
Abstract
Background
Aphallia is a rare congenital anomaly often associated with other urogenital anomalies. The management of aphallia cases for both the immediate and long-term treatment of patients with aphallia pose a major dilemma. Patients are at risk for psychosocial and psychosexual challenges throughout life.
Methods
A systematic review was conducted on aphallia cases. We searched online databases until March 2023 for relevant articles and performed according to the PRISMA-P guidelines.
Results
Of the 43 articles screened, there were 33 articles included. A total of 41 patients were analyzed qualitatively. Asia is the region with the most aphallia cases with 53% (n:22), while the United States is the country with the most most reported aphallia cases 31% (n:13). Most cases were identified as male sex (n: 40), and most cases were neonate with 68% (n:28) cases. Physical examination generally found 85% (N = 35) with normal scrotal development and palpable testes. The most affected system with anomalies is the genitourinary system with fistulas in 80% (n:29) cases. Initial management in 39% (n:16) of patients involved vesicostomy. Further management of 31% (n:13) included phalloplasty or penile reconstruction, and 12% (n:5) chose female sex. 17% (n:7) of patients refused medical treatment or were lost to follow-up, and 12% (n = 5) patients deceased.
Conclusion
Aphallia is a rare condition and is often associated with other inherited genitourinary disorders. In most cases, physical examinations are normal except for the absence of a phallus, and laboratory testing shows normal results. The initial management typically involves the vesicostomy procedure. Subsequent management focuses on gender determination. Currently, male sex is preferred over female. Due to the significant variability, the rarity of cases, and the lack of long-term effect reporting in many studies on aphallia, further research is needed to minimize bias.
Similar content being viewed by others


Background
Aphallia, is a rare congenital anomaly (1:30 million) and is associated with other urogenital anomalies. Under 100 cases of aphallia have been reported worldwide [1]. The absence or failure of the development of the genital tuberculum will cause aphallia. The penis and clitoris originate from the genital tubercle, which develops from mesenchymal prominence in the cloaca membrane during the fourth week of pregnancy. This failure may be caused by an initial disruption in cloacal maturation or poor development of the caudal mesenchyme. This can also lead to proximal urethrorectal communication, which will explain the high incidence of concurrent anorectal anomalies seen in aphallia patients [2].
Both the immediate and long-term management of aphallia patients pose a major dilemma [1] Patients are at risk for psychosocial and psychosexual challenges throughout life [3]. These patients require a multidisciplinary approach that often includes psychologists, endocrinologists, pediatric urologists, pediatric surgeons, plastic surgeons and social workers because not all community health care centers have access to every one of the specialties mentioned above [3]. In this review we aim to address the variability of disease presentation, the associated anomalies of the disease and will review the current knowledge of the treatment options in all age patients of aphallia.
Material and methods
Search strategy
We included case reports/ series involving patients with aphallia. This review follows the guidelines in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses—Protocol (PRISMA-P) to increase comprehensiveness and transparency of reporting [4]. We searched two electronic databases, Medline and Sciencedirect, until March 2023. The following keywords and medical subject headings were used: Aphallia, penile agenesis, absence of penile shaft, absence of penis, clitoral absence, absence of phallus, and absence of corpora cavernosa.
Study selection
The database search was conducted by two authors (P.Y. and E.T). Eligibility criteria for inclusion in the review was a specific focus on aphallia in all age of patients. Operation technique focus and non-English articles were excluded.
All articles reporting one or more cases of aphallia were obtained in full-text. Two authors (P.Y. and E.T) independently extracted data from all studies into data summary tables. The articles which fulfilled the eligibility criteria were included in this review. The following data were collected: age, clinical findings, supporting investigations, laboratory findings and management. The final selected papers were reviewed by three authors (P.E.Y., Y.Z., J.A.T.)
Data extraction and synthesis
The information that was extracted included the following: author and year of study; demographics of the patient, including age, proportion of males and female, weight and country, presenting signs and symptoms with percentage distribution; laboratory data and imaging findings with percentage distribution; and management with percentage distribution. Due to the qualitative, summative nature of this review and significant variations in participants, presentation, laboratory data, imaging and treatments, a meta-analysis could not be conducted and effect sizes could not be calculated.
Results
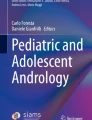
Our search resulted in 94 potentially relevant articles, of which 30 articles are duplicates. From the 64 articles identified, a total of 43 articles were screened for eligibility; and 33 articles met the full inclusion criteria (Fig. 1).

Prisma flow chart
They included 41 patients with aphallia. The results of these 33 studies are summarized in Table 1.
Demographics
The most cases were reported in the USA which were 31% (n:13) of all cases [2, 7, 8, 12, 16, 30, 32,33,34], followed by India with 21% (n:9) [14, 18, 19, 21, 25, 29, 34] Iran with 12% (n:5) [5, 13, 17], China with 7.3% [1, 6, 23], Turkey with 4% (n:2) [15, 31], France with 4% (n:2) [23, 27], Japan with 4% (n:2) [26, 27], Morocco with 4% (n:2) [9, 10], Mexico with 2% (n:1) [3], UK with 2% (n:1) [11], and Senegal with 2% (n:1) [22].
The majority of cases involve males with 97% (n:40) of all cases (1–3,7–29), and 2% (n:1) was female [2]. Of the 35 cases, the majority with 48% (n:20) cases were term neonates [2, 3, 8,9,10,11,12, 14, 17, 18, 21, 22, 25, 28, 30, 33], while 19% (n:8) were preterm neonates [2, 13, 24, 26, 32, 34], 9% (n:4) were infants [1, 16, 25, 34], 9% (n:4) were under five [5, 7, 19, 27],and 12% (n:5) were over 5 years old [6, 15, 23, 29, 31]. The patient with the lowest gestational age was 31 weeks [13], with the oldest patient ‘s age was 31 years old [23].
Only 14 cases reported weight. As many as 19% (n:8) of cases reported low birth weight neonate [13, 18, 21, 25, 26, 32], and 14% (n:6) of cases were normal birth weight neonates [9, 11, 14, 17, 25, 27]. The case with the lowest birth weight was 1,440 g [26] and the case with the largest birth weight was 4,000 g [25]. All characteristic data are shown in Table 2.
Presentation
On physical examination, as many as 95% (n:39) cases reported scrotum development, and 2% (n:1) case reported well-formed labia major [2]. From 39 cases, 85% (n:35) cases reported normal scrotum development [1,2,3, 5,6,7,8,9,10,11,12,13,14,15,16,17,18,19, 22,23,24,25, 27,28,29,30,31, 33, 34], and 9% (n:4) reported bifid scrotum [13, 21, 26, 32]. Almost all male cases reported testicular development (with 39 of the 40), with 82% (n:34) with descending testis [1,2,3, 5,6,7, 9,10,11,12,13,14,15,16,17,18,19,20,21,22,23, 25,26,27,28,29,30, 32,33,34] and 12% (n:5) with undescendent testes [8, 24, 25, 31].
The majority of the patients’ anus was in a normal position in 78% (n:32) cases [1,2,3, 5,6,7, 9,10,11,12,13, 15,16,17,18,19,20, 22, 27,28,29,30,31,32,33], with 2% (n:1) an anteriorly displaced anus [2], 17% (n:7) with imperforated anus [8, 14, 21, 22, 24,25,26], and 2% (n:1) with funnel anus [11]. As many as 22% (n:8) of the cases were found to have skin tags in the perineal area (2,21,27,29).
Other findings were 4% (n:2) cases with sepsis [18, 24], 7% (n:3) cases with respiratory distress [2, 13, 14], 2% (n:1) case with Potter sequence [24] and 4% (n:2) cases with clubfoot [13, 24]. All of these presentations are presented in Table 3.
Laboratory examination
Laboratory tests were conducted differently in each case. All such tests are presented in Table 4. Karyotype examination was performed in 29 cases. Almost all of these cases reported karyotype XY with 68% (n:28) [1, 2, 6, 8,9,10,11,12,13, 15, 16, 18, 20,21,22,23,24,25, 27, 28, 30, 31, 33], and 2% (n:1) case reported 46XX karyotype [2].
Only 16 cases reported kidney function [2, 6, 9,10,11, 13, 14, 16,17,18,19,20, 27, 33], indicating 21.9% (n:9) cases had normal kidney function results [2, 6, 9, 11, 16, 19, 27, 33, 34], and 17% (n:7) cases had abnormal kidney function results [2, 10, 11, 13, 17, 18, 27]. In 5 cases with abnormal kidney function, 5% (n:2) cases were found with renal dysplasia [2, 17], 2% (n:1) with atrophic renal due to multicystic bladder [13], 2% (n:1) with a single left urethra with rectobladder fistula draining to an anal funnel [11], and 2% (n:1) with sepsis due to urinary tract infection [18].
As few as 12% (n:5) cases reported bacteriuria with 4% (n:2) with symptomatic bacteriuria [18, 34], and 7% (n:3) with asymptomatic bacteriuria [19, 27, 31]. Only 8 cases reported hormonal profile and all cases showed normal results [3, 10, 15, 16, 18, 19, 23, 28].
Other lab examinations showed 7% (n:3) of all cases had metabolic acidosis [11, 18, 33], 7% (n:3) had kidney failure [13, 17, 20], while 2% (n:1) had sepsis and acute kidney injury due urinary tract infection [18].
Imaging investigation
Most cases used postnatal ultrasound in 75% (n: 31) cases [1,2,3, 5,6,7,8,9,10,11,12,13,14,15,16,17,18,19, 23, 25,26,27,28,29,30, 33, 34] followed by 46% (n:19) using cystography [2, 10, 13, 15, 16, 22, 23, 25,26,27,28, 30, 31, 33], 22% (n:9) using urography [2, 7, 15, 19, 23, 27, 29, 31, 33], 22% (n:9) using magnetic resonance imaging (MRI) [7, 8, 11, 12, 15, 16, 19, 23, 28], 17% (n:7) using nuclear imaging [2, 15, 16, 19, 33, 34], 17% (n:7) of cases using prenatal ultrasound [8, 12, 16, 24, 26, 28, 32], 14% (n:6) used computerized tomography (CT) scan [1, 1, 3, 5, 6, 15, 22], and 12% (N5) used endoscopy [2, 12, 27, 33].
Some studies used other imaging studies to exclude other system anomalies. As many as 17% of cases (n: 7) used echocardiogram [1, 3, 7, 13, 14, 18, 22], 4% (n: 2) used GI contrast [11, 30], and 7% (n: 3) used chest X-ray [14, 24, 27]. Only 1 case reported not using an imaging investigation because the parent did not provide consent [21].
Anomalies were found in the genitourinary system, cardiovascular system, respiratory system, digestive system, and muscular system (Table 5).
The genitourinary system is the most affected system with anomalies in aphallia cases. Fistulas occurred in 80% (n: 29) of cases and were the most commonly reported anomalies [1,2,3, 5,6,7, 9,10,11,12,13, 15,16,17, 19, 22, 23, 25,26,27, 29,30,31,32,33,34]. Urethrorectal fistulas are the most common fistula occurred in 46% (n:19) cases [1, 13, 16, 17, 19, 22, 23, 25, 27, 29,30,31, 33, 34], followed by urethroperineal fistula with 17% (n:7) cases [2, 7, 20, 25], vesicorectal fistula with 9% (n:4) cases [3, 5, 11, 15], urachal fistula by 4% (n: 2) [26, 32], and ureterorectal fistula with 2% (n: 1) case [12].
Other genitourinary anomalies found are in the kidneys, ureters, bladder, prostate and urethra. Renal abnormalities occurred in 63% (n:26) cases. Of the 22 cases with renal anomalies, renal agenesis occurred in 12% (n:5) [11, 14, 15, 25, 30], hypoplastic kidney in 4% (n:2) cases [3, 5], renal dysplasia in 19% (n:8) [2, 12, 13, 17, 20, 23, 24, 33], and hydronephrosis in 34% (n:14) [2, 8,9,10,11, 13, 18, 19, 25, 30, 31, 33, 34].
The ureteral anomaly occurred in 29% (n:12) of all cases. From 12 cases reported, ureteral reflux occurred in 26% (n:11) [2, 9, 10, 13, 15, 19, 22, 28, 33], absence of ureter occurred in 7% (n:3) [2, 15, 20], ectopic ureter in 2% (n:1) [2], and ureterocele occurred in 2% (n:1) [15].
Bladder anomalies occurred in 21% (n:9) of all cases [2, 12, 20, 21, 24, 27, 32]. Of the 9 cases, 7% (n:3) with absence of bladder [2, 12, 20], 4% (n:2) with hypoplastic bladder [24, 32], 4% (n:2) with posterior bladder diverticulum [2], hemibladder in 2% (n:1) case [21], and three bladders in 2% (n:1) [27].
Prostate absence occurred in 2% (n:1) of all cases [15], and hypoplastic prostate in 2% (n:1) of all cases [23]. The urethra anomalies occurred in 21% (n:9) [2, 3, 24, 26, 27, 32, 33], involving 9% (n:4) with absence of the urethra [3, 24, 26, 32], 7% (n:3) with posterior ureteral valve [2, 33], 4% (n:2) with urethral stenosis [2, 33], and 2% (n:1) with urethral stone [27].
The anomaly in the respiratory system occurred in 9% (n:4) of all cases [1, 11, 14, 24]. right lung absent occurred in 2% (n:1) case [24], 2% (n:1) case with pulmonary hypoplasia [14], 2% (n:1) case with pulmonary hypertension [1], and 2% case (n:1) with pulmonary hyperplasia [14]. Anomalies in the cardiovascular system were found in 12% (n:5) of all cases [1, 13, 14, 24]. Of the 5 cases, patent ductus arteriosus occurred in 4% (n:2) [1, 13], atrial septal defect in 5% (n:2) [1, 14], 7% (n:3) in tricuspid valve insufficiency [1, 13], and 2% (n:1) with hypertrophic myocardia [24].
In the digestive system, anomalies occurred in 9% (n:3) of all cases. Omphalocele occurred in 4% (n:2) [21, 32], and 2% (n:1) with duplicated colon, caecum, appendix, and short bowel syndrome [26]. In extremity anomalies, clubfoot bilateral occurred in 4% (n:2) of all cases [13, 24].
Management
Anomalies can be different in each case, causing management to differ in each case (Table 6). As many as 39% (n = 16) patients underwent vesicostomy [7,8,9,10,11, 13, 16, 18, 20,21,22, 26, 27, 32, 33]. Renal transplant and nephrectomy respectively were performed in 2% (n:1) of all cases [2, 23]. Ureteral reimplant was performed in 4% (n:2) [2], urethrostomy in 9% (n:4) [2, 19, 20, 27], and perineal urethroplasty in 9% (n:4) case [6, 16, 19, 27]. As few as 9% (n = 4) cases required dialysis [2, 12, 18, 20].
Further management in 7% patient (n = 3) involved phalloplasty [12, 20, 34], followed by 24% (n:10) that planned for penile reconstruction [6, 10, 11, 13, 16, 22, 25, 27, 29, 30], and 12% (n = 5) that chose feminization [28, 32, 33]. The number of patients who refused medical treatment or were lost to follow-up were as many as 17% (n:7) of all cases [1, 13,14,15, 17, 18, 25], and 12% (n = 5) of all patients deceased [13, 21, 25, 31].
Discussion
Penile agenesis is a very rare genitourinary occurrence with a prevalence of 1 in 30 million births [1]. Aphallia is defined as the absence of a phallus and ectopic urethral opening and associated with well-developed scrotum and bilateral palpable testes [35].
In males, the absence of the penis is characterized by the absence of three penile components: two corpora cavernosa and the corpus spongiosum. Aphallia can also occur in female patients, although it is considered less common and more difficult to diagnose. This is most likely due to a high association with bladder agenesis and intrauterine fetal demise [35].
In this review, the country with the most reported cases of aphallia was the United State [2, 7, 8, 12, 16, 30, 32,33,34], but regionally the most cases were in Asia. Patients with aphallia generally present at birth [2, 3, 8,9,10,11,12, 14, 17, 18, 21, 22, 25, 28, 30, 33], but in some cases patients come after being older than 1 month, for unknown reasons. All patients were male (1–3,7–29), except for one case where the clitoris was absent in a woman [2]. Most of the previous reports of aphallia were limited to boys, with some reports of clitoral agenesis in girls. This may be related to the underdiagnoses of aphallia in girls, where the absent clitoris is far less conspicuous than an absent penis.
Physical examination in the majority of studies showed that most patients had normal scrotal growth [1,2,3, 5,6,7,8,9,10,11,12,13,14,15,16,17,18,19, 22,23,24,25, 27,28,29,30,31, 33, 34], normally descended testes [1,2,3, 5,6,7, 9,10,11,12,13,14,15,16,17,18,19,20,21,22,23, 25,26,27,28,29,30, 32,33,34], and a normally sited anus [1,2,3, 5,6,7, 9,10,11,12,13, 15,16,17,18,19,20, 22, 27,28,29,30,31,32,33]. There can be abnormalities such as imperforated anus [8, 14, 21, 22, 24,25,26], bifid scrotum [13, 21, 26, 32], and undescended testes which occurred in a minority of cases for unknown reasons [8, 24, 25, 31].
This systematic review shows the various Imaging and laboratory modalities used with aphallia, and almost every case used a different modality. This may be because of the many anomalies that occurred, so it requires a different approach for each case and it should be noted that most cases have multiple anomalies.
Laboratory examination in karyotype examination revealed the majority of the cases are male [1, 2, 6, 8,9,10,11,12,13, 15, 16, 18, 20,21,22,23,24,25, 27, 28, 28, 30, 31, 33], and the majority had normal laboratory results. All hormonal profiles were in the normal range [3, 10, 15, 18, 19, 23, 28]. Besides, there are some abnormal laboratory tests on a small portion of cases that involve bacteriuria [18, 19, 27, 31, 34], metabolic acidosis [11, 18, 33], renal failure [13, 17, 20], and sepsis [18]. This may be due to abnormalities that occurred in the patients.
In this review, investigations found that all cases had genitourinary anomalies [1,2,3, 5,6,7, 9,10,11,12,13, 15,16,17, 19, 22, 23, 25,26,27, 29,30,31,32,33,34], with the most common anomaly was fistulas. The majority of the fistula were urethrorectal fistulas [1, 13, 16, 17, 19, 22, 23, 25, 27, 29,30,31, 33, 34] followed by urethroperineal fistula [2, 7, 20, 25]. The majority of abnormalities after fistula in the genitourinary system occurred in the kidneys. Hydronephrosis is the most common anomaly in kidneys [2, 8,9,10,11, 13, 18, 19, 25, 30, 31, 33, 34], followed by renal dysplasia [2, 12, 13, 17, 20, 23, 24, 33], and renal agenesis [11, 14, 15, 25, 30]. In the ureter, most anomalies were vesicoureteral reflux [2, 9, 10, 13, 15, 19, 22, 28, 33]. There were also found a small number of anomalies such as hypoplastic renal [3, 5], duplication of renal [2], absence of ureter [2, 15, 20], ectopic ureter [2], ureterocele [15], absence of bladder [2, 12, 20], absent [15] or hypoplastic prostate [23], and absence of urethra [3, 24, 26, 32].
Apart from abnormalities in the genitourinary system, in the respiratory system [1, 11, 14, 24], cardiovascular system [1, 13, 14, 24], digestive system [21, 26, 32], and musculoskeletal system abnormalities were also found in a small number of cases [13, 24].
The management of each case can be different because almost every case had different anomalies. Cystostomy was performed in most cases as the initial management of aphallia [7,8,9,10,11, 13, 16, 18, 20,21,22, 26, 27, 32, 33], especially those found to have a fistula, to allow draining of the urine, and to correct the fistula.
For advanced management, phalloplasty was more often done compared to patients who choose the female sex. Although aphallia is associated with congenital abnormalities, the mortality rate is quite low, and is caused by complications mainly due to sepsis and uricemia [13, 21, 25, 31].
Aphallia management is divided into three distinct phases: acute, subacute, and chronic. Previously, aphallia patients needed to be checked for chromosomes to exclude other causes of sexual differentiation and abnormalities such as congenital adrenal hyperplasia or other penile abnormalities (severe hypospadias, epispadias, and hidden or micropenis) [35].
In the acute phase, therapy is supportive and involves managing life-threatening complications. Vesicostomy can be performed, especially in patients who present with sepsis or urinary tract obstruction due to the absence of the urethra, to drain the urinary tract, relieve pressure, and prevent infection. In aphallia, urine obstruction is not always present, as seen in the case of urethra-perineal fistula, and no urine transfer is required at this stage [35].
Subacutely, perineal urethrostomy or catheterization vesicostomy can be performed for the separation of urethrorectal fistulas and in patients with a urethra that is too small or absent in order to gain access to the bladder [16]. Additionally, a pseudophallus can be created to enable patients to identify themselves as male [16].
The gender determination of aphallia is still controversial. In the past, surgery was recommended as the only reconstructive option in these cases, known as feminization genitoplasty. This recommendation was based on the belief that raising these patients as males could be disruptive, and it was considered better to be an imperfect female than an inadequate male. The management strategy includes early bilateral orchidectomy to prevent postnatal androgen implantation, followed by vaginal interposition and hormonal therapy during puberty. However, these patients often experience high levels of gender dysphoria, due to prenatal androgen implantation [35].
Prenatal and early neonatal androgen imprinting has been studied in animal models, pregnant women undergoing hormone therapy, and children with congenital adrenal hyperplasia. It has been shown that fetal exposure to testosterone has an influence on childhood sex interests, such as playmates and activity preferences, as well as later sexual orientation, which tends towards typically male behaviors and gynecophilia [35].
Sex determination considerations should be based on the sex that provides the best prognosis in terms of reproductive function, the ability to function sexually, the appearance of the external genitalia, and the patient’s self-identification with a particular sex. Therefore, although some authors still recommend feminizing genitoplasty for infants and newborns, it is now generally accepted that genetically normal males with aphallia should be supported surgically as males until the patient is old enough to identify their own sex, thus reducing gender dysphoria [35].
Chronic management is to create the functional prosthetic and aesthetic neophallus [16]. Construction of a functional neophallus requires a multidisciplinary team approach. One of the most considered treatment options for long-term management is phalloplasty, which can be performed before the patient reaches puberty. The gold standard technique for phalloplasty is microsurgical phalloplasty with a radial forearm free flap, which has shown good results and positive outcomes in terms of patients’ self-esteem and sexual well-being [36].
This study has several limitations. This review includes only studies published in English and may result in publication bias (language) in selecting studies due to the exclusion of other relevant articles published in languages other than English. Some articles lack data regarding patients, including age, clinical presentation, investigations, and evaluation of family history. This may be due to the rarity of cases and the variability of cases of aphallia, so that there is no standard method of aphallia. In addition, evaluating the progression of aphallia treatment is a challenge because many studies have not reported the long-term progress of the treatment chosen. Long-term follow-up is essential, but there is a distinct lack of information regarding the long-term outcomes of these patients. These patients need lifelong follow-up in a team of specialists, especially after puberty.
Conclusions
This systematic review shows that aphallia is a rare congenital anomaly, and all cases were associated with other genitourinary congenital abnormalities, especially fistulas between the genital tract and the rectum. Although often associated with other congenital abnormalities, most physical examinations and laboratory tests showed normal results except for the phallus. Initial management generally includes vesicostomy, and for advanced management, sex determination is recommended. Currently, male sex is preferred over female sex, possibly due to the predominance of male patients.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
References
Qiang S, Li FY, Zhou Y, et al. Congenital absence of the penis (aphallia): a rare case report. Medicine. 2019;98:e15129.
Friedman AA, Zelkovic PF, Reda EF, et al. Male and female aphallia associated with severe urinary tract dysplasia. J Pediatr Urol. 2016;12:268.e1-7.
Palacios-Juárez J, Hanson-Viana E, Rodríguez-Quintero JH, et al. Aphallia: do sociocultural issues affect treatment decisions? BMJ Case Rep. 2018;2018:bcr2018226459.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
Kian B, Esmaeilian S, Kayedi M. A rare case report of aphallia with hypoplastic kidney and vesicorectal fistula. Radiol Case Rep. 2022;17:4656–9.
Luo S-S, Yang Z, Ma N, et al. Congenital aphallia associated with congenital urethrorectal fistula: a rare case report. Medicine. 2022;101:e28878.
Blachman-Braun R, Galvez C, Guevara C, et al. Aphallia associated with anorectal malformation. Sultan Qaboos Univ Med J. 2022;22:428–9.
Vaizer RP, Benton JZ, Morganstern BA. First case of a term male born with aphallia and complete urethral atresia. Urology. 2021;156:e127-30.
El Qadiry R, Lalaoui A, Nassih H, et al. A new presentation: Aphallia, vesicoureteral reflux, rectovesical fistula, and adrenal insufficiency. Case Rep Pediatr. 2020;2020:1–3.
Bencharef O, Fouraiji K, Kamili EOEA, et al. Penile agenesis with urethrorectal fistula and vesicoureteral reflux. Fetal Pediatr Pathol. 2022;41:338–40.
Decker E, Upasani A, Giuliani S, et al. A rare case of complete penile agenesis. Urology. 2020;138:e8-9.
Chaudhry R, Theisen KM, Dangle PP, et al. Congenital aphallia: novel use of acellular dermal matrix during scrotal flap phalloplasty. Urology. 2017;105:167–70.
TalebpourAmiri F, NasiryZarrinGhabaee D, Naeimi RA, et al. Aphallia: report of three cases and literature review. Int J Reprod Biomed. 2016;14:279–84.
Shastri S, Sharma D, Kumar R. A case report of aphallia with urorectal septum malformation sequence in a newborn: a very rarely seen condition. IMCRJ. 2015;8:317–20.
Demirer Z, Aip BF, Uguz S, et al. A rare case of penis agenesis (Aphallia) with associated multiple urogenital anomalies. Int J Surg Case Rep. 2015;15:10–2.
Joshi A, Gross J, Thomalla JV. Congenital aphallia: review of pathogenesis and current treatment guidelines. Urology. 2015;86:384–7.
Aslanabadi S, Zarrintan S, Abdollahi H, et al. A rare case of aphallia with right kidney hypoplasia and left kidney dysplasia. Arch Iran Med. 2015;18:257–9.
Bahe P, Sharma D, Bahe A, et al. An infant with aphallia and its associated complication: a rare case report and review of literature. Trop Doct. 2016;46:51–3.
Bothra M, Jain V. Absent phallus: issues in management. J Pediatr Endocrinol Metab. 2012;25:1013–5.
Willihnganz-Lawson KH, Malaeb BS, Shukla AR. De Castro technique used to create neophallus: a case of aphallia. Urology. 2012;79:1149–51.
Arunachalam P, Pillai SB, Citla SD. Classical cloacal exstrophy with intravesical phallus. J Pediatr Surg. 2012;47:E5-8.
Kane AD, Ngom G, Ndour O, et al. Aphallia: a case report and literature review. Afr J Paediatr Surg. 2011;8:324–5.
Wang H, Guo K, Wang J, et al. Aphallia in an adult male with 46. XY karyotype Int J Urol. 2011;18:540–2.
Gérard-Blanluet M, Lambert V, Khung-Savatovsky S, et al. Aphallia, lung agenesis and multiple defects of blastogenesis. Fetal Pediatr Pathol. 2011;30:22–6.
Rattan KN, Kajal P, Pathak M, et al. Aphallia: experience with 3 cases. J Pediatr Surg. 2010;45:E13-16.
Nakano Y, Aizawa M, Honma S, et al. Completely separated scrotum and vesicointestinal fistula without exstrophy as a novel manifestation of aphallia: a case report. Urology. 2009;74:1303–5.
Shamsa A, Kajbafzadeh AM, Javad Parizadeh SM, et al. Aphallia associated with urethro-rectal fistula and stones in the bladder and urethra. Saudi J Kidney Dis Transpl. 2008;19:435–8.
Coquet-Reinier B, Merrot T, Chaumoître K, et al. Atypical aphallia. Pediatr Surg Int. 2007;23:1131–3.
Chibber PJ, Shah HN, Jain P, et al. Male gender assignment in aphallia: a case report and review of the literature. Int Urol Nephrol. 2005;37:317–9.
Threatt CB, Wiener JS. Aphallia with congenital urethrorectal fistula. Urology. 2003;61:458–9.
Ciftci AO, Şenocak ME, Büyükpamukçu N. Male gender assignment in penile agenesis: a case report and review of the literature. J Pediatr Surg. 1995;30:1358–60.
Carr MC, Benacerraf BR, Mandell J. Prenatal diagnosis of an XY fetus with aphallia and cloacal exstrophy variant. J Ultrasound Med. 1994;13:323–5.
Skoog SJ, Barry BA. Aphallia: its classification and management. J Urol. 1989;141:589–92.
Puri A, Saxena R. Re: Willihnganz-Lawson et al.: De Castro technique used to create neophallus: a case of aphallia (Urology 2012;79:1149-1151). Urology. 2012;80:1165–6.
Gabler T, Charlton R, Loveland J, et al. Aphallia: a review to standardize management. Pediatr Surg Int. 2018;34:813–21.
Lumen N, Monstrey S, Selvaggi G, et al. Phalloplasty: a valuable treatment for males with penile insufficiency. Urology. 2008;71:272–6.
Acknowledgements
Not applicable.
Funding
This study did not receive any sources of funding.
Author information
Authors and Affiliations
Contributions
P.Y., P.E.Y., Y.Z., J.A.T. contribution to conceptualization, methodology, and supervision. P.Y and E.T.P.U. performed data curation and investigation. P.Y., P.E.Y., Y.Z., J.A.T., and E.T.P.U. were major contributors to writing the manuscript. All authors agreed on the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yuri, P., Yunir, P.E., Utama, E.T.P. et al. Aphallia - congenital absence of the penis: a systematic review. BMC Urol 24, 75 (2024). https://doi.org/10.1186/s12894-024-01445-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12894-024-01445-4