
Abstract
Background
Data are currently lacking regarding perioperative stroke recurrence in hip fracture patients with previous stroke. We aimed to analyze the incidence and risk factors of perioperative stroke recurrence in elderly patients with previous stroke who underwent hip fracture surgery.
Methods
We used 2019 and 2020 data from the United States National Inpatient Sample database. We identified elderly patients with previous ischemic stroke who had undergone hip fracture surgery to analyze the incidence of stroke recurrence. A 1:4 propensity score matching was used to balance confounding factors related to demographic data and matched the control group with the stroke recurrence group. Risk factors for stroke recurrence were determined using univariate and multivariate logistic analysis.
Results
The incidence of perioperative stroke recurrence in elderly patients with previous stroke who underwent hip fracture surgery was 5.7% (51/882). Multivariate logistic regression analysis showed that intertrochanteric fracture (odds ratio 2.24, 95% confidence interval 1.14–4.57; p = 0.021), hypertension (odds ratio 2.49, 95% confidence interval 1.26–5.02; p = 0.009), and postoperative pneumonia (odds ratio 4.35, 95% confidence interval 1.59–11.82; p = 0.004) were independently associated with stroke recurrence.
Conclusions
The perioperative stroke recurrence rate in elderly hip fracture patients with previous stroke was 5.7%. Intertrochanteric fracture, hypertension, and postoperative pneumonia were identified as factors significantly associated with stroke recurrence in this study. Adequate systemic support post-fracture, effective blood pressure management, and proactive infection prevention may help reduce stroke recurrence, especially in patients with intertrochanteric fractures.
Similar content being viewed by others


Background
With population aging, hip fractures complicated by stroke have become more common in elderly patients, with a reported incidence ranging between 4% and 15% [1, 2]. Hip fractures and stroke can be disabling and potentially fatal, seriously endangering the health and quality of life of elderly patients [3, 4]. Stroke is one of the most important risk factors for hip fractures [5], with ischemic stroke being the most common [6]. Patients with stroke have an up to four-fold increased risk of hip fractures owing to the high incidence of falls and loss of bone mass on the paretic side [7].
Previous studies have examined the incidence and risk factors of perioperative stroke in non-cardiac and non-neurologic surgery [8,9,10,11]. Perioperative stroke is defined as a brain infarction of ischemic or hemorrhagic etiology that occurs during surgery or within 30 days after surgery [12], with a reported incidence of 0.1–10% [13, 14]. It has been well documented that previous stroke can significantly increase the risk of perioperative stroke [14,15,16]. However, to our knowledge, no study has specifically addressed the incidence and risk factors associated with recurrent stroke in elderly patients with preoperative stroke who have undergone hip fracture surgery. Relevant data are needed to establish expert consensus or clinical guidelines for elderly patients with hip fracture and preoperative stroke.
In recent years, administrative databases have been widely used in clinical research, and offer the potential to examine infrequent exposures or outcomes. The National Inpatient Sample (NIS) is a comprehensive database containing information on hospital discharge covering both payers and age groups. It accounts for approximately 20% of all admissions to non-federal hospitals in the United States [17]. In this study, we used the NIS database, aiming to identify elderly patients with preoperative stroke who underwent hip fracture surgery to analyze the incidence and risk factors of perioperative stroke recurrence.
Methods
Database and patients
We selected study subjects from the 2019 and 2020 National Inpatient Sample (NIS) databases according to the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes [18,19,20]. Patients with preoperative stroke were identified using ICD-10 I63 codes, patients with intraoperative stroke were identified using both ICD-10 G9732 and I97811 codes, and patients with postoperative stroke were identified using both ICD-10 G9752 and I97821 codes. Perioperative stroke is defined as a stroke that occurs either during or after surgery. Therefore, we defined recurrent perioperative stroke as patients with preoperative stroke experienced intraoperative or postoperative stroke. Hip fractures included femoral neck fractures and intertrochanteric fractures, and hip fracture surgeries included primary hip arthroplasty and proximal femoral internal fixation. Specific ICD-10-CM codes involved in this study are provided in Supplementary Material 1.
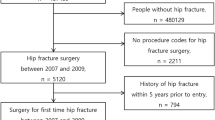
There were 99,469 elderly patients with hip fractures who underwent hip fracture surgery, among whom 882 patients had preoperative stroke. Among these 882 patients, 51 experienced perioperative recurrent stroke (Fig. 1). To analyze the relationship between perioperative characteristics and stroke recurrence, we performed propensity score matching (PSM) based on patient demographics. We matched 51 cases of stroke recurrence with a control group of patients without stroke recurrence at a 1:4 ratio, with calipers set at 0.05 using the R MatchIt package. Patient demographics and perioperative characteristics before PSM were presented in Supplementary Material 2. A plot illustrating the balance of covariates before and after PSM was provided in Supplementary Material 3.

Flowchart of the study population
Included variables
The demographic variables included age, sex, ethnicity, and household income. The hip fracture was classified as either femoral neck or intertrochanteric. The types of surgery included hip replacement and proximal femoral fixation. Previous ischemic stroke was classified into four subtypes as follows: anterior circulation infarction, posterior circulation infarction, cerebellar artery infarction, other or unspecified infarction. Whether long-term use of antithrombotics after stroke was identified using ICD10 Z7901 and Z7902 codes. Elixhauser comorbidities included obesity, alcohol abuse, drug abuse, dementia, depression, acquired immune deficiency syndrome, autoimmune conditions, diabetes, hypertension, chronic heart failure, chronic pulmonary disease, chronic kidney disease, peripheral vascular disease, hypothyroidism, other thyroid disorders, leukemia, lymphoma, metastatic cancer, and solid tumors. The Elixhauser comorbidity score was calculated according to international standards [21] to evaluate preexisting disease burden. The postoperative complications of interest included deep vein thrombosis, pulmonary embolism, pneumonia, respiratory failure, acute heart failure, myocardial infarction, cardiac dysrhythmias, acute renal failure, urinary tract infection, electrolyte disorders, and sepsis.
Statistical analysis
Missing values in the clinical data were filled in via multiple imputations using the mice package in R. All included variables were subjected to univariate analysis. We evaluated categorical variables using Chi-square or Fisher’s exact tests and non-normal/normal continuous variables using Mann–Whitney U or t- tests. Statistically significant variables in the univariate analysis and clinically relevant variables were entered into the multivariable model. Statistical analysis was performed using R (version 2023.03.1 + 446; The R Foundation for Statistical Computing, Vienna, Austria) software, and statistical significance was set at p < 0.05.
Results
The incidence of perioperative stroke recurrence in elderly patients with previous stroke who underwent hip fracture surgery was 5.7% (51/882). In the univariate analysis, there was no significant difference in demographic data (age, sex, race, and household income) between the stroke recurrence and non-stroke recurrence groups. Regarding fracture type, the stroke recurrence group had a higher proportion of intertrochanteric fractures than the non-stroke recurrence group (68.6% vs. 50%, p = 0.026), whereas the proportion of femoral neck fractures had no significant difference between the two groups. No statistically significant differences were observed between the two groups in surgical type, stroke type, and use of antithrombotics.
With respect to comorbidities, the difference in Elixhauser Score between the two groups was not statistically significant. Only the prevalence of hypertension (51% vs. 34.3%, p = 0.042) in stroke recurrence group was significantly higher than the non-stroke follow-up group. Concerning postoperative complications, the incidence of pneumonia in the recurrent stroke group was significantly higher than that in the non-recurrent stroke group (17.6% vs. 5.9%, p = 0.014), followed by urinary tract infections (33.3% vs. 22.1%, p = 0.135), acute heart failure (9.8% vs. 4.9%, p = 0.318), sepsis (11.8% vs. 7.4%, p = 0.459), electrolyte disorders (47.1% vs. 45.1%, p = 0.925), and myocardial infarction (11.8% vs. 9.8%, p = 0.877). Univariate analysis on patient demographics and perioperative characteristics after PSM were summarized in Table 1.
Multivariate logistic regression showed that intertrochanteric fracture (OR 2.24, 95% CI 1.14–4.57; p = 0.021), hypertension (OR 2.49, 95% CI 1.26–5.02; p = 0.009), and postoperative pneumonia (OR 4.35, 95% CI 1.59–11.82; p = 0.004) were significantly associated with perioperative stroke (Table 2; Fig. 2).

Forest map of multivariate logistic analysis of influencing factors for perioperative recurrent stroke
Discussion
In this study, we used 2019 and 2020 data from the NIS database to examine the incidence and risk factors of perioperative recurrent stroke in elderly patients with preoperative ischemic stroke undergoing hip fracture surgery. PSM was used to balance confounding factors related to demographic data and matched the control group with the stroke recurrence group. Risk factors for stroke recurrence were determined using univariate and multivariate analyses. The incidence of perioperative stroke recurrence was 5.7%. Our findings indicated that intertrochanteric fractures, hypertension, and postoperative pneumonia were associated with stroke recurrence.
To our knowledge, we are the first to report the incidence of perioperative recurrent stroke in hip fracture patients with previous stroke. Previous study reported that found that patients who experienced a stroke within 30 days before elective non-neurologic and non-cardiac surgery had a higher risk of perioperative recurrent stroke (adjusted OR, 8.02; 95% CI, 6.37–10.10; p < 0.001) compared with patients without previous stroke [14]. However, data on specific incidence rates are lacking. Christiansen et.al [15] showed that the incidence of perioperative stroke in patients with preoperative stroke undergoing noncardiac and nonvascular surgery within three months was 9.9%. This result is higher than ours, probably because no subgroup analysis of surgery was performed. Lamo‑Espinosa et al. [22] reported that the overall incidence of stroke in patients with hip fracture was 6.72%, which is close to our results. However, it is not targeted at the perioperative period and patients with previous stroke. Our study adds further insight into the incidence of perioperative stroke recurrence in hip fracture patients with previous stroke. We reported an incidence rate of 5.7%. With reference to previous studies, the incidence rate is still relatively high. Elderly patients with hip fractures are in a hypercoagulable state due to traumatic stress as well as changes in relation to hemodynamics and composition due to fracture, pain, and blood loss [23]. Moreover, patients with stroke often have hypertension, diabetes, heart disease, hyperlipidemia, and other medical diseases. When hip fracture coexists with previous stroke, the risk of stroke recurrence increases; therefore, sufficient attention should be paid to prevent recurrent stroke in these patients during the perioperative period.
In this study, we found that intertrochanteric fractures were associated with a 2.2-fold increased risk of recurrent stroke (OR 2.24, 95% CI 1.14–4.57; p = 0.021). Excessive blood loss may be a critical pathophysiological factor underlying the high risk of stroke recurrence in intertrochanteric fractures. It has been reported that extracapsular hip fractures are associated with significantly more preoperative blood loss and transfusions compared to their intracapsular counterparts [24]. Although proximal femoral nail fixation is minimally invasive technique for treating intertrochanteric fractures, it can cause greater blood loss (up to 2100 mL) than expected [25, 26]. Additionally, low albumin level has been identified as a risk factor for stroke following hip fractures [22]. During a stroke, the autoregulation of cerebral blood flow is impaired, which may take one-to-two weeks, or even longer than a month, to recover [27]. During this period, the cerebral blood supply relies heavily on the maintenance of cerebral perfusion pressure, which is vulnerable to anesthesia and trauma. Perioperative blood loss in intertrochanteric fractures may cause hemodynamic instability and affect cerebral perfusion, thereby increasing the risk of stroke recurrence. Adequate systemic support might help in reducing the recurrence of stroke.
Stroke patients generally require secondary prevention with antithrombotic drugs. A large proportion of these patients are already receiving antithrombotic therapy before sustaining a hip fracture. However, antithrombotic therapy may be discontinued due to concerns about serious perioperative bleeding and higher transfusion demands associated with intertrochanteric fractures. This discontinuation may be another factor that increases the risk of stroke recurrence. This study found no significant association between long-term use of antithrombotic therapy and stroke recurrence. Unfortunately, the NIS database lacks detailed information on antithrombotic therapy, such as the timing and specific drugs used postoperatively. A previous study has identified the discontinuation of antiplatelet (P = 0.004) as a significant risk factor for perioperative stroke [11]. Additionally, evidence suggests that continuing anticoagulant treatment in intertrochanteric fracture patients does not increase perioperative blood loss [26]. Therefore, for patients with hip fracture and stroke, continuing antithrombotic therapy perioperatively remains critical to prevent stroke recurrence after carefully weighing the risk of bleeding.
The timing of surgery may be another critical factor influencing stroke recurrence. Current guidelines recommend that hip fractures be classified as emergencies [28], and anticoagulation therapy or manageable medical conditions should not justify delaying surgery [29, 30]. However, early surgery may also increase the risk of stroke recurrence and mortality [16], as cerebrovascular autoregulation may not yet be fully restored post-stroke [27]. Guidelines suggest that elective surgery for patients with concomitant stroke should be postponed for 3–6 months or longer [13, 14, 16]. Despite these recommendations, there are currently no clear guidelines on whether and when to perform surgical hip repair in patients with acute stroke and hip fracture, and the relevant literature is limited. A 2017 study by Christiansen et al. [15] analyzed the risk of cardiovascular adverse events and mortality following non-cardiac, non-neurological emergency surgery at different times post-stroke. The study indicated that, compared to early surgery (performed 4–14 days post-stroke, 93 cases), patients who underwent immediate surgery (performed 1–3 days post-stroke, 69 cases) had a significantly lower risk of major adverse cardiovascular events within 30 days (P = 0.029), with no difference in 30-day all-cause mortality (P = 0.678). One case report described early closed reduction and internal fixation treatment for an intertrochanteric fracture with hemiplegia 30 days after acute stroke. At the 2-year follow-up, the patient had regained basic functional capacity, the fracture had healed well, and the Harris Hip Score was 75 [31]. In the absence of consistent guidelines, for patients with acute stroke and intertrochanteric fractures, the risks and benefits should be carefully weighed to develop individualized treatment strategies, including the surgical approach and timing.
Hypertension is an important risk factor for stroke. Consistent with our results, Mashour et al. [5] found that hypertension was an independent predictor of perioperative stroke (OR 3.8, 95% CI 3.1–4.7). Another study showed that elderly patients with acute ischemic stroke after hip fracture experienced hypertension more frequently (73.3%), which was associated with an increased risk of acute ischemic stroke after hip fracture (OR 2.8, 95% CI 1.6–5.1) [32]. The Perindopril Protection Against Recurrent Stroke Study (PROGRESS) results revealed that pharmaceutical antihypertensive therapies could reduce the risk of stroke in hypertensive individuals with a history of stroke [33]. A 2018 meta-analysis of eight trials showed that pharmaceutical antihypertensive therapies could reduce the stroke recurrence rate (8.7% vs. 10.1%) [34]. Regarding blood pressure targets, some studies have shown that intensive blood pressure reduction (systolic blood pressure target, < 110–130 mmHg) in elderly patients with hypertension can reduce the risk of stroke by 33% compared with standard blood pressure reduction (systolic blood pressure target, < 130–150 mmHg) [35]. Therefore, for patients with stroke and concomitant hypertension, appropriate antihypertensive treatment is necessary to control blood pressure within the ideal range and reduce the incidence of perioperative stroke.
In addition, we found that postoperative pneumonia was associated with stroke recurrence. Several studies have provided evidence that systemic infections may trigger or induce acute stroke [36]. A recent large prospective study in the United Kingdom found an increase in the risk of stroke in the days following acute upper respiratory or urinary tract infection [37]. Boehme et al. [38] reported that sepsis is significantly associated with an increased risk of ischemic stroke (OR 28.4, 95% CI 20.0–40.1) and hemorrhagic stroke (OR 12.1, 95% CI 7.5–19.4) within 15 days. Infection-induced inflammation and thrombosis may be the mechanisms underlying the increased stroke risk. However, the relationship between infections and stroke is bidirectional. Infections can cause strokes; however, strokes also induce immunosuppression, which then increases the risk of infection [39]. It is estimated that approximately one-third of patients with acute stroke develop pneumonia [40]. Stroke-induced immunosuppression predisposes patients to opportunistic infections, potentially leading to pneumonia or urinary tract infections and worsened stroke outcomes [39]. Thus, recognizing the possibility that pneumonia increases the risk of perioperative stroke recurrence and that stroke induces pneumonia is critical.
Therefore, it is crucial to develop targeted prevention strategies based on existing evidence to prevent stroke recurrence. First, patients with hip fractures, especially those with intertrochanteric fractures, should receive comprehensive systemic support when necessary. This may include blood transfusions, albumin infusion, and fluid support to ensure adequate cerebral perfusion. Second, perioperative blood pressure management is essential, particularly for patients with a history of hypertension. Individualized blood pressure targets should be established based on the patient’s specific conditions. Third, proactive infection prevention is necessary, especially for preventing pulmonary infections. Bedridden patients should be regularly repositioned, engaged in appropriate passive activities, and receive chest physiotherapy to facilitate sputum clearance. If an infection occurs, effective antibiotic treatment should be promptly administered.
The strength of this study was its identification of preoperative stroke and perioperative stroke recurrence using ICD-10 coding, which made it possible to report outcomes in relation to perioperative stroke recurrence in elderly patients with hip fracture and preoperative stroke, which have rarely been previously reported. In addition, the NIS database involves a large number of patients and uses a multicenter sampling method, meaning that the data are likely to be representative of common practice across the country. However, this study had some limitations. First, owing to the lack of certain intraoperative and postoperative indicators, we were unable to investigate the effects of anesthesia methods, bleeding volume, intraoperative blood pressure, surgical time, and postoperative anticoagulation therapy on stroke recurrence. Second, the incomplete information on stroke types and the lack of data concerning stroke times meant that the association between preoperative stroke subtypes and stroke recurrence could not be determined. Third, as the timing of pneumonia was not recorded, we were unable to determine if pneumonia is a risk factor for stroke recurrence or is a consequence of stroke itself.
Conclusions
The perioperative stroke recurrence rate in elderly hip fracture patients with previous stroke was 5.7%. Intertrochanteric fracture, hypertension, and postoperative pneumonia were identified as factors significantly associated with stroke recurrence in this study. Adequate systemic support post-fracture, effective blood pressure management, and proactive infection prevention may help reduce stroke recurrence, especially in patients with intertrochanteric fractures.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Youm T, Aharonoff G, Zuckerman JD, Koval KJ. Effect of previous cerebrovascular accident on outcome after hip fracture. J Orthop Trauma. 2000;14:329–34.
Griffiths R, Alper J, Beckingsale A, Goldhill D, Heyburn G, Holloway J, et al. Management of proximal femoral fractures 2011: Association of anaesthetists of Great Britain and Ireland. Anaesthesia. 2012;67:85–98.
Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int J Establ Result Coop Eur Found Osteoporos Natl Osteoporos Found USA. 2004;15:897–902.
Gs K, Mj P, Ga P. Mortality and morbidity after hip fractures. BMJ. 1993;307.
Luan L, Li R, Wang Z, Hou X, Gu W, Wang X, et al. Stroke increases the risk of hip fracture: a systematic review and meta-analysis. Osteoporos Int J Establ Result Coop Eur Found Osteoporos Natl Osteoporos Found USA. 2016;27:3149–54.
Wang W, Jiang B, Sun H, Ru X, Sun D, Wang L, et al. Prevalence, incidence, and mortality of stroke in China: results from a Nationwide Population-based survey of 480 687 adults. Circulation. 2017;135:759–71.
Ramnemark A, Nilsson M, Borssén B, Gustafson Y. Stroke, a major and increasing risk factor for femoral neck fracture. Stroke. 2000;31:1572–7.
Bateman BT, Schumacher HC, Wang S, Shaefi S, Berman MF. Perioperative acute ischemic stroke in noncardiac and nonvascular surgery: incidence, risk factors, and outcomes. Anesthesiology. 2009;110:231–8.
Mashour GA, Shanks AM, Kheterpal S. Perioperative stroke and associated mortality after noncardiac, nonneurologic surgery. Anesthesiology. 2011;114:1289–96.
Bateman BT, Schumacher HC, Wang S, Shaefi S, Berman MF. Perioperative Acute ischemic stroke in noncardiac and nonvascular surgery. Anesthesiology. 2009;110:231–8.
Vasivej T, Sathirapanya P, Kongkamol C. Incidence and risk factors of Perioperative Stroke in Noncardiac, and Nonaortic and its major branches surgery. J Stroke Cerebrovasc Dis off J Natl Stroke Assoc. 2016;25:1172–6.
Mashour GA, Moore LE, Lele AV, Robicsek SA, Gelb AW. Perioperative care of patients at high risk for stroke during or after non-cardiac, non-neurologic surgery: consensus statement from the Society for Neuroscience in Anesthesiology and critical Care*. J Neurosurg Anesth. 2014;26:273–85.
Benesch C, Glance LG, Derdeyn CP, Fleisher LA, Holloway RG, Messe SR, et al. Perioperative neurological evaluation and management to Lower the risk of Acute Stroke in patients undergoing noncardiac, nonneurological surgery: a Scientific Statement from the American Heart Association/American Stroke Association. Circulation. 2021;143:e923–46.
Glance LG, Benesch CG, Holloway RG, Thirukumaran CP, Nadler JW, Eaton MP, et al. Association of Time Elapsed since ischemic stroke with risk of recurrent stroke in older patients undergoing elective nonneurologic, noncardiac surgery. JAMA Surg. 2022;157:e222236.
Christiansen MN, Andersson C, Gislason GH, Torp-Pedersen C, Sanders RD, Foge Jensen P, et al. Risks of Cardiovascular adverse events and death in patients with previous stroke undergoing emergency noncardiac, nonintracranial surgery: the importance of operative timing. Anesthesiology. 2017;127:9–19.
Jørgensen ME, Torp-Pedersen C, Gislason GH, Jensen PF, Berger SM, Christiansen CB, et al. Time elapsed after ischemic stroke and risk of adverse cardiovascular events and mortality following elective noncardiac surgery. JAMA. 2014;312:269–77.
Steiner C, Elixhauser A, Schnaier J. The healthcare cost and utilization project: an overview. Eff Clin Pract ECP. 2002;5:143–51.
Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi J-C, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43:1130–9.
Quan H, Li B, Saunders LD, Parsons GA, Nilsson CI, Alibhai A, et al. Assessing validity of ICD-9-CM and ICD-10 administrative data in recording clinical conditions in a unique dually coded database. Health Serv Res. 2008;43:1424–41.
Frolova N, Bakal JA, McAlister FA, Rowe BH, Quan H, Kaul P, et al. Assessing the use of international classification of diseases-10th revision codes from the emergency department for the identification of acute heart failure. JACC Heart Fail. 2015;3:386–91.
van Walraven C, Austin PC, Jennings A, Quan H, Forster AJ. A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Med Care. 2009;47:626–33.
Lamo-Espinosa JM, Mariscal G, Gómez-Álvarez J, San-Julián M. Incidence and risk factors for stroke after hip fracture: a meta-analysis. Sci Rep. 2023;13:17618.
Gleason LJ, Mendelson DA, Kates SL, Friedman SM. Anticoagulation management in individuals with hip fracture. J Am Geriatr Soc. 2014;62:159–64.
Harper KD, Navo P, Ramsey F, Jallow S, Rehman S. Hidden preoperative blood loss with Extracapsular Versus Intracapsular Hip fractures: what is the difference? Geriatr Orthop Surg Rehabil. 2017;8:202–7.
Tengberg PT, Foss NB, Palm H, Kallemose T, Troelsen A. Tranexamic acid reduces blood loss in patients with extracapsular fractures of the hip: results of a randomised controlled trial. Bone Jt J. 2016;98–B:747–53.
Tüzün HY, Bilekli AB, Erşen Ö. The factors that affect blood loss in intertrochanteric fractures treated with proximal femoral nail in the elderly. Eur J Trauma Emerg Surg off Publ Eur Trauma Soc. 2022;48:1879–84.
Dawson SL, Panerai RB, Potter JF. Serial changes in static and dynamic cerebral autoregulation after acute ischaemic stroke. Cerebrovasc Dis. 2003;16:69–75.
White SM, Griffiths R, Holloway J, Shannon A. Anaesthesia for proximal femoral fracture in the UK: first report from the NHS hip fracture Anaesthesia Network. Anaesthesia. 2010;65:243–8.
Griffiths R, Babu S, Dixon P, Freeman N, Hurford D, Kelleher E, et al. Guideline for the management of hip fractures 2020: Guideline by the Association of Anaesthetists. Anaesthesia. 2021;76:225–37.
Switzer JA, O’Connor MI. AAOS Management of Hip fractures in older adults evidence-based Clinical Practice Guideline. J Am Acad Orthop Surg. 2022;30:e1297–301.
Zhang Z-L, Li X-S, Zhao W-Q, Huang J-F, Zhu Y-H. Early surgical treatment of closed reduction and internal fixation for a 30-day old intertrochanteric fracture with hemiplegia after acute stroke: a case report. Med (Baltim). 2023;102:e34098.
Zhang Y, Fu M, Guo J, Zhao Y, Wang Z, Hou Z. Characteristics and perioperative complications of hip fracture in the elderly with acute ischemic stroke: a cross-sectional study. BMC Musculoskelet Disord. 2022;23:642.
Randomised trial of. A perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet. 2001;358:1033–41.
Zonneveld TP, Richard E, Vergouwen MDI, Nederkoorn PJ, de Haan R, Roos YB, et al. Blood pressure-lowering treatment for preventing recurrent stroke, major vascular events, and dementia in patients with a history of stroke or transient ischaemic attack. Cochrane Database Syst Rev. 2018;7:CD007858.
Zhang W, Zhang S, Deng Y, Wu S, Ren J, Sun G, et al. Trial of intensive blood-pressure control in older patients with hypertension. N Engl J Med. 2021;385:1268–79.
Elkind MSV. Why now? Moving from stroke risk factors to stroke triggers. Curr Opin Neurol. 2007;20:51–7.
Kim Y-E, Huh K, Park Y-J, Peck KR, Jung J. Association between Vaccination and Acute Myocardial Infarction and ischemic stroke after COVID-19 infection. JAMA. 2022;328:887–9.
Boehme AK, Ranawat P, Luna J, Kamel H, Elkind MSV. Risk of Acute Stroke after hospitalization for Sepsis: a case-crossover study. Stroke. 2017;48:574–80.
Ghelani DP, Kim HA, Zhang SR, Drummond GR, Sobey CG, De Silva TM. Ischemic stroke and infection: a brief update on mechanisms and potential therapies. Biochem Pharmacol. 2021;193:114768.
Sellars C, Bowie L, Bagg J, Sweeney MP, Miller H, Tilston J, et al. Risk factors for chest infection in acute stroke: a prospective cohort study. Stroke. 2007;38:2284–91.
Acknowledgements
The authors thank the joint surgery department of Sun Yat-sen Memorial Hospital of Sun Yat-sen University for their help in obtaining the data from the NIS database.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
ZWH and CP were responsible for the study conception and design; FZR contributed to data acquisition; YB and CYL supervised the statistical analyses; ZWH interpreted the data; ZWH and QJ drafted the manuscript; YXB, WHZ and CHY critically revised and edited the manuscript; CP and WHZ supervised this study and was responsible for the integrity of the data and the accuracy of the analyses.
Corresponding author
Ethics declarations
Ethical approval
This study was exempt from formal review by the Ethics Committee of Guangdong Provincial Hospital of Chinese Medicine, given the use of de-identified, previously collected data.
Consent to participate
Not Applicable.
Consent for publication
Not Applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

{kind=link}
Cite this article
Chen, P., Zhang, W., Qi, J. et al. The incidence and risk factors of perioperative recurrent stroke in elderly patients with previous ischemic stroke receiving hip fracture surgery. BMC Musculoskelet Disord 25, 636 (2024). https://doi.org/10.1186/s12891-024-07753-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07753-y