
Abstract
Background
In insulin-treated patients with type 2 diabetes mellitus (T2DM), glycemic control is usually suboptimal.
Methods
This study compared the risks of mortality and cardiovascular events in insulin-treated patients adding or not adding alpha-glucosidase inhibitors (AGIs).
Results
This cohort study included data from the Taiwan National Health Insurance Research Database. In total, 17,417 patients newly diagnosed as having T2DM and undergoing insulin therapy during 2000–2012 were enrolled. Overall incidence rates of all-cause mortality, hospitalized coronary artery disease (CAD), stroke, and heart failure were compared between 4165 AGI users and 4165 matched nonusers. The incidence rates of all-cause mortality were 17.10 and 19.61 per 1000 person-years in AGI nonusers and users, respectively. Compared with nonusers, AGI users had a higher mortality risk [adjusted hazard ratio (aHR) = 1.21, 95% confidence interval (CI) = 1.05–1.40; p = 0.01]. Regarding AGI use, aHRs (95% CI) for cardiovascular death, non-cardiovascular death, hospitalized CAD, stroke, and heart failure were 1.20 (0.83–1.74), 1.27 (1.07–1.50), 1.12 (0.95–1.31), 0.98 (0.85–1.14), and 1.03 (0.87–1.22) respectively.
Conclusion
AGI use was associated with higher risks of all-cause mortality and non-cardiovascular death in insulin-treated patients with T2DM. Therefore, adding AGIs in insulin-treated patients may not be appropriate.
Similar content being viewed by others


Background
Hyperglycemia increases cardiovascular risks [1]; even when lower than the diabetic threshold, blood glucose levels remain a continuous risk factor for cardiovascular death [2]. After adjustments for major risk factors, type 2 diabetes mellitus (T2DM) is associated with considerably increased risks of premature cardiovascular and non-cardiovascular deaths [3]. Thus, in the current clinical scenario, maintaining blood glucose levels within the reference range and preventing diabetic complications are essential. However, T2DM is a progressive disease characterized by a slow, continuous decline in β-cell function [4]. The UK Prospective Diabetes Study (UKPDS) revealed that after 3 years, approximately 50% of the patients required multiple therapies to meet their glycemic target [5]. Moreover, administration of exogenous insulin injections is frequently required for adequately treat T2DM. Even with insulin therapy, approximately 70% of patients with T2DM do not reach their therapeutic goal [6]. Insulin-treated patients may have higher mortality risks than do non–insulin-treated patients [7]. Yki-Järvinen [8] reported that using insulin combination therapy instead of insulin monotherapy can improve glycemic control. However, objective data on the combined use of oral agents and insulin injections are scant, and there is no consensus regarding the optimal insulin combination therapy.
Alpha-glucosidase inhibitors (AGIs) can reversibly bind to the carbohydrate-binding region of alpha-glucosidases and thereby compete with oligosaccharide binding and delay the cleavage of oligosaccharides to monosaccharides. AGIs can thus retard intestinal glucose absorption and blunt postprandial hyperglycemia [9]. The reduction of postprandial glucose levels can attenuate glucose toxicity and increase insulin sensitivity. The results from the acarbose arm of UKPDS revealed that over a 3-year treatment course, acarbose had a persistent hemoglobin A1c (HbA1c) level–reducing effect similar to that of other therapies [10]. AGIs can also reduce fasting blood glucose levels and postprandial glucose excursion without increasing body weight. AGIs could be ideal complementary drugs in insulin combination therapy. Additionally, rice is the staple food in Asian people, AGIs can retard the absorption of carbohydrate and play an important role in controlling blood sugar in this area.
The Acarbose Cardiovascular Evaluation (ACE) trial [11]—a randomized, controlled trial in patients with impaired glucose tolerance and coronary heart disease—reported that acarbose had a neutral effect on major cardiovascular event outcomes. However, several short-term (< 1 year) randomized, controlled trials have demonstrated that acarbose can significantly reduce HbA1c and postprandial glucose levels in insulin-treated patients with T2DM [12, 13]. Furthermore, no relevant long-term results have been reported; therefore, in the current nationwide retrospective cohort study, we evaluated the long-term outcomes of adding AGIs in insulin-treated patients with T2DM.
Methods
Data source
National Health Insurance (NHI) is a mandatory, single-payer insurance program, implemented in Taiwan in 1995, that enrolls approximately 99% of Taiwan’s residents (approximately 23 million people) [14]. We retrieved data from the NHI Research Database (NHIRD), which contains beneficiaries’ information, including outpatient and inpatient claims, drug prescriptions, and medical procedures. Longitudinal Health Insurance Database 2000 (LHID2000), an NHIRD dataset, contains all the original claims data of 1,000,000 beneficiaries, randomly sampled from the NHIRD beneficiaries in 2000. These data include beneficiaries’ birthdate, sex, medical orders, procedures, and medical diagnoses [according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)]. We collected patient information from the LHID2000. In the LHID2000, information that could be used to identify individuals or care providers is concealed before release to researchers. The Research Ethics Committee of China Medical University and Hospital approved our study (CMUH104-REC2–115) and waived the need for informed consent.
Study population
The overall observation period of this retrospective cohort study was 14 years (January 1, 2000, to December 31, 2013). We selected patients newly diagnosed as having T2DM (ICD-9-CM: 250.x) at the age of 30–100 years during 2000–2012. To ensure diagnostic accuracy, only patients with ≥2 diagnoses of T2DM in the outpatient claims or ≥ 1 discharge diagnosis of T2DM in the inpatient claims were considered eligible for inclusion. All patients received insulin treatment after T2DM diagnosis.
We excluded patients diagnosed as having type 1 diabetes mellitus (ICD-9-CM: 250.1x) and hepatic failure (ICD-9-CM: 570, 572.2, 572.4, and 572.8), those undergoing dialysis (ICD-9-CM: 39.95, V56.0, V56.8, and V45.1), those with severe hypoglycemia at emergency department visits or hospitalization (to preclude patients with previous hypoglycemia), those with missing basic information, and those who had used AGIs before insulin prescription.
AGI exposure
We identified patients who received prescriptions of AGIs (including acarbose and miglitol) after receiving insulin therapy. The index date was defined as the date of first AGI use. AGI nonusers, defined as patients who did not use AGIs during the entire observation period, were randomly assigned an index date after insulin therapy, within the follow-up period.
Comorbidities and other demographic information
The comorbidities included in this study were coronary artery disease (CAD; ICD-9-CM: 410–414), stroke (ICD-9-CM: 430–438), peripheral arterial occlusive disease (ICD-9-CM: 440.2x, 443.9, 84.1x, 39.25, 39.29, 39.50, and 39.59), heart failure (ICD-9-CM: 428), and atrial fibrillation (ICD-9-CM: 427.3). To increase the validity of the comorbidity diagnoses in the administrative dataset, only patients with ≥2 outpatient or ≥ 1 inpatient claim for these comorbidities were included. We also used the Charlson comorbidity index to quantify other comorbidity profiles of the patients [15]; the adapted Diabetes Complications Severity Index (aDCSI) score [16] was used to evaluate diabetes severity. The Charlson comorbidity index and Diabetes Complications Severity Index scores were calculated according to the patient status 1 year before the index date. We considered the use of basal, premixed, and prandial insulin; antidiabetic drugs other than AGIs (including metformin, sulphonylureas, dipeptidyl peptidase-4 inhibitors, and thiazolidinediones) after the date of diagnosis of diabetes; antihypertensive drugs [such as angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), beta-blockers, calcium-channel blockers, diuretics, and potassium-sparing diuretics]; statins; and aspirin.
Main outcomes
The primary outcome of this study was all-cause mortality. Mortality was defined by discharge from hospital with certified death (the discharge date was defined as the death date) or by termination of the NHI coverage after discharge from hospital due to critical illness (the end of NHI coverage was defined as the death date). The secondary outcomes of this study were CAD, stroke, and heart failure hospitalizations. These cardiovascular events were assessed from the CAD, stroke, or heart failure diagnoses at hospitalization. Diagnostic accuracy of using ICD-9-CM in NHIRD has been validated previously [17]. The observation period was from the index date to the date of withdrawal from NHI, the date the outcomes were first noted, or December 31, 2013 (the end of the study), whichever occurred first. The primary diagnosis at discharge from hospitalization within 3 months before death was assessed for possible identifiable causes of death [18]. Identifiable causes of cardiovascular death were appropriated from the draft definition provided by Hicks et al. [19]; the diagnoses not included in cardiovascular-related deaths were classified as non-cardiovascular deaths.
Statistical analysis
Propensity score-matching was adopted to minimize bias due to confounding variables and augment comparability between the two study groups [20]. Nearest-neighbor probability was measured using a multivariable logistic regression model with AGI receipt as a dependent variable to construct matched pairs, in which the proportion between 0.995 and 1.0 indicated a perfect analog. We performed 1:1 propensity score-matching for sex, age, Charlson comorbidity index, Diabetes Complications Severity Index score, and comorbidity as well as for use of antidiabetic drug, antihypertensive drug, statin, and aspirin, by using multiple logistic regression analysis. Demographic information was analyzed using the chi-square and Student t tests for categorical and continuous variables, respectively. Cox proportional hazard model was applied to estimate hazard ratios (HRs) and their 95% confidence intervals (CIs) for events related to AGI use. The Kaplan–Meier method was used to calculate cumulative incidence of mortality, and the log-rank test was used to compare the difference in mortality between AGI users and nonusers. To evaluate the dose effect, we analyzed the risk of all-cause mortality according to the cumulative defined daily dose (DDD) of AGI use (< 12.47, 12.47–74.96, or > 74.96 DDD/year), relative to AGI nonuse. Here, defined daily dose, the assumed average maintenance dose per day for adults, for both acarbose and miglitol was 300 mg. We considered a two-tailed p of < 0.05 to be significant. The SAS (version 9.4 for Windows; SAS Institute, Inc., Cary, NC, USA) was used for data analysis.
Results
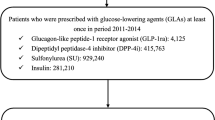
In total, 17,417 patients newly diagnosed as having T2DM receiving insulin therapy during 2000–2012 were included (Fig. 1). After exclusion of ineligible patients, 7335 AGI users and 6683 nonusers remained (Table 1). Compared with AGI users, more AGI nonusers were male and elderly; moreover, the nonusers had shorter diabetes durations, higher Charlson comorbidity index scores, lower Diabetes Complications Severity Index scores, and lower CAD incidence rates and had undergone less intensive treatments. After 1:1 propensity score-matching, the aforementioned variables did not differ significantly between AGI users and nonusers. Finally, both the study (users) and control (nonusers) cohorts each included 4165 patients. Approximately 48.1% of all patients were women. The mean (standard deviation) age of AGI users and non-users were 64.2 (13.1) and 64.3 (13.2) years; the mean follow-up time of AGI users and non-users were 5.38 (3.22) and 4.78 (3.13) years, respectively.

Flow of patient selection and study design
Moreover, in AGI users and nonusers, 405 and 351 deaths occurred, respectively (incidence rate = 19.61 and 17.10 per 1000 person-years, respectively; adjusted HR (aHR) = 1.21, 95% CI = 1.05–1.40; p = 0.010; Table 2). Figure 2 illustrates the cumulative incidence of all-cause mortality based on the Kaplan–Meier method results, revealing a higher mortality risk in AGI users than in nonusers (log-rank test, p = 0.0551).

Cumulative incidence of all-cause mortality in AGI users and nonusers
As presented in Table 2, the aHRs of < 12.47, 12.47–74.96, and > 74.96 cumulative DDD/year of AGI for all-cause mortality were 1.15, 1.15, and 1.41, respectively, with the p for trend = 0.002. As presented in Table 3, the aHRs for cardiovascular death, non-cardiovascular death, hospitalized CAD, stroke, and heart failure in AGI users compared with nonusers were 1.20, 1.27, 1.12, 0.98, and 1.03, respectively.
Factors that increased risk of all-cause mortality included Charlson comorbidity index score of 1 or ≥ 2, stroke or heart failure history, and diuretics use. Male patients as well as those aged 40–64 years or ≥ 65 years were also at higher risk of all-cause mortality (Table 2). Dipeptidyl peptidase-4 inhibitor, thiazolidinedione, ACEI or ARB, beta-blocker, and statin use was associated with lower mortality risks.
Discussion
After propensity score-matching for multiple clinical variables, adding AGIs in insulin-treated patients were associated with higher risks of all-cause mortality compared with insulin-treated patients not adding AGIs. This mortality risk associated with AGI use displayed a dose–response trend. The increased risk of mortality was predominantly associated with non-cardiovascular death. Our study also demonstrated that adding AGIs in insulin-treated patients had no significant effect on the risks of hospitalized CAD, stroke, and heart failure as compared with patients not adding AGIs.
The STOP-NIDDM trial results revealed that acarbose use in patients with impaired glucose tolerance reduced cardiovascular disease risk [21]. However, the ACE trial indicated that in Chinese patients with impaired glucose tolerance and coronary heart disease, acarbose did not reduce the risk of major cardiovascular events [11]. A meta-analysis of seven long-term randomized controlled trials found that compared with a placebo, acarbose could reduce myocardial infarction and cardiovascular event risks in patients with T2DM [22]. In their nationwide cohort study, Chang et al. demonstrated that metformin add-on AGI was associated with lower acute myocardial infarction risks compared with metformin add-on sulphonylurea [23]. Hsu et al. compared the use of acarbose as an add-on treatment to metformin with sulfonylurea, and reported low myocardial infarction and ischemic stroke hospitalization risks, but no effect on all-cause mortality [24]. AGIs can reduce HbA1c, postprandial glucose levels, and glucose excursion [25]. Subsequently, reduction in blood glucose levels can diminish the superoxide overproduction in the mitochondrial electron transport chain, which reduces oxidative stress [25]. Some studies have also determined that AGI use can restore endothelial function and reduce carotid intima–media thickening, low-grade inflammation, and cardiac interstitial fibrosis [25]. However, the Cochrane systematic review of acarbose use in patients with T2DM did not reveal any prognostic benefits on mortality or morbidity [26]. The long-term outcomes of AGI use remain inconclusive.
Some randomized controlled trials of adding acarbose in insulin-treated patients have revealed significant reductions in HbA1c and postprandial glucose levels [12, 13]; however, long-term outcomes have not been reported. The present study demonstrated that adding AGIs in insulin-treated patients have no significant effect on major cardiovascular events and cardiovascular death. This result is consistent with that of the aforementioned Cochrane systematic review [26] but differs from that of the MeRia study, Chang et al., and Hsu et al. This difference may be due to our patients having received insulin therapy; whereas in the other studies, patients were administered AGI monotherapy or metformin add-on dual therapy. Insulin-treated patients had longer T2DM duration with more complications, and AGI administration may not have been sufficient to reverse the atherosclerotic events.
Our study indicated that AGI use in insulin-treated patients may increase mortality risk and that higher cumulative defined daily dose of AGI can increase the propensity of mortality compared with AGI nonuse. The mechanism of action of AGI in insulin-treated patients and the resulting mortality risk remains unknown. AGI use does not appear to have severe toxicity, except for flatulence and diarrhea, which are commonly noted among AGI users [9]. Poor appetite with flatulence and dehydration after diarrhea should be closely monitored in AGI users to prevent the related mortality.
Taken together, the following are our speculations regarding mortality risk and adding AGIs in insulin-treated patients with T2DM. Although we balanced basal, prandial insulin, and oral antidiabetic drugs use between the study and control cohorts, combining AGI and insulin to treat hyperglycemia may not be as efficient for glycemic control as increasing insulin or combining insulin with other antidiabetic agents; the mortality risk reduction may also not be as efficient as other antidiabetic agents. Another possibility is that individuals who were on larger cumulative defined daily doses of AGI might have more suboptimal glycemic control with possible higher complication burden and mortality risk, and therefore required higher dose of AGI for achieving optimal glycemic control.
According to the draft of definition for cardiovascular-related causes of death by Hicks et al. [19], which does not include cerebrovascular diseases, the proportion of cardiovascular and non-cardiovascular deaths in our study were 14.9 and 75.8%, respectively. This result is consistent with the report of the national survey of mortality in Taiwan’s patients with T2DM during 2005–2014 [27]. Thus, most of the deaths in our insulin-treated patients with T2DM were non-cardiovascular.
Men, older patients, and patients with further comorbidities presented a higher mortality risk; these are high-risk groups who need closely monitoring when considering insulin treatments. This study demonstrated that statin use was associated with a lower mortality risk than was statin nonuse—consistent with a previous meta-analysis of statin therapy [28]. Dipeptidyl peptidase-4 inhibitor use in insulin-treated patients was associated with higher survival rates—consistent with our previous results [29]. Thus, the addition of dipeptidyl peptidase-4 inhibitors to insulin treatment may be a promising approach.
Our study revealed that ACEI and ARB use reduced mortality risk in insulin-treated patients; however, diuretic use for hypertensive treatment increased mortality risk. Most data suggested that adequate blood pressure control may be more critical than selecting particular agents for the management of hypertension [30]. As per the American Diabetes Association guidelines [30], the treatment of hypertension in patients with diabetes may include drugs that reduce the risk of cardiovascular events (such as ACEI, ARB or diuretics). However, the studies on the optimal drug choice for hypertensive treatment in patients with underlying insulin treatments are limited. Our study revealed that for treating hypertension in insulin-treated patients, ACEI or ARB might be more adequate than diuretics.
There are some limitations in this study. First, information on patients’ smoking status, alcohol consumption, physical activity level, body weight, and height are not provided in the NHIRD; similarly, blood glucose, HbA1c, cholesterol levels and renal function status are not available in the database. Nevertheless, through the propensity score-matching of multiple critical variables by maximally controlling for the confounding factors has potentially increased the accuracy of our results. Second, when using the claims data for analysis, assessing patient adherence to the dosage of prescribed insulin or oral antidiabetic drugs is difficult. In addition, as insulin prescription in the NHI system is monitored as the number of insulin pens used for reimbursement purposes, we could not derive an accurate insulin dosage, which may influence the results of mortality and cardiovascular events. Third, we did not measure the risk of hypoglycemia in our study because we could not calculate the rates for hypoglycemia accurately from the database. Hypoglycemia incidence in outpatient claims might be underestimated because patients do not report their hypoglycemia to their physicians; inpatient records of hypoglycemia might also be underestimated because some hypoglycemic patients are cared for by family members without being admitted to hospitals or are referred to the emergency department without admission. Finally, because this was a retrospective cohort study, it contained some inevitable biases; a large scale randomized trial is needed to evaluate our results for therapeutic applications.
Conclusions
In summary, adding AGIs in insulin-treated patients might increase all-cause mortality risk as compared with no adding AGIs; and most of the increased death risk is from non-cardiovascular causes. Thus, future studies on addition of antidiabetic agents other than AGIs with insulin for superior glycemic control and long-term favorable prognosis are warranted.
Availability of data and materials
Data are available from the National Health Insurance Research Database (NHIRD) published by Taiwan National Health Insurance (NHI) Bureau. The data utilized in this study cannot be made available in the paper, the supplemental files, or in a public repository due to the “Personal Information Protection Act” executed by Taiwan’s government, starting from 2012. Requests for data can be sent as a formal proposal to the NHIRD (http://nhird.nhri.org.tw) or by email to nhird@nhri.org.tw.
Abbreviations
- T2DM:
-
Type 2 diabetes mellitus
- AGI:
-
Alpha-glucosidase inhibitor
- CAD:
-
Coronary artery disease
- DDD:
-
Defined daily dose
References
Hanefeld M, Fischer S, Julius U, Schulze J, Schwanebeck U, Schmechel H, et al. Risk factors for myocardial infarction and death in newly detected NIDDM: the diabetes intervention study, 11-year follow-up. Diabetologia. 1996;39:1577–83.
Coutinho M, Gerstein HC, Wang Y, Yusuf S. The relationship between glucose and incident cardiovascular events: a meta regression analysis of published data from 20 studies of 95,783 individuals followed for 12.4 years. Diabetes Care. 1999;22:233–40.
Rao Kondapally Seshasai S, Kaptoge S, Thompson A, Di Angelantonio E, Gao P, Sarwar N. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med. 2011;364:829–41.
United Kingdom Prospective Diabetes Study Group. United Kingdom prospective diabetes study 24: a 6-year, randomized, controlled trial comparing sulfonylurea, insulin, and metformin therapy in patients with newly diagnosed type 2 diabetes that could not be controlled with diet therapy. Ann Intern Med. 1998;128:165–75.
Turner RC, Cull CA, Frighi V, Holman RR. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49). JAMA. 1999;281:2005–12.
Stark Casagrande S, Fradkin JE, Saydah SH, Rust KF, Cowie CC. The prevalence of meeting A1C, blood pressure, and LDL goals among people with diabetes, 1988–2010. Diabetes Care. 2013;36:2271–9.
Gamble JM, Simpson SH, Eurich DT, Majumdar SR, Johnson JA. Insulin use and increased risk of mortality in type 2 diabetes: a cohort study. Diabetes Obes Metab. 2010;12:47–53.
Yki-Järvinen H. Combination therapies with insulin in type 2 diabetes. Diabetes Care. 2001;24:758–67.
Lebovitz HE. Alpha-Glucosidase inhibitors. Endocrinol Metab Clin N Am. 1997;26:539–51.
Holman RR, Cull CA, Turner RC. A randomized double-blind trial of acarbose in type 2 diabetes shows improved glycemic control over 3 years (U.K. Prospective Diabetes Study 44). Diabetes Care. 1999;22:960–4.
Holman RR, Coleman RL, Chan JCN, Chiasson JL, Feng H, Ge J, et al. Effects of acarbose on cardiovascular and diabetes outcomes in patients with coronary heart disease and impaired glucose tolerance (ACE): a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017;5:877–86.
Coniff RF, Shapiro TB, Seaton TB, Hoogwerf BJ, Hunt JA. A double-blind placebo controlled trial evaluating the safety and efficacy of acarbose for the treatment of patients with insulin-requiring type 2 diabetes. Diabetes Care. 1995;18:928–32.
Hwu CM, Ho LT, Fuh MM, Siu SC, Sutanegara D, Piliang S, et al. Acarbose improves glycemic control in insulin-treated Asian type 2 diabetic patients: results from a multinational, placebo-controlled study. Diabetes Res Clin Pract. 2003;60:111–8.
Cheng TM. Taiwan’s new national health insurance program: genesis and experience so far. Health Aff (Millwood). 2003;22:61–76.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83.
Chang HY, Weiner JP, Richards TM, Bleich SN, Segal JB. Validating the adapted diabetes complications severity index in claims data. Am J Manag Care. 2012;18:721–6.
Sung SF, Hsieh CY, Lin HJ, Chen YW, Yang YHK, Li CY. Validation of algorithms to identify stroke risk factors in patients with acute ischemic stroke, transient ischemic attack, or intracerebral hemorrhage in an administrative claims database. Int J Cardiol. 2016;215:277–82.
Johansson LA, Westerling R. Comparing hospital discharge records with death certificates: can the differences be explained? J Epidemiol Community Health. 2002;56:301–8.
Hicks KA, James Hung HM, Mahaffey KW, et al. Standardized definitions for cardiovascular and stroke end point events in clinical trials. Draft definitions for CDISC. 2014. https://mdepinet.org/wp-content/uploads/S_1_6_Hicks.pdf. Accessed 19 Sept 2019.
D’Agostino RB Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat Med. 1998;17:2265–81.
Chiasson JL, Josse RG, Gomis R, Hanefeld M, Karasik A, Laakso M, et al. Acarbose treatment and the risk of cardiovascular disease and hypertension in patients with impaired glucose tolerance: the STOP-NIDDM trial. JAMA. 2003;290:486–94.
Hanefeld M, Cagatay M, Petrowitsch T, Neuser D, Petzinna D, Rupp M. Acarbose reduces the risk for myocardial infarction in type 2 diabetic patients: meta-analysis of seven long-term studies. Eur Heart J. 2004;25:10–6.
Chang YC, Chuang LM, Lin JW, Chen ST, Lai MS, Chang CH. Cardiovascular risks associated with second-line oral antidiabetic agents added to metformin in patients with type 2 diabetes: a nationwide cohort study. Diabet Med. 2015;32:1460–9.
Hsu PF, Sung SH, Cheng HM, Shin SJ, Lin KD, Chong K, et al. Cardiovascular benefits of acarbose vs sulfonylureas in patients with type 2 diabetes treated with metformin. J Clin Endocrinol Metab. 2018;103:3611–9.
Standl E, Theodorakis MJ, Erbach M, Schnell O, Tuomilehto J. On the potential of acarbose to reduce cardiovascular disease. Cardiovasc Diabetol. 2014;13:81.
Van de Laar FA, Lucassen PL, Akkermans RP, Van de Lisdonk EH, Rutten GEHM, Van Weel C. Alpha-glucosidase inhibitors for type 2 diabetes mellitus. Cochrane Database Syst Rev. 2005;2:CD003639.
Li HY, Wu YL, Tu ST, Hwu CM, Liu JS, Chuang LM. Trends of mortality in diabetic patients in Taiwan: a nationwide survey in 2005–2014. J Formos Med Assoc. 2019;118:S83–9.
Collins R, Reith C, Emberson J, Armitage J, Baigent C, Blackwell L, et al. Interpretation of the evidence for the efficacy and safety of statin therapy. Lancet. 2016;388:2532–61.
Yen FS, Chiang JH, Hwu CM, Yen YS, Lin BJ, Wei JCC, et al. All-cause mortality of insulin plus dipeptidyl peptidase-4 inhibitors in persons with type 2 diabetes. BMC Endocr Disord. 2019;19:3.
de Boer IH, Bangalore S, Benetos A, Davis AM, Michos ED, Muntner P, et al. Diabetes and hypertension: a position statement by the American diabetes association. Diabetes Care. 2017;40:1273–84.
Acknowledgements
This manuscript was edited by Wallace Academic Editing.
Funding
This study is supported in part by the Taiwan Ministry of Health and Welfare Clinical Trial Center (MOHW106-TDU-B-212-113004), China Medical University Hospital, Academia Sinica Taiwan Biobank Stroke Biosignature Project (BM10601010036), Taiwan Clinical Trial Consortium for Stroke (MOST 106–2321-B-039-005), Taipei Veterans General Hospital (V105C-204). These funding agencies did not influence the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
FSY and CMH participated in the study design. JCW and MCL participated in the study coordination and data collection. MCL and CCH participated in the data analysis, all authors contributed in interpretation of the results and discussions. FSY and CMH participated in the manuscript writing. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work, and have given approval for this paper to be published.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The data utilized in this study cannot be made available in the paper, or in a public repository. Requests for raw data need to be permitted by the NHIRD Office (http://nhird.nhri.org.tw). The NHIRD office has permitted us to use the data for this study. In the LHID2000, information that could be used to identify individuals or care providers is concealed before release to researchers. The Research Ethics Committee of China Medical University and Hospital approved our study (CMUH104-REC2–115) and waived the need for informed consent.
Consent for publication
Not applicable.
Competing interests
The authors that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yen, FS., Wei, J.CC., Lin, MC. et al. Long-term outcomes of adding alpha-glucosidase inhibitors in insulin-treated patients with type 2 diabetes. BMC Endocr Disord 21, 25 (2021). https://doi.org/10.1186/s12902-021-00690-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-021-00690-0