
Abstract
Background
Dynamic knee valgus (DKV) is a risk factor for non-contact anterior cruciate ligament (ACL) injuries. Understanding the changes in the electromyographic activity of the lower extremity muscles in individuals with DKV helps trainers design ACL injury prevention exercises. Therefore, the present meta-analysis aimed to investigate the muscle activation of the lower limb muscles in individuals with DKV during single-leg and overhead squats.
Methods
Articles with titles, abstracts, and full texts were searched and screened independently by two reviewers in the Web of Science, Scopus, PubMed, and Google Scholar databases, without restrictions on publication date and in English using specified keywords from their inception to January 5, 2024. The quality of articles was evaluated using a modified version of the Downs and Black quality checklist. This meta-analysis used mean difference (MD) to compare the muscle activity patterns between individual with DKV and healthy individuals. Heterogeneity was detected using I-square (I2) test.
Results
In total, four papers with 130 participants were included in the study. Evidence showed a significant difference between the DKV group and the healthy group regarding the activities of the adductor magnus (MD: 6.25, P < 0.001), vastus medialis (MD: 13.23, P = 0.002), vastus lateralis (MD: 11.71, P = 0.004), biceps femoris (MD: 3.06, P = 0.003), and tibialis anterior muscles (MD: 8.21, P = 0.02). Additionally, muscle activity in the DKV group was higher than that in the healthy group.
Conclusions
This meta-analysis reveals distinct muscle activation patterns in individuals with dynamic knee valgus (DKV), with increased activity in key muscles suggesting compensatory responses. These findings underscore the need for targeted rehabilitation to address muscle imbalances and improve knee stability.
Similar content being viewed by others
Background
Dynamic knee valgus (DKV) during dynamic movements, has been identified as a potential risk factor for ACL injury and patellofemoral pain syndrome among athletes. This biomechanical malalignment places increased stress on the ACL, potentially leading to injury [1, 2]. Hewett et al., [3] reported that DKV is a significant predictor of ACL injury. Pre-season screenings of athletes and prospective follow-ups of ACL injuries revealed that athletes who experienced ACL injuries exhibited more valgus during landing compared to healthy individuals [3]. Studies have shown that a 10% increase in DKV angle leads to a 45% increase in patellofemoral joint pressure [4, 5]. The prevalence rates of DKV in the dominant and non-dominant lower limbs have been reported as 26.3% and 26.9%, respectively [6].
DKV is a combination of hip adduction and internal rotation, knee abduction, anterior tibial displacement, tibia external rotation, and ankle eversion [7]. The line of gravity in this movement pattern is located lateral to the foot-thigh line and causes medial knee displacement in individuals with DKV [7]. Three-dimensional analyses have identified DKV as a multi-plane and multi-joint movement disorder [7]. Neuromuscular dysfunction seems to be one of the causes of DKV. Defects in neuromuscular function may cause the muscles to become unable to absorb the load on the knee joint, transferring the load to passive joint structures such as the ACL [8]. Therefore, prevention and rehabilitation strategies have recently focused on improving neuromuscular control to prevent this mechanism of injury.
The Hip and knee muscles in the neuromuscular system appear to play an important role in preventing DKV. Evidence shows that athletes with weak gluteal and hamstring muscles are more likely to have DKV during landing and are at greater risk for non-contact ACL injury [9]. Additionally, calf muscles have also been reported to be involved in activities such as shear and landing-jump movements in which the ACL is at risk of rupture [10]. A previous study concluded that the gastrocnemius muscle exerts pressure on the ACL in closed kinetic chain activities and has an antagonist role [11]. In this regard, Padua et al., [12] found a relationship between the incidence of DKV during overhead squats and the increased co-contraction of the gastrocnemius muscle and the tibialis anterior muscle [12]. These findings suggest that two types of kinetic chains (i.e. down-up and up-down) play an important role in the mechanism of DKV [13]. In other words, any change in the recruitment pattern of trunk and hip muscles affects the kinematics of distal joints [14]. Conversely, the ankle muscles influence the movements of the knee joint [15].
In recent years, single-leg and double-leg squats have been primary used to evaluate the biomechanics of the lower extremities [16, 17]. There are biomechanical and neuromuscular similarities between squats and many exercise movements and daily activities, which may explain why this task has been considered in recent studies [18, 19]. Munro et al., [20] reported that the knee valgus angle was significantly greater in the single-leg squat test than in single-leg landing and vertical jump tests [20]. Additionally, the slow movement in squats allows rehabilitation specialists and physicians to visually identify abnormal movement patterns, such as DKV, and use verbal feedback to modify the movement [21].
Accordingly, this study is crucial for advancing our understanding of muscle activity patterns in DKV and guiding evidence-based interventions to optimize neuromuscular function and reduce the incidence of lower extremity injuries in individuals with DKV. Therefore, the present systematic review and meta-analysis aimed to investigate muscle activation of the lower limb muscles in individuals with DKV during single-leg and overhead squats.
Methods
This systematic review study and meta-analysis was conducted in accordance with the Preferred Reporting Item of Systematic Review and Meta-Analysis (PRISMA) checklist [22].
The search strategy
Two researchers (SHB and FS) independently searched for published studies related to the electromyographic activity of lower extremity muscles in individuals with DKV in the Web of Science, Scopus, PubMed, and Google Scholar databases from their inception to January 5, 2024. The databases were searched and screened without publication date and in English. Whenever there was no consensus between the researchers (SHB and FS), a meeting was held with the third author (BT) to coordinate and resolve conflicts. The research question was defined using the PICO framework. Specifically, the study investigated electromyography of lower limb muscles (O) in individuals with dynamic knee valgus (P), compared to healthy individuals (C). Since the present study is not a clinical trial, no interventions were implemented (I). Three categories of related keywords and synonyms were used to search the titles, abstracts, and keywords of the articles in all databases. The operators “OR” and “AND” were applied within each category of keywords. The keywords used in different databases are reported in Table 1.
Eligibility criteria
All studies that investigated the muscle activation of the lower extremity muscles of individuals with DKV during single-leg and overhead squats were examined in the present research. Case studies, review articles, letter to the editor articles, and articles with only abstracts available were excluded from the present study. The inclusion criteria for this study comprised cross-sectional and case–control studies that compared healthy males or females with individuals diagnosed with DKV, aged between 18 and 35 years. The studies included in the analysis utilized surface electromyography to assess the activity (mean/peak activity) of eleven lower extremity muscles: Gluteus maximus, Gluteus medius, Adductor magnus, Vastus medialis, Vastus lateralis, Biceps femoris, Semitendinosus, Medial gastrocnemius, Lateral gastrocnemius, Tibialis anterior, and Peroneus longus. Muscle activity was evaluated during single-leg and overhead squats. Studies that assessed electromyographic activity of lower extremity muscles during descending stairs, papers that involved interventions, and articles with statistical populations including individuals with patellofemoral pain syndrome and osteoarthritis were excluded from the present meta-analysis.
Process of selecting and collecting the articles
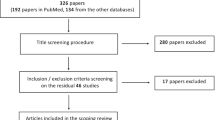
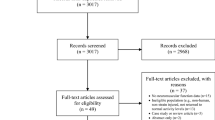
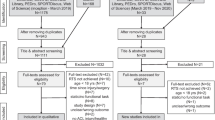
After searching the above databases, two researchers (SHB and FS) examined the titles, abstracts, and full-texts of the articles based on the inclusion and exclusion criteria. The obtained titles and abstracts were saved in EndNote X9 and duplicates were removed. The full texts of the articles whose abstracts met the inclusion criteria were then downloaded and analyzed. In case of disagreement between the two researchers (SHB and FS), the articles were discussed in a meeting to reach a consensus. If an agreement could not be reached, the opinion of the third author (BT) was sought. Fig. 1 shows the search and selection strategy of the articles.

PRISMA flowchart of search results
Quality evaluation
A modified version of the Downs and Black quality index checklist was used to determine the methodology quality of the studies [23]. The original Downs and Black quality index checklist includes 27 questions. By eliminating the questions related to intervention and treatment studies (4, 6, 8, 9, 13, 14, 17, 19, 23, and 24), the number of questions was reduced to 17 (ICC = 0.75–0.88) [24]. The modified checklist used in the present study had 18 items. All questions were scored with 0 (no/unable to determine) or 1 (yes) except for question number five which was scored with 0 (no matching/no description of two or multiple items), 1 (partially/one item not described), and 2 (description of all items/matching). The questions were divided into five areas: reporting (six questions: 1, 2, 3, 5, 7, and 10), external validity (two questions: 11 and 12), internal validity/measurement bias (four questions: 15, 16, 18, and 20), internal/intervening validity or bias in choosing the participants (four questions: 21, 22, 25, and 26), and power study (one question: 27) [25]. The studies were classified into high quality (≥ 70%), medium quality (40–69%), and low quality (< 40%) categories based on the quality evaluation scores [26]. The two researchers independently completed and scored a quality evaluation checklist. If there was disagreement between the two authors about scoring the questions, a final score was determined by the third author (BT) in a joint session.
Data extraction
A predefined data extraction sheet was completed for all studies investigated in the present study. The information extracted from the studies included the article reference (the surname of the first author and the year of publication), statistical population of the participants, statistical sample characteristics (sample size, gender, age, height, body mass, body mass index, exercise activity experience, training duration per week), task type (single-leg and overhead squats), muscles, intensity of measuring muscle activity (flexion/ extension peak angle), electromyographic variables (during descending/ ascending phases), results of the studies, and significance level. The primary researcher (SHB) conducted the statistical analysis using Review Manager 5.4 software. Muscle activity data (Mean ± SD) during the ascending and descending phases of single-leg and overhead squats were extracted for the DKV and healthy groups. Subsequently, a second researcher (FS) independently replicated the analysis. Mean differences (MD) were calculated and reported with a 95% confidence interval (CI). A random-effects model with forest plots was used in this study. This approach is typically employed for handling small sample size heterogeneity, which is common in the literature, along with addressing selection bias [25]. The statistical heterogeneity was calculated at three levels: low (< 50%), medium (50–75%), and high (> 75%) [27].
Results
Study selection
In total, 204 abstracts were examined based on the inclusion and exclusion criteria. Our study did not involve a manual search for additional papers. All included papers were identified through our systematic search methodology. Finally, four articles [12, 28,29,30] were selected and their quality was evaluated (Fig. 1).
The characteristics of the studies
Table 2 summarizes the demographic characteristics of the participants. A total of 130 participants from 4 articles were included in this study, comprising 94 women and 36 men aged 18 to 35 years. Among these, 60 individuals were in the DKV group and 70 were in the healthy group. One study [30] included only females, while the other three studies [12, 28, 29] included both sexes. These studies aimed to compare the muscle activation of the lower limb muscles during single-leg and overhead squats between individuals with DKV and healthy individuals. Among the studies included in this analysis, two studies [29, 30] investigated the muscles of the hip, knee, and ankle joints; one study [12] examined the hip and ankle joint muscles; and one study [28] assessed only the hip joint muscles.
This study analyzed electromyographic (EMG) data normalized to percent of maximal voluntary contraction (%MVC) from various lower limb muscles during single leg squats (SLS) and overhead squats (OHS). The muscles studied included the Gluteus maximus, Gluteus medius, Adductor magnus, Vastus medialis, Vastus lateralis, Biceps femoris, Semitendinosus, Medial gastrocnemius, Lateral gastrocnemius, Tibialis anterior, and Peroneus longus.
The mean qualitative score of the studies was 69.5% (rating from 56 to 83%). Two studies [28, 29] were rated as high quality, while two studies [12, 30] were rated as medium quality. The results of evaluating the quality of the studies are shown in Table 3.
Analysis of the results
The meta-analysis results of the activity patterns of the hip, knee, and ankle joint muscles are shown in Figs. 2, 3, and 4, respectively. The muscle activation of the lower limb muscles during single-leg and overhead squats were considered in the final analysis.

The forest plot for the findings regarding the activity of the hip muscle (DKV vs Healthy)

The forest plot for the findings regarding the activity of the knee muscle (DKV vs Healthy)

The forest plot for the findings regarding the activity of the ankle muscle (DKV vs Healthy). Abbreviations: IV: inverse variance; CI: confidence interval
The meta-analysis revealed that individuals with DKV exhibited heightened muscle activity in the adductor magnus, vastus medialis, vastus lateralis, biceps femoris, and tibialis anterior muscles compared to those without the condition. This alteration in neuromuscular patterns at the hip, knee, and ankle joints was statistically significant. Conversely, no significant differences were found in the gluteus maximus, gluteus medius, semitendinosus, medial gastrocnemius, lateral gastrocnemius, and peroneus longus muscles between the two groups. However, compared to the healthy group, the muscle activity in the group affected by DKV was higher.
The activity patterns of hip joint muscles
Gluteus maximus muscle
Four studies [12, 28,29,30] investigated the activity of the gluteus maximus muscle. Results showed that there was no significant difference between the DKV and healthy groups regarding the activity of the gluteus maximus muscle. The activity of the gluteus maximus muscle was greater in the DKV group than in the healthy group in all studies (MD: 1.14, 95% CI [-0.23, 2.51], Z = 1.63, P = 0.10, I2 = 0%) except for one [29].
Gluteus medius muscle
Among the three studies [12, 29, 30] investigating the activity of the gluteus medius muscle, two studies [12, 29] reported a decrease in, while activity one study [30] indicated an increase in the DKV group. Additionally, there was no significant difference between the DKV and healthy groups (MD: 0.50, 95% CI [-0.67, 1.66], Z = 0.84, P = 0.40, I2 = 0%).
Adductor magnus muscle
Four studies [12, 28,29,30] investigated the activity of the adductor magnus muscle. In all of these studies, the activity of the adductor magnus muscle was reported to be greater in the DKV group than in the healthy group. The results suggested a significant difference between the DKV and healthy groups in the activity of the adductor magnus muscle (MD: 6.25, 95% CI [3.96, 8.54], Z = 5.35, P < 0.001, I2 = 0%).
The activity patterns of knee joint muscles
Vastus medialis muscle
Among the two studies [29, 30] that investigated the activity of the vastus medialis muscle, the muscle activity in the DKV group was higher than in the healthy group. The Outcomes suggested a significant difference between the DKV and healthy groups regarding the activity of the vastus medialis muscle (MD: 13.23, 95% CI [4.76, 21.71], Z = 3.06, P = 0.002, I2 = 5%).
Vastus lateralis muscle
Two studies [29, 30] investigated the activity of the vastus lateralis muscle. Both studies reported increased muscle activity in the DKV group. Moreover, the outcomes suggest that there is a significant difference between the DKV and healthy groups regarding the activity of the vastus lateralis muscle (MD: 11.71, 95% CI [3.80, 19.61], Z = 2.90, P = 0.004, I2 = 0%).
Biceps femoris muscle
Two studies [29, 30] investigated the activity of the biceps femoris muscle. The muscle activity in the DKV group was higher than in the healthy group. The results suggested a significant difference between the two groups regarding the activity of the biceps femoris muscle (MD: 3.06, 95% CI [1.07, 5.05], Z = 3.01, P = 0.003, I2 = 0%).
Semitendinosus muscle
Only one study [29] investigated the activity of this muscle. The results suggested an increase in the activity of the semitendinosus muscle in the DKV group compared with that in the healthy group. However, no significant difference was observed between the two groups (MD: 4.90, 95% CI [-5.11, 14.91], Z = 0.96, P = 0.34).
The activity patterns of ankle joint muscles
Medial gastrocnemius muscle
The activity of the medial gastrocnemius muscle was investigated in three studies [12, 29, 30]. One study [29] reported that the activity of the medial gastrocnemius muscle decreased during single-leg squats, whereas two other studies reported an increase in the activity of this muscle during overhead squats. The outcomes showed that there was no significant difference between the DKV and healthy groups regarding the activity of the medial gastrocnemius muscle (MD: 2.67, 95% CI [-0.33, 5.68], Z = 1.75, P = 0.08, I2 = 52%).
Lateral gastrocnemius muscle
Only one study [12] investigated this during overhead squats. The results indicated that the activity of the lateral gastrocnemius muscle in the DKV group was greater than that of the healthy group but, that there was no significant difference between the two groups (MD: 5.80, 95% CI [-0.61, 12.21], Z = 1.77, P = 0.08, I2 = 0%).
Tibialis anterior muscle
Two studies [12, 30] investigated the activity of the tibialis anterior muscle during overhead squat. The result suggest that there is a significant difference between the two groups, with the activity of the tibialis anterior muscle being greater in the DKV group than in the healthy group (MD: 8.21, 95% CI [1.26, 15.17], Z = 2.31, P = 0.02, I2 = 28%).
Peroneus longus muscle
The activity of the peroneus longus muscle during overhead squats was investigated only in one study [30]. The results showed that the activity of the peroneus longus muscle was greater in the dynamic knee valgus group than in the healthy group. However, there was no significant difference between the two groups (MD: 18.68, 95% CI [-13.96, 51.32], Z = 1.12, P = 0.26, I2 = 66%).
Discussion
The present study aimed to investigate the muscle activation of the lower limb muscles in individuals exhibiting dynamic knee valgus during single-leg and overhead squats. The results of this systematic review and meta-analysis indicated that there were significant differences between the groups in only 5 muscles out of the 11 muscles examined (adductor magnus, vastus medialis, vastus lateralis, biceps femoris, and tibialis anterior muscles) examined. The findings also revealed that the activity level of all muscles in individuals with dynamic knee valgus was higher compared to the healthy group.
Hip
The results of the present meta-analysis showed that there wasn’t a significant difference between the DKV and healthy groups. In 75% of the examined studies, it was suggested that the activity level of the gluteus maximus muscle in both descending and ascending phases was greater in individuals with DKV than in healthy participants. Barbosa et al., [31] reported a relationship between increased activity of the gluteus maximus muscle and increased DKV [31]. This increase in activity was likely due to the weakness of the gluteal muscles which resulted in a compensatory increase in muscle activity in individuals with DKV [32]. The gluteus maximus is an external rotator. Therefore, its increased activity during the squat task may serve to counteract internal rotation, hip adduction, and knee valgus [33]. Although the activity of the gluteus medius muscle in the DKV group was greater than that of the healthy group, there was no significant difference between the DKV and healthy groups in this muscle. The gluteus medius muscle is primarily an abductor, but it also contributes to hip internal rotation. The gluteus medius rotational torque arm increases with hip flexion, especially at angles greater than 30 degrees [34]. According to the findings of Hollman et al., [33] the hip is flexed at 40–50 degrees in a single-leg squat. The increased recruitment of gluteus medius motor neurons does not prevent hip adduction during squat but rather intensifies hip internal rotation and adduction during hip flexion (a coupling motion) [33]. Accordingly, it is necessary to consider the kinematics of the hip joint and the function of gluteal muscles in the evaluation and rehabilitation of individuals with DKV. Additionally, evidence showed that the activity of the adductor magnus muscle in the DKV group increased during both single-leg and overhead squats. The overactivity of the adductor magnus muscle in the DKV group may be due to its role in controlling hip extension during squat [28]. If the gluteus maximus muscle does not have sufficient strength to control the amount of extension, the adductor magnus muscle becomes overactive as a synergist muscle to control hip extension. These findings highlight the importance of hip activity muscles in controlling knee movements in the frontal plane.
Knee
The results of the present meta-analysis also showed that there was a significant difference between the DKV and healthy groups regarding the activity of the lateral muscles of the knee. It was also shown that the activity of the lateral muscles in the DKV group was higher than that in the healthy group. The increased activity of the biceps femoris muscle may be a compensatory response to the increased activity of the vastus medialis and lateralis muscles for knee stability [30]. According to Palmieri-Smith et al., [35] there was a relationship between increased DKV and the enhanced feed-forward activity of lateral muscles (vastus lateralis and biceps femoris) [35]. It has been shown that the long head of the biceps femoris externally rotates the leg during the descending phase. This external rotation manifests as knee abduction and/or tibia internal rotation, ultimately leading to medial knee displacement [30]. Given the position of the biceps femoris and semitendinosus, the increased activity of the semitendinosus muscle in the DKV group is notable. The semitendinosus muscle acts as an agonist for the ACL. The enhanced activity of the medial hamstring muscle may help limit knee valgus and external rotation, thereby reducing strain on the ACL [36]. Unfortunately, few studies have investigated the activity of the medial hamstring muscle during squatting.
The quadriceps and hamstring muscles potentially provide dynamic stability of the knee in the frontal plane due to their abductor/adductor torque. However, because of the mutual junctions of the quadriceps muscles and the patellar tendon, they cannot preferentially control abduction (vastus medialis) and adduction (vastus lateralis) [37]. The increased activity of the vastus lateralis can lead to knee abduction if the loads applied to the knee are not counteracted by the activity of the medial muscles [38]. Knee abduction and hip internal rotation create valgus rotational forces in the lower extremity [30]. The activity of the vastus medialis muscle was significantly greater in the DKV group compared to the healthy group, with a notable difference observed between the two groups. The increased activity of the vastus medialis muscle may help counteract abduction loads and reduce valgus laxity [39]. The co-contraction of medial knee muscles, which provide a varus torque arm, appears to be an effective method for reducing the valgus loads [37].
Ankle
The results of the present meta-analysis regarding the ankle joint area showed a significant difference between the DKV and healthy groups in only one case: tibialis anterior muscle. There was no significant difference between the two groups for the other muscles (peroneus longus, medial gastrocnemius, and lateral gastrocnemius). However, the activity level of the calf muscles in the DKV group was greater than that of the healthy group. Researchers believe that the increased activity of the anterior tibialis, medial gastrocnemius, and lateral gastrocnemius muscles may be attributed to the increased plantar flexion torque and ankle joint stiffness [12]. Previous studies have reported that increased co-contraction of agonist and antagonist muscles around a joint leads to greater overall joint stiffness [40]. Additionally, the results of a previous meta-analysis suggested a relationship between reduced ankle dorsiflexion range of motion and DKV [41]. The increased activity of the anterior tibialis, medial gastrocnemius, and lateral gastrocnemius muscles likely contributed to reduction in dorsiflexion ankle range of motion on the sagittal plane and an increase in the knee range of motion on the frontal plane (valgus) [12, 42]. The limitation of ankle dorsiflexion range of motion leads to hindfoot pronation (at the subtalar joint) and eversion, which are associated with tibia internal rotation and DKV on the frontal plane [43]. Although the peroneus longus muscle is the primary evertor of the ankle joint and crucial stabilizer against sudden inversion forces [44], only one study has investigated its role [30]. Therefore, the current study cannot conclude the difference between individuals with DKV and healthy individuals regarding the activity of the peroneus longus muscle during weight-bearing activities. Since the knee joint is not isolated from the rest of the lower extremity kinetic chain during weight-bearing activities, the activity patterns of the hip and ankle muscles influence the load applied to the knee joint.
Limitations
There are some limitations to the present investigation. One limitation is that the meta- analysis was not registered on the PROSPERO website before conducting the research. Additionally, in previous studies, the researchers who measured the research variables were not blinded to the participants’ grouping and a majority of the participants in the previous studies were females.
Furthermore, the squat tasks were performed at varying speeds. It remains unclear whether dorsiflexion restriction is due to increased activity of the tibialis anterior and gastrocnemius muscles or an adaptation to DKV, as the analyses are based on cross-sectional studies that do not establish causal relationships between the research variables. Although the quadriceps and hamstrings play a crucial role in controlling knee movement during overhead squats, these muscles were only studied in one study. Therefore, further research is needed to understand the activity patterns of these muscles in individuals with DKV. Given the very limited evidence (with only 4 articles included), the results of this systematic review and meta-analysis should be interpreted with caution and require validation or confirmation through future studies.
Conclusions
The results of the present meta-analysis highlight significant muscle activation in the lower limb muscles among individuals with dynamic knee valgus (DKV). These findings suggest distinct patterns of muscle activity in individuals with DKV compared to healthy individuals during single-leg and overhead squats. Increased activity levels were observed in certain muscles including the adductor magnus, vastus medialis, vastus lateralis, biceps femoris, and tibialis anterior, in the DKV group. This indicates a compensatory response and potential factors contributing to altered movement patterns and knee stability. Understanding the muscle activation patterns associated with DKV can help design targeted rehabilitation programs to address specific muscle imbalances and movement dysfunctions.
Data Availability
All data generated or analyzed during this study are included in this published article.
Abbreviations
- DKV:
-
Dynamic knee valgus
- ACL:
-
Anterior cruciate ligament
- MD:
-
Mean differences
- CI:
-
Confidence interval
- PRISMA:
-
Preferred Reporting Item of Systematic Review and Meta-Analysis
- ICC:
-
Intraclass correlation coefficient
- %MVC:
-
Maximal voluntary contraction
- SLS:
-
Single leg squats
- OHS:
-
Overhead squats
References
Ellenberger L, Oberle F, Lorenzetti S, Frey WO, Snedeker JG, Spörri J. Dynamic knee valgus in competitive alpine skiers: observation from youth to elite and influence of biological maturation. Scand J Med Sci Sports. 2020;30(7):1212–20. https://doi.org/10.1111/sms.13657.
Neal BS, Barton CJ, Gallie R, O’Halloran P, Morrissey D. Runners with patellofemoral pain have altered biomechanics which targeted interventions can modify: a systematic review and meta-analysis. Gait Posture. 2016;45:69–82. https://doi.org/10.1016/j.gaitpost.2015.11.018.
Hewett TE, Myer GD, Ford KR, Heidt RS Jr, Colosimo AJ, McLean SG, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501. https://doi.org/10.1177/0363546504269591.
Waiteman MC, Briani RV, Pazzinatto MF, Ferreira AS, Ferrari D, de Oliveira SD, et al. Relationship between knee abduction moment with patellofemoral joint reaction force, stress and self-reported pain during stair descent in women with patellofemoral pain. Clin Biomech. 2018;59:110–6. https://doi.org/10.1016/j.clinbiomech.2018.09.012.
Yalfani A, Ahmadi M, Asgarpoor A. The effect of kinetic factors of dynamic knee valgus on patellofemoral pain: a systematic review and meta-analysis. J Bodyw Mov Ther. 2024;37:246–53. https://doi.org/10.1016/j.jbmt.2023.11.001.
Sanchis GJB, Lopes JM, de Assis SJC, Catão RLA, Santos TRT, Roncalli AGDCO. Dynamic knee valgus prevalence in children and its association with pain intensity, foot mobility, and sex—A cross-sectional study. Heliyon. 2022;8(10). https://doi.org/10.1016/j.heliyon.2022.e10984
Griffin LY, Albohm MJ, Arendt EA, Bahr R, Beynnon BD, DeMaio M, et al. Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, Jan 2005. Am J Sports Med. 2006;34(9):1512–32. https://doi.org/10.1177/0363546506286866.
Hoshiba T, Fukubayashi T. Biomechanical adaptations in subjects after anterior cruciate ligament reconstruction: preventing secondary injury. Sports Injuries Prevent. 2015:257–65. https://doi.org/10.1007/978-4-431-55318-2_21.
Rath M. Effect of foot type on knee valgus, ground reactio. 2016.
Hewett TE, Ford KR, Hoogenboom BJ, Myer GD. Understanding and preventing acl injuries: current biomechanical and epidemiologic considerations-update 2010. N Am J Sports Phys Ther. 2010;5(4):234.
Adouni M, Shirazi-Adl A, Marouane H. Role of gastrocnemius activation in knee joint biomechanics: gastrocnemius acts as an ACL antagonist. Comput Methods Biomech Biomed Eng. 2016;19(4):376–85. https://doi.org/10.1080/10255842.2015.1032943.
Padua DA, Bell DR, Clark MA. Neuromuscular characteristics of individuals displaying excessive medial knee displacement. J Athl Train. 2012;47(5):525–36. https://doi.org/10.4085/1062-6050-47.5.10.
Jamaludin NI, Sahabuddin FNA, Raja Ahmad Najib RKM, Shamshul Bahari MLH, Shaharudin S. Bottom-up kinetic chain in drop landing among university athletes with normal dynamic knee valgus. Int J Environ Res Public Health. 2020;17(12):4418. https://doi.org/10.3390/ijerph17124418.
Snyder KR, Earl JE, O’Connor KM, Ebersole KT. Resistance training is accompanied by increases in hip strength and changes in lower extremity biomechanics during running. Clin Biomech. 2009;24(1):26–34. https://doi.org/10.1016/j.clinbiomech.2008.09.009.
Khamis S, Yizhar Z. Effect of feet hyperpronation on pelvic alignment in a standing position. Gait Posture. 2007;25(1):127–34. https://doi.org/10.1016/j.gaitpost.2006.02.005.
Ali N, Rouhi G, Robertson G. Gender, vertical height and horizontal distance effects on single-leg landing kinematics: implications for risk of non-contact ACL injury. J Hum Kinet. 2013;37(1):27–38. https://doi.org/10.2478/hukin-2013-0022.
Lyle MA, Valero-Cuevas FJ, Gregor RJ, Powers CM. Control of dynamic foot-ground interactions in male and female soccer athletes: females exhibit reduced dexterity and higher limb stiffness during landing. J Biomech. 2014;47(2):512–7. https://doi.org/10.1016/j.jbiomech.2013.10.038.
Bell DR, Padua DA, Clark MA. Muscle strength and flexibility characteristics of people displaying excessive medial knee displacement. Arch Phys Med Rehabil. 2008;89(7):1323–8. https://doi.org/10.1016/j.apmr.2007.11.048.
Schoenfeld BJ. Squatting kinematics and kinetics and their application to exercise performance. J Strength Condition Res. 2010;24(12):3497–506. https://doi.org/10.1519/JSC.0b013e3181bac2d7.
Munro A, Herrington L, Comfort P. The relationship between 2-dimensional knee-valgus angles during single-leg squat, single-leg-land, and drop-jump screening tests. J Sport Rehabil. 2017;26(1):72–7. https://doi.org/10.1123/jsr.2015-0102.
Donohue MR, Ellis SM, Heinbaugh EM, Stephenson ML, Zhu Q, Dai B. Differences and correlations in knee and hip mechanics during single-leg landing, single-leg squat, double-leg landing, and double-leg squat tasks. Res Sports Med. 2015;23(4):394–411. https://doi.org/10.1080/15438627.2015.1076413.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, The PRISMA, et al. statement: an updated guideline for reporting systematic reviews. BMJ. 2020;2021:372. https://doi.org/10.1016/j.ijsu.2021.105906.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84. https://doi.org/10.1136/jech.52.6.377.
Barton CJ, Levinger P, Menz HB, Webster KE. Kinematic gait characteristics associated with patellofemoral pain syndrome: a systematic review. Gait Posture. 2009;30(4):405–16. https://doi.org/10.1016/j.gaitpost.2009.07.109.
Sancho I, Malliaras P, Barton C, Willy RW, Morrissey D. Biomechanical alterations in individuals with Achilles tendinopathy during running and hopping: a systematic review with meta-analysis. Gait Posture. 2019;73:189–201. https://doi.org/10.1016/j.gaitpost.2019.07.121.
Malliaras P, Barton CJ, Reeves ND, Langberg H. Achilles and patellar tendinopathy loading programmes: a systematic review comparing clinical outcomes and identifying potential mechanisms for effectiveness. Sports Med. 2013;43:267–86. https://doi.org/10.1007/s40279-013-0019-z.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60. https://doi.org/10.1136/bmj.327.7414.557.
Bell DR, Vesci BJ, DiStefano LJ, Guskiewicz KM, Hirth CJ, Padua DA. Muscle activity and flexibility in individuals with medial knee displacement during the overhead squat. Athl Train Sports Health Care. 2012;4(3):117–25. https://doi.org/10.3928/19425864-20110817-03.
Mauntel TC, Begalle RL, Cram TR, Frank BS, Hirth CJ, Blackburn T, et al. The effects of lower extremity muscle activation and passive range of motion on single leg squat performance. J Strength Condition Res. 2013;27(7):1813–23. https://doi.org/10.1519/JSC.0b013e318276b886.
Dinis R, Vaz JR, Silva L, Marta S, Pezarat-Correia P. Electromyographic and kinematic analysis of females with excessive medial knee displacement in the overhead squat. J Electromyogr Kinesiol. 2021;57:102530. https://doi.org/10.1016/j.jelekin.2021.102530.
Barbosa AC, Vieira ER, Barbosa MA, Fernandes I, Damázio M, Badaró B. Gluteal activation and increased frontal plane projection angle during a step-down test in young women. Hum Mov. 2018;19(1):64–70. https://doi.org/10.5114/hm.2018.73614.
Shultz SJ, Perrin DH, Adams JM, Arnold BL, Gansneder BM, Granata KP. Assessment of neuromuscular response characteristics at the knee following a functional perturbation. J Electromyogr Kinesiol. 2000;10(3):159–70. https://doi.org/10.1016/S1050-6411(00)00002-X.
Hollman JH, Galardi CM, Lin I-H, Voth BC, Whitmarsh CL. Frontal and transverse plane hip kinematics and gluteus maximus recruitment correlate with frontal plane knee kinematics during single-leg squat tests in women. Clin Biomech. 2014;29(4):468–74. https://doi.org/10.1016/j.clinbiomech.2008.09.009.
Delp SL, Hess WE, Hungerford DS, Jones LC. Variation of rotation moment arms with hip flexion. J Biomech. 1999;32(5):493–501. https://doi.org/10.1016/S0021-9290(99)00032-9.
Palmieri-Smith RM, Wojtys EM, Ashton-Miller JA. Association between preparatory muscle activation and peak valgus knee angle. J Electromyogr Kinesiol. 2008;18(6):973–9. https://doi.org/10.1016/j.jelekin.2007.03.007.
Zebis MK, Andersen LL, Bencke J, Kjær M, Aagaard P. Identification of athletes at future risk of anterior cruciate ligament ruptures by neuromuscular screening. Am J Sports Med. 2009;37(10):1967–73. https://doi.org/10.1177/0363546509335000.
Saki F. Relationship between functional movement screen scores and selected physical fitness factors in boy taekwondo athletes. J Appl Exerc Physiol. 2018;13(26):249–60. https://doi.org/10.22080/jaep.2017.12636.1653.
Lloyd DG, Buchanan TS, Besier TF. Neuromuscular biomechanical modeling to understand knee ligament loading. Med Sci Sports Exerc. 2005;37(11):1939–47. https://doi.org/10.1249/01.mss.0000176676.49584.ba.
Zhang L-Q, Wang G. Dynamic and static control of the human knee joint in abduction–adduction. J Biomech. 2001;34(9):1107–15. https://doi.org/10.1016/S0021-9290(01)00080-X.
Lacquaniti F, Licata F, Soechting J. The mechanical behavior of the human forearm in response to transient perturbations. Biol Cybern. 1982;44:35–46. https://doi.org/10.1007/BF00353954.
Lima YL, de Paula Lima PO, Bezerra MA, de Oliveira RR, Almeida GPL. The association of ankle dorsiflexion range of motion and dynamic knee valgus: a systematic review with meta-analysis. Phys Ther Sport. 2018;31:e4. https://doi.org/10.1016/j.ptsp.2020.04.020.
Macrum E, Bell DR, Boling M, Lewek M, Padua D. Effect of limiting ankle-dorsiflexion range of motion on lower extremity kinematics and muscle-activation patterns during a squat. J Sport Rehabil. 2012;21(2):144–50. https://doi.org/10.1123/jsr.21.2.144.
DiGiovanni CW, Langer P. The role of isolated gastrocnemius and combined Achilles contractures in the flatfoot. Foot Ankle Clin. 2007;12(2):363–79. https://doi.org/10.1016/j.fcl.2007.03.005.
Suda EY, Sacco IC. Altered leg muscle activity in volleyball players with functional ankle instability during a sideward lateral cutting movement. Phys Ther Sport. 2011;12(4):164–70. https://doi.org/10.1016/j.ptsp.2011.01.003.
Acknowledgements
Not applicable
Funding
The author did not receive any funds.
Author information
Authors and Affiliations
Contributions
F.S. Design of the work, Revised main manuscript text, Analysis. SH.B. Wrote the main manuscript text, Creation of new software used in the work, Analysis.B.T. Interpretation of data, Revised main manuscript text, Analysis.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Khou, S.B., Saki, F. & Tahayori, B. Muscle activation in the lower limb muscles in individuals with dynamic knee valgus during single-leg and overhead squats: a meta-analysis study. BMC Musculoskelet Disord 25, 652 (2024). https://doi.org/10.1186/s12891-024-07759-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07759-6