In non-GSD ones, multivariate regression showed that HOMA-IR was the most significantly positive factor associated to GBC among the hazard factors including serum TG, LDL-c levels, HOMA-IR, female being, while DM had a significantly inversion negative association (P < 0.001).
Conclusion
We found initially that elevated serum TG levels could be the most remarkable independent predicting factor for GBC risk with GSD, while insulin resistance might act as the first one in non-GSD. More importantly, we advocated initially the sharp rise of serum TG levels as the potential of a candidate diagnostic or prognostic biomarker of GBC with GSD.
Trial registration
The study may be performed in accordance with the ethical standards provided by the responsible committee of our institution (First Affiliated Hospital of Xi’an Jiaotong University. XJTU1AF2020LSK-160) at which the work was carried out an in accordance with the Declaration of Helsinki. The ethics committee of our institution strictly comply with the requirements of ICH-GCP、GCP and relevant regulations to construct, operate and implement operating procedures.
Similar content being viewed by others


Background
Gallbladder cancer, highest burden in China, is the fifth most common cancer involving the gastrointestinal tract, and its five-year survival rate is only 5%; but it is the most common malignant tumor of the biliary tract worldwide [1, 2]. Its main risk factor is prolonged exposure to gallbladder stone disease (GSD), a common gastrointestinal disease, which is prone to develop into severe cholecystitis, or even strongly associated with gallbladder, pancreatic and colorectal cancer occurrence, and the National Institutes of Health estimated that almost 3,000 deaths (0.12% of all deaths) per year were attributed to the complications of GSD [3]. The association might result from their common initial etiologic including bacterial infections and other inflammatory conditions [4]. Singh, T. D. et al. studied the promoter methylation of certain tumor associated genes in the molecular pathogenesis of GBC and GSD and revealed that downregulation of SOCS1 only occurred in GBC and methylation frequency increase of 14–3-3 sigma, MASPIN and THBS1 genes from early to advanced GBC grades; with the latter several genes showed in GSD significantly as well [5]. There exists a strong link between the burden of GSD, especially for cholesterol gallstones, and highly prevalent metabolic disorders such as obesity, dyslipidemia, type 2 diabetes, hyperinsulinemia, hypertriglyceridemia and the metabolic syndrome [6, 7], as well as GBC [8, 9].
Although a personal history of gallstones has long been found to be strongly related to GBC risk, aetiology of GBC remains poorly understood. Cholecystectomy (or some other form of gallstone therapy) is indicated in most patients with symptomatic cholelithiasis – especially those with non-functioning gallbladders. But the issues of its complications and the optimal surgical time should not be ignored [10, 11]. Besides, it might be the best choice to cut off the links between GSD and GBC. Of the above, lifestyle changes including weight loss, more exercise, prevention and treatment of hyperlipidemia and diabetes mellitus will be the most possible to be realize. People in northwestern China feed on foods with high lipid and sugar, and with the westernization of diet in recent years, epidemiological investigations reported their stronger inclination to develop metabolic syndrome such as hyperlipidemia, obesity, diabetes mellitus and non-alcoholic fatty liver disease (NAFLD). Therefore, this study recruited subjects from in this typical area, and reviewed the clinical records of patients with GBC during a 12-year period, so as to reveal the bridge relating to metabolic syndrome between GBC and GSD. It may shed light the research of the risk factors of GBC development and provide preventive approaches for further gallbladder cancer resulting from GSD.
Methods
Study population
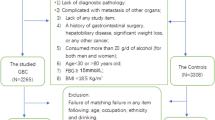
Anthropometric and laboratory parameters of 3524 Chinese GBC patients, were retrospectively reviewed at the time of preliminary diagnosis before surgery in the first Affiliated Hospital of Xi’an Jiaotong University from Jan 2009 to Dec 2020. Included criteria: 1) age 30 to 80 years old; 2) BMI ≥ 18.5 kg/m2; 3) GBC was verified by pathology; 4) underwent radical cholecystectomy in our hospital. 1259 patients were excluded because: 1) without undergone cholecystectomy and verified by pathology; 2) complicated with metastasis of other organs; 3) lack of any of the data. Then 3808 individuals who had undergone health check-ups annually in the same healthcare center were performed a complete clinical and analytical evaluation (including any item following), and choose the newest ones were chosen. Finally, 2210 patients and 2210 health controls aged 30 to 80 years, were chosen after excluding those who: 1) consumed more than 20 g/day of alcohol during the past 12 months (for both men and women) by the diagnostic standard of nonalcoholic fatty liver and the characteristics of Chinese men's drinking habits [12]; 2) BMI < 18.5 kg/m2; 3) any missing data including age, gender, height, weight, systolic pressure (SBP), diastolic pressure (DBP), serum total cholesterol (TC), triglyceride (TG), low density lipoprotein (LDL-c), high density lipoprotein (HDL-c), fasting insulin, fasting blood glucose (FBG), retinol binding protein (RBP), or ultrasonographic examination for gallbladder stones and NAFLD; 4) matching failure in any of the following item: age, ethnicity, occupation, and drinking. In additional, we conducted this study in accordance with the Institutional Ethics Committee requirements of the above-mentioned hospital (XJTU1AF2020LSK-160).
Determination of anthropometric and laboratory parameters
All study points of each GBC patients have been completed by his surgeon in charge during their stay in hospital and stored in our hospital information system. The control participants individually have completed a questionnaire and a measuring scale containing our study items which were stored in our medical information management system.
FBG was determined by the GOD/POD method; Lipid parameters: TC by the CHO/POD method, HDL-C by the AB-Wako method, TG by the GPO/POD method in the blood from the antecubital vein serum were determined in the 10-h fasting state (DiaSys, Holzheim, Germany, all). LDL-C was estimated by the Friedewald equation. Blood RBP and FINS was assayed by immunoturbidimetry or radioimmunoassay, respectively.
A color Doppler ultrasonography instrument (Toshiba, SSA-510A, Japan) was used to identify gallbladder and hepatic diseases. The subjects were fasting and in the supine position. The liver, gallbladder, pancreas and spleen were sequentially examined. GSD and NAFLD were diagnosed as previously reported [12].
Determination of diabetes, hypertension, hypertriglyceridemia and insulin resistance
Diabetes diagnosis was completed by a professional endocrinologist according to the latest China diagnostic criteria: for example, the newest diabetes patients were diagnosed by Guideline for prevention and treatment of type 2 diabetes mellitus in China 2020 [13]. Hypertension was diagnosed by cardiovascular specialist based on guidelines for pharmacological treatment of hypertension in adults published by the World Health Organization (WHO), for example, SBP ≥ 140 mmHg or DBP ≥ 90 mmHg were diagnosed as hypertension in the latest edition [14]. Homeostasis model assessment-insulin resistance (HOMA-IR) was calculated from fasting glucose and insulin. \(HOMA-IR=[FBG\left(mmol/L\right)\times FIN\left(mU/L\right)]/22.5\) [15]. TG > 1.7 mmol/L is defined as hypertriglyceridemia according to the 2018 American Humane Association/American College of Cardiology (AHA/ACC) Guideline [16].
Statistical analysis
All the data were statistically analyzed with SPSS version 19.0 software (SPSS Inc., Chicago, IL, USA) and the significance level was set at P < 0.05. Data are presented as the means ± standard deviations (SD) as the data was normally distributed. To compare variables between two groups or subgroups, Chi-square tests for categorical variables and Student’s t-test for continuous variables were used. We did our mainly analyzed the statistical significance between gender, each of the metabolic syndrome factors, and GBC hazards using multivariate logistic regression model in groups stratified by GBD.
Results
General characteristics and serum indexes in the GBC and control groups
The different characteristics in general characteristics and serum indexes between gallbladder cancer and the control group are summarized in Table 1. There were 2210 of 2265 patients with GBC and 2210 subjects of 3808 healthy controls aged 30 to 80 including 1421 (64.3%) and 1034 (46.8%) female participants in GBC and the control group respectively. There was a higher risk of GBC in Female (HR = 2.048, 95%CI: 1.816 ~ 2.311). There were significantly higher BMI, FINS, TG, LDL-c, and HOMA-IR levels and lower SBP, DBP, HDL-c and FBG levels in GSD group versus the controls, and there were the significantly higher incidences of DM, NAFLD and GSD, lower incidence of HBP (P < 0.05, respectively), see Table 1.
The effects of HTG on GBC
As shown in Table 2, the effects of HTG and GSD on hazard rate of GBC were determined. Significantly higher morbidity with GBC was found in HTG subjects than non-HTG ones in GSD (χ2 = 334.347, OR = 19.077, P < 0.001). Similar result was observed in non-GSD (χ2 = 1213.294, OR = 19.906, P < 0.001). And Table 1 revealed that HTG also had a higher GBC risk in total (χ2 = 1791.004, OR = 20.562, P < 0.001).
Relationships between the indexes of BMI, hyperlipidemia, NAFLD and hazard rate of GBC
Table 3 shows the risk factors for developing GBC stratified by GSD based on univariate and multivariate logistic regression. Univariate logistic regression showed significantly positive correlation between female being, hypertriglyceridemia, serum TG, LDL-c levels, HOMA-IR, FINS, and hazard of GBC (P < 0.05, all), while significantly negative correlation between serum HDL-c, FBG levels, SBP, DBP, HBP and hazard of GBC (P < 0.05). Of them, serum TG level was the most remarkable hazardous factor of GBC with GSD (OR = 37.784, P < 0.001). Multivariate logistic regression without HTG showed that there was significantly positive correlation between, HOMA-IR, serum TG, LDL-c and hazard of GBC (P < 0.05, all), while significantly negative correlation between serum HDL-c levels, HBP and hazard of GBC (P < 0.001, all). Of them, serum TG was the the most significantly positive association to GBC (OR = 16.912, P < 0.001). Similar results were observed by multivariate analysis including HTG. Of them, HTG was the most significantly positive association to GBC (OR = 10.636, P < 0.001).
To investigate the possible reason that caused above result, we further analyzed data stratified by non-GSD based on univariate and multivariate logistic regression analysis (as Shown in Table 4). Univariate logistic regression showed significantly positive correlation between female being, BMI, DM, HTG, NAFLD, serum TG, LDL-c levels, HOMA-IR, FINS and hazard of GBC (P < 0.05, all), and significantly negative correlation between serum HDL-c, FBG levels, SBP, HBP and hazard of GBC (P < 0.05). Multivariate logistic regression showed that there was significantly positive correlation between female being, serum TG, LDL-c, HOMA-IR levels and hazard of GBC (P < 0.05, all), and significantly negative correlation between serum HDL-c levels, DM, HBP and hazard of GBC (P < 0.05, all). Of them, HOMA-IR was the most significantly positive association to GBC with (OR = 8.739, P < 0.001).
Discussion
Epidemiological studies have identified that GSD is one of several GBC risk factors, despite epidemiologic data, definitive evidence for the role of gallstones as a cause for gallbladder cancer is lacking, GSD might associate to the elevated hazard of GBC by 2.4-fold (gallstone diameter = 2.0 ~ 2.9 cm) to 9.2–10.1-fold (gallstone > 3 cm) [17, 18]. In this clinical case–control study matched for ethnicity, occupation, and drinking conducted in northwestern China, we identified that Female, insulin resistance and hypercholesterolemia were independent risk factor of GBC predicting [8, 19]; and DM didn’t associate significantly with GBC in GSD patients as the recent report [20]. Interestingly, our study revealed initially that TG was the most remarkable independent predicting factor of GBC risk in GSD patients among metabolic/environmental factors; while HTG was in the patients without GSD.
First, our study showed that DM was not significantly correlated to GBC risk in the GSD patients, which HOMA-IR was a significant position to GBC risk in the patient without or with GSD. We tend to consider hyperinsulinemia as an independent predicting factor of GBC risk [21], while DM as a risk factor for gallbladder cancer as a result of synergistic hypertension and hyperlipidemia [20]. The recent study reported that insulin might reduce the levels of insulin growth factor binding proteins (IGFBP) 1 and IGFBP2 in the circulation, resulting in the increase of circulating insulin growth factor (IGF); the latter and insulin might stimulate target cells toward malignant transformation [22]. In additional, few study has clarified that LDL-c is associated with GBC, while it is undoubted that very low dentine lipid (VLDL) receptor has been reported to be involved in the pathogenesis of GBC by regulating the expression of the components of the fibroblast growth factor receptor signaling pathway through Mitogen-Activated Protein Kinase (MAPK) [23], while high LDL-c levels could interrupt "endogenous lipid pathway" as result of VLDL accumulation because HTG will lead to the formation of large triglyceride-rich VLDL particles due to the fact that triglycerides overproduction is disproportionately greater than increasing apoB production, especially as seen in the insulin resistant state [24].
Second, our result revealed that HTG was significant positive correlated to GBC risk in GSD patients, and elevated serum TG was an independent risk factor of GBC predicted as the most remarkable. It might be because: there are little data on the role of elevated TG-related biomarkers on gallbladder cancer risk, but HTG, relating to GSD, might decrease sensitivity to cholecystokinin, and increase both biliary cholesterol saturation and bile viscosity enhancing mucin production [25, 26], and cholesterol stones and gallbladder infections were associated with increased MUC3 and MUC5B expression [27]. Epidemiological data have revealed that gallbladder stone is considered the most important risk factor for GBC, and the large volume or high weight of gallstones could further increase the risk [28]. The synergistic effect of the gallbladder stones and infections leads to the thickening of gallbladder mucosa, which leads to the occurrence of gallbladder cancer in symptomatic GSD patients. Even so, it is known that the synthesis of TG requires glycerol and fatty acids, most of which are for glucose metabolism origin; the former is converted from dihydroxyketone phosphate produced by glycolysis; the latter is synthesized from acetyl CoA produced by oxidative decomposition of glucose. In short, continuous elevated TG might infer to accumulation of glucose or insulin resistant, with which blood glucose accumulation is transformed into TG by hepatocytes and TG is released into blood, resulting in the increase of TG concentration in blood [24]. Several prospective epidemiological studies showed that excess body weight in combination with physical inactivity is a major determinant for the development of insulin resistance with associated with hyperglycemia and hyperinsulinemia and further leads to tumor development by several biological pathways, such as chronic low-grade inflammation, glucose toxicity, advanced glycosylated end product metabolism and the adenosine monophosphate kinase pathway [21]. Clearly, elevated blood TG is the most remarkable independent predicting factor of GBC risk, possibly because elevated TG is associated with GSD [24], and other indexes of metabolic syndrome [29], yet the effect of the latter is possibly interfered constructively or destructively. Speculatively, our result, the observed persistent increase in serum TG, might be considered as the potential of a candidate diagnostic or prognostic biomarker of GBC in the patients with GSD.
Third, our study revealed that HTG is a significant predicting factor of GBC risk including in the patients without GSD, the data revealed that hypertriglyceridemia might increase the risk of prostate cancer [30], hepatocellular cancer [31], endometrial cancer [32], pancreatic cancer [33] and so on, which tended to consider the above correlation between HTG and GBC due to high secretion of bile acids, while bile acid metabolic dysfunction is a causal factor of gallstones [33, 34]. Thus, we speculate that obesity and/or insulin resistance should be the main causes in patients without GSD [35], as our multivariate logistic regression showed that HOMA-IR was the most remarkable independent predicting factor of GBC risk. There is convincing evidence that obesity may disturb lipid and endogenous hormones metabolism, result in gallbladder dysfunction, increase the risk of gallstones, and thus play a role in GBC [9, 36], while the recent study supported that obesity might be protective factor for several cancers (for example premenopausal breast cancer, non-small cell lung cancer and head and neck cancers) [35]. Undoubtedly, central accumulation of body fat is associated with insulin resistance [37], which has a role in the aetiology of biliary tract cancers (including GBC) [38]; insulin could stimulate the insulin receptor or the IGF-1R, activate their intrinsic tyrosine kinase activity, induce the production of lipid messengers by the phosphatidylinositol 3-kinase, and then trigger AKT-mammalian target of rapamycin pathway regulating cell growth and differentiation and the Ras-Raf-MEK-MAPK pathway inducing cell proliferation [39]. Moreover, insulin might upregulate the metabolic activity of the cell, producing reactive oxygen species causing DNA double strand break or mutation in vitro [40].
Strengths and limitations
We reviewed a large number of participants’ case history with more than ten years, making sure that the patients had been diagnosed by surgery and pathology in the case group and the matched participants come from the same occupation, and similar environment. However, the present study has several limitations. First, this is not a multicenter and cohort study, and statistics may be biased. Secondly, we provided little enlightenment about the cause for the negative correlation between HBP, SBP, DBP and GBC, even HBP might be an independent protective factor in our study. Maybe elevated neuropeptides vasoactive intestinal peptide levels linking gastrointestinal motility regulation reduce diarrhea, secondary to avoiding HTG, which needs the further proof of animal and molecular epidemiological study [41]. Third, there might be errors in the family history of cancer due to the small family units in China and Chinese personality characteristics; therefore, we haven’t completed an accurate data on family history of cancer and matching, as these statistics may be biased. Final, in the exclusion criteria of nonalcoholic fatty liver disease, we chose the same threshold for men and women, which may have a certain import on the results.
Conclusions
In summary, we found that hyperlipidemia, insulin resistance, Female may be associated with GBC risk in GSD patients. Of them, elevated serum triglyceride levels could be the remarkable independent predicting factor of GBC risk. More importantly, it is initially found that the sharp rise of serum TG levels might be advocated as the potential of a candidate diagnostic or prognostic biomarker of GBC with GSD. Meanwhile, we clarified that insulin resistance is a remarkable independent predicting factor of GBC risk without GSD. However, the viewpoint needs to be confirmed in the next step multicenter, cohort studies.
Availability of data and materials
Not applicable. The authors declare that the data supporting the findings of this study are available within the article.
Abbreviations
- GBC:
-
Gallbladder cancer
- BMI:
-
Body mass index
- TG:
-
Triglyceride
- TC:
-
Total cholesterol
- HDL-c:
-
High density lipoprotein cholesterol
- LDL-c:
-
Low density lipoprotein cholesterol
- NAFLD:
-
Nonalcoholic fatty liver disease
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- FBG:
-
Fasting blood glucose
- FINS:
-
Fasting blood insulin
- RBP:
-
Retinol binding protein
- HOMA-IR:
-
Homeostasis Model Assessment of IR
- IR:
-
Insulin resistance
- HBP:
-
High blood pressure
- DM:
-
Diabetes mellitus
- MetS:
-
Metabolic syndrome
- IGF:
-
Insulin growth factor
- NASH:
-
Non-alcoholic steatohepatitis
- HCC:
-
Hepatocellular carcinoma
- VLDL:
-
Very low-density lipoprotein
- IGFBP:
-
Insulin growth factor binding proteins
- MAPK:
-
Mitogen-Activated Protein Kinase
References
Lai CH, Lau WY. Gallbladder cancer–a comprehensive review. Surgeon. 2008;6(2):101–10.
Kim SH, Jung D, Ahn JH, Kim KS. Differentiation between gallbladder cancer with acute cholecystitis: considerations for surgeons during emergency cholecystectomy, a cohort study. Int J Surg. 2017;45:1–7.
Pak M, Lindseth G. Risk factors for cholelithiasis. Gastroenterol Nurs. 2016;39(4):297–309.
Espinoza JA, Bizama C, Garcia P, Ferreccio C, Javle M, Miquel JF, et al. The inflammatory inception of gallbladder cancer. Biochim Biophys Acta. 2016;1865(2):245–54.
Singh TD, Gupta S, Shrivastav BR, Tiwari PK. Epigenetic profiling of gallbladder cancer and gall stone diseases: evaluation of role of tumour associated genes. Gene. 2016;576(2 Pt 2):743–52.
Portincasa P, Di Ciaula A, de Bari O, Garruti G, Palmieri VO, Wang DQ. Management of gallstones and its related complications. Expert Rev Gastroenterol Hepatol. 2016;10(1):93–112.
Di Ciaula A, Portincasa P. Recent advances in understanding and managing cholesterol gallstones. F1000Res. 2018;7(F1000 Faculty Rev):1529.
Huang J, Patel HK, Boakye D, Chandrasekar VT, Koulaouzidis A, Lucero-Prisno Iii DE, et al. Worldwide distribution, associated factors, and trends of gallbladder cancer: a global country-level analysis. Cancer Lett. 2021;521:238–51.
Borena W, Edlinger M, Bjorge T, Haggstrom C, Lindkvist B, Nagel G, et al. A prospective study on metabolic risk factors and gallbladder cancer in the metabolic syndrome and cancer (Me-Can) collaborative study. PLoS ONE. 2014;9(2): e89368.
Rice CP, Vaishnavi KB, Chao C, Jupiter D, Schaeffer AB, Jenson WR, et al. Operative complications and economic outcomes of cholecystectomy for acute cholecystitis. World J Gastroenterol. 2019;25(48):6916–27.
Lamberts MP. Indications of cholecystectomy in gallstone disease. Curr Opin Gastroenterol. 2018;34(2):97–102.
Sheng B, Zhao Q, Ma M, Zhang J. An inverse association of weight and the occurrence of asymptomatic gallbladder stone disease in hypercholesterolemia patients: a case-control study. Lipids Health Dis. 2020;19(1):228.
Chinese Elderly Type 2 Diabetes P, Treatment of Clinical Guidelines Writing G, Geriatric E, Metabolism Branch of Chinese Geriatric S, Geriatric E, Metabolism Branch of Chinese Geriatric Health Care S, et al. Clinical guidelines for prevention and treatment of type 2 diabetes mellitus in the elderly in China (2022 edition). Zhonghua Nei Ke Za Zhi. 2022;61(1):12–50.
Al-Makki A, DiPette D, Whelton PK, Murad MH, Mustafa RA, Acharya S, et al. Hypertension pharmacological treatment in adults: a world health organization guideline executive summary. Hypertension. 2022;79(1):293–301.
Placzkowska S, Pawlik-Sobecka L, Kokot I, Piwowar A. Estimation of reference intervals of insulin resistance (HOMA), insulin sensitivity (Matsuda), and insulin secretion sensitivity indices (ISSI-2) in polish young people. Ann Agric Environ Med. 2020;27(2):248–54.
Wolska A, Yang ZH, Remaley AT. Hypertriglyceridemia: new approaches in management and treatment. Curr Opin Lipidol. 2020;31(6):331–9.
Bragelmann J, Barahona Ponce C, Marcelain K, Roessler S, Goeppert B, Gallegos I, et al. Epigenome-wide analysis of methylation changes in the sequence of gallstone disease, dysplasia, and gallbladder cancer. Hepatology. 2021;73(6):2293–310.
Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut Liver. 2012;6(2):172–87.
Andreotti G, Chen J, Gao YT, Rashid A, Chang SC, Shen MC, et al. Serum lipid levels and the risk of biliary tract cancers and biliary stones: a population-based study in China. Int J Cancer. 2008;122(10):2322–9.
Lai HC, Chang SN, Lin CC, Chen CC, Chou JW, Peng CY, et al. Does diabetes mellitus with or without gallstones increase the risk of gallbladder cancer? Results from a population-based cohort study. J Gastroenterol. 2013;48(7):856–65.
Becker S, Dossus L, Kaaks R. Obesity related hyperinsulinaemia and hyperglycaemia and cancer development. Arch Physiol Biochem. 2009;115(2):86–96.
Pollak M. The insulin and insulin-like growth factor receptor family in neoplasia: an update. Nat Rev Cancer. 2012;12(3):159–69.
Zhou H, Guo W, Zhao Y, Wang Y, Zha R, Ding J, et al. MicroRNA-135a acts as a putative tumor suppressor by directly targeting very low density lipoprotein receptor in human gallbladder cancer. Cancer Sci. 2014;105(8):956–65.
Smelt AH. Triglycerides and gallstone formation. Clin Chim Acta. 2010;411(21–22):1625–31.
Ivanchenkova RA, Gatsenko VP, At’kova ER, Meshkov AN. Disorders of lipid metabolism in patients with cholelithiasis and gallbladder cholesterosis depending on apolipoprotein E genotype. Klin Med (Mosk). 2010;88(4):43–8.
Ivanchenkova RA, Sharashkina NV. Heterogeneity of low-density lipoproteins in cholesterolosis of the gallbladder and cholelithiasis. Klin Med (Mosk). 2004;82(10):46–9.
Yoo KS, Choi HS, Jun DW, Lee HL, Lee OY, Yoon BC, et al. MUC expression in gallbladder epithelial tissues in cholesterol-associated gallbladder disease. Gut Liver. 2016;10(5):851–8.
Roa I, Ibacache G, Roa J, Araya J, de Aretxabala X, Munoz S. Gallstones and gallbladder cancer-volume and weight of gallstones are associated with gallbladder cancer: a case-control study. J Surg Oncol. 2006;93(8):624–8.
Pejic RN, Lee DT. Hypertriglyceridemia. J Am Board Fam Med. 2006;19(3):310–6.
Wuermli L, Joerger M, Henz S, Schmid HP, Riesen WF, Thomas G, et al. Hypertriglyceridemia as a possible risk factor for prostate cancer. Prostate Cancer Prostatic Dis. 2005;8(4):316–20.
Asgharpour A, Cazanave SC, Pacana T, Seneshaw M, Vincent R, Banini BA, et al. A diet-induced animal model of non-alcoholic fatty liver disease and hepatocellular cancer. J Hepatol. 2016;65(3):579–88.
Hirasawa A, Makita K, Akahane T, Yokota M, Yamagami W, Banno K, et al. Hypertriglyceridemia is frequent in endometrial cancer survivors. Jpn J Clin Oncol. 2013;43(11):1087–92.
Feng HY, Chen YC. Role of bile acids in carcinogenesis of pancreatic cancer: an old topic with new perspective. World J Gastroenterol. 2016;22(33):7463–77.
Di Ciaula A, Wang DQ, Molina-Molina E, Lunardi Baccetto R, Calamita G, Palmieri VO, et al. Bile acids and cancer: direct and environmental-dependent effects. Ann Hepatol. 2017;16(Suppl 1:s3-405):s87–105.
Avgerinos KI, Spyrou N, Mantzoros CS, Dalamaga M. Obesity and cancer risk: emerging biological mechanisms and perspectives. Metabolism. 2019;92:121–35.
Wang F, Wang B, Qiao L. Association between obesity and gallbladder cancer. Front Biosci (Landmark Ed). 2012;17:2550–8.
Yazici D, Sezer H. Insulin resistance, obesity and lipotoxicity. Adv Exp Med Biol. 2017;960:277–304.
Shebl FM, Andreotti G, Meyer TE, Gao YT, Rashid A, Yu K, et al. Metabolic syndrome and insulin resistance in relation to biliary tract cancer and stone risks: a population-based study in Shanghai. China Br J Cancer. 2011;105(9):1424–9.
Berger NA. Obesity and cancer pathogenesis. Ann N Y Acad Sci. 2014;1311:57–76.
Othman EM, Leyh A, Stopper H. Insulin mediated DNA damage in mammalian colon cells and human lymphocytes in vitro. Mutat Res. 2013;745–746:34–9.
Chey WY, Frankel WL, Roy S, Datta S, Sen CK, Dillhoff M, et al. Primary pancreatic Secretinoma: further evidence supporting secretin as a Diarrheogenic hormone. Ann Surg. 2017;266(2):346–52.
Acknowledgements
The authors thank all subjects for participating in this study.
Funding
This work has been supported by funding by the ‘‘Natural Science Foundation of Shaanxi Province of China” (2020JM-395). The funding source had no role in the study design, collection, analysis and interpretation of the data, in the writing of the report or in the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
Yong Wan and Jianqin Zhang were responsible for analyzing the data, organizing the manuscript and literature review in the background and discussion; Mao Ma and Min Chen were responsible for interpreting the results. Binwu Sheng was responsible for drafting the background and conclusions, in addition to finalizing the writing. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was reviewed and approved by the First Affiliated Hospital of Xi’an Jiaotong University. XJTU1AF2020LSK-160. All participants provided written informed consent before being admitted to the First Affiliated Hospital of our University.
Consent for publication
Not applicable in the retrospective study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wan, Y., Zhang, J., Chen, M. et al. Elevated serum triglyceride levels may be a key independent predicting factor for gallbladder cancer risk in gallbladder stone disease patients: a case–control study. BMC Endocr Disord 22, 270 (2022). https://doi.org/10.1186/s12902-022-01189-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-022-01189-y