
Abstract
Background
Older subjects have a higher risk for vertebral compression fracture. Maintaining a higher bone mineral density (BMD) at this age can protect individuals from osteoporosis-related events. Body mass index (BMI) has been found to have a robust association with BMD. However, excessive BMI is detrimental to bone health and may cause systemic disorders. Therefore, the present study aimed to determine the association between BMI and BMD, and identify a reasonable BMI range.
Methods
A total of 961 participants were recruited from community-dwelling residents between August 2021 and May 2022. A weighted multivariate linear regression model was applied to identify the relationship between BMI and BMD. Meanwhile, subgroup stratified analysis by BMI quartile and gender was also performed. A non-linear relationship and threshold value were determined based on the smooth curve fittings and threshold effects analysis model.
Results
A robust relationship was found between BMI and BMD, which remained significant in subgroups stratified by gender and BMI quartile. The BMI inflection point values in lumbar BMD and femoral neck BMD were 25.2 kg/m2 and 27.3 kg/m2, respectively. For individuals with BMI < 25.2 kg/m2, an increase in BMI was related to an increase in lumbar BMD. For BMI > 25.2 kg/m2, an increase in BMI was associated with a decrease in lumbar BMD. For subjects with BMI < 27.3 kg/m2, the femoral neck BMD rose by 0.008 kg/m2 for each unit rise in BMI. However, when BMI exceeded 27.3 kg/m2, the femoral neck BMD increased only by 0.005 kg/m2. Fracture risk assessment based on the spinal deformity index (SDI) failed to determine the optimal BMI range.
Conclusions
This study found an inflection point between BMI and lumbar/ femoral neck BMD in older community-dwelling subjects. An appropriate BMI but not an excessive BMI may allow older adults to have a better BMD.
Similar content being viewed by others


Introduction
Osteoporosis is a systemic skeletal metabolic disorder characterized by a low bone mass density (BMD) and microarchitectural deterioration of bone tissue, with an increased risk of fragility fractures [1, 2]. An epidemiological survey on osteoporosis released by the National Health Commission in 2018 showed that the prevalence of osteoporosis among individuals over 65 years old was 32.0% (10.7% in males and 51.6% in females). By 2050, 533 million people in China are expected to suffer from bone loss or osteoporosis.
Obesity has emerged as a major public health issue that affects numerous people worldwide [2, 3]. Body mass index (BMI) is commonly used to assess overall obesity. However, although there may be an overall positive relationship between BMI and BMD across the entire population, obesity is generally considered detrimental to bone mass [4, 5]. In addition, studies that have examined the effects of BMI on BMD and the existence of a threshold effect are insufficient and contentious [1, 6]. Some studies have demonstrated that high BMI protects against osteoporosis, while others seem to contradict this finding [6, 7]. Evidence suggests that although obesity is associated with higher BMD, it may be less protective against fracture than previously assumed, and excessive BMI may be associated with other systemic disorders. Therefore, balancing a healthy BMI and a higher BMD is critical.
The present study sought to determine whether a curve exists between BMI and BMD and to identify a reasonable BMI range in community-dwelling older adults over 60. We hypothesized that BMI has an inflection point and that maintaining BMI at this point would result in the best balance between BMI and BMD. The present study can serve as a guideline for reducing the incidence of osteoporosis-related adverse events while maintaining BMI at a reasonable range in community-dwelling older adults.
Materials and methods
Participants
This cross-sectional study was conducted after approval from the institutional review board at Xuanwu Hospital Capital Medical University (2018086). The inclusion criteria were as follows:
-
1.
Aged ≥ 60 years.
-
2.
Dwelling in the local community for at least five years.
-
3.
Voluntary participation (with informed consent).
We excluded subjects with the following:
-
1.
A history of spinal surgery.
-
2.
Mental illness, disability, or communication barriers.
-
3.
Inability to cooperate.
-
4.
Incomplete clinical data.
-
5.
Diagnosis of ankylosing spondylitis.
The present study is a secondary analysis of a broader study designed to explore the epidemiological characteristics of skeletal system degeneration in older adults. A total of 1250 participants were recruited between August 2021 and May 2022, of whom 961 met the inclusion criteria. Of the 289 excluded subjects, 49 had missing BMI information, 104 had missing BMD information, 78 had missing radiography information, and 58 had ankylosing spondylitis.
Study variables
Each subject was required to complete a detailed questionnaire on demographic characteristics and lifestyle information about alcohol consumption, smoking status, daily exercise, and medication history, particularly glucocorticoids and anti-osteoporosis drugs. Physical activity was assessed using the rating of perceived exertion, which divides exercise intensity into a scale of 1–20 with > 12 indicating moderate intensity and above. A history of glucocorticoid use was defined as regular use of medicine for more than three months, while a history of anti-osteoporosis drug use was defined as periodic use of medicine for more than six months. Other variables included age, sex, weight, height, education level, hypertension status, diabetes status, tooth loss status, and waist circumference, which were recorded based on recent measurements reported by the subjects. The key variables were BMI (independent variable) and BMD (dependent variable). The respondents’ height and weight were measured with shoes and any heavy clothing removed. BMI was calculated as weight in kilograms divided by height in metres squared. Lumbar and femoral neck BMD were measured using dual-energy X-ray absorptiometry. Lumbar and femoral neck BMD were calculated as the mean BMD of the lumbar spine (L1 to L4) and the bilateral femoral neck, respectively. Full-length spinal radiographs were obtained according to standard procedure. To determine the rationality of the current results, semiquantitative visual assessment of each vertebra from T4 to L4 was performed by two trained resident doctors. The chief physician made the final decision when the grading results were inconsistent. The spinal deformity index (SDI) is a summary measure of the vertebral fracture status of the spine that incorporates both the number and severity of vertebral fractures [8]. For each vertebra, a visual semiquantitative grade of 0, 1, 2, or 3 is assigned for no fracture or mild, moderate, or severe fracture, respectively, and the SDI is calculated by summing the fracture grades of all vertebrae (T4 to L4) [9, 10]. Stratification by BMI threshold and the difference in the SDI between groups were compared to determine the appropriate range for BMI.
Statistical analysis
Continuous variables are expressed as means ± standard deviations and were analysed using two independent-sample t tests if they were normally distributed. Categorical variables are presented as percentages and were analysed using the chi-square test. To simulate the linear relationship between BMI and BMD. First, we used BMI as a continuous independent variable, BMD as a dependent variable, and age, gender, education level, activity status, diabetes status, hypertension status, smoking status, alcohol consumption status, history of labour, tooth loss, history of glucocorticoid use and anti-osteoporosis drugs as covariates to explore the linear relationships between BMI and BMD. Then, we grouped the participants according to BMI quartiles. Quartile 1 of BMI was set as a dummy variable, and age, gender, education level, activity status, diabetes status, hypertension status, smoking status, drinking status, history of labour, tooth loss, and history of glucocorticoid and anti-osteoporosis drug use were set as covariates to further explore the linear relationships between the BMI quartiles and BMD. Finally, we explored the linear relationship between BMI and BMD based on subgroups stratified by gender after adjusting for covariates. Standardized regression coefficients (β) and 95% confidence intervals (CIs) were used to describe the data. To simulate the nonlinear relationship between BMI and BMD, smooth curve fittings were conducted to determine whether there was an inflection point between BMI and BMD. A threshold effects analysis model was used to determine the relationship and threshold between BMI and BMD. The interrater reliability was assessed using the interclass correlation coefficient. All analyses were performed using EmpowerStats (version: 2.0, X&Y Solutions, Inc., Boston, MA; http://www.empowerstats.com) and R software (version: 4.1.3), and statistical significance was set at p < 0.05.
Results
Baseline characteristics
A total of 961 participants, 371 males and 590 females, aged 60–83 years were included in the final analysis. The demographic characteristics of the participants are presented in Table 1. The BMI, waist circumference, lumbar BMD, and femoral neck BMD for men were 24.76 ± 3.87 kg/m2, 90.68 ± 10.54 cm, 1.05 ± 0.18 g/cm2, and 0.81 ± 0.12 g/cm2, respectively. In women, the respective values were 24.51 ± 3.34 kg/m2, 83.60 ± 8.51 cm, 1.01 ± 0.21 g/cm2, and 0.73 ± 0.14 g/cm2. Compared with female participants, male participants were more likely to have hypertension, diabetes, or tooth loss. Compared with female participants, male participants also had significantly higher levels of education, history of manual labour, moderate activity or above, smoking, drinking, waist circumference, and lumbar and femoral neck BMD and a lower proportion of history of glucocorticoid and anti-osteoporosis drug use.
Relationship between BMI and lumbar BMD
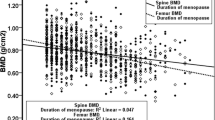
The weighted multivariate regression analysis of the relationship between BMI and lumbar BMD is displayed in Table 2. After adjusting for covariates, BMI was positively correlated with lumbar BMD (β = 0.007; 95% confidence interval (CI) 0.003–0.011; p = 0.001). Subgroup analysis stratified by sex revealed a positive correlation between BMI and lumbar BMD for both men (β = 0.008; 95% CI 0.001–0.014; p = 0.008) and women (β = 0.006; 95% CI 0.001–0.011; p = 0.007). Similarly, the results of subgroup analysis stratified by BMI quartile revealed a significant positive correlation between BMI and lumbar BMD. A BMI threshold of 25.2 kg/m2 was found at the inflection point after smooth curve fitting was performed to characterize the nonlinear relationship between BMI and lumbar BMD (Fig. 1). An increase in BMI was associated with an increase in lumbar BMD in individuals with BMI < 25.2 kg/m2 and a decrease in lumbar BMD in individuals with BMI > 25.2 kg/m2 (Table 3).

The association between body mass index and lumbar bone mineral density. The solid red line represents the smooth curve fitting between variables. Blue bands represents the 95% confidence interval from the fitting. age, gender, education level, activities status, diabetes, hypertension, smoking, drinking, history of labour, tooth loss, history of glucocorticoid and anti-osteoporosis drugs were adjusted
Relationship between BMI and femoral neck BMD
Table 2 shows the association between BMI and femoral neck BMD after adjusting for covariates. BMI was positively associated with femoral neck BMD (β = 0.005; 95% CI 0.002–0.007; p = 0.001). Subgroup analyses stratified by sex and BMI quartile also revealed a significant positive correlation between BMI and femoral neck BMD. After performing smooth curve fitting, we found that the BMI curve between BMI and femoral neck BMD differed (Fig. 2). Threshold effect analysis was employed to determine the BMI turning point, and a BMI of 27.3 kg/m2 for femoral neck BMD was identified. For subjects with BMI < 27.3 kg/m2, the femoral neck BMD increased by 0.008 kg/m2 for each unit increase in BMI. When BMI exceeded 27.3 kg/m2, the femoral neck BMD increased by only 0.005 kg/m2 (Table 3).

The association between body mass index and femoral neck bone mineral density. The solid red line represents the smooth curve fitting between variables. Blue bands represents the 95% confidence interval from the fitting. age, gender, education level, activities status, diabetes, hypertension, smoking, drinking, history of labour, tooth loss, history of glucocorticoid and anti-osteoporosis drugs were adjusted
SDI outcomes based on the BMI threshold
The interclass correlation coefficient was 0.908, suggesting excellent interrater reliability for the assessment results. Figures 3 and 4 indicate the SDI severity distribution according to the BMI inflection point for lumbar BMD and femoral neck BMD, respectively. There was a significant difference in the severity distribution between subjects with BMI ≤ 25.2 kg/m2 and those with a BMI > 25.2 kg/m2, ≤ 27.3 kg/m2, and > 27.3 kg/m2. When the subjects were grouped based on the BMI turning point in lumbar BMD, there was a significant difference in the severity distribution between the groups (Fig. 3). For individuals with a BMI ≤ 25.2 kg/m2, those with SDIs of 0, 1 and 2 accounted for 84.21%, 9.14%, and 6.65%, respectively. For individuals with BMI > 25.2 kg/m2, those with SDIs of 0, 1, 2, and 3 accounted for 76.12%, 12.45%, 9.95%, and 1.48%, respectively. When subjects were grouped according to the BMI turning point in femoral neck BMD, the difference in severity distribution remained significant (Fig. 4). For individuals with BMI ≤ 27.3 kg/m2, those with SDIs of 0, 1, 2, and 3 accounted for 85.14%, 9.88%, 4.32%, and 0.66%, respectively. For individuals with BMI > 27.3 kg/m2, those with SDIs of 0, 1, 2, and 3 accounted for 47.67%, 30.32%, 19.64%, and 2.37%, respectively.

The violin plot indicates the spinal deformity index distribution according to BMI saturation value for lumbar bone mineral density
* indicate that p < 0.05 between two groups

The violin plot indicates the spinal deformity index distribution according to BMI saturation value for femoral neck bone mineral density
* indicate that p < 0.05 between two groups
Discussion
The multivariate linear regression model revealed a significant positive correlation between BMI and BMD in community-dwelling older adults. The results of smooth curve fitting and threshold effect analysis demonstrated turning points between BMI, lumbar BMD, and femoral BMD.
Excessive BMI, namely, obesity and osteoporotic fractures, has become a severe public health concern worldwide. However, the relationship between BMI and fracture risk is controversial, necessitating a deep understanding of this relationship [6]. Li et al. [1] reported a significant positive association between BMI and lumbar BMD in all subgroup analyses after adjusting for covariates in a retrospective study based on the National Health and Examination Survey in America. Leslie et al. [11]. explored whether there is a more rapid rate of BMD loss in women with obesity and found a robust linear effect of increasing BMI on attenuated BMD loss at the lumbar spine. Similar results were reported by Zhang et al. [12]. , and a significant positive correlation was found between BMI and femoral neck BMD. However, an excessive BMI is associated with the risk of developing type 2 diabetes, nonalcoholic fatty liver disease, heart conditions, and obstructive sleep apnoea-hypopnea and may trigger an inflammatory response that could increase the possibility of osteoporosis and fragility fractures [12, 13]. Higher BMI, though, may be associated with a higher BMD within a specific range, while beyond this range, excessive BMI increases the risk of fracture. Therefore, overall BMI might be less protective against fracture than previously assumed [11]. Shen et al. [14]. conducted a cross-sectional study to determine the association between BMI and hip BMD and found that despite having more robust bones, men with obesity had a greater incidence of hip fracture. In a study investigating the effect of collinearity between BMI and BMD on fracture risk, Chan et al. [15]. demonstrated that greater BMI was associated with reduced fracture risk in men and women according to the univariate analysis. After adjusting for femoral neck BMD, however, higher BMI was associated with an increased risk of fracture. A mediated analysis showed that femoral neck BMD mediated the majority of the effect of BMI on fracture risk. These findings indicate that patients with higher BMI should have equally greater BMD because higher BMI alone may decrease the risk of fracture, while higher BMI but lower BMD increases the risk of fracture. In addition, it is important to note that the above studies are cross-sectional and comprehensive. Different associations may be present at different life stages. Therefore, prospective randomized controlled studies are needed to further validate the above results.
Our study revealed an inflection point between BMI and BMD, with a turning point at 25.2 kg/m2 for lumbar BMD and 27.3 kg/m2 for femoral neck BMD Excessive BMI (> 25.2 kg/m2) might negatively affect lumbar BMD. However, femoral neck BMD increased consistently even after BMI exceeded this practical value (27.3 kg/m2), and the magnitude of the increase decreased. In a study of a prediction model for osteoporotic vertebral compression fracture, Chanplakorn et al. [16]. reported that a lower femoral neck BMD was an independent risk factor for osteoporotic vertebral compression fracture. In addition, obesity might negatively affect other bone parameters, such as the trabecular bone score and composite indices of femoral neck strength [17,18,19]. It seems intricate to describe a reasonable BMI that achieves higher BMD between the lumbar and femoral neck. It is noteworthy that a higher BMI benefits lumbar BMD within a specific range, while beyond this range, a higher BMI increases the risk of fracture. Hence, the protective effect of BMI on BMD should not be exaggerated [20, 21]. Actually, the best way to evaluate the appropriate BMI was to conduct a prospective follow-up study, based on the follow-up data, to obtain the probability of fracture in different BMI samples, so as to determine the most appropriate BMI range. However, due to the lack of corresponding data, we tried to use SDI as an alternative way. As an assessment tool that integrates both the number and severity of fractures from T4-L4, the SDI allows a better fracture risk assessment, and the baseline SDI is also related to lumbar BMD [22]. Kerkeni et al. [22]. assessed the future risk of vertebral fracture in postmenopausal women and reported that the 3-year incidence of vertebral fracture among those with a baseline SDI < 2, 2 ≥ SDI < 4, and SDI ≥ 4 was 17.3 ± 3.6%, 25.4 ± 2.6%, and 47.6 ± 3.1%, respectively. According to the BMI inflection point for lumbar BMD, 93.35% and 6.65% of the participants had a BMI ≤ 25.2 kg/m2, while 88.57% and 11.43%, respectively, had a SDI < 2 and ≥ 2, respectively, for those with a BMI ≤ 25.2 kg/m2, while 88.57% and 11.43%, respectively, had a SDI ≥ 4. There was a significant difference in the severity distribution between patients with a BMI ≤ 25.2 kg/m2 and those with a BMI > 25.2 kg/m2. Moreover, when grouped according to the BMI inflection point for femoral neck BMD, patients with a SDI < 2 and 2 ≥ SDI < 4 accounted for 95.02% and 4.98%, respectively, of those with a BMI ≤ 27.3 kg/m2, while those with a SDI < 2 and 2 ≥ SDI < 4 accounted for 77.99% and 22.01%, respectively, of those with a BMI > 27.3 kg/m2. Similarly, there was a significant difference in the severity distribution between patients with a BMI ≤ 27.3 kg/m2 and those with a BMI > 27.3 kg/m2. To explore whether a BMI < 25.2 kg/m2 is more appropriate, as a BMI > 24 kg/m2 is considered overweight, and we want to keep the older population within a reasonable BMI range while maintaining a high BMD. Therefore, we compared the difference in SDI severity between patients with a BMI < 25.2 kg/m2 and those with a BMI < 27.3 kg/m2 to determine whether a BMI < 25.2 kg/m2 or < 27.3 kg/m2 was appropriate and more likely to reduce fracture risk. However, there was no significant difference in the severity distribution between patients with a BMI ≤ 25.2 kg/m2 and those with a BMI ≤ 27.3 kg/m2 (p = 0.552). Based on these findings, determining a reasonable range for BMI is difficult and warrants a prospective follow-up study.
Interestingly, different trends were observed between lumbar BMD and femoral neck BMD with increasing BMI. This suggests that other potential factors, including skeletal and nonskeletal mechanisms, are essential for explaining the present phenomenon [11, 23, 24]. One piece of evidence supporting this hypothesis is that weight loss interventions can lead to lumbar BMD loss over time but do not significantly affect femoral neck BMD loss [5, 11, 25].
Although the mechanism of maintaining the BMI inflection point and, hence, achieving optimal BMD remains unknown, it is likely to be multifactorial. One hypothesis holds that increased static mechanical compliance due to BMI accumulation causes axial static mechanical pressure and changes in the bone structure [4]. In addition, individuals with a higher BMI have greater synthesis and release of endocrine hormones such as oestrogen and insulin, which benefit BMD by inhibiting bone resorption and boosting bone remodelling [12]. Since osteoblasts and adipocytes are differentiated from mesenchymal stem cells, obesity can stimulate the development of mesenchymal stem cells into adipocytes [26, 27]. Inappropriate accumulation of bone marrow adipocytes in the skeletal system can lead to an imbalance in osteocyte activity and a reduction in bone turnover. This may explain the association between BMI and BMD. Another possible reason for the BMI inflection point is inflammation caused by obesity [25]. The proliferation of adipocytes in the bone marrow microenvironment hastens the release of proinflammatory and immunoregulatory substances, which accelerates the production and activation of osteoclasts [28, 29], while diminishing the differentiation of osteoblasts and inducing osteoclasts [28, 30]. However, using BMI to classify obesity does not directly assess adiposity. The evidence suggests that fat mass index is adverse to BMD in overweight and obese individuals, suggesting that an optimal BMI should be accompanied by a reasonable lean mass or lean body mass index rather than a higher fat mass index [2, 31].
The main strength of this study is the large sample size. Therefore, the present findings may serve as a guideline for community-dwelling older adults. However, there are some limitations in the present study. First, although DEXA is the current gold standard for evaluating lumbar vertebral quality, in patients with degenerative spinal conditions, the BMD and T score measured via DEXA may be elevated due to factors such as spinal scoliosis, degenerative joint disease, osteophyte formation, and sclerosis [32, 33], which may have affected the accuracy of the present study. Second, body composition was not considered in this study, which may affect the current results as lean body mass is thought to be positively associated with BMD. In contrast, fat content is negatively associated with BMD.
Conclusions
The present study revealed a strong positive correlation between BMI and lumbar/femoral neck BMD according to multivariate linear regression models. The threshold effect analysis showed that the BMI turning points were 25.2 kg/m2 and 27.3 kg/m2 for lumbar BMD and femoral neck BMD, respectively. Maintaining an appropriate but not excessive BMI may improve BMD. However, the different trends between lumbar BMD and femoral neck BMD with increasing BMI make it difficult to determine a reasonable range.
Data availability
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
body mass index
- BMD:
-
bone mineral density
- SDI:
-
spinal deformity index
References
Li Y. Association between obesity and bone mineral density in middle-aged adults. J Orthop Surg Res. 2022;17(1):268.
Kang DH, Guo LF, Guo T, et al. Association of body composition with bone mineral density in northern Chinese men by different criteria for obesity. J Endocrinol Invest. 2015;38(3):323–31.
Ouyang Y, Quan Y, Guo C et al. Saturation Effect of Body Mass Index on Bone Mineral Density in Adolescents of Different Ages: A Population-Based Study. Front Endocrinol (Lausanne). 2022; 13(922903.
Wang GX, Fang ZB, Li HL et al. Effect of obesity status on adolescent bone mineral density and saturation effect: A cross-sectional study. Front Endocrinol (Lausanne). 2022; 13(994406.
Zheng R, Byberg L, Larsson SC, et al. Prior loss of body mass index, low body mass index, and central obesity independently contribute to higher rates of fractures in elderly women and men. J Bone Min Res. 2021;36(7):1288–99.
Nielson CM, Marshall LM, Adams AL, et al. BMI and fracture risk in older men: the osteoporotic fractures in men study (MrOS). J Bone Miner Res. 2011;26(3):496–502.
Lopez-Gomez JJ, Perez-Castrillon JL, Garcia de Santos I et al. Influence of obesity on bone turnover markers and fracture risk in Postmenopausal Women. Nutrients. 2022; 14(8).
Harry K, Genant CY, Wu C, Van Kuuk et al. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res. 1993; 8(9).
Crans GG, Genant HK, Krege JH. Prognostic utility of a semiquantitative spinal deformity index. Bone. 2005;37(2):175–9.
Genant HK, Wu CY, van Kuijk C, et al. Vertebral fracture assessment using a semiquantitative technique. J Bone Min Res. 1993;8(9):1137–48.
Leslie WD, Morin SN, Majumdar SR, et al. Effects of obesity and diabetes on rate of bone density loss. Osteoporos Int. 2018;29(1):61–7.
Zhang Y, Pu J. The Saturation Effect of Obesity on Bone Mineral Density for Older People: The NHANES 2017–2020. Front Endocrinol (Lausanne). 2022; 13(883862.
Faienza MF, D’Amato G, Chiarito M et al. Mechanisms Involved in Childhood Obesity-Related Bone Fragility. Front Endocrinol (Lausanne). 2019; 10(269.
Shen J, Nielson CM, Marshall LM, et al. The Association between BMI and QCT-Derived proximal hip structure and strength in older men: a cross-sectional study. J Bone Min Res. 2015;30(7):1301–8.
Chan MY, Frost SA, Center JR, et al. Relationship between body Mass Index and Fracture Risk is mediated by bone Mineral Density. J Bone Min Res. 2014;29(11):2327–35.
Chanplakorn P, Lertudomphonwanit T, Daraphongsataporn N, et al. Development of prediction model for osteoporotic vertebral compression fracture screening without using clinical risk factors, compared with FRAX and other previous models. Arch Osteoporos. 2021;16(1):84.
Hammoud E, Toumi H, Jacob C, et al. Does the severity of obesity influence bone Mineral density values in Premenopausal women? J Clin Densitom. 2021;24(2):225–32.
Hammoud E, Toumi H, Jacob C, et al. Influence of Sarcopenia on bone health parameters in a group of eumenorrheic obese premenopausal women. J Bone Min Metab. 2020;38(3):385–91.
El Khoury C, Toumi H, Lespessailles E, et al. Decreased composite indices of femoral Neck Strength in Young obese men. J Clin Densitom. 2017;20(2):268–70.
Rinonapoli G, Pace V, Ruggiero C et al. Obesity and bone: a complex relationship. Int J Mol Sci. 2021; 22(24).
Gandham A, Zengin A, Bonham MP et al. Incidence and predictors of fractures in older adults with and without obesity defined by body mass index versus body fat percentage. Bone. 2020; 140(115546.
Kerkeni S, Kolta S, Fechtenbaum J, et al. Spinal deformity index (SDI) is a good predictor of incident vertebral fractures. Osteoporos Int. 2009;20(9):1547–52.
Beck TJ, Petit MA, Wu G, et al. Does obesity really make the femur stronger? BMD, geometry, and fracture incidence in the women’s health initiative-observational study. J Bone Min Res. 2009;24(8):1369–79.
Scott D, Seibel M, Cumming R, et al. Sarcopenic Obesity and its temporal associations with changes in bone Mineral Density, Incident Falls, and fractures in older men: the Concord Health and Ageing in Men Project. J Bone Min Res. 2017;32(3):575–83.
Savvidis C, Tournis S, Dede AD. Obesity and bone metabolism. Horm (Athens). 2018;17(2):205–17.
Khan AU, Qu R, Fan T, et al. A glance on the role of actin in osteogenic and adipogenic differentiation of mesenchymal stem cells. Stem Cell Res Ther. 2020;11(1):283.
Gomez-Ambrosi J, Rodriguez A, Catalan V, et al. The bone-adipose axis in obesity and weight loss. Obes Surg. 2008;18(9):1134–43.
Abhaya Krishnan Muthusami S. Hormonal alterations in PCOS and its influence on bone metabolism. J Endocrinol. 2017;232(2):R99–113.
Segar AH, Fairbank JCT, Urban J. Leptin and the intervertebral disc: a biochemical link exists between obesity, intervertebral disc degeneration and low back pain-an in vitro study in a bovine model. Eur Spine J. 2019;28(2):214–23.
Guo L, Chen K, Yuan J, et al. Estrogen inhibits osteoclasts formation and bone resorption via microRNA-27a targeting PPARgamma and APC. J Cell Physiol. 2018;234(1):581–94.
Zhu K, Hunter M, James A, et al. Discordance between fat mass index and body mass index is associated with reduced bone mineral density in women but not in men: the Busselton Healthy Ageing Study. Osteoporos Int. 2017;28(1):259–68.
Zhang B, Zhou L-P, Zhang X-L, et al. Which Indicator among lumbar vertebral hounsfield unit, vertebral bone quality, or dual-energy X-Ray absorptiometry-measured bone Mineral density is more efficacious in Predicting Thoracolumbar Fragility fractures? Neurospine. 2023;20(4):1193–204.
Li W, Zhu H, Tian H et al. Combinations of two imaging parameters to improve bone mineral density (BMD) assessment in patients with lumbar degenerative diseases. BMC Musculoskelet Disord. 2023; 24(1).
Acknowledgements
We thank the Department of Orthopedics, Xuanwu Hospital Capital Medical University staff and all the patients who participated in the study.
Funding
This work was supported by Capital’s Funds for Health Improvement and Research (No.2024-1-2012), the Beijing Hospitals Authority’s Ascent Plan [No. DFL20190802], National Key Research and Development Program of China (No. 2020YFC2004900), and Beijing Hospitals Authority Clinical Medicine Development of Special Funding Support [No. XMLX202116]. The funders played no role in the design of this study, the collection, analysis and interpretation of data or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Peng Cui was a major contributor in performing the data analysis and writing the manuscript. Wei Wang and Zheng Wang contributed significantly to data acquisition and manuscript preparation. Xinli Hu and Xu Liu analyzed and interpreted the data and helped perform the literature search. Chao Kong and Shibao Lu conceived and designed the work that led to the submission, played an important role in interpreting the results, and writing the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethical statement
The study was approved by institutional review board at Xuanwu Hospital Capital Medical University (2018086) and all methods were carried out under relevant guidelines and regulations. Written informed consent was obtained from all the community-dwelling residents in this study.
Consent for publication
Not Applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cui, P., Wang, W., Wang, Z. et al. The association between body mass index and bone mineral density in older adults: a cross-sectional study of community population in Beijing. BMC Musculoskelet Disord 25, 655 (2024). https://doi.org/10.1186/s12891-024-07782-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07782-7