
Abstract
Background
Despite the importance of enhancing exercise, exercising can cause injuries that lead to disability and increase the load on the medical sector. This study aimed to estimate the prevalence of exercise-related injuries among gym members in the Kingdom of Saudi Arabia (KSA) and evaluate the more common types of such injuries. It also investigated the association between injury prevalence and the factors selected.
Methods
A cross-sectional study with a self-reported survey was conducted targeting members of Fitness Time gyms across the KSA. The survey consisted of three parts: part one concerns participant demographic data and part two contains four questions regarding the participants’ training experience. Part three contains ten questions targeting those with a history of injury. Descriptive statistical analysis was performed using frequencies and percentages for categorical variables. Crosstabs and chi-squared tests were used to assess the prevalence of exercise-related injuries when appropriate. Binary logistic regression was employed to investigate the association between injury prevalence and the potential associated factors. Odds ratios and their 95% confidence intervals were calculated and the threshold for statistical significance was set at p ≤ 0.05.
Results
A total of 713 subjects participated in the study. The mean age was 36.5 ± 11.2 years and (n = 422, 59.2%) of the participants were female. The study found a prevalence of injury among gym members of about (n = 404, ~57%). The most commonly reported types of injuries were muscle strain (n = 126, 37%) and bruising (n = 45, 13%). The most prevalent anatomical location of injury was the knee (n = 287, 84.3%), followed by the shoulder (n = 283, 83.3%), and the least common was the head/neck (n = 7, 2.1%). The present study suggests some factors associated with exercise-related injury. A significant statistical association (p < 0.5) was found between injury prevalence and age, gender, educational level, period of training, and presence of a trainer. However, no association was detected between injury prevalence and Body Mass Index (BMI), place of residence, or source of advice.
Conclusion
Over half of the participants of this study reported at least one exercise-related injury. This study identifies factors associated with injury prevalence related to exercise among gym participants. Promoting safety and minimizing the incidence of injuries are crucial.
Similar content being viewed by others


Background
Physical inactivity is a well-established risk factor for numerous non-communicable diseases and shortens life expectancy [1]. With the current global high level of physical inactivity, encouraging physical activity (PA) has become an essential element of public health promotion [2]. Physical activity/exercise can significantly reduce the risk of developing serious health problems, such as type 2 diabetes, heart disease, obesity, and osteoporosis [3]. In addition to the benefits of activity/exercise for physical health, PA can also promote individuals’ mental health [4, 5]. To obtain those benefits, individuals need to exercise for at least 150–300 min of moderate-intensity aerobic PA or 75–150 min of vigorous-intensity PA throughout the week [6].
Many people attend gyms to enhance their health and fitness in order to achieve an ideal body [7,8,9]. Around the world, there were more than 184 million gym members before the COVID-19 pandemic [10]. With the global growth in gym members, the number of gyms and fitness centres is also increasing. In Australia, for example, there were approximately 6,462 gyms and fitness centres across the country in 2021 [11]. In the Kingdom of Saudi Arabia (KSA), there were 1,280 health/fitness clubs in 2019 [12]. The percentage of individuals aged 15 years or older who were engaged in sports activities rose from 17.4% in 2018 to 29% in 2021 [13, 14]. Recently, the trend for physical exercise has increased in the KSA, according to the Vision of the Kingdom 2030, and there is an intention to increase the number of sports clubs, sports academies, and sports centres [14].
Despite the benefits of exercise, exercising in an inappropriate way may increase the risk of musculoskeletal injuries and lead to disability [15, 16]. Musculoskeletal injury is the primary adverse event when performing exercise without prior awareness, which may force subjects to stop exercising [17]. Consequently, the promotion of exercise safety and injury-prevention strategies among gym members is needed to minimize the rate of injuries and pressure on the health sector, especially rehabilitation services [18, 19]. A number of studies have been conducted to estimate the prevalence of injury related to exercise and explore the most common types of such injuries [20,21,22]. A previous systematic review found that certain activities like gymnastics and weightlifting exhibit higher musculoskeletal injury rates than sports such as swimming or cycling [23]. In a cross-sectional study, Italian runners demonstrated a significant rate of running-related injuries, highlighting a notable prevalence of musculoskeletal issues among them [24]. Among gym members, an earlier cross-sectional study by Ristolainen et al. [21] reported that both acute and overuse injuries are more frequent, with 44.0% acute and 35% overuse injuries among gym members compared to 19.8% and 17.4%, respectively, among non-members [21]. This study included adolescents aged 14–16 years, which may limit the generalizability of the study findings in the other age groups [21]. In the KSA, a study conducted by Alwabli et al. [20] assessed 247 female gym members in Al-Qassim Province. Findings showed that approximately half the members experienced injuries due to exercise. The most commonly injured body part was the ankle (20.9%), followed by the knee (19.0%), and the most commonly injured soft tissues were the muscles (55.7%). Although this study confirmed evidence that exercise is a factor associated with different types of injury, its methodology had several limitations relating to gender and region [20]. Moreover, the current study was conducted to overcome the limitations in previous studies and fill the gap by including participants from both genders and different age groups across the KSA. It aims to estimate the prevalence of exercise-related injuries among gym members in the KSA and to evaluate the more common types of those injuries. It also aims to investigate the association between injury prevalence and the following factors: age, gender, body mass index (BMI), educational level, place of residence, period of training, presence of a trainer, and advice source.
Methods
A cross-sectional study was designed and reported in line with the STrengthening the Reporting of Observational studies in Epidemiology (STROBE) [25, 26]. An online survey was prepared using Google Forms software with a restricted consent form targeting the members of the Fitness Time gym in Saudi Arabia. Fitness Time was selected because it has approximately 140 branches across the KSA and 30,000 members. The study included registered members of the Fitness Time gym who were aged 15 years and above. Surveys with missing data were excluded from the analysis.
Sample size
A sample of registered Fitness Time gym members across the KSA was targeted to complete the survey. The sample size (n = 384) was estimated using the following equation: n = z2 ∗ p ∗ (1-p)/W², where n is the estimated sample size, z is the normal distribution (defined as 1.96 for research with 95% confidence), p is the estimated proportion of individuals who experienced exercise-related injury based on a previous study (50%) [20], and W is the study margin of error (5%) [27].
Outcome measure
An Arabic version of a previously developed survey was used after receiving permission to do so [20]. The survey is valid as it was used in the same population [20]. The survey contains three parts. Part one concerns participant demographic data (age, gender, height, weight, level of education, and region). The BMI was calculated based on the height and weight reported by the participants. Part two contains four closed-ended questions regarding the period of training, the presence of a trainer, sources of advice, and self-reported injuries. Part three contains ten questions targeting those who had a history of injury, such as the injury location, type, and management (see Supplementary file # 1).
Data collection
An advertising message that included a brief introduction to the study and a code for the online survey link was printed and distributed by Fitness Time’s main centre to other gyms in different regions across the KSA to reach all members. Hard copies of the advertising message were hung in different places in each gym to ensure its distribution. The survey was halted after one month and the data were downloaded for analysis.
Statistical analysis
SPSS statistical software package version 25 (IBM Corp., New York, USA) was used for all statistical analysis. Descriptive statistical analysis was performed using frequencies and percentages for categorical variables. Crosstabs and chi-squared tests were used to assess the prevalence of exercise-related injuries among the gym members when appropriate. Binary logistic regression was used to investigate the association between injury prevalence and factors that included age, gender, BMI, educational level, place of residence, period of training, presence of a trainer, and advice source. The odds ratios (ORs) and their 95% confidence intervals (95% CIs) were calculated and the threshold for statistical significance was set at p ≤ 0.05.
Results
Prevalence of exercise-related injury
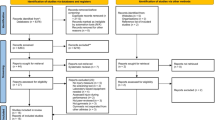
Over one month, 737 responses were received. After excluding incomplete surveys, 713 were included and analysed. The prevalence of exercise-related injuries was calculated to be approximately (n = 404, 57%). A flow diagram of the study participants is presented in Fig. 1.

Flowchart of study participation
Characteristics of the participants
The demographic characteristics of the participants are presented in Table 1. The largest group of participants contained those aged 31–40 years (n = 251,35.2%) and only (n = 17, 2.4%) were over the age of 60. About (n = 422, 59.2%) of the responses were from females. In terms of BMI, the largest group (n = 286, 40.1%) contained participants in the overweight category and the most common educational qualification level was a bachelor’s degree (n = 431,60.4%). The largest proportion of responses were received from participants in the Central Region of the KSA (n = 275, 38.6%).
Results regarding participants’ experience of training are presented in Table 2. More than half the participants (n = 439, 61.6%) had training experience for more than nine months. About (n = 390, 54.7%) of the participants had not been instructed by a trainer, and the majority of the participants (n = 694, 97.3%) had been advised on ways to avoid injuries while exercising. The most common source of advice was a personal trainer (n = 250, 35.1%). In summary of the demographic overview of participants, primarily aged 31–40, with a majority being female and having a bachelor’s degree. Most participants were from the Central Region of the KSA and had training experience exceeding nine months. While a considerable portion hadn’t been instructed by a trainer, nearly all had received advice on injury prevention, predominantly from personal trainers.
Self-reported injuries
This part of the results concerns self-reported injuries, including their locations, types, and management. The most common injury sites were the knee, shoulder, back, forearm and foot, and the least commonly injured sites were the head and neck (Fig. 2).

Most commonly injured parts of the body
Of the participants who reported an exercise-related injury, (n = 122, 36%) received an injury that affected the muscles, (n = 288, 85%) experienced pain immediately after the injury, (n = 111, 32%) reported using pain-relieving cream, and (n = 180, 53%) sought medical care. The most-reported diagnosis was muscle strain (n = 126, 37%). Most of the participants (n = 221, 65%) stated that they had experienced their first injury and (n = 201, 59%) reported that the injury stopped them exercising for at least five days. Most of the participants reported that there had been no other injuries (n = 226, 67%). Interestingly, (n = 250, 74%) of the participants who reported injuries had been training for at least one month (Table 3).
The study found that knee, shoulder, back, forearm, and foot were the most common injury sites among participants, with muscle strain being the predominant diagnosis. Despite most injuries causing immediate pain, only about half sought medical care, with a majority experiencing their first injury and being temporarily sidelined from exercise for at least five days. Notably, a significant portion of those reporting injuries had been training for at least one month.
Association between injury prevalence and predictor factors
A significant statistical association (p < 0.5) was found between injury prevalence and age, gender, educational level, period of training, and presence of a trainer (Table 4). Female participants were 1.5 times more likely to experience injury than males (p = 0.005, 95% CI, 1.136, 2.091). Participants aged 41–50 years were approximately five times more likely to experience injury than participants ≤ 20 years old (p = 0.005, 95% CI, 1.63, 16.52). Participants with a high school level of education were also five times more likely to sustain an injury compared to those who had a PhD (p = 0.047, 95% CI, 1.02, 27.03). Regarding the period of training, those who had joined the gym more than nine months previously were 2.7 times more likely to have an injury than those who had joined less than one month earlier (p = 0.006, 95% CI, 1.33, 5.59). Finally, those who had previously trained with a trainer but had stopped were 1.97 times more likely to experience injury than participants who trained with a trainer (p = 0.017, 95% CI, 1.13, 3.44). However, no association was detected between injury prevalence and BMI group, place of residence, or advice source (see Supplementary file #2).
Further analysis of eight predictor factors considering the participants’ gender and history of injury is presented in Supplementary file # 3.
The study revealed significant statistical associations between injury prevalence and various demographic and training-related factors, with females, individuals aged 41–50 years, those with a high school education, longer training periods, and cessation of training with a trainer showing higher likelihoods of experiencing injuries.
Discussion
This study aimed to estimate the prevalence of exercise-related injuries among gym members in Saudi Arabia in 2022 and to evaluate the more common types of such injuries. The study also sought to examine the association between injury prevalence and certain factors. The results showed that the prevalence of injury is about 57% among the gym members who participated in the survey (n = 713). This percentage is higher than the prevalence of injury among adolescents (46%) [22] and sports club members (44.0%) [21] in Finland. The prevalence is also higher than that in a study conducted in Qassim Province in the KSA, in which 49% reported having been injured [20]. The current study included participants aged 15 years and above and only (n = 46, 6.5%) were ≤ 20 years of age, whereas the two Finnish studies included adolescents [21, 22]. In addition, the current study included a larger sample size and both males and females about (n = 228, 32%) of whom were > 40 years of age, compared to the study conducted in the KSA that focused on female gym members (n = 274) only 8.9% of whom were > 40 years old [20]. However, according to a previous systematic review, injury in fitness centres could be due to various reasons, including overuse, inadequate post-exercise recovery periods, insufficient conditioning of targeted body regions, frequent application of heavy weights, and inappropriate technique in certain exercises [28].
The most commonly reported types of injury found in the current study were muscle strain (n = 126, 37%) followed by bruising (n = 45, 13%). This finding is in agreement with a study of Saudi female gym-goers, which found 56% of participants experienced muscle strain followed by 15.5% with bruising [20]; and a study conducted among Finnish adolescents that found that muscle injury (16.6%) accounted for the most common type of overuse injury among sports club members [21]. These findings are in agreement with the literature, as muscle injury is the most common type of sports injury, with more than 90% being due to contusion or muscle strain. Muscle strain could occur when an excessive pulling force is applied to muscle, causing overstretching [29].
The most prevalent anatomical location of injury reported in the current study was the knee (n = 287, 84.3%) followed by the shoulder (n = 283, 83.3%), and the least common site was the head/neck (n = 7, 2.1%). This result is consistent with findings from a Finnish study that reported the knee joint as the most common overuse injury location (16.8%) and the hand and wrist as the most commonly reported locations for acute injuries (13.6%) among sports club members, followed by the ankle (11.7%) [21]. In the study conducted in Al-Qassim, ankle injuries were more prevalent (20.9%), followed by injury to the knee joint (19%) [20]. Finding the knee joint to be the most common site of injury is not surprising, as it is the most commonly injured joint reported among young sports participants in other studies [30,31,32]. However, approximately 71.1% of the participants in the current study were overweight or obese (n = 507) and this supports the findings that a higher BMI may increase the risk of knee injuries, which can be attributed to the increased mechanical load on knee joints while exercising [33, 34].
In addition, the current study investigated eight factors that may be associated with the prevalence of musculoskeletal gym injuries to build knowledge for injury-prevention strategies. Five factors were found to be associated with the prevalence of injury: age, gender, educational level, period of training, and presence of a trainer.
Regarding age, participants aged 41–50 years (n = 147) who account for 20.6% of the participants and 59.86% of whom were female, were found to be more prone to injury (p = 0.005, 95% CI, 1.63, 16.52). This finding is in contrast to previous studies that found that injuries are common in younger participants [20, 35]. This may be due to participants in this age group behaving as if they were younger, even though there are physiological changes that occur in middle age, such as decreased muscle mass and flexibility, reduced bone density, and slower tissue repair. These factors can increase the vulnerability of middle-aged individuals to injuries during sports and exercise [36]. In addition, females are more at risk of having an injury than males in the current study, in contrast with studies on CrossFit athletes that reported that males are more likely to sustain injuries than females [37, 38]. One explanation for this is that the behaviour of males and young people is different when they are exercising as they may be greater risk takers compared to females and older people [21, 30, 31]. The contrasting finding in this study could relate to a lack of guidance from a trainer.
The presence of a personal trainer is important to prioritize and rationalize exercise for clients [39]. In the current study, just over half the participants (n = 390, 54.7%) had never been trained by a trainer and 51.3% had been injured in the absence of a trainer. The absence of a coach or guide has been found to be a predictor factor for injury prevalence, which is in contrast to previous findings that reported no significant statistical difference between those who trained with and those who trained without an instructor (p = 0.78) [19]. However, in fitness gyms, personal trainers have varied educational backgrounds, as well as varying knowledge of exercise [40]. Sometimes, personal trainers work beyond their scope of practice [41]. Thus, the advice provided in relation to exercise and training programmes can vary greatly among professional personal trainers, who also report common injuries among gym members [42].
The current study also found that those who had joined the gym more than nine months earlier were 2.7 times more likely to experience injury than those who had been members for less than one month. Most of the respondents had trained for more than nine months (n = 439, 61.6%), and those who had injuries about (40.7%). This supports the findings from previous study that showed a relation between the period of exercise participation and injury prevalence [43]. One possible explanation for that is that more participation in exercise may cause overuse injuries [21]. In contrast, a study in Finland [21] did not find a significant relation between injury prevalence and period of gym participation. This may relate to the participants’ age in the Finland study, as younger people have greater flexibility and mobility, which can contribute to better movement mechanics and reduce the risk of strains or overuse injuries during exercise [36].
Despite evidence of a positive relation between injury prevalence and a high BMI [20, 44], BMI was not found to be a predictor factor for injury in this study. This finding supports previous studies [44,45,46,47]. One possible reason could be that the respondents of this study undertook moderate-intensity exercise. It is known that exercise of moderate intensity does not pose a risk of injury when compared with high-intensity exercises [47].
Although this study was conducted in the KSA, the findings might fit into the larger picture of exercise-related injuries. Examining exercise-related injuries in gym members within various cultural and geographical contexts provides valuable insights into the multifaceted nature of fitness and health. By recognizing the factors that contribute to injury risk and tailoring interventions accordingly, stakeholders can work towards creating safer and more inclusive exercise environments for individuals worldwide [48]. Although the injury aetiologies are multifactorial, understanding the factors that are identified as associated with exercise-related injuries holds significant practical implications for gym trainers and fitness enthusiasts alike. By recognizing these factors, they can implement strategies to minimize the risk of injuries and promote safe and effective exercise practices.
Strengths and limitations of the study
Among the strengths of the current study are the size of the sample and that the gym members were located in all the regions of the KSA. In addition, the findings of this study provide information regarding the most common sites/soft tissues liable to injury. It also builds knowledge of injury prevention by identifying the predictor factors of musculoskeletal injury prevalence related to exercise among gym participants. However, this study also has some limitations. One major limitation is that the study design uses a self-reported survey, which might result in bias, especially with regard to the accuracy of the values of the participants’ BMI. The study also lacks information about the participants’ psychosocial life and the types, intensity, and duration of their exercise. Future research is required to investigate the causality of the suggested factors and injury prevalence, in order to develop suitable injury-prevention strategies.
Conclusion
The prevalence of injury among gym members in the KSA that took part in the study (n = 713) is about 57%. The most commonly reported types of injuries were muscle strain (n = 126, 37%) followed by bruises (n = 45, 13%). The most prevalent anatomical location of injury was the knee (n = 287, 84.3%), followed by the shoulder (n = 283, 83.3%), and the least common was the head/neck (n = 7, 2.1%). The present study suggests that being female, aged 41–50 years old, having a moderate level of education, and having been training for a period of more than nine months without the presence of a trainer or guide are all risk factors for sustaining exercise-related musculoskeletal injury. Consequently, considering these predictor factors and increasing participants’ awareness may promote safety and reduce the incidence of injuries. Reducing the prevalence of injury among participants is crucial to ensure that they have a good quality of life. It would also reduce the load and financial cost of the medical sector in having to treat fewer gym-related injuries.
Data availability
Any data related to this study can be provided by the corresponding author upon reasonable request.
Abbreviations
- BMI:
-
body mass index
- CI:
-
confidence interval
- KSA:
-
Kingdom of Saudi Arabia
- PA:
-
physical activity
- OR:
-
odds ratio
References
Washington DC, US Department of Health and Human Services. 2018 Physical Activity Guidelines Advisory Committee scientific report. 2018. https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf. Accessed 01 Aug 2023.
Lee I-M, Shiroma EJ, Lobelo F, et al. Effect of physical inactivity on major noncommunicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380:219–29.
Pavlović R, Solaković S, Simeonov A, et al. Physical activity and health: the benefits of physical activity in the prevention of diabetes mellitus and cardiovascular disorders. EJPESS. 2022;9:22–43.
Pascoe M, Bailey AP, Craike M, et al. Physical activity and exercise in youth mental health promotion: a scoping review. BMJ Open Sport Exerc Med. 2020;6:e000677.
Klaperski S, Koch E, Hewel D, et al. Optimizing mental health benefits of exercise: the influence of the exercise environment on acute stress levels and wellbeing. Ment Health Prev. 2019;15:200173.
World Health Organization. Physical activity. 2022. https://www.who.int/news-room/fact-sheets/detail/physical-activity. Accessed 01 Aug 2023.
Batrakoulis A, Veiga OL, Franco S, et al. Health and fitness trends in Southern Europe for 2023: a cross-sectional survey. AIMS Public Health. 2023;10:378–408.
Andreasson J, Johansson T. The fitness revolution: historical transformations in the global gym and fitness culture. Sport Sci Rev. 2014;23:91–111.
Sassatelli R. The commercialization of discipline: keep-fit culture and its values. J Mod Ital Stud. 2012;5:396–411.
IHRSA. The 2020 IHRSA global report. https://www.ihrsa.org/publications/the-2020-ihrsa-global-report/. Accessed 01 Aug 2023.
Statista Research Department. Number of fitness centers and gyms in Australia from financial year 2016 to 2021. https://www.statista.com/statistics/505441/australia-gym-and-fitness-centers/. Accessed 01 Aug 2023.
Number of health/fitness clubs in Africa and the Middle East in. 2019, by country. https://www.statista.com/statistics/308789/health-club-amount-in-africa-and-the-middle-east-countries/. Accessed 01 Aug 2023.
General Authority for Statistics. GASTAT. (17, 40%) of population are practicing sports for more than 150 minutes on a weekly basis. https://www.stats.gov.sa/en/news/315. Accessed 01 Aug 2023.
Saudi Vision. 2030 paves the way for building a distinguished future for the sports sector. https://mos.gov.sa/ar/mediacenter/news/Pages/n2262023.aspx. Accessed 01 Aug 2023.
Morrow J Jr, Defina L, Leonard D, et al. Meeting physical activity guidelines and musculoskeletal injury: the WIN study. MSSE. 2012;44:1986.
Caine D, Maffulli N, Caine C. Epidemiology of injury in child and adolescent sports: injury rates, risk factors, and prevention. Clin Sports Med. 2008;27:19–50.
Hootman JM, Macera CA, Ainsworth BE, et al. Epidemiology of musculoskeletal injuries among sedentary and physically active adults. Med Sci Sports Exerc. 2002;34:838–44.
Understanding the risks and benefits of physical activity important in public health. https://uk.humankinetics.com/blogs/excerpts/understandingthe-risks-and-benefits-of-physical-activity-important-inpublic-health. Accessed 01 Aug 2023.
Gilchrist J, Jones BH, Sleet DA, et al. Exercise-related injuries among women: strategies for prevention from civilian and military studies. MMWR Recomm Rep. 2000;49:13–33.
Alwabli Y, Al Ruwaili K, Alghadoni M, et al. Exercise-related injuries among female gym members in Qassim 2019. IJMDC. 2020;4:883–8.
Ristolainen L, Toivo K, Parkkari J, et al. Acute and overuse injuries among sports club members and non-members: the Finnish Health Promoting Sports Club (FHPSC) study. BMC Musculoskelet Disord. 2019;20:1–12.
Räisänen AM, Kokko S, Pasanen K, et al. Prevalence of adolescent physical activity-related injuries in sports, leisure time, and school: the National Physical Activity Behaviour Study for children and adolescents. BMC Musculoskelet Disord. 2018;19:1–8.
Trompeter K, Fett D, Platen P. Prevalence of Back pain in sports: a systematic review of the literature. Sports Med. 2017;47(6):1183–207.
Maselli F, Esculier JF, Storari L, et al. Low back pain among Italian runners: a cross-sectional survey. Phys Ther Sport. 2021;48:136–45.
Strengthening the reporting of observational studies in epidemiology. https://www.strobe-statement.org/. Accessed 04 July 2024.
Von Elm E, Altman DG, Egger M, et al. STrengthening the reporting of OBservational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335:806–8.
Ruano J, Teixeira VH. Prevalence of dietary supplement use by gym members in Portugal and associated factors. J Int Soc Sports Nutr. 2020;17:1–8.
Bonilla DA, Cardozo LA, Vélez-Gutiérrez JM, et al. Exercise selection and common injuries in fitness centers: a systematic integrative review and practical recommendations. IJERPH. 2022;19:12710.
Garrett WE Jr. Muscle strain injuries. Am J Sports Med. 1996; 24.6_suppl: S2-S8.
Almaawi A, Awwad W, Bamugaddam A, et al. Prevalence of knee injuries among male college students in Riyadh, Kingdom of Saudi Arabia. J Orthop Surg Res. 2020;15:1–8.
Louw Q, Grimmer K, Vaughan K. Knee injury patterns among young basketball players in Cape Town. South Afr J Sports Med. 2003;15:9–15.
Clayton RA, Court-Brown CM. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury. 2008;39:1338–44.
Pihlajamäki HK, Parviainen MC, Kautiainen H, et al. Incidence and risk factors of exercise-related knee disorders in young adult men. BMC Musculoskelet Disord. 2017;18:340.
Richmond SA, Nettel-Aguirre A, Doyle-Baker PK et al. Examining measures of weight as risk factors for sport-related injury in adolescents. J Sports Med. 2016:7316947.
Noteboom L, Kemler E, van Beijsterveldt AMC, et al. Factors associated with gym-based fitness injuries: a case-control study. JSAMS Plus. 2023;2:100032.
Amarya S, Singh K, Sabharwal M. Ageing process and physiological changes. In Gerontology. IntechOpen. 2018.
Weisenthal BM, Beck CA, Maloney MD, et al. Injury rate and patterns among CrossFit athletes. Orthop J Sports Med. 2014;2:2325967114531177.
Moran S, Booker H, Staines J, et al. Rates and risk factors of injury in CrossFit: a prospective cohort study. J Sports Med Phys Fit. 2017;57:1147–53.
Haman L, Yring H, Prell H, et al. Personal trainers’ health advice in the fitness gym space from a gender perspective. Int J Qual Stud Health Well-being. 2000;15:1794364.
Malek H, Nalbone D, Berger D, et al. Importance of health science education for personal trainers. J Strength Cond. 2002;16:19–24.
Anderson G, Elliott B, Woods N. The Canadian personal training survey. J Exerc Physiol Online. 2010;13:1–12.
Waryasz GR, Daniels AH, Gil JA, et al. Personal trainer demographics, current practice trends and common trainee injuries. Orthop Rev. 2016;8:6600.
Ristolainen L, Heinonen A, Turunen H, et al. Type of sport is related to injury profile: a study on cross country skiers, swimmers, long-distance runners and soccer players. A retrospective 12‐month study. Scand J Med Sci Sports. 2010;20:384–93.
Ezzat AM, Schneeberg A, Koehoorn M, et al. Association between body composition and sport injury in Canadian adolescents. Physiother Can. 2016;68:275–81.
Warsh J, Pickett W, Janssen I. Are overweight and obese youth at increased risk for physical activity injuries? Obes Facts. 2010;3:225–30.
Richmond SA, Kang J, Emery CA. Is body mass index a risk factor for sport injury in adolescents? J Sci Med Sport. 2013;16:401–5.
Janney CA, Jakicic JM. The influence of exercise and BMI on injuries and illnesses in overweight and obese individuals: a randomized control trial. IJBNPA. 2010;7:1–11.
Wiese-Bjornstal DM. Sociocultural aspects of sport injury and recovery. In Oxford research encyclopedia of psychology. 2018.
Acknowledgements
The author would like to thank the Leejam Sports Company (Fitness Time) for their help in collecting data. The author would also like to thank the participants.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
ASA: Conception, design of the study, acquisition of data, analysis and interpretation of data, drafting of manuscript, and critically revising the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the guidelines of the Declaration of Helsinki, and the protocol of this study was approved by the Institutional Review Board, College of Medicine, KSU (Reference no. 21/01151/IRB). An online informed consent form was embedded with the survey. The participants were informed of the study aim, methods, their voluntary participation, and the privacy and confidentiality of the collected information.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Alrushud, A.S. A cross-sectional study of musculoskeletal injuries related to exercise among gym members in Saudi Arabia in 2022: prevalence, common types, and predictor factors. BMC Musculoskelet Disord 25, 621 (2024). https://doi.org/10.1186/s12891-024-07733-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07733-2