
Abstract
Background
Studies comparing the effectiveness of arthroscopic knee surgery and conservative treatment on knee osteoarthritis (OA) came up with inconsistent results. Systematic review on this topic still is still lacking. This systematic review and meta-analysis aimed to evaluate the effectiveness of arthroscopic knee surgery on knee OA, compared to conservative treatments.
Materials and methods
Literature searches were performed in PubMed, Embase, and Cochrane Library databases for randomized controlled trials (RCTs) published before on 1st July 2024. Studies comparing the effectiveness of arthroscopy and conservative treatments only on knee OA were included. Quality of included studies was evaluated by risk of bias 2 (ROB2). Long-term results in terms of pain relief, functional recovery and patients reported satisfaction were meta-analyzed to evaluate the therapeutic effectiveness.
Results
Ten studies were included in this review, among which only 1 was considered as low risk of bias. Five studies were involved in meta-analyses and no difference was found in therapeutic effectiveness of arthroscopic surgery and conservative treatment on knee OA, in the evaluation of VAS (p = 0.63), WOMAC (p = 0.38), SF-36 (p = 0.74) and patient satisfaction (p = 0.07).
Conclusion
The evidence does not support the effectiveness of arthroscopic knee surgery compared to conservative treatments in knee OA.
Similar content being viewed by others


Introduction
Osteoarthritis (OA) is a chronic degenerative joint disease characterized by the progressive breakdown of joint cartilage, leading to joint pain, stiffness, and functional impairment. It is the most common form of arthritis, affecting millions of people worldwide [1]. Although there is a worldwide trend showing a significant increase in the incidence of OA among younger patients, it affects the elderly most [2]. OA can affect any joint in the body but is most commonly found in the knee [3]. The pathogenesis of OA is complex and not yet fully understood. However, current research suggests that the development and progression of OA are influenced by a combination of genetic, environmental, and mechanical factors [4, 5]. These factors can lead to the loss of chondrocytes and the extracellular matrix through different mechanisms, including mechanical, inflammatory, and metabolic, ultimately causing OA [5,6,7,8].
Diagnosis of knee OA typically involves a combination of patient history, physical examinations and imaging. Among auxiliary examinations, X-ray is most commonly used. The progression of OA can be evaluated using the Kellgren-Lawrence grading system, a widely used radiographic classification system, based on a scale of 0–4, with higher grades indicating more severe joint damage [5, 9, 10].
The management of knee OA aims to reduce pain, improve function, and prevent further joint damage [5]. This can involve a combination of non-pharmacologic interventions such as exercise, weight loss, and physical therapy, as well as pharmacologic interventions such as nonsteroidal anti-inflammatory drugs (NSAIDs) and analgesics [11, 12]. In advanced cases, surgical interventions may be necessary, with total knee arthroplasty (TKA) and unicompartmental knee arthroplasty (UKA) being the most common. However, both techniques are invasive, and should be considered last-resort treatments for knee OA [13, 14].
Arthroscopy is a minimally invasive surgical technique that can remove loose bodies or inflamed synovial tissue contributing to pain and inflammation in the knee joint. It can also be used to repair or remove damaged cartilage or bone [15,16,17]. However, its effectiveness is debated compared to non-surgical treatments. Kirkley conducted a randomized controlled trial (RCT) and found that arthroscopy was no more effective than placebo surgery in improving pain or function in patients with knee OA [18]. Other RCTs, however, have supported the therapeutic effectiveness of arthroscopy in treating degenerative knee OA [19, 20]. Even systematic reviews have reached different conclusions on the topic [21, 22]. The most recent systematic reviews and meta-analysis concluded that arthroscopic surgery provided little or no clinically important benefit in pain, function and knee-specific quality of life compared with a placebo procedure [22]. However, the study included participants with degenerative knee disease, encompassing knee OA and meniscal tears, which means studies recruiting patients without OA were also included. Strictly speaking, the conclusion could only be applied to degenerative knee diseases, leaving the effectiveness of arthroscopy on OA unresolved. Therefore, the present study aims to evaluate the effectiveness of arthroscopy on knee OA compared to any conservative treatment systematically.
Materials and methods
The work was conducted following the instructions of the Cochrane Handbook for Systematic Reviews and reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement [23, 24]. The review protocol was prospectively registered on PROSPERO (ID: CRD42022379604).
Inclusion and exclusion criteria
As the study focused on the effectiveness of arthroscopy for knee OA, the inclusion criteria were as follows: (1) participants were diagnosed with knee OA; (2) Studies were RCTs or quasi-RCTs comparing arthroscopic surgery with any other non-surgical treatments or placebo; (3) Outcome measurements focused on the treatment effectiveness, with at least one of the two important symptoms, pain and joint function, included.
The exclusion criteria were as follows: (1) Studies that included patients with Kellgren-Lawrence grade 0; (2) Studies involving patients with other serious knee diseases, such as cruciate ligament injury; (3) Studies conducted on animals or cadaveric specimens; (4) Conference abstract or protocols of unfinished studies.
Search strategy
Articles published in PubMed, Embase and the Cochrane Library in English were searched without any time restriction. The search terms included debridement, lavage, knee, osteoarthritis, arthroscopy, RCT and arthroscopic. The literature search was last performed on 1st July 2024. The detailed search strategy is provided as supplemental material 1.
The search results were imported into Endnote software by one of the authors, and duplicates were removed after manual checking. Two authors independently scanned the titles and abstracts, to exclude articles that clearly did not meet our eligibility criteria. The remaining studies were then read in full text. In cases where the two authors had differing views, they first discussed the discrepancies. If they still could not reach an agreement, a senior author made the final decision.
Data extraction
Data extraction from the included studies was conducted independently by two authors. The extracted data included author, year, the number, gender and age of patients, interventions, outcomes and the longest follow up times. Since OA is a chronic disease, for each outcome measure, data from the longest time point was extracted.
Risk of bias assessment
The risk of bias in the included studies was evaluated using the ROB 2 recommended by Cochrane. This evaluation was conducted independently by two authors, who then crosschecked each other’s assessments. Any discrepancies were first discussed between the two authors, and if they still could not reach an agreement, a senior author made the final decision.
Outcomes and statistical analysis
The preset outcomes were pain relief, functional improvement, time to receive arthroplasty and patients-reported satisfaction. Among them, Visual Analogue Scale (VAS) for pain and Western Ontario and McMaster Universities Arthritis Index (WOMAC) were considered primary outcome measurements. Additionally, assessments such as Knee Injury and Osteoarthritis Outcome Score (KOOS), International Knee Documentation Committee (IKDC) score, Lysholm score, and the Short Form-36 (SF-36) were used to evaluate the functional recovery.
Meta-analyses were undertaken using RevMan V.5.4 to calculate the pooled effect, if an outcome measure was used by at least two included studies. For continuous variables, the mean difference (MD) and standard deviation (SD) of the studies were pooled using the inverse variance method. Since the full scores varied across, the full score for VAS was set as 10 while the full score for WOMAC was set as 100. If data transformation or normalization was done across different studies, the standard mean difference (SMD) was used instead of MD. For dichotomous data, the risk ratios (RR) were calculated. Statistical heterogeneity was tested using the I² test, with I² statistic of 0–50% representing low heterogeneity and 50–100% representing high heterogeneity. When I² < 50%, a fixed effects model was used, otherwise, a random effects model was used. Sensitivity analysis was performed by omitting each study to assess its influence on the pooled results when more than three studies were synthesized. Reporting bias was evaluated using the Egger test if an outcome included more than 10 studies. For all data synthesis, confidence intervals (CIs) were set at 95%, and p < 0.05 was considered statistically significant.
Results
Searching and selection results
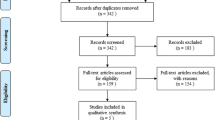
The initial search identified 1281 records. After removing duplicates, we screened 879 records. We retrieved 37 studies for full-text screening, of which 10 met our inclusion criteria and were included. Some studies were excluded because their study cohorts included patients without OA or patients with Kellgren-Lawrence grade zero [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48]. Additionally, some studies were excluded because they were health economics studies, imaging studies or lacked predefined outcome assessments [33, 49, 50]. Study that performed arthroscopy in both treatment and control group was also excluded [51]. The results of the search are shown in Fig. 1.

Flow chart of literature search
Characteristics of included studies
All ten included studies were parallel-group RCTs conducted between 1993 and 2023 [18,19,20, 52,53,54,55,56,57,58]. Moseley conducted 2 trials with the first being a pilot study for the latter one. Since the two studies did not share data, both were included. These studies were conducted in veteran affairs medical centers, resulting in a male predominance among their subjects [54, 55]. In contrast, female subjects outnumbered males in all other studies.
The arthroscopic surgery in these studies primarily included debridement, meniscectomy, synovectomy, lavage, microfracture, and removal of loose bodies. The control methods included physical therapy, platelet-rich plasma (PRP) or hyalgan injections, nonsteroidal anti-inflammatory drugs (NSAIDs) and sham surgery. The follow-up time ranged from 6 to 36 months, except for Zhang’s study, which did not provide an exact follow-up duration [19].
Outcome measurements varied among the studies, and some preset assessments in our study protocol, such as IKDC, Lysholm scores and time to receive arthroplasty, were not used in any of the studies, and thus will not be reported below. Subgroup analysis and publication bias will also not be shown, as the conditions for these analyses were not met according to our protocol. The characteristics of the included studies are presented in Table 1.
Risk of bias
Only one study was assessed as having a low risk of bias [18]. Most studies were evaluated as having a high risk of bias in measurement of outcome due to the differences in intervention methods, which made blinding of assessor difficult. However, two studies managed to achieve low risk in this section by covering the arthroscopy scars during assessment. In contrast, Merchan’s study used homogeneous baseline data derived from data after the removal of late deaths, which is a statistically incorrect method [20]. According to the instruction of ROB 2, this study was evaluated as having a high risk in this section. All studies reported nearly all data in every cluster, so in missing data section, all studies were evaluated as low risk. The detailed risk of bias assessment is shown in Fig. 2.

Summary of risk of bias of included studies
Pain relief
All studies reported the effectiveness of arthroscopy on pain relief, though the scales they used differed. However, Moseley [55] and Saeed [57] did not perform statistical analyses, and Merchan [20] and Zhang [19] did not evaluated the effectiveness on pain relief in a separate scale. Among these studies, only Singh found a significantly better pain relief in PRP injection group compared to the arthroscopy group at a 9-month follow-up, while the other studies did not show any significant advantages of arthroscopy over non-surgical treatments in terms of pain relief. The synthesis results of available data did not support the superiority of either of arthroscopy or conservative treatments (p = 0.63), with a statistical heterogeneity of 81%. The forest plot is shown in Fig. 3. Additionally, the meta-analysis of pain scores passed the sensitive analysis.

Forest plot of pooled analysis of pain scores
Functional recovery
Among the included studies, Saeed’s was the only one that did not evaluate functional recovery [57]. Moseley did not perform statistical analyses in his pilot study [55]. Merchan compared the effectiveness of arthroscopic surgery and conservative treatment using a knee rating score mainly based mainly on range of motion and ambulation, concluding that arthroscopic treatment was more effective [20]. Zhang reached a similar result in favor of arthroscopy using HSS as the assessing tool [19]. The conventional methods in both studies were mainly medical treatments. However, Singh’s study demonstrated that PRP injection seemed to have an edge over arthroscopic surgery, as concluded from the WOMAC scores, particularly in patients with OA of Kellgren-Lawrence grading two [56]. In the other studies, no significant difference between arthroscopy and conventional therapy was found in terms of functional recovery, regardless of the scales used.
Meta analyses were performed based on the WOMSC (p = 0.38) and SF-36 (p = 0.74) assessments, with WOMAC preset as a primary outcome. No statistical significance was found in either synthesis, indicating similar therapeutic effectiveness of arthroscopy and conventional therapy in terms of functional recovery. The forest plots are shown in Fig. 4.

Forest plots of pooled analyses of (A) WOMAC scores and (B) SF-36
Patients’ satisfaction
Only 2 studies reported patients’ satisfaction as categorical variables. Moseley did not draw any conclusions, while Zhang reported a significantly higher satisfaction rate in the arthroscopy group compared to medical therapy [19, 55]. However, the pooled data showed no significant difference between the treatment methods (p = 0.07). The forest plot is shown in Fig. 5.

Pooled analysis of patients reported satisfaction
Discussion
This systematic review and meta-analysis searched 3 databases and identified 10 RCTs comparing the therapeutic effectiveness of arthroscopic surgery and conventional managements on OA. Although only one study ensured double-blinding and was evaluated as low risk of bias in the overall assessment, most studies used appropriate randomization methods. The results of data synthesis demonstrated that patients with OA did not benefit more from arthroscopy than from conventional managements in term of pain relief and function improvements. Additionally, patient-reported satisfaction with arthroscopy did not show an advantage over non-surgical therapy.
A previous meta-analysis indicated that arthroscopic knee surgery provided little or no clinically important benefit in pain or function in the short or longer term, and probably provided no clinically important benefit in knee-specific or generic quality of life, nor did it improve treatment success. This study included trials comparing arthroscopic surgery with placebo surgery or non-surgical treatment in people with degenerative knee disease, with most participants having OA or meniscus injury [22]. Unlike that study, our review included only patients with OA, though meniscus injury was acceptable. To ensure OA diagnosis was a required condition, we excluded studies including participants with Kellgren-Lawrence grading 0. Despite this more specific population, our study yielded similar results, concluding that arthroscopy should not be preferred over conservative treatment.
A recent systematic review demonstrated that arthroscopic debridement is effective in mild to moderate knee OA at short-term follow-up, which was inconsistent with our results. The discrepancy may be due to different inclusion and exclusion criteria. That study included all types of arthroscopic joint debridement for treating OA, while we only included RCTs. This resulted in a higher level of evidence for our results while a more comprehensive result for that study. In addition, the previous study did not conduct a quantitative meta-analysis, reducing the persuasiveness of their results [59].
Another study published in 2019 concluded that low-quality evidence from a few small trials indicated no benefit of arthroscopic surgery over other non-surgical treatments [60]. Although this study included participants similar to our review, both studies excluding patients with Kellgren-Lawrence grading 0, the results of selection differed. Kats’s study [25] was excluded in our review, since patients with Kellgren-Lawrence grading 0 were found in context, whereas the previous study mistakenly included it. In addition, the previous study researched more types of surgery, such as high tibial osteotomy, while our review focused solely on arthroscopy. Despite these differences, both studies did not support the advantages of arthroscopic surgery over conservative treatments, with our study drawing this conclusion based on more evidence.
Karpinski’s review did not provide a clear view, since quantitative analysis was not performed, and he cautioned that the results should be interpreted carefully since the use of other therapeutic variables such as painkillers or NSAIDs was not controlled in some RCTs [61]. They also included participants with only meniscus injury. Furthermore, systematic reviews and meta-analyses published more than five years ago are now outdated given the publication of new RCTs in recent years [16, 21, 62].
There were still some limitations in this study. First, the quantitative analyses were all based on limited data, and the small sample might reduce the accuracy of the results. The authors had expected numerous RCTs and data on this topic, but the search results were unexpectedly sparse. We cross-checked the searching results with the included studies of some previously published systematic reviews and confirmed the accuracy of our search, as no records were missed. Second, different articles used different assessments to evaluate the same outcomes, potentially leading to bias. The authors carefully reviewed the methods of each study to ensure homogeneity of the pooled data. Third, the protocol for this study was revised once in PROSPERO. However, the revision occurred before the literature search began, so the prospective design and the scientific nature of the study were not compromised. Fourth, the present study included only RCTs with homogeneous populations, limiting the generalizability of the results.
Despite these limitations, the study has its strength. First, as discussed, this study is unique, particularly in its population focus, and demonstrate that arthroscopy does not provide better treatment effectiveness than non-surgical treatment on patients with OA. Second, the basis for our conclusion is all RCTs, and the methodology used in this review is systematic, making this level 1 evidence. Third, quantitative analyses were performed whenever possible, providing credible results. Fourth, the study was registered on public sites, and all work was conducted according to the preset protocol, enhancing the reliability of the final results.
Conclusion
The evidence does not support the effectiveness of arthroscopic knee surgery compared to conservative treatments in knee OA.
Data availability
Data is availability through request to corresponding author.
References
Hawker GA, King LK. The Burden of Osteoarthritis in older adults. Clin Geriatr Med. 2022;38(2):181–92.
Price AJ, Alvand A, Troelsen A, Katz JN, Hooper G, Gray A, Carr A, Beard D. Knee replacement. Lancet (London England). 2018;392(10158):1672–82.
Giorgino R, Albano D, Fusco S, Peretti GM, Mangiavini L, Messina C. Knee osteoarthritis: Epidemiology, Pathogenesis, and mesenchymal stem cells: what else is New? An update. Int J Mol Sci 2023, 24(7).
Jiang Y. Osteoarthritis year in review 2021: biology. Osteoarthritis Cartilage. 2022;30(2):207–15.
Hunter DJ, Bierma-Zeinstra S, Osteoarthritis. Lancet (London England). 2019;393(10182):1745–59.
Creamer P, Lethbridge-Cejku M, Hochberg MC. Where does it hurt? Pain localization in osteoarthritis of the knee. Osteoarthritis Cartilage. 1998;6(5):318–23.
Bortoluzzi A, Furini F, Scirè CA. Osteoarthritis and its management - epidemiology, nutritional aspects and environmental factors. Autoimmun rev. 2018;17(11):1097–104.
Zhang Y, Jordan JM. Epidemiology of osteoarthritis. Clin Geriatr Med. 2010;26(3):355–69.
Kohn MD, Sassoon AA, Fernando ND. Classifications in brief: Kellgren-Lawrence classification of Osteoarthritis. Clin Orthop Relat Res. 2016;474(8):1886–93.
Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502.
Block JA. Osteoarthritis: OA guidelines: improving care or merely codifying practice? Nat Rev Rheumatol. 2014;10(6):324–6.
Nelson AE, Allen KD, Golightly YM, Goode AP, Jordan JM. A systematic review of recommendations and guidelines for the management of osteoarthritis: the chronic osteoarthritis management initiative of the U.S. bone and joint initiative. Semin Arthritis Rheum. 2014;43(6):701–12.
Higashi H, Barendregt JJ. Cost-effectiveness of total hip and knee replacements for the Australian population with osteoarthritis: discrete-event simulation model. PLoS ONE. 2011;6(9):e25403.
Wylde V, Hewlett S, Learmonth ID, Dieppe P. Persistent pain after joint replacement: prevalence, sensory qualities, and postoperative determinants. Pain. 2011;152(3):566–72.
Reichenbach S, Rutjes AW, Nüesch E, Trelle S, Jüni P. Joint lavage for osteoarthritis of the knee. Cochrane Database Syst Rev 2010(5):Cd007320.
Brignardello-Petersen R, Guyatt GH, Buchbinder R, Poolman RW, Schandelmaier S, Chang Y, Sadeghirad B, Evaniew N, Vandvik PO. Knee arthroscopy versus conservative management in patients with degenerative knee disease: a systematic review. BMJ Open. 2017;7(5):e016114.
Mao B, Pan Y, Zhang Z, Yu Z, Li J, Fu W. Efficacy and safety of Hyaluronic Acid intra-articular injection after arthroscopic knee surgery: a systematic review and Meta-analysis. Orthop Surg. 2023;15(1):16–27.
Kirkley A, Birmingham TB, Litchfield RB, Giffin JR, Willits KR, Wong CJ, Feagan BG, Donner A, Griffin SH, D’Ascanio LM, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2008;359(11):1097–107.
Zhang YF, Liu H. Clinical efficacy of knee arthroscopy in the treatment of degenerative knee osteoarthritis. Biomedical Res (India). 2018;29(5):958–61.
Merchan EC, Galindo E. Arthroscope-guided surgery versus nonoperative treatment for limited degenerative osteoarthritis of the femorotibial joint in patients over 50 years of age: a prospective comparative study. Arthroscopy. 1993;9(6):663–7.
Spahn G, Hofmann GO, Klinger HM. The effects of arthroscopic joint debridement in the knee osteoarthritis: results of a meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2013;21(7):1553–61.
O’Connor D, Johnston RV, Brignardello-Petersen R, Poolman RW, Cyril S, Vandvik PO, Buchbinder R. Arthroscopic surgery for degenerative knee disease (osteoarthritis including degenerative meniscal tears). Cochrane Database Syst Rev. 2022;3(3):Cd014328.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906.
Higgins JPTTJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database of Systematic Reviews; 2023.
Katz JN, Brophy RH, Chaisson CE, de Chaves L, Cole BJ, Dahm DL, Donnell-Fink LA, Guermazi A, Haas AK, Jones MH, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013;368(18):1675–84.
Vermesan D, Prejbeanu R, Laitin S, Damian G, Deleanu B, Abbinante A, Flace P, Cagiano R. Arthroscopic debridement compared to intra-articular steroids in treating degenerative medial meniscal tears. Eur Rev Med Pharmacol Sci. 2013;17(23):3192–6.
Gauffin H, Tagesson S, Meunier A, Magnusson H, Kvist J. Knee arthroscopic surgery is beneficial to middle-aged patients with meniscal symptoms: a prospective, randomised, single-blinded study. Osteoarthr Cartil. 2014;22(11):1808–16.
Aae TF, Randsborg PH, Breen AB, Visnes H, Vindfeld S, Sivertsen EA, Løken S, Brinchmann J, Hanvold HA, Årøen A. Norwegican cartilage project - a study protocol for a double-blinded randomized controlled trial comparing arthroscopic microfracture with arthroscopic debridement in focal cartilage defects in the knee. BMC Musculoskelet Disord. 2016;17:292.
Berg B, Roos EM, Englund M, Kise NJ, Tiulpin A, Saarakkala S, Engebretsen L, Eftang CN, Holm I, Risberg MA. Development of osteoarthritis in patients with degenerative meniscal tears treated with exercise therapy or surgery: a randomized controlled trial. Osteoarthr Cartil. 2020;28(7):897–906.
van der Graaff SJA, Eijgenraam SM, Meuffels DE, van Es EM, Verhaar JAN, Hofstee DJ, Auw Yang KG, Noorduyn JCA, van Arkel ERA, van den Brand I, et al. Arthroscopic partial meniscectomy versus physical therapy for traumatic meniscal tears in a young study population: a randomised controlled trial. Br J Sports Med. 2022;56(15):870–6.
Noorduyn JCA, van de Graaf VA, Willigenburg NW, Scholten-Peeters GGM, Kret EJ, van Dijk RA, Buchbinder R, Hawker GA, Coppieters MW, Poolman RW. Effect of physical therapy vs arthroscopic partial meniscectomy in people with degenerative meniscal tears: five-year follow-up of the ESCAPE Randomized Clinical Trial. JAMA Netw open. 2022;5(7):e2220394.
Sonesson S, Kvist J, Yakob J, Hedevik H, Gauffin H. Knee arthroscopic surgery in Middle-aged patients with meniscal symptoms: a 5-Year follow-up of a prospective, randomized study. Orthop J Sports Med 2020, 8(1).
Ma N, Wang H, Xu X, Wan Y, Liu Y, Wang M, Yu W, Dai Y, Peng J, Guo Q, et al. Autologous-cell-derived, tissue-engineered cartilage for repairing articular cartilage lesions in the knee: study protocol for a randomized controlled trial. Trials. 2017;18(1):519.
Randsborg PH, Brinchmann J, Løken S, Hanvold HA, Aae TF, Årøen A. Focal cartilage defects in the knee - a randomized controlled trial comparing autologous chondrocyte implantation with arthroscopic debridement. BMC Musculoskelet Disord. 2016;17:117.
Kise NJ, Risberg MA, Stensrud S, Ranstam J, Engebretsen L, Roos EM. Exercise therapy versus arthroscopic partial meniscectomy for degenerative meniscal tear in middle aged patients: randomised controlled trial with two year follow-up. BMJ (Clinical Res ed). 2016;354:i3740.
Stensrud S, Risberg MA, Roos EM. Effect of exercise therapy compared with arthroscopic surgery on knee muscle strength and functional performance in middle-aged patients with degenerative meniscus tears: a 3-mo follow-up of a randomized controlled trial. Am J Phys Med Rehabil. 2015;94(6):460–73.
Sihvonen R, Paavola M, Malmivaara A, Itälä A, Joukainen A, Nurmi H, Kalske J, Järvinen TL. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369(26):2515–24.
Herrlin SV, Wange PO, Lapidus G, Hallander M, Werner S, Weidenhielm L. Is arthroscopic surgery beneficial in treating non-traumatic, degenerative medial meniscal tears? A five year follow-up. Knee Surg Sports Traumatol Arthrosc. 2013;21(2):358–64.
Herrlin S, Hållander M, Wange P, Weidenhielm L, Werner S. Arthroscopic or conservative treatment of degenerative medial meniscal tears: a prospective randomised trial. Knee Surg Sports Traumatol Arthrosc. 2007;15(4):393–401.
Hubbard MJ. Articular debridement versus washout for degeneration of the medial femoral condyle. A five-year study. J bone Joint Surg Br Volume. 1996;78(2):217–9.
Yim J-H, Seon J-K, Song E-K, Choi J-I, Kim M-C, Lee K-B, Seo H-Y. A comparative study of Meniscectomy and Nonoperative Treatment for degenerative horizontal tears of the medial Meniscus. Am J Sports Med. 2013;41(7):1565–70.
Østerås H, Østerås B, Torstensen TA. Medical exercise therapy, and not arthroscopic surgery, resulted in decreased depression and anxiety in patients with degenerative meniscus injury. J Bodyw Mov Ther. 2012;16(4):456–63.
Katz JN, Collins JE, Jones MH, Losina E, Marx RG, Guermazi A, Spindler KP, Cole BJ, MacFarlane LA, Selzer F, et al. Radiographic Changes following Surgical and Non-surgical Treatment for degenerative meniscal tear. Osteoarthr Cartil. 2023;31:S46.
Damsted C, Skou ST, Hölmich P, Lind M, Varnum C, Jensen HP, Hansen MS, Thorlund JB. Early surgery Versus Exercise Therapy and Patient Education for traumatic and nontraumatic meniscal tears in young Adults-An exploratory analysis from the DREAM Trial. J Orthop Sports Phys Ther. 2024;54(5):1–10.
Clausen SH, Skou ST, Boesen MP, Radev DI, Kurt EY, Damsted C, Holmich P, Lind M, Torring S, Isaksen C, et al. Two-year MRI-defined structural damage and patient-reported outcomes following surgery or exercise for meniscal tears in young adults. Br J Sports Med. 2023;57(24):1566–72.
Kalske R, Kiadaliri A, Sihvonen R, Englund M, Turkiewicz A, Paavola M, Malmivaara A, Itala A, Joukainen A, Nurmi H et al. Arthroscopic Partial Meniscectomy for a Degenerative Meniscus Tear Is Not Cost Effective Compared With Placebo Surgery: An Economic Evaluation Based on the FIDELITY Trial Data. Clinical orthopaedics and related research : 2024, 07.
Sihvonen R, Paavola M, Malmivaara A, Itälä A, Joukainen A, Kalske J, Nurmi H, Kumm J, Sillanpää N, Kiekara T, et al. Arthroscopic partial meniscectomy for a degenerative meniscus tear: a 5 year follow-up of the placebo-surgery controlled FIDELITY (Finnish degenerative Meniscus lesion study) trial. Br J Sports Med. 2020;54(22):1332–9.
Katz JN, Shrestha S, Losina E, Jones MH, Marx RG, Mandl LA, Levy BA, MacFarlane LA, Spindler KP, Silva GS, et al. Five-year outcome of operative and Nonoperative Management of Meniscal Tear in persons older Than forty-five years. Arthritis Rheumatol (Hoboken NJ). 2020;72(2):273–81.
Collins JE, Losina E, Marx RG, Guermazi A, Jarraya M, Jones MH, Levy BA, Mandl LA, Martin SD, Wright RW, et al. Early magnetic resonance imaging-based changes in patients with Meniscal tear and Osteoarthritis: eighteen-Month Data from a Randomized Controlled Trial of Arthroscopic partial meniscectomy Versus Physical Therapy. Arthritis Care Res (Hoboken). 2020;72(5):630–40.
Birmingham TB, Primeau CA, Shariff SZ, Reid JNS, Marsh JD, Lam M, Dixon SN, Giffin JR, Willits KR, Litchfield RB, et al. Incidence of total knee arthroplasty after arthroscopic surgery for knee osteoarthritis: a secondary analysis of a Randomized Clinical Trial. JAMA Netw open. 2024;7(4):e246578.
Wu CZ, Shi ZY, Chen JL, Wang PE, Yuan WH, Jin HT, Tong PJ, Wu Z, Lin WJ, Chen WB, et al. Mid-term outcomes of microfragmented adipose tissue plus arthroscopic surgery for knee osteoarthritis: a randomized, activecontrol, multicenter clinical trial. World J stem Cells. 2023;15(12):1063–76.
Chang RW, Falconer J, Stulberg SD, Arnold WJ, Manheim LM, Dyer AR. A randomized, controlled trial of arthroscopic surgery versus closed-needle joint lavage for patients with osteoarthritis of the knee. Arthritis Rheum. 1993;36(3):289–96.
Forster MC, Straw R. A prospective randomised trial comparing intra-articular hyalgan injection and arthroscopic washout for knee osteoarthritis. Knee. 2003;10(3):291–3.
Moseley JB, O’Malley K, Petersen NJ, Menke TJ, Brody BA, Kuykendall DH, Hollingsworth JC, Ashton CM, Wray NP. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002;347(2):81–8.
Moseley JB, Wray NP, Kuykendall D, Willis K, Landon G. Arthroscopic treatment of osteoarthritis of the knee: a prospective, randomized, placebo-controlled trial. Results of a pilot study. Am J Sports Med. 1996;24(1):28–34.
Singh N, Trivedi V, Kumar V, Mishra NK, Ahmad S, Ayar SJ, Kataria SS, Kharbanda H. A comparative study of osteoarthritis knee arthroscopy versus intra-articular platelet Rich plasma injection: a Randomised Study. Malaysian Orthop J. 2022;16(2):31–40.
Saeed K, Khan SA, Ahmed IJPJMHS. Efficacy of intra articular hyaluronic acid versus arthroscopic debridement in terms of improvement in pain score in Kellgran-Lawrence Grading II & III osteoarthritis of knee joint. 2015, 9:1011–5.
Agarwal N, Ostwal AA. Comparative effectiveness of knee arthroscopy Versus Intra-articular platelet Rich plasma injection for Osteoarthritis of the knee: a randomized study. Int J Pharm Clin Res. 2023;15(7):830–3.
Cotter EJ, Weissman AC, Yazdi AA, Muth SA, Cole BJ. Arthroscopic debridement of mild and moderate knee osteoarthritis results in clinical improvement at short-term Follow-Up: a systematic review. Arthroscopy Journal of Arthroscopic and Related Surgery; 2024.
Palmer JS, Monk AP, Hopewell S, Bayliss LE, Jackson W, Beard DJ, Price AJ. Surgical interventions for symptomatic mild to moderate knee osteoarthritis. Cochrane Database Syst Rev. 2019;7(7):Cd012128.
Karpinski K, Müller-Rath R, Niemeyer P, Angele P, Petersen W. Subgroups of patients with osteoarthritis and medial meniscus tear or crystal arthropathy benefit from arthroscopic treatment. Knee Surg Sports Traumatol Arthrosc. 2019;27(3):782–96.
Thorlund JB, Juhl CB, Roos EM, Lohmander LS. Arthroscopic surgery for degenerative knee: systematic review and meta-analysis of benefits and harms. BMJ. 2015;350:h2747.
Funding
The work was funded by Guangdong Basic and Applied Basic Research Foundation (2023A1515110336).
Author information
Authors and Affiliations
Contributions
Conceptualization: Zhong Zhang, Beini Mao and Yijian Liang; searching, selection and data extraction: Zhong Zhang, Zhengjun Hu and Beini Mao; data synthesis: Zhong Zhang, Deng Zhao and Huaqiang Huan; interpretation of results: Zhong Zhang, Beini Mao and Yijian Liang; draft preparation: Zhong Zhang and Yijian Liang; revision: Zhong Zhang and Beini Mao.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, Z., Hu, Z., Zhao, D. et al. Arthroscopic surgery is not superior to conservative treatment in knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trails. BMC Musculoskelet Disord 25, 712 (2024). https://doi.org/10.1186/s12891-024-07813-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07813-3