
Abstract
Objective
With the development of surgical technology, the level of digital medicine is constantly improving. The birth of new technologies has a certain impact on traditional methods. At present, robot-assisted technology has been applied to patients with calcaneal fractures, which poses a challenge to traditional surgery. We aimed to assess whether robot-assisted internal fixation confers certain surgical advantages through a literature review.
Design
The databases PubMed, EMBASE, the Cochrane Library, the China National Knowledge Infrastructure (CNKI), and the Wanfang Data Knowledge Service Platform were systematically searched for both randomized and nonrandomized studies involving patients with calcaneal fractures.
Main results
Five studies were identified that compared clinical indexes. For the clinical indexes, robot-assisted surgery is generally feasible because of intraoperative fluoroscopy, complications, the Gissane angle, the calcaneal width, and the American Orthopedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot score 3 and 6 months after the operation (P < 0.05). However, on the operation time, Böhler’s angle at 3 and 6 months, Gissane angle and calcaneal width at 6 months after the operation did not show good efficacy compared with those of the traditional group (P > 0.05).
Conclusions
Based on the current evidence, the advantages of robot-assisted fixation over traditional fixation are clear. The long-term clinical effects of the two methods are also good, and the short-term effect of robot assistance is better. However, the quality of some studies is low, and more high-quality randomized controlled trials (RCTs) are needed for further verification.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Calcaneal fractures constitute approximately 1–2% of adult fractures and primarily result from sudden increases in high-energy axial load due to falls from heights and traffic accidents [1, 2]. Due to the mechanism of injury, 65 to 70% of calcaneal fractures usually present with subtalar joint displacement and posterior articular process collapse. Revised sentence: Calcaneal fractures pose a significant disability burden. Given the intricate anatomy and limited understanding of hindfoot kinematics, calcaneal fractures represent one of the most complex and contentious injuries [3, 4]. Currently, the main treatment options are surgery and conservative treatment. The occurrence of malunion, subtalar arthritis, and subfibular impingement is frequently observed as complications following treatment [5]. To reduce the incidence of complications, articular surface repair becomes inevitable. The optimal treatment for such fractures, however, remains a subject of ongoing debate [6, 7].
The current surgical methods include open reduction and internal fixation (ORIF), which are usually performed via two main methods. One is the extended lateral approach, which allows a comprehensive view of the fracture site and helps to finely reduce and stabilize bone fragments, reducing the difficulty caused by fixation, and the other is the sinus tarsi approach, which aims to minimize soft tissue destruction [8]. The percutaneous fixation technique involves the direct insertion of a screw into the fractured segment of the calcaneus through a small incision, offering advantages such as minimized soft tissue trauma and potentially expedited postoperative recovery [9, 10]. The alternative technique is external fixation, which necessitates the application of an external frame to uphold the alignment and stability of the calcaneal fracture. This approach is commonly employed in intricate fractures or circumstances where internal fixation is suboptimal. The external frame provides support and facilitates controlled adjustment, thereby contributing to overall stability. [11]. Surgery-related complications encompass infection, wound healing issues, internal fixation-related problems, post-traumatic arthritis, neurovascular injuries and more. The procedure requires meticulous preoperative planning, intraoperative monitoring and surgical expertise [12,13,14,15]. The extended lateral approach is currently considered the preferred method for treating intra-articular calcaneal fractures. [16, 17]. However, due to the weakness and single blood supply of the lateral calcaneal flap, approximately 20% of patients are affected by complications [18]. Therefore, there is an increasing endeavor to develop smaller alternatives in order to minimize soft tissue injury and subsequent complications, including the adoption of minimally invasive surgery (MIS), which represents a paradigm shift in surgical intervention methods. Computer-assisted surgery (CAS) has significantly enhanced the precision and accuracy of surgical intervention for calcaneal fractures, while 3D printing technology has introduced a personalized dimension to the management of such fractures [19,20,21,22,23,24]. Böhler’s angle and the Gissane angle were used to evaluate the reduction [25].
However, it is difficult to achieve functional reduction and precise plate and screw implantation in such a small field of view. The maintenance of reduction screw implantation necessitates repeated fluoroscopy, which still results in screw position bias due to the blind spot in the fluoroscopy angle, thereby augmenting the operator and patient’s radiation exposure risk. The utilization of robot-assisted techniques for the reduction and fixation of calcaneal fractures via the tarsal sinus approach significantly mitigates the potential risks associated with incision and radiation exposure [26, 27].
Therefore, it is controversial whether robot-assisted fixation has obvious advantages over traditional methods. The issue is currently being investigated and validated through numerous related experiments. As a result, we have compiled relevant articles and conducted a meta-analysis to establish an evidence-based foundation for medical practitioners’ decision-making.
Materials and methods
Search strategy
The literature was systematically reviewed by two investigators following the principles of the patient/population intervention comparison outcome model. The search keywords “robot” and “calcaneal fracture” were used in PubMed, EMBASE, The Cochrane Library, CNKI (China National Knowledge Infrastructure), and the Wanfang Data Knowledge Service Platform, specifically searching in the title/abstract field. These terms were connected using “AND” and “OR”. There were no limitations on initial time periods or languages; however, the deadline for inclusion was set as January 1, 2024. Eligible articles were selected based on predetermined criteria. In cases of disagreement between reviewers, more experienced individuals made final decisions regarding article selection.
Selection criteria
(1) Participants: The inclusion criteria were defined as follows: calcaneal fracture was diagnosed by imaging and specialist physical examination, and surgical treatment was performed after providing informed consent from the patients and their families. The study did not impose any age restrictions on the patients. The exclusion criteria were as follows: other severe concomitant disease and ineligibility for surgery; multiple fractures; and conservative treatment or external fixation.
(2) Intervention and comparison: The intervention group consisted of patients who underwent robot-assisted fixation, while the control group comprised patients who underwent traditional fixation alone. Patients who had undergone other surgical methods were excluded.
(3) Outcomes: The clinical indexes included the time to operation, number of intraoperative fluorographies and complications. The Böhler angle, Gissane angle, calcaneal width, and American Orthopedic Foot and Ankle Society (AOFAS) Ankle–Hindfoot score at 3 and 6 months post-surgery were utilized as the study’s research outcomes.
(4) Study design: The inclusion criteria encompassed randomized controlled trials and retrospective studies comparing robot-assisted fixation with conventional fixation techniques.
Quality assessment
We utilized the Cochrane Handbook to assess the risk of data from randomized controlled trials, and based on the findings, we categorized the studies into three tiers. Furthermore, for this retrospective study, we employed the Newcastle‒Ottawa Scale (NOS) to appraise the quality of the articles. Studies with NOS scores exceeding 5 were considered indicative of moderate to high-quality research.
Data extraction
The following data were extracted: first author, publication date, country, study design, number of patients, mean age, percentage of sex distribution, duration of follow-up examination (in months), and interventions. In cases of disagreement, a third reviewer made the final decision.
Data analysis and statistical methods
We utilized Review Manager, version 5.3, for data analysis. The odds ratio (OR) was employed to compute the dichotomous outcomes. Additionally, I² values were utilized to evaluate heterogeneity among articles. If I²> 50, a random effect model was applied; otherwise, a fixed effect model was selected.
Results
Search results
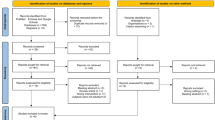
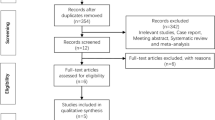
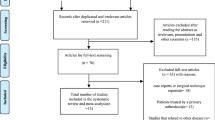
A total of 227 articles were identified through our query method, including 7 from PubMed, 5 from Embase, 1 from the Cochrane Library, 200 from CNKI, and 14 from the Wan Fang Data Knowledge Service Platform. Among these articles, a total of 31 studies were excluded due to duplication. Based on the evaluation of titles and abstracts, we selected a final set of 182 articles. After careful examination of their full texts for comprehension and relevance, only 5 articles met our inclusion criteria. The complete process of document screening is illustrated in Fig. S1.
Risk of bias assessment
In these incorporated documents, the methodological quality of the two types of experiments was assessed based on their respective evaluation criteria, as stated in the methods and materials section. Among the included studies, one was a randomized controlled trial (RCT), while the remaining were retrospective studies. The RCTs were deemed to possess superior quality, whereas the retrospective studies were considered to be of good quality; detailed contents are presented in Fig. 1.

Risk of bias assessment of the RCTs. (A) Risk of bias graph. (B) Risk of bias summary; quality assessment score of the retrospective study (C)
Study characteristics
The included articles consisted of one randomized controlled trial (RCT) and four retrospective studies, all of which were conducted at single-center institutions. Nearly every article provided comprehensive demographic information about the study population. Each article provided that the study population was composed of patients. Ultimately, our study included 253 people. Among them, 128 patients were in the traditional group, and 125 patients were in the robot-assisted fixation group. The characteristics of these studies are presented in Table 1.
Outcomes of the meta-analysis
Operation time
The analysis included three reports with a total of 177 cases, providing data on operation time. A random effects model was employed, revealing significant heterogeneity (I²=99%, P < 0.00001). Notably, the duration in the robot-assisted group was comparable to that observed in the traditional group. (RR=-11.04, 95% CI: -37.38, 15.29; P = 0.41). (Fig. 2A)

Forest plot diagram showing the operative time, number of intraoperative fluoroscopies and complications. (A) Operative time of robot-assisted fixation vs. traditional fixation. (B) Number of intraoperative fluoroscopies for robot-assisted fixation vs. traditional fixation. (C) Complications of robot-assisted fixation vs. traditional fixation
Intraoperative fluoroscopy times
Two reports provided intraoperative fluoroscopy data (n = 104). The analysis was conducted using a fixed model, and no significant heterogeneity was observed (I²=0%, P = 0.44). Consequently, robot-assisted fixation exhibits evident advantages over conventional methods in terms of reducing the need for intraoperative fluoroscopy procedures. (RR= -7.10, 95% CI: -7.65, -6.56, P < 0.00001). (Fig. 2B)
Complications
The analysis included four articles that provided relevant data on complications. Despite employing a fixed model, no heterogeneity was observed (I²=0%, P = 0.59). Notably, the experimental group exhibited a distinct advantage. (RR = 0.12, 95% CI: 0.04, 0.39; P = 0.0004). (Fig. 2C)
Imaging and functional evaluation at 3 months
Two studies with 165 patients reported the results of imaging and functional evaluation at 3 months. A fixed model was used for the Böhler angle, Gissane angle, and calcaneal width, and no heterogeneity was detected (Fig. 3A: Böhler angle, I²=0%, P = 0.85; Fig. 3B: Gissane angle, I²=0%, P = 0.45; Fig. 3C: Calcaneal width, I²=0%, P = 0.41). The imaging results of the robot-assisted group exhibited significantly superior outcomes compared to those of the traditional group, with the exception of Böhler’s angle. (Fig. 3A: Böhler angle, RR = 0.86, 95% CI: -0.02, 1.75, P = 0.06; Fig. 3B: Gissane angle, RR = 2.79, 95% CI: 1.75, 3.82, P < 0.00001; Fig. 3C: RR=-0.92, 95% CI: -1.37, -0.48, P < 0.0001). We still used a fixed model to evaluate the AOFAS score, and slight heterogeneity was found (I²=4%, P = 0.31). An advantage of the experimental group was shown (RR = 6.58, 95% CI: 3.78, 9.37; P < 0.00001; Fig. 3D).

Forest plot diagram showing the Böhler angle, Gissane angle, calcaneal width, and AOFAS score 3 months after surgery. (A) Böhler angle of robot-assisted fixation vs. traditional fixation. (B) Gissane angle of robot-assisted fixation vs. traditional fixation. (C) Calcanear width for robot-assisted fixation vs. traditional fixation. (D) AOFAS score of robot-assisted fixation vs. traditional fixation
Imaging and functional evaluation at 6 months
Two studies with 177 patients supported the use of imaging and functional evaluation at 6 months. Random models were used for Böhler’s angle, Gissane angle, and calcaneal width, and high heterogeneity was detected (Fig. 4A: Böhler’s angle, I²=69%, P = 0.07; Fig. 4B: Gissane angle, I²=75%, P = 0.02; Fig. 4C: Calcane width, I²=80%, P = 0.007). The imaging evaluations of the robot-assisted group and the traditional group were consistent. (Fig. 4A: Böhler angle, RR = 1.97, 95% CI: -0.33, 4.27, P = 0.09; Fig. 4B: Gissane angle, RR = 1.23, 95% CI: -2.00, 4.46, P = 0.46; Fig. 4C: RR=-0.50, 95% CI: -1.63, 0.62, P = 0.38). The AOFAS score was evaluated using a fixed model, and no heterogeneity was observed (I²=0%, P = 0.36). The experimental group demonstrated a distinct advantage. (RR = 4.92, 95% CI: 2.60, 7.25; P < 0.0001; Fig. 4D).

Forest plot diagram showing the Böhler angle, Gissane angle, calcaneal width, and AOFAS score at 6 months after surgery. (A) Böhler angle of robot-assisted fixation vs. traditional fixation. (B) Gissane angle of robot-assisted fixation vs. traditional fixation. (C) Calcanear width for robot-assisted fixation vs. traditional fixation. (D) AOFAS score of robot-assisted fixation vs. traditional fixation
Sensitivity analysis
We performed sensitivity analyses for indicators with heterogeneity > 80%. In terms of operation time (I²=74%, P = 0.05; Fig. 5A) and calcaneal width (I²=35%, P = 0.22; Fig. 5B), the heterogeneity was reduced, and the superiority of robot assistance was reflected. (operation time: RR= -26.30, 95% CI:-32.25, -20.35, P < 0.00001; Fig. 5A; calcaneal width: RR= -0.98, 95% CI:-1.63, -0.33, P = 0.003; Fig. 5B)

Forest plot diagram showing the sensitivity analysis of the operation time and calcaneal width: (A) operation time for robot-assisted fixation vs. traditional fixation and (B) calcaneal width for robot-assisted fixation vs. traditional fixation
Discussion
The calcaneus is a thin cortical structure with a large amount of cancellous bone, and its anatomical appearance is complex. The Sanders classification is the most widely utilized system for evaluating intra-articular calcaneal fractures, based on the number of intra-articular fracture lines observed in coronary computed tomography (CT) scans. [28]. The treatment of Sanders type II and III calcaneal fractures is difficult. If not treated properly, the disability rate is approximately 30% [29, 30]. The key to surgical treatment of calcaneal fractures is to restore the height, length, width, and force line of the bone, anatomically reduce the subtalar articular surface of the calcaneus, and provide strong fixation to restore function to the greatest extent.
It was concluded from our analysis that robot-assisted operation did not have an advantage in terms of operation time, and we subsequently conducted a sensitivity analysis to exclude the surgical indicators of Yuan’s article, reflecting the superiority of robot-assisted operation time [31]. The reasons related to the long operation time were analyzed. First, robot-assisted surgery adds preliminary steps such as intraoperative scanning and reconstruction and screw implantation planning [32]. Second, surgeons may not be proficient in surgical robot operation, but the learning curve of robot-assisted surgery is short, and clinicians can quickly master assisted technology after training. Third, because the length of the screw cannot be clearly determined by hand, repeated removal of the screw may occur, which significantly increases the number of fluoroscopies and prolongs the operation time [33, 34].
The robot-assisted group experienced minimal complications. The main complications were wound infection and poor healing, which resolved after dressing change and debridement [35]. Receiving timely intervention for any pertinent indications guarantees optimal wound healing and minimizes the likelihood of complications [36]. The presence of implant-related complications, such as plate or screw loosening, may necessitate revision surgery to address issues of instability or discomfort. Regular follow-up assessments, imaging studies, and patient feedback are imperative in identifying and managing hardware-related complications to ensure the stability and efficacy of fixation [13, 37]. Despite undergoing surgical intervention, some patients may develop posttraumatic arthritis, particularly in cases where the joints are severely affected. Over time, arthritic changes can occur, impacting joint functionality and causing discomfort. This long-term complication may necessitate ongoing treatment such as pain management strategies, lifestyle adjustments, or in severe instances, joint replacement or fusion surgery [14, 38]. With the continuous progress in computer technology, biomechanics and medicine, people have gradually designed more excellent internal fixation materials and found better internal fixation methods [39,40,41,42].
The absence of a statistically significant difference in fracture recovery time was also observed. [27]. In the measurement of Bohler’s angle, we found no difference between the two groups in the short-term or long-term follow-up. On the other hand, in the short-term measurements of the Gissane angle and calcaneal width, robot assistance showed advantages, but this difference gradually disappeared with fracture rehabilitation. However, in the short-term and long-term evaluation of AOFAS function, robot assistance has obvious advantages, possibly because the orthopedic robot has a navigation system that can monitor screw placement in real time during surgery, thereby improving the reduction accuracy and alignment of fracture fragments [31].
The advantage of robot-assisted surgery lies in the application of preoperative planning tools to achieve “digital” surgery, personalized planning of screw placement channels, and “precision” and “homogeneity” of key surgical operations. This approach avoids the loss of internal fixation stability caused by traditional surgery based on hand feelings and experience. The disadvantage is that the patient’s position needs to be kept unchanged during the operation; otherwise, the adjustment needs to be proofread, and the operation time is increased.
The rehabilitation protocol after surgery is equally important, with early mobilization aimed at preventing stiffness and promoting joint function [43]. The physical therapy sessions are centered around the restoration of range of motion, enhancement of muscular strength, and optimization of functional mobility [44]. The implementation of a weight-bearing protocol with protective measures was employed to minimize excessive pressure on the surgically reconstructed calcaneus during the initial phase of rehabilitation [45]. Gait training is crucial for postoperative rehabilitation following calcaneal fracture surgery. Ensuring accurate and efficient walking patterns can effectively prevent gait abnormalities and associated complications [46]. The regular monitoring of patient progress enables the modification of the rehabilitation program according to individual responses and rehabilitation trajectories [47].
However, there are limitations to our study. First, the number of articles and the sample size were small, and second, there was some heterogeneity in some indicators, which may have affected the overall results. We hope that future work will include more studies and randomized controlled trials.
Conclusion
Current evidence indicates that robot-assisted treatment is as safe, feasible and effective as ORIF in the treatment of calcaneal fractures. Compared with ORIF, robot-assisted surgery is superior for postoperative recovery. Robot assistance can provide a safe and feasible alternative to ORIF.
Data availability
The data can be obtained by DOI: 10.1111/os.13650; DOI: 10.19548/j.2096-269x.2023.06.007; DOI: 10.7507/1002-1892.202101029; DOI:10.3760/cma.j.cn501098-20220627-00457; GB/7 7714-2015
Abbreviations
- CNKI:
-
China National Knowledge Infrastructure
- AOFAS:
-
American Orthopedic Foot and Ankle Society
- RCTs:
-
Randomized controlled trials
- ORIF:
-
Reduction and internal fixation
- MIS:
-
Minimally invasive surgery
- CAS:
-
Computer-assisted surgery
- NOS:
-
Newcastle‒Ottawa Scale
- OR:
-
Odds ratio
- CT:
-
Computed tomography
References
Kamath KR, Mallya S, Hegde A. A comparative study of operative and conservative treatment of intraarticular displaced calcaneal fractures, (2045–2322 (Electronic)).
Schippers P, Engels R, Benning D, Fischer S, Wunderlich F, Afghanyar Y, Arand C, Nienhaus M, Drees P, Gercek E, Küchle R. Functional outcomes after intramedullary nailing (C-Nail®) of severe calcaneal fractures with mean follow-up of 36 months, European journal of trauma and emergency surgery. official publication of the European Trauma Society; 2024.
Park CA-O, Yan H, Park J. Randomized comparative study between extensile lateral and sinus tarsi approaches for the treatment of Sanders type 2 calcaneal fracture, (2049–4408 (Electronic)).
Biz CA-O, Refolo M, Zinnarello FD, Crimì AA-O, Dante F, Ruggieri PA-O. A historical review of calcaneal fractures: from the crucifixion of Jesus Christ and Don Juan injuries to the current plate osteosynthesis, (1432–5195 (Electronic)).
Ma C, Zhao J, Zhang Y, Yi N, Zhou J, Zuo Z, Jiang B. Comparison of the modified sinus tarsi approach versus the extensile lateral approach for displaced intra-articular calcaneal fractures, (2305–5839 (Print)).
Kline AJ, Anderson Rb Fau WH, Davis CP Davis Wh Fau - Jones, B.E. Jones Cp Fau - Cohen, Cohen BE. Minimally invasive technique versus an extensile lateral approach for intra-articular calcaneal fractures, (1071 – 1007 (Print)).
Mehta CA-O, An VVG, Phan K, Sivakumar B, Kanawati AJ, Suthersan M. Extensile lateral versus sinus tarsi approach for displaced, intra-articular calcaneal fractures: a meta-analysis, (1749-799X (Electronic)).
Cai YT, Song YK, He MC, He XM, Wei QS, He W. Global research trends and hotspots in calcaneal fracture: a bibliometric analysis (2000–2021). Front Surg. 2022;9:940432.
Smith M, Medlock G, Johnstone AJ. Percutaneous screw fixation of unstable ankle fractures in patients with poor soft tissues and significant co-morbidities. Foot Ankle Surgery: Official J Eur Soc Foot Ankle Surg. 2017;23(1):16–20.
Biz C, Barison E, Ruggieri P, Iacobellis C. Radiographic and functional outcomes after displaced intra-articular calcaneal fractures: a comparative cohort study among the traditional open technique (ORIF) and percutaneous surgical procedures (PS). J Orthop Surg Res. 2016;11(1):92.
Hadeed A, Werntz RL, Varacallo M. External Fixation Principles and Overview, StatPearls, StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC., Treasure Island (FL) ineligible companies. Disclosure: Ryan Werntz declares no relevant financial relationships with ineligible companies. Disclosure: Matthew Varacallo declares no relevant financial relationships with ineligible companies., 2024.
Guo S, Dipietro LA. Factors affecting wound healing. J Dent Res. 2010;89(3):219–29.
Hernandez Rosa J, Villanueva NL, Sanati-Mehrizy P, Factor SH, Taub PJ. Review of maxillofacial hardware complications and indications for salvage. Craniomaxillofacial Trauma Reconstruction. 2016;9(2):134–40.
Punzi L, Galozzi P, Luisetto R, Favero M, Ramonda R, Oliviero F, Scanu A. Post-traumatic arthritis: overview on pathogenic mechanisms and role of inflammation. RMD open. 2016;2(2):e000279.
Beutel BG, Lifchez SD, Melamed E. Neurovascular complications of the Upper Extremity following Cardiovascular procedures. J hand Microsurgery. 2016;8(2):65–9.
Khazen G, Rassi CK. Sinus Tarsi Approach for Calcaneal Fractures: The New Gold Standard? (1558–1934 (Electronic)).
Bernasconi AA-O, Iorio P, Ghani Y, Argyropoulos M, Patel S, Barg A, Smeraglia F, Balato G, Welck M. Use of intramedullary locking nail for displaced intraarticular fractures of the calcaneus: what is the evidence? (1434–3916 (Electronic)).
Schepers T. The sinus tarsi approach in displaced intra-articular calcaneal fractures: a systematic review, (1432–5195 (Electronic)).
Weber M, Lehmann D, Fau - Sägesser O, Sägesser F, Krause DF, Krause F. Limited open reduction and internal fixation of displaced intra-articular fractures of the calcaneum, (2044–5377 (Electronic)).
Zhang B, Lu H, Quan Y, Wang Y, Xu HA-O. Fract Mapp intra-articular Calcaneal Fractures, (1432–5195 (Electronic)).
Zheng W, Xie L, Xie H, Chen C, Chen H, Cai L. With versus without bone grafts for operative treatment of displaced intra-articular calcaneal fractures: a meta-analysis, (1743–9159 (Electronic)).
Kiewiet NJ, Sangeorzan BJ. Calcaneal Fracture Management: Extensile Lateral Approach Versus Small Incision Technique, (1558–1934 (Electronic)).
Park HJ, You KH, Huang B, Yoon JH, Kim HN. Can 3-Dimensional Printing for Calcaneal fracture surgery decrease operation time and improve quality of fracture reduction? J foot Ankle Surgery: Official Publication Am Coll Foot Ankle Surg. 2023;62(1):21–6.
Mao JT, Chen CM, Lin CW, Lu HL, Kuo CC. Comparison of the Radiographic and clinical outcomes between the Sinus Tarsi and extended lateral approaches for Intra-articular Calcaneal fractures: a retrospective study. J Personalized Med 14(3) (2024).
Seat A, Seat C. Lateral Extensile Approach Versus Minimal Incision Approach for Open Reduction and Internal Fixation of Displaced Intra-articular Calcaneal Fractures: A Meta-analysis, (1542–2224 (Electronic)).
Ceccarini P, Manfreda F, Petruccelli R, Talesa G, Rinonapoli G, Caraffa A. Minimally invasive sinus tarsi approach in Sanders II-III calcaneal fractures in high-demand patients, (1840–2445 (Electronic)).
Yuan XA-O, Tan K, Hu J, Zhang B, Zhang HA-O. Does robot-assisted percutaneous hollow screw placement combined with tarsal sinus incision reduction in the treatment of calcaneal fracture perform better at a minimum two year follow-up compared with traditional surgical reduction and fixation? (1432–5195 (Electronic)).
Li Z, Xiao F, Huang H, Xia J, Zhou H, Li B, Yang Y. Impact of sustentaculum tali screw positioning on radiographic and functional outcomes in calcaneal fractures. J Orthop Surg Res. 2024;19(1):136.
Rao K, Dibbern K, Day M, Glass N, Marsh JL, Anderson DD. Correlation of Fracture Energy with Sanders classification and post-traumatic osteoarthritis after displaced intra-articular calcaneus fractures. J Orthop Trauma. 2019;33(5):261–6.
Bernstein J, Ahn J. Brief: fractures in brief: calcaneal fractures. Clin Orthop Relat Res. 2010;468(12):3432–4.
Yuan X, Zhang B, Hu J, Lu B, Tang Z. A comparative study on internal fixation of calcaneal fractures assisted by robot and traditional open reduction internal fixation]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021;35(6):729–33.
Yuan X, Zhang B, Hu J, Lu B, Tang Z. [A comparative study on internal fixation of calcaneal fractures assisted by robot and traditional open reduction internal fixation], Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi = Zhongguo Xiufu chongjian waike zazhi = Chinese. J Reparative Reconstr Surg. 2021;35(6):729–33.
Pazour J, Horák Z, Džupa V. Does the position of a sustentacular screw influence the stability of a plate osteosynthesis of a calcaneal fracture? A biomechanical study. Proc Inst Mech Eng H. 2021;235(9):993–1000.
Parekh J, Shepherd DE, Hukins DW, Hingley C, Maffulli N. In vitro investigation of friction at the interface between bone and a surgical instrument, Proceedings of the Institution of Mechanical Engineers. Part H, Journal of engineering in medicine 227(6) (2013) 712-8.
Zhang Jinfeng C, Yimin W, Junqiang H, Wei S, Yonggang F, Han Z, Xuelin W, Jing. Comparison of robot-assisted percutaneous cannulated screw fixation and open reduction internal fixation in the treatment of Sanders II II;//III III calcaneal fractures: a retrospective cohort study. J Clin Orthop Res. 2023;8(06):356–62.
Backes M, Schepers T, Beerekamp MS, Luitse JS, Goslings JC, Schep NW. Wound infections following open reduction and internal fixation of calcaneal fractures with an extended lateral approach. Int Orthop. 2014;38(4):767–73.
Nouh MR. Spinal fusion-hardware construct: basic concepts and imaging review. World J Radiol. 2012;4(5):193–207.
Biz C, Hoxhaj B, Aldegheri R, Iacobellis C. Minimally invasive surgery for tibiotalocalcaneal arthrodesis using a Retrograde Intramedullary nail: preliminary results of an innovative modified technique. J foot Ankle Surgery: Official Publication Am Coll Foot Ankle Surg. 2016;55(6):1130–8.
Ouyang H, Deng Y, Xie P, Yang Y, Jiang B, Zeng C, Huang W. Biomechanical comparison of conventional and optimised locking plates for the fixation of intraarticular calcaneal fractures: a finite element analysis. Comput Methods Biomech BioMed Eng. 2017;20(12):1339–49.
Zhang H, Lv ML, Liu Y, Sun W, Niu W, Wong DW, Ni M, Zhang M. Biomechanical analysis of minimally invasive crossing screw fixation for calcaneal fractures: implications to early weight-bearing rehabilitation, clinical biomechanics (Bristol. Avon). 2020;80:105143.
Wilkinson BG, Marsh JL. Minimally invasive treatment of displaced intra-articular calcaneal fractures. Qld Gov Min J. 2020;51(3):325–38.
Eftekhar Ashtiani R, Alam M, Tavakolizadeh S, Abbasi K. The Role of Biomaterials and Biocompatible Materials in Implant-Supported Dental Prosthesis, Evidence-based complementary and alternative medicine: eCAM 2021 (2021) 3349433.
Aprisunadi N, Nursalam M, Mustikasari E, Ifadah ED, Hapsari. Effect of early mobilization on hip and lower extremity postoperative: a Literature Review. SAGE open Nurs. 2023;9:23779608231167825.
Pollock A, Baer G, Campbell P, Choo P.L., Forster A, Morris J, Pomeroy V.M., Langhorne P. Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochrane Database Syst Rev. 2014;20144:Cd001920.
Anderson TB, Duong H, Bearing W. StatPearls, StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC., Treasure Island (FL) ineligible companies. Disclosure: Hieu Duong declares no relevant financial relationships with ineligible companies.; 2024.
Shousha TM, Abo-Zaid NA, Hamada HA, Abdelsamee MYA, Behiry MA. Virtual reality versus Biodex training in adolescents with chronic ankle instability: a randomized controlled trial. Archives Med Science: AMS. 2023;19(4):1059–68.
Cunha B, Ferreira R, Sousa ASP. Home-Based Rehabilitation of the shoulder using Auxiliary systems and Artificial Intelligence: an overview, sensors. (Basel Switzerland) 23(16) (2023).
Acknowledgements
Not Applicable.
Funding
The present study received financial support from the National Natural Science Foundation of China (82002365) and the Natural Science Foundation of Cangzhou (221001009D).
Author information
Authors and Affiliations
Contributions
Search articles- Jiaxin Shen,; Data analysis-all authors; Manuscript preparation-all authors; Manuscript revision-all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not Applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Shi, J., Shen, J., Guo, W. et al. Robot-assisted versus traditional fixation for the treatment of calcaneal fractures: a meta-analysis. BMC Musculoskelet Disord 25, 591 (2024). https://doi.org/10.1186/s12891-024-07726-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07726-1