
Abstract
Background
Physiotherapeutic management is the first-line intervention for patients with entrapment neuropathies such as carpal tunnel syndrome (CTS). As part of physiotherapy, neurodynamic interventions are often used to treat people with peripheral nerve involvement, but their mechanisms of action are yet to be fully understood. The MONET (mechanisms of neurodynamic treatment) study aims to investigate the mechanisms of action of neurodynamic exercise intervention on nerve structure, and function.
Methods
This mechanistic, randomised, single-blind, controlled trial will include 78 people with electrodiagnostically confirmed mild or moderate CTS and 30 healthy participants (N = 108). Patients will be randomly assigned into (1) a 6-week progressive home-based neurodynamic exercise intervention (n = 26), (2) a steroid injection (= 26), or (3) advice (n = 26) group. The primary outcome measure is fractional anisotropy of the median nerve at the wrist using advanced magnetic resonance neuroimaging. Secondary outcome measures include neuroimaging markers at the wrist, quantitative sensory testing, electrodiagnostics, and patient reported outcome measures. Exploratory outcomes include neuroimaging markers at the cervical spine, inflammatory and axonal integrity markers in serial blood samples and biopsies of median nerve innervated skin. We will evaluate outcome measures at baseline and at the end of the 6-week intervention period. We will repeat questionnaires at 6-months. Two-way repeated measures ANCOVAs, followed by posthoc testing will be performed to identify differences in outcome measures among groups and over time.
Discussion
This study will advance our understanding of the mechanisms of action underpinning neurodynamic exercises, which will ultimately help clinicians to better target these treatments to those patients who may benefit from them. The inclusion of a positive control group (steroid injection) and a negative control group (advice) will strengthen the interpretation of our results.
Trial registration
NCT05859412, 20/4/2023.
Similar content being viewed by others


Background
Clinical guidelines recommend a conservative approach to entrapment neuropathies in people who present with mild to moderate symptoms [1,2,3]. Regardless of the type of entrapment neuropathy, the leading conservative treatments include steroid injection, and physical therapy [4, 5]. Various physical therapy modalities are offered as first-line interventions to manage symptoms before more invasive options (e.g., surgery) are considered [6,7,8]. Neurodynamic interventions have been incorporated as part of the physical therapy management of patients with peripheral nerve injuries, including entrapment neuropathies [8,9,10].
Neurodynamic interventions are aimed at restoring the homeostasis in and around the nervous system, by gliding the nerve in relation to its surrounding tissue while minimising neural strain [11,12,13]. These neurodynamic interventions facilitate the movement between neural structures and their surroundings (interface) by using a combination of joint movements or exercise [12]. Their efficacy has been confirmed as part of a combined intervention with education and splinting in some people with carpal tunnel syndrome (CTS) [14]. The uncertainty about the magnitude and specificity of these improvements in the wider population with CTS could be addressed by better understanding the mechanisms of action of neurodynamic exercises to identify those most likely to benefit.
Preclinical studies in animal models have investigated the mechanism of action of neurodynamic treatments suggesting an anti-inflammatory effect by reducing proinflammatory cytokines [15] and glial activation [16, 17]. There is also increasing in-vivo and in-vitro evidence that they may have a pro-regenerative and/or anti-degenerative effect on peripheral nerves [18,19,20] and can reduce the intraneural scar formation in a model of chronic constriction injury [21]. In humans, neurodynamic exercises in combination with other conservative treatments modified mechanical properties of peripheral nerves (i.e., decreased nerve stiffness) [22] and improved sensory and motor conduction velocities [23] along with pinch and grip strength [24]. Our previous study [25] showed changes in intraneural oedema using neurodynamic exercises only, but apart from T2 signal intensity, no advanced imaging or other mechanistic markers were included. How neurodynamic exercises in isolation can contribute to the pro-regenerative effect on peripheral nerves, changes in somatosensory function and the dispersion of inflammatory by-products are yet to be explored [25, 26].
A better understanding of how neurodynamic interventions work is an important first step towards personalised and precision physical therapy. We have previously shown that a set of eight nerve and tendon gliding exercises have a positive impact on symptoms [14] and can reduce MRI signals of oedema within the affected median nerve in patients with CTS [25]. CTS is an ideal model system to explore the mechanisms of action of neurodynamic treatments. It is the most common entrapment neuropathy [27] and provides good access to investigations of the function and structure of the affected nerve. We have demonstrated the presence of nerve degeneration and regeneration [26], intraneural [25], and systemic inflammation [28] using CTS as a model system. Importantly, patients with CTS are routinely treated with steroid injection (a potent anti-inflammatory medication), which has established short term benefits [29] and can therefore serve as a positive control treatment.
This single-blind randomised mechanistic controlled trial therefore uses CTS as a model system to investigate the mechanisms of action of a 6-week progressive home-based neurodynamic exercise intervention on nerve function, structure and neuroinflammation in patients with CTS compared to a positive control intervention (steroid injection) and a negative control intervention (advice). We will also include a healthy control group who will provide normative data on nerve structure, function, and inflammatory markers. The deep and comprehensive phenotyping of our patient cohort includes different advanced neuroimaging sequences (i.e., diffusion, T2 mapping and anatomical images with magnetisation transfer preparation) that combined with our functional (i.e., quantitative sensory testing, nerve conduction studies, serum protein levels in blood) could help disentangle the mechanisms of action of neurodynamic exercises locally. In future analyses, we will explore whether these neurodynamic exercises have an effect proximally at the level of the dorsal root ganglia (DRG).
Methods
This randomised, mechanistic, single blind, controlled trial will be carried out at Oxford University, UK, and will be reported according to the CONSORT guidelines [30].
Participants
We will include people with a confirmed diagnosis of mild or moderate of CTS based on clinical [31] and electrodiagnostic [32] criteria.
We will identify eligible patients from the neurophysiology department at Oxford University Hospitals Foundation NHS Trust (OUH), primary care services and through public advertisement (flyers, leaflets, community notice boards, emailing lists and social media). An age and gender matched cohort of healthy volunteers recruited through flyers, leaflets, community notice boards, emailing lists and social media will be included to establish normative data.
Inclusion criteria for people with CTS and healthy controls include being 18 years or older, willing, and able to give informed consent for participation in the study, and having sufficient command of the English language to complete questionnaires and the detailed assessments. The electrodiagnostic testing will include median, ulnar and radial nerve sensory and motor studies to determine the presence of CTS and the absence of other peripheral neuropathies, according to established protocols [32]. The temperature of the hand will be standardised before testing to > 31 °C. Sensory nerve action potential latencies, amplitudes and nerve conduction velocities will be recorded orthodromically over the wrist for the median (index finger), ulnar (little finger) and superficial radial nerve (snuffbox). Compound muscle action potentials will be registered for the median nerve (abductor pollicis brevis stimulated from the wrist and antecubital fossa), and ulnar nerve (adductor digiti minimi stimulated from the wrist, below and above the elbow). Additionally, we will record orthodromic sensory nerve action potentials by stimulating the ring finger and register the response at the wrist. The presence of a ‘double peak’ (increased latency of median sensory nerve action potential compared to ulnar sensory nerve action potential) will be classified as abnormal [33]. The motor latency difference between the median nerve (second lumbrical) and ulnar nerve (palmar interossei) will be assessed over a fixed distance of 8 cm with a delay of the median motor potential relative to the ulnar latency > 0.4 ms deemed abnormal [34].
The severity of CTS will be graded according to Bland’s criteria [32]. Only patients with mild (sensory conduction velocity from index finger to wrist < 40 m/s with motor terminal latency from wrist to abductor pollicis brevis [APB] < 4.5 ms) and moderate CTS (motor terminal latency > 4.5ms and < 6.5ms with preserved index finger sensory nerve action potential) will be included. People with severe CTS are recommended surgery according to clinical guidelines [1, 2] and thus will not be included in this study.
People with CTS will be excluded if they had previous ipsilateral CTS surgery (patients with unilateral surgery on the non-study hand are eligible to participate) or are planning to undergo surgery in the next 6 weeks, had a steroid injection for their CTS in the 6 months prior to the study enrolment or who had already more than 1 steroid injection, have an electrodiagnostic test that reveals abnormalities other than CTS (e.g., ulnar neuropathy), present with another medical condition affecting the upper limb or neck (e.g., rheumatoid arthritis, cervical radiculopathy or myelopathy), a history of significant trauma to the upper limb or neck, diabetes, hypothyroidism, severe anxiety or depression, altered coagulation (e.g., haemophilia) or having strong anticoagulant medication that prevents skin biopsies, contraindications for steroid injections (e.g., infection of the skin, allergy to any components of the injection) or for MRI (e.g., metallic implants), or those who are pregnant, lactating or planning pregnancy during the course of the study. Healthy participants will be excluded if they present with a history of hand, arm or neck pain in the past three months, abnormalities in nerve conduction studies suggestive of CTS, or with a systemic medical condition.
Study procedure
Consented participants (see ethics below) will receive the baseline set of questionnaires to complete before the first baseline appointment at the Nuffield Department of Clinical Neurosciences, University of Oxford. This first appointment will include a detailed bedside neurological assessment and measures of nerve function. If participants present with bilateral symptoms of CTS, the most affected hand will be evaluated. At this point, participants not meeting the inclusion criteria will be excluded from the study (e.g., severe electrodiagnostic test findings). Eligible participants will provide a blood sample and a finger skin biopsy.
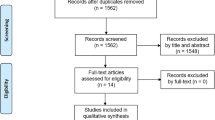
Participants will be invited for a second baseline appointment for an MRI of the wrist and the neck. Following the scan, patients will receive their assigned intervention. After the 6-week intervention period, patients will be invited for a follow-up appointment to repeat the same assessments. Finally, questionnaires will be sent out to patients at 6 months (Fig. 1).
Healthy controls will only attend the baseline appointments during which the same measures will be performed as in patients.

Trial flow chart
Assignment of interventions and blinding
Patients will be randomly assigned to one of three interventions after their first baseline appointment. Assignment will be randomised and stratified by electrodiagnostic test severity (mild/moderate) using an online tool (https://www.randomizer.org) and implemented in REDcap. The allocation ratio will be 1:1:1. The examiner performing the outcome measures will be blinded. The central research team, including the statistician, will also be blinded.
Interventions
Neurodynamic exercises
The ‘active’ intervention is a progressive neurodynamic mobilisation adapted from our previously established protocol [35, 36]. Patients will attend a single session (~ 30 min) with an investigator who will instruct them the home exercise programme consisting of eight nerve and tendon gliding exercises (Fig. 2). The investigator will train patients with the help of a set of videos demonstrating the exercises on either the right or the left hand, as suggested by our patient partners. Patients will be asked to perform 10 repetitions of each exercise six times a day for six weeks (~ 1.5 min per session) in a manner that does not increase symptoms. These exercises are progressed on week 3 and 5th to increase the nerve gliding or tension as per each patient’s tolerance (Fig. 2, B and C, exercises in brackets). Patients will receive a leaflet detailing the neurodynamic exercises during their second baseline appointment (Suppl. Information. Appendix A), an exercise diary as well as a link to the exercise videos in weeks 1, 3 and 5. They will also be instructed to keep performing their usual activities but not start any new treatments during the 6 weeks of the study intervention (Suppl. Information. Appendix A).

Progressive home-based programme of nerve and tendon gliding exercises
(A) Weeks 1–2, (B) weeks 3–4, and (C) weeks 5–6. The brackets surrounding two figures indicate the combination of movements for that exercise, from the start to the end point
Steroid injections
Steroid injections are routine first-line treatment for patients with CTS [37] and will be used as a positive control group as they have established short term benefits [38, 39] and change nerve structure [40]. Patients in this group will receive a single injection of 40 mg depomedrone suspended in polyethylene glycol into the carpal tunnel (extraneurally) using the landmark technique [41]. Briefly, the needle will be inserted into the proximal carpal tunnel at the distal wrist crease immediately ulnar to the palmaris longus tendon [41]. A trained medical doctor will perform this technique as per standard practice at OUH NHS Trust. Participants will receive an information leaflet, and will be instructed to keep performing their usual activities but not start any new treatments during the 6 weeks of the study intervention (Suppl. Information Appendix B).
Advice group
The advice group will serve as a negative control group and will receive no additional intervention during the 6-week intervention period. Patients randomly assigned to this group will meet the investigator, who will provide them with an information leaflet detailing the advice (Suppl. Information Appendix C). Patients will be instructed to keep performing their usual activities but not start any new treatments during the 6 weeks of the study intervention.
Patients allocated to the advice group will be offered the 6-week home based exercise program as post-trial care (end of the 6-week treatment period) if they wish.
Primary mechanistic outcome measure
Magnetic resonance neurography (MRN): Fractional Anisotropy (FA)
All participants will attend a MRN session on a 3 Tesla MAGNETOM Prisma scanner (Siemens, Germany) to visualise the median nerve at the wrist using a dedicated 16-channel wrist coil (Siemens, Germany).
Participants will be positioned in a ‘superman’ position, lying prone with the wrist above their head resting in the centre of the bore. The protocol includes the acquisition of multishell (b = 0, b = 300 and 800 s/mm2) diffusion-weighted imaging scans. In addition, true fast imaging with steady-state free precession (TRUFI) with/without magnetisation transfer (MT) preparation, and T2-mapping scanning will be acquired (see other markers in MRN). Scan parameters are summarised in Table 1.
All diffusion image pre-processing will be performed using the FMRIB Software Library (FSL) Diffusion Toolbox v 6.0 (Oxford, UK). Briefly, TOPUP [42, 43] and EDDY [44] tools will be applied to correct for distortions and eddy currents followed by DTIFIT [45] to compute the diffusion tensor model. FLIRT will be used to co-register the diffusion metrics to the anatomical sequences.
Median nerve region of interests will be determined at three levels: the distal radio-ulnar joint (proximal), pisiform (mid-carpal tunnel) and hook of hamate (distal carpal tunnel). Fractional anisotropy (no units) will be computed as our primary outcome measure.
Secondary mechanistic outcome measures
Other markers in MRN of the median nerve at the wrist
The MRN protocol of the wrist includes the acquisition of true fast imaging with steady-state free precession (TRUFI) with/without MT preparation and a multi-spin-echo scan for T2-mapping scanning (Table 1). Multi-spin-echo and TRUFI will be processed using a custom-made Python script. TRUFI volumes acquired with different phases will be combined by calculating the square root of the sum of the squares of each volume. T2 maps will be obtained from the multi-spin-echo volumes using non-linear least-squares regression. FLIRT will be used to co-register the T2 maps to the high resolution anatomical images.
MR outcome measures of the median nerve will be computed at the three levels of the carpal tunnel described for the primary outcome measure (i.e., proximal, mid, and distal carpal tunnel). In structural images, we will compute the cross-sectional area (mm2) and flattening ratio (arbitrary units). Mean diffusivity (mm2/s), and radial/axial diffusivity (mm2/s) will be obtained from diffusion images. Finally, T2 (ms), and magnetisation transfer ratio (arbitrary units) will be computed from their respective sequences. Metrics derived from multishell data will be explored.
Somatosensory function
We will use the standardised Quantitative Sensory Testing (QST) battery of the German Network for Neuropathic pain [46] to evaluate the somatosensory function over the median nerve territory of the studied hand.
Thermal thresholds will be explored with series of three repetitions to compute the average temperature (°C) for cold and warm detection thresholds (CDT, WST), hot and cold pain threshold (HPT, CPT) and five repetitions for thermal sensory limen (TSL) using a Thermotester (Somedic, Sweden, 25 × 50 mm thermode). Paradoxical heat sensations (PHS) will be recorded during TSL testing. Pain ratings during HPT and CPT will be recorded on an 11-point numerical rating scale (NRS), from ‘0’ representing no pain to ‘10’, worst pain imaginable and averages used for analyses.
Mechanical detection thresholds (MDT) will be assessed using five series of ascending/descending von Frey monofilaments (mN, geometric mean calculated). Mechanical pain threshold (MPT) will be explored with a set of weighted pinpricks (mN, geometric mean calculated). Mechanical pain sensitivity will be examined with a NRS of 0–100 using a shortened protocol of two sets of seven pseudo-random pinprick stimulations [47]. Dynamic mechanical allodynia (DMA) will be explored [26, 48] using a cotton wisp, cotton wool tip, and a standardised brush (Somedic, Sweden) [46] that will be interleaved during the MPS assessment. The geometric mean will be calculated for MPS and DMA. Wind-up ratio will be calculated as the average pain rating on a 100-NRS scale between three trains of 10 pinprick stimuli divided by three single stimuli. Vibration detection threshold (VDT) will be determined as a disappearance threshold through the average of three repetitions using a Rydel Seiffer tuning fork (64 Hz, 8/8 scale). Pressure pain threshold will be determined as the average of three series of ascending stimulus intensities (kPa) using a manual algometer (Wagner Instruments, USA).
All stimuli will be first demonstrated over the lateral, proximal forearm (radial territory) of the non-studied side, with the exception of VDT which be shown over the ulnar styloid. All thermal and mechanical stimuli will then be assessed over the palmar aspect of the index finger (proximal phalanx), except VDT (over the second metacarpophalangeal head) and PPT (over the thenar eminence). Additionally, pain thresholds including HPT, CPT, MPT and PPT will be assessed in the contralateral lower limb (upper anterolateral aspect of the tibialis anterior muscle) to determine potential effects on generalised hypersensitivity.
QST outcome measures will be transformed into Z-scores [46] using our healthy control participants as well as existing control data sets [26, 49], who will be matched for age and sex. Additionally, we will classify each participant with CTS to a specific and unique somatosensory profile [50]: (1) sensory loss; (2) thermal hyperalgesia; or (3) mechanical hyperalgesia.
Neurophysiological function
We will use surface electrodes to measure the median SNAP amplitudes (µV), CMAP amplitudes (mV) and conduction velocities (m/s), as described above [32].
Neurodynamic tests
We will explore the mechanosensitivity of the median, ulnar and radial nerve using Upper Limb Neurodynamic Tests (ULNT) in patients bilaterally [12]. The median nerve bias test (ULNT 1) will be performed with the patient lying supine and the movement sequence will involve maximum end range shoulder abduction, wrist and finger extension, forearm supination, shoulder external rotation and elbow extension [12]. The ulnar nerve bias (ULNT 3) sequence starts with the patient lying supine and their arm resting by the side followed by wrist extension, forearm pronation, elbow flexion, shoulder external rotation, shoulder girdle depression and shoulder abduction [12]. The radial nerve bias (ULNT 2B) starts with the patient in supine and diagonally on the plinth. The sequence involves shoulder girdle depression, elbow extension, forearm pronation, wrist and finger flexion, followed by shoulder abduction [12]. The end point of these tests is the first onset of symptoms (P1). The test will be considered positive if (1) patient’s symptoms are at least partially reproduced, and (2) structural differentiation (away from the site of pain) changes the symptoms [51].
We will also quantify the elbow extension angle at P1 with an inclinometer in a slightly modified ULNT1 manoeuvre. The testing will involve shoulder at 90 degrees abduction, neutral shoulder rotation, wrist and fingers extension and finally, elbow extension. This assessment will be performed in patients and healthy participants (reference values).
Pinch grip strength
Tip to tip pinch of the thumb and index finger, key pinch between the radial side of index finger and thumb, and tripod pinch using the thumb, index and middle finger (kg, averaged 3 repetitions) will be assessed using a mechanical pinch gauge dynamometer bilaterally (B&L Engineering, CA, USA) as per standard recommendations [52, 53].
Self-reported outcome measures
We will use a battery of validated questionnaires to evaluate patients’ symptoms, functional deficits, quality of life, sleep, and psychological co-morbidities at all time points. Patients assigned to the neurodynamic exercise group will be asked to complete an exercise diary daily (electronically or on paper) to monitor adherence for the duration of the intervention (6-weeks). Healthy participants will only complete questionnaires determining function, quality of life, sleep and psychological comorbidities (Table 2).
Exploratory outcomes
Blood inflammatory markers (e.g., cytokine panels)
We will collect 26 ml of venous blood from antecubital venepuncture. Serum will be extracted from whole blood collected into BD Vacutainer SST tubes (gold cap) and centrifuged at 1.3 g for 10 min at 4 °C 30 min after venepuncture. Serum fraction will be immediately frozen at -80 degrees and stored for batch processing in accordance with the Human Tissue Act. In future analyses, we can explore the concentrations of serum inflammatory protein levels and other markers of interest, including but not limited to TGF-β, CCL5, and IL-4, as per our previous work [28].
For future analyses and biobanking, we will also sample blood into RNA stabilising tubes (Tempus™ blood RNA tube, Fisher Scientific), serum clot activator tubes (red cap BD, Wokingham UK) and EDTA containing tubes (lavender cap, BD, Wokingham UK).
Cutaneous markers (e.g., inflammatory markers, innervation markers)
Future exploratory analysis will involve looking at the presence of inflammatory and innervation markers via 3 mm skin punch biopsies performed on the ventrolateral side of the proximal phalanx of the index finger [48] (baseline and 6 weeks in patients, baseline only in healthy controls). In patients, the 6-weeks biopsy will be performed slightly more proximal, avoiding the primary biopsy site as we have previously done [26]. Samples will be processed for immunostaining (fixation in fresh periodate-lysine-paraformaldehyde for 30 min before being washed in 0.1 M phosphate buffer and cryoprotected in 15% sucrose in 0.1 M phosphate buffer and freezing in optimal cutting temperature gel at -80 degrees) and molecular experiments (snap freezing in liquid nitrogen before storing at -80 degrees).
MRN markers at the DRG
As preclinical literature suggests changes at the level of the DRG after peripheral nerve injury [54, 55], all participants will be scanned to visualise their cervical DRG with a 64-channel head/neck coil (Siemens, Germany). Participants will be lying supine. The protocol includes T2 weighted (T2W) and Diffusion Weighted (DW) scans. T2W and DW images will be acquired using Sampling Perfection with Application optimised Contrast using different flip angle Evolution (SPACE) and Readout Segmentation Of Long Variable Echo trains (RESOLVE) sequences, respectively. DW images will be registered to T2W images (Supplementary Table 1).
MR outcome measures will be obtained from structural images, such as volume (mm3) for the DRG. FA, mean diffusivity (mm2/s), and radial/axial diffusivity (mm2/s) will be calculated from diffusion images. Metrics derived from multishell data will be explored.
Additional cohort characterisation
Demographic variables
We will collect demographic data on age, sex, height, weight, ethnicity, profession, working status, and years of education. Medical information will include the most affected side, presence of unilateral/bilateral symptoms, duration of symptoms, previous history of carpal tunnel syndrome (personal and in the family), previous treatment received for carpal tunnel syndrome (CTS), current and previous medications, smoking and alcohol intake.
Clinical assessment
Patients will complete two body charts, one reflecting the presence of symptoms in their body, and a detailed diagram of hand symptoms. Patients will undergo a detailed neurological examination which will include upper limb myotome testing (C4-T1) recorded on the five-point British Medical Research Council scale (M0 = no contraction, M1 = flicker or trace of contraction; M2 = active movement, with gravity eliminated; M3 = active movement against gravity; M4 = active movement against gravity and resistance; M5 = normal power) [56]; biceps, triceps and brachioradialis reflexes recorded as normal, absent, reinforced or hyperreflexia (adapted from National Institute of Neurological Disorders and Stroke Scale (NINDS) [57], and exploring potential loss of sensation to light touch and pinprick recorded as absent, reduced, normal or increased on two separate body charts.
Safety and adherence to neurodynamic exercises
Patients assigned to the neurodynamic exercise group will be asked to complete an electronic (or paper-based) exercise diary daily to monitor treatment adherence for the duration of the intervention (6-weeks). Patients will be asked to indicate how many times they perform the exercises each day.
We will also use periodic phone calls during the 6-week study period (3rd day after randomisation, weekly thereafter) to check on progress in each of the intervention groups, decrease study attrition, give advice on exercise performance when needed, check if there are potential adverse events associated with the exercise intervention or the steroid injection, and to confirm that they have not started any new treatments during the intervention period in the steroid and advice groups. This was suggested by our patients’ partners to increase adherence.
Sample size calculation
Sample size is based on our previous MRI study demonstrating intraneural signal reduction after neurodynamic exercises [25]. Conservatively assuming a 30% smaller effect size (within subjects repeated measures ANOVA with 3 groups & 2 time points), n = 63 patients are required (n = 21 per group, d = 0.22, power = 80%, alpha = 0.05). To account for a 20% drop out rate, we will include 78 participants (26 per group). We will include 30 healthy participants to establish normative data.
Statistical analysis
Data will be analysed using R Studio (v 7.2, RStudio, Boston, USA) [58]. The distribution of the data will be checked for normality, and parametric, or non-parametric methods will be used as appropriate. Participants’ characteristics in each group will be described at baseline.
Two-way repeated measures ANCOVAs (factors time and intervention, adjusted for baseline measurements as a continuous covariate) followed by post-hoc testing will be performed to identify differences in primary/secondary outcome measures among groups and over time. If there is deviation from normality, we will use non-parametric alternatives (i.e. ranked ANCOVA).
If the missing values mechanism is likely to be missing at random (MAR) or missing completely at random (MCAR), we will perform multiple imputation by chained equations. The appropriate model will be fitted in all the completed datasets, then coefficient estimates and standard errors will be pooled across imputations using Rubin’s rules.
The level of statistical significance will be set at p = 0.05. Adjustments for multiple comparisons will be used as appropriate.
Data management
All study data will be entered on paper or directly onto EXCEL or REDCap database. The name and any other identifying details will not be included in any study data electronic file, with the exception of REDCap to send out reminders to complete follow up questionnaires.
Data entries will be randomly checked for accuracy by an independent researcher (up to 30%). All data will be kept on firewall and password-protected computers and any paper information will be stored safely in lockable cabinets in a swipe-card secured building and would only be accessed by the research team. MRI data will be stored in a secure University server.
As this a mechanistic study and not a clinical trial, we do not have an external monitoring committee but we will internally monitor and regularly audit data collection and delivery of interventions. No interim analysis will be done of the longitudinal data. All research data and records will be stored in accordance with data protection and University policies.
Ethics and dissemination
Protocol amendments will be approved by the ethics committee and then disseminated to site investigators via meetings and updating of study resources and guidelines. Changes in the protocol will be reported to the trial registry and mentioned in future publications.
Patient and public involvement (PPI)
Patient partners highlighted the relevance of this study. They were involved in the design of the videos in the neurodynamic exercise group (i.e., including demonstrative videos with either right or left hand) and how these videos should be displayed (i.e., individual videos explaining each exercise and a summary video with the full sequence). Additionally, they provided feedback on the potential burden of the duration of the baseline assessment and suggested two separate appointments (i.e., MRI on a separate day). They agreed on the feasibility to perform the sessions suggested in the home-based neurodynamic intervention. They suggested ways to optimise the adherence to the neurodynamic intervention by facilitating access to the home-based program using different devices (i.e., computer or mobile phones), and the use of electronic and paper-based exercise diaries along with daily email reminders to input the number of exercise sessions per day.
Patient partners will continue to be involved throughout the study (e.g., suggestions with recruitment, sense-making, interpretation of the data, evaluation of the output) and to help with the dissemination of the findings. The dissemination of our findings will involve publication in scientific journals, social media outlets, webinars, electronic newsletters, presentations at conferences, as guided by our patient partners. We will adapt the content of our findings to health care professionals, researchers and people with CTS according to our PPIs suggestions.
Discussion
Carpal tunnel syndrome is the most common entrapment neuropathy [27] but recruitment through secondary care could be challenging, especially when recruiting patients with mild carpal tunnel syndrome. Primary care facilities will be incorporated as needed to facilitate recruitment. Since our intervention and follow-up is significanly shorter than the current wait times (18 weeks at the time of the study in the UK) and the treatment provided is within the current clinical guidelines [1, 2], we expect this to be an incentive for potential eligible participants to be enrolled.
Neurodynamic exercises have shown effectiveness in the conservative management of people with entrapment neuropathies [14, 25] although their mechanisms of action are not fully understood. This study will explore the mechanisms of effect of neurodynamic exercises in detail, looking at their potential effect on microstructural nerve integrity, nerve function and inflammatory markers using carpal tunnel syndrome as a model system. Our findings are likely to help us understand which patients are likely to benefit from this treatment, an important first step in the progression towards precision physiotherapy.
Data availability
No datasets were generated or analysed during the current study.
References
National Institute of. Health and Excellent Care. Carpal tunnel syndrome. 2022.
Royal College of Surgeons of England. Commissioning guide: treatment of carpal tunnel syndrome. 2017.
American Academy of Orthopaedic Surgeons. Carpal Tunnel Syndrome - Clinical Practice Guideline (CPG). 2016 [cited 2023 Oct 31]; https://www.aaos.org/quality/quality-programs/upper-extremity-programs/carpal-tunnel-syndrome/
Wright AR, Atkinson RE. Carpal Tunnel Syndrome: An Update for the Primary Care Physician. Hawaii J Health Soc Welf [Internet]. 2019 Nov 1 [cited 2023 Apr 21];78(11 Suppl 2):6. /pmc/articles/PMC6874691/
Parish R, Morgan C, Burnett CA, Baker BC, Manning C, Sisson SK et al. Practice patterns in the conservative treatment of carpal tunnel syndrome: Survey results from members of the American Society of Hand Therapy. J Hand Ther [Internet]. 2020 Jul 1 [cited 2023 Apr 21];33(3):346–53. https://pubmed.ncbi.nlm.nih.gov/30956070/
Erickson M, Lawrence M, Jansen CWS, Coker D, Amadio P, Cleary C. Hand pain and sensory deficits: Carpal tunnel syndrome. Journal of Orthopaedic and Sports Physical Therapy [Internet]. 2019 May 1 [cited 2023 Apr 21];49(5):CPG1–85. https://www.jospt.org/doi/https://doi.org/10.2519/jospt.2019.0301
Lee J, Gupta S, Price C, Baranowski AP. Low back and radicular pain: A pathway for care developed by the British Pain Society. Br J Anaesth [Internet]. 2013 Jul 1 [cited 2023 Apr 21];111(1):112–20. http://www.bjanaesthesia.org/article/S0007091217329744/fulltext
Basson A, Olivier B, Ellis R, Coppieters M, Stewart A, Mudzi W. The effectiveness of neural mobilization for neuromusculoskeletal conditions: A systematic review and meta-Analysis. Journal of Orthopaedic and Sports Physical Therapy [Internet]. 2017 Sep 1 [cited 2022 Dec 29];47(9):593–615. https://www.jospt.org/doi/https://doi.org/10.2519/jospt.2017.7117
Murape T, Ainslie TR, Basson CA, Schmid AB. Does the efficacy of neurodynamic treatments depend on the presence and type of criteria used to define neural mechanosensitivity in spinally-referred leg pain? A systematic review and meta-analysis. S Afr J Physiother. 2022;78(1).
Peacock M, Douglas S, Nair P. Neural mobilization in low back and radicular pain: a systematic review. J Man Manip Ther [Internet]. 2023 [cited 2023 Apr 21];31(1):4–12. https://pubmed.ncbi.nlm.nih.gov/35583521/
Coppieters MW, Butler DS. Do ‘sliders’ slide and ‘tensioners’ tension? An analysis of neurodynamic techniques and considerations regarding their application. Man Ther. 2008;13(3):213–21.
Butler DS. The sensitive nervous system. Adelaide, Australia: Noigroup; 2000.
Coppieters MW, Hough A, Dilley A. Different nerve-gliding exercises induce different magnitudes of median nerve longitudinal excursion: an in vivo study using dynamic ultrasound imaging. J Orthop Sports Phys Ther. 2009;39(3):164–71.
Lewis KJ, Coppieters MW, Ross L, Hughes I, Vicenzino B, Schmid AB. Group education, night splinting and home exercises reduce conversion to surgery for carpal tunnel syndrome: a multicentre randomised trial. J Physiother [Internet]. 2020 Apr 1 [cited 2022 Dec 29];66(2):97–104. https://pubmed.ncbi.nlm.nih.gov/32291222/
Zhu GCC, Tsai KLL, Chen YWW, Hung CHH. Neural Mobilization Attenuates Mechanical Allodynia and Decreases Proinflammatory Cytokine Concentrations in Rats With Painful Diabetic Neuropathy. Phys Ther [Internet]. 2018 Apr 1 [cited 2022 May 29];98(4):214–22. https://pubmed.ncbi.nlm.nih.gov/29309710/
Santos FM, Silva JT, Giardini AC, Rocha PA, Achermann APP, Alves AS et al. Neural mobilization reverses behavioral and cellular changes that characterize neuropathic pain in rats. Mol Pain [Internet]. 2012 Jan [cited 2022 Nov 9];8:57. https://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3495676&tool=pmcentrez&rendertype=abstract
Martins DF, Mazzardo-Martins L, Gadotti VM, Nascimento FP, Lima DAN, Speckhann B et al. Ankle joint mobilization reduces axonotmesis-induced neuropathic pain and glial activation in the spinal cord and enhances nerve regeneration in rats. Pain [Internet]. 2011 Nov [cited 2022 Dec 29];152(11):2653–61. https://pubmed.ncbi.nlm.nih.gov/21906878/
da Silva JT, dos Santos FM, Giardini AC, de Oliveira Martins D, de Oliveira ME, Ciena AP et al. Neural mobilization promotes nerve regeneration by nerve growth factor and myelin protein zero increased after sciatic nerve injury. Growth Factors [Internet]. 2015 Feb 1 [cited 2022 Dec 29];33(1):8–13. https://pubmed.ncbi.nlm.nih.gov/25489629/
Carta G, Fornasari BE, Fregnan F, Ronchi G, De Zanet S, Muratori L et al. Neurodynamic Treatment Promotes Mechanical Pain Modulation in Sensory Neurons and Nerve Regeneration in Rats. Biomedicines [Internet]. 2022 Jun 1 [cited 2023 May 19];10(6):1296. /pmc/articles/PMC9220043/
Zhu GC, Chen YW, Tsai KL, Wang JJ, Hung CH, Schmid AB. Effects of Neural Mobilization on Sensory Dysfunction and Peripheral Nerve Degeneration in Rats With Painful Diabetic Neuropathy. Phys Ther [Internet]. 2022 Oct 1 [cited 2023 Jun 6];102(10). https://pubmed.ncbi.nlm.nih.gov/35913760/
Lima Martins Ê, Henrique H, Santana S, Peixoto Medrado A, Blanco Martinez AM, Fontes Baptista A. Neurodynamic mobilization reduces intraneural fibrosis after sciatic crush lesion in rats. Brazilian J Med Hum Health. 2017;5(2).
Neto T, Freitas SR, Andrade RJ, Vaz JR, Mendes B, Firmino T et al. Shear Wave Elastographic Investigation of the Immediate Effects of Slump Neurodynamics in People With Sciatica. J Ultrasound Med [Internet]. 2020 Apr 1 [cited 2023 Jun 13];39(4):675–81. https://pubmed.ncbi.nlm.nih.gov/31633231/
Wolny T, Saulicz E, Linek P, Shacklock M, Myśliwiec A. Efficacy of Manual Therapy including neurodynamic techniques for the treatment of carpal tunnel syndrome: a Randomized Controlled Trial. J Manipulative Physiol Ther. 2017;40(4):263–72.
Oskay D, Meriç A, Kirdi N, Firat T, Ayhan Ç, Leblebicioǧlu G. Neurodynamic mobilization in the conservative treatment of cubital tunnel syndrome: long-term follow-up of 7 cases. J Manipulative Physiol Ther [Internet]. 2010 [cited 2023 Jun 26];33(2):156–63. https://pubmed.ncbi.nlm.nih.gov/20170781/
Schmid AB, Elliott JM, Strudwick MW, Little M, Coppieters MW. Effect of splinting and exercise on intraneural edema of the median nerve in carpal tunnel syndrome–an MRI study to reveal therapeutic mechanisms. J Orthop Res [Internet]. 2012 Aug [cited 2022 Nov 14];30(8):1343–50. http://www.ncbi.nlm.nih.gov/pubmed/22231571
Baskozos G, Sandy-Hindmarch O, Clark AJ, Windsor K, Karlsson P, Weir GA et al. Molecular and cellular correlates of human nerve regeneration: ADCYAP1/PACAP enhance nerve outgrowth. Brain [Internet]. 2020 Jul 1 [cited 2022 Dec 29];143(7):2009–26. https://pubmed.ncbi.nlm.nih.gov/32651949/
Burton CL, Chen Y, Chesterton LS, Van Der Windt DA. Trends in the prevalence, incidence and surgical management of carpal tunnel syndrome between 1993 and 2013: an observational analysis of UK primary care records. BMJ Open [Internet]. 2018 Jun 1 [cited 2022 Dec 29];8(6):e020166. https://pubmed.ncbi.nlm.nih.gov/29921681/
Sandy-Hindmarch O, Bennett DL, Wiberg A, Furniss D, Baskozos G, Schmid AB. Systemic inflammatory markers in neuropathic pain, nerve injury, and recovery. Pain [Internet]. 2022 Mar 1 [cited 2022 Dec 29];163(3):526–37. https://pubmed.ncbi.nlm.nih.gov/34224495/
Huisstede BM, Hoogvliet P, Randsdorp MS, Glerum S, van Middelkoop M, Koes BW. Carpal tunnel syndrome. Part I: effectiveness of nonsurgical treatments–a systematic review. Arch Phys Med Rehabil [Internet]. 2010 Jul [cited 2022 Dec 29];91(7):981–1004. https://pubmed.ncbi.nlm.nih.gov/20599038/
Barbour V, Bhui K, Chescheir N, Clavien PA, Diener MK, Glasziou P, et al. CONSORT Statement for randomized trials of nonpharmacologic treatments: a 2017 update and a CONSORT extension for nonpharmacologic trial abstracts. Ann Intern Med. 2017;167(1):40–7.
Neurology R. of the QSS of the AA of. Practice parameter for carpal tunnel syndrome (Summary statement). Neurology [Internet]. 1993 Nov 1 [cited 2023 Aug 7];43(11):2406–2406. https://n.neurology.org/content/43/11/2406
Bland JDP. A neurophysiological grading scale for carpal tunnel syndrome. Muscle Nerve [Internet]. 2000 Aug [cited 2022 Dec 29];23(8):1280–3. https://pubmed.ncbi.nlm.nih.gov/10918269/
Uncini A, Lange DJ, Solomon M, Soliven B, Meer J, Lovelace RE. Ring finger testing in carpal tunnel syndrome: a comparative study of diagnostic utility. Muscle Nerve [Internet]. 1989 [cited 2023 Nov 3];12(9):735–41. https://pubmed.ncbi.nlm.nih.gov/2641997/
Preston DC, Logigian EL. Lumbrical and interossei recording in carpal tunnel syndrome. Muscle Nerve. 1992;15(11).
Lewis KJ, Coppieters MW, Vicenzino B, Hughes I, Ross L, Schmid AB. Occupational Therapists, Physiotherapists and Orthopaedic Surgeons Agree on the Decision for Carpal Tunnel Surgery. Int J Health Policy Manag [Internet]. 2020 Jul 1 [cited 2022 Dec 29];11(7):1001–8. https://pubmed.ncbi.nlm.nih.gov/33590739/
Lewis KJ, Ross L, Coppieters MW, Vicenzino B, Schmid AB. Education, night splinting and exercise versus usual care on recovery and conversion to surgery for people awaiting carpal tunnel surgery: a protocol for a randomised controlled trial. BMJ Open. 2016;6(9):e012053.
RCS BOA. Commissioning guide: treatment of carpal tunnel syndrome. Royal College of Surgeons of England (RCS); 2017.
Huisstede BM, Randsdorp MS, van den Brink J, Franke TPC, Koes BW, Hoogvliet P. Effectiveness of oral Pain medication and corticosteroid injections for carpal tunnel syndrome: a systematic review. Volume 99. Archives of Physical Medicine and Rehabilitation; 2018.
Ashworth NL, Bland JDP, Chapman KM, Tardif G, Albarqouni L, Nagendran A. Local corticosteroid injection versus placebo for carpal tunnel syndrome. Cochrane Database of Systematic Reviews [Internet]. 2023 Feb 1 [cited 2023 Jul 31];2(2):CD015148. https://www.cochranelibrary.com/cdsr/doi/https://doi.org/10.1002/14651858.CD015148/full
Hsu YC, Yang FC, Hsu HH, Huang GS. Diffusion tensor imaging findings of the median nerve before and after carpal tunnel corticosteroid injection in patients with carpal tunnel syndrome: a preliminary study. Acta Radiol [Internet]. 2019 Mar 1 [cited 2023 Sep 13];60(3):347–55. https://pubmed.ncbi.nlm.nih.gov/29979105/
Menge TJ, Rinker EB, Fan KH, Block JJ, Lee DH. Carpal Tunnel Injections: A Novel Approach Based on Wrist Width. J Hand Microsurg [Internet]. 2016 Apr 27 [cited 2023 Jul 31];08(01):021–6. http://www.thieme-connect.de/products/ejournals/html/https://doi.org/10.1055/s-0036-1581192
Andersson JLR, Skare S, Ashburner J. How to correct susceptibility distortions in spin-echo echo-planar images: Application to diffusion tensor imaging. Neuroimage [Internet]. 2003 Oct 1 [cited 2023 Nov 2];20(2):870–88. https://pubmed.ncbi.nlm.nih.gov/14568458/
Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TEJ, Johansen-Berg H et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage [Internet]. 2004 [cited 2023 Nov 2];23 Suppl 1(SUPPL. 1). https://pubmed.ncbi.nlm.nih.gov/15501092/
Andersson JLR, Sotiropoulos SN. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage [Internet]. 2016 Jan 15 [cited 2023 Nov 2];125:1063–78. https://pubmed.ncbi.nlm.nih.gov/26481672/
Behrens TEJ, Woolrich MW, Jenkinson M, Johansen-Berg H, Nunes RG, Clare S et al. Characterization and propagation of uncertainty in diffusion-weighted MR imaging. Magn Reson Med [Internet]. 2003 [cited 2023 Nov 2];50(5):1077–88. https://pubmed.ncbi.nlm.nih.gov/14587019/
Rolke R, Magerl W, Campbell KA, Schalber C, Caspari S, Birklein F et al. Quantitative sensory testing: A comprehensive protocol for clinical trials. European Journal of Pain [Internet]. 2006 [cited 2023 Aug 4];10(1):77. https://pubmed.ncbi.nlm.nih.gov/16291301/
Pascal MMV, Themistocleous AC, Baron R, Binder A, Bouhassira D, Crombez G et al. DOLORisk: study protocol for a multi-centre observational study to understand the risk factors and determinants of neuropathic pain. Wellcome Open Res [Internet]. 2019 [cited 2023 May 9];3. https://pubmed.ncbi.nlm.nih.gov/30756091/
Schmid AB, Bland JDP, Bhat MA, Bennett DLH. The relationship of nerve fibre pathology to sensory function in entrapment neuropathy. Brain. 2014;137(12).
Ferris JK, Timothy Inglis J, Madden KM, Boyd LA. Brain and body: A review of central nervous system contributions to movement impairments in diabetes [Internet]. Vol. 69, Diabetes. American Diabetes Association Inc.; 2020 [cited 2023 Feb 18]. pp. 3–11. https://pubmed.ncbi.nlm.nih.gov/31862690/
Baron R, Maier C, Attal N, Binder A, Bouhassira D, Cruccu G et al. Peripheral neuropathic pain: a mechanism-related organizing principle based on sensory profiles. Pain [Internet]. 2017 [cited 2023 Jun 22];158(2):261–72. http://www.ncbi.nlm.nih.gov/pubmed/27893485
Nee RJ, Jull GA, Vicenzino B, Coppieters MW. The validity of upper-limb neurodynamic tests for detecting peripheral neuropathic pain. J Orthop Sports Phys Ther. 2012;42(5):413–24.
Geere J, Chester R, Kale S, Jerosch-Herold C. Power grip, pinch grip, manual muscle testing or thenar atrophy – which should be assessed as a motor outcome after carpal tunnel decompression? A systematic review. BMC Musculoskelet Disord [Internet]. 2007 [cited 2023 May 31];8:114. Available from: /pmc/articles/PMC2213649/.
Mathiowetz V, Kashman N, Volland G, Weber K, Dowe M, Rogers S. Grip and pinch strength: normative data for adults. Arch Phys Med Rehabil. 1985;66(2).
Schmid AB, Coppieters MW, Ruitenberg MJ, McLachlan EM. Local and remote immune-mediated inflammation after mild peripheral nerve compression in rats. J Neuropathol Exp Neurol [Internet]. 2013 Jul [cited 2023 Mar 11];72(7):662–80. http://www.ncbi.nlm.nih.gov/pubmed/23771220
Hu P, Bembrick AL, Keay KA, McLachlan EM. Immune cell involvement in dorsal root ganglia and spinal cord after chronic constriction or transection of the rat sciatic nerve. Brain Behav Immun [Internet]. 2007 Jul [cited 2023 Nov 7];21(5):599–616. https://pubmed.ncbi.nlm.nih.gov/17187959/
Riddoch G. Medical Research Council. Aids to the examination of the Peripheral Nervous System. Memorandum no 45 her. London: Majesty’s Stationery Office; 1975.
Hallett M. NINDS myotatic reflex scale. Neurology [Internet]. 1993 [cited 2023 Jun 7];43(12):2723. https://pubmed.ncbi.nlm.nih.gov/7802740/
R Core Team. R: A Language and Environment for Statistical Computing [Internet]. Vienna, Austria: R Foundation for Statistical Computing. 2021. https://www.r-project.org/
Levine DW, Simmons BP, Koris MJ, Daltroy LH, Hohl GG, Fossel AH et al. A self-administered questionnaire for the assessment of severity of symptoms and functional status in carpal tunnel syndrome. J Bone Joint Surg. 1993;75(11).
Mayer TG, Neblett R, Cohen H, Howard KJ, Choi YH, Williams MJ, et al. The Development and Psychometric Validation of the Central Sensitization Inventory. Pain Pract [Internet]. 2012;12(4):276–85. Available from: /pmc/articles/PMC3248986/?report = abstract.
Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med. 1996;29(6).
Kowalchuk Horn K, Jennings S, Richardson G, van Vliet D, Hefford C, Abbott JH. The patient-specific functional scale: Psychometrics, clinimetrics, and application as a clinical outcome measure. J Orthop Sports Phys Ther. 2012;42(1).
Stratford P, Gill C, Westaway M, Binkley J. Assessing disability and change on individual patients: a report of a patient specific measure. Physiotherapy Can. 1995;47(4):258–63.
Bouhassira D, Attal N, Alchaar H, Boureau F, Brochet B, Bruxelle J et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain [Internet]. 2005 Mar [cited 2023 Aug 5];114(1):29–36. http://journals.lww.com/00006396-200503000-00005
Freynhagen R, Baron R, Gockel U, Tölle TR, painDETECT. A new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin [Internet]. 2006 Oct [cited 2023 Aug 5];22(10):1911–20. https://pubmed.ncbi.nlm.nih.gov/17022849/
Pincus T, Williams ACDC, Vogel S, Field A. The development and testing of the depression, anxiety, and positive outlook scale (DAPOS). Pain. 2004;109(1–2).
Osman A, Barrios FX, Kopper BA, Hauptmann W, Jones J, O’Neill E. Factor structure, reliability, and validity of the Pain Catastrophizing Scale. J Behav Med. 1997;20(6):589–605.
McCracken LM, Dhingra L. A short version of the Pain Anxiety Symptoms Scale (PASS-20): preliminary development and validity. Pain Res Manag [Internet]. 2002 [cited 2023 Jan 5];7(1):45–50. https://pubmed.ncbi.nlm.nih.gov/16231066/
Bastien CH, Vallières A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med [Internet]. 2001 [cited 2023 Jan 5];2(4):297–307. https://pubmed.ncbi.nlm.nih.gov/11438246/
EuroQol Group. EuroQol–a new facility for the measurement of health-related quality of life. Health Policy [Internet]. 1990 Dec [cited 2023 Sep 14];16(3):199–208. http://www.ncbi.nlm.nih.gov/pubmed/10109801
Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989;10(4).
Acknowledgements
We would like to thank our participants and patient advisers for contributing to this study as well as our peer reviewers.
Funding
This research was funded in whole, or in part, by the Wellcome Trust [222101/Z/20/Z]. For the purpose of Open Access, the author has applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission.
AS and ESS received support from the Wellcome Trust (222101/Z/20/Z). MT received support from Wellcome Trust (203139/Z/16/Z and 203139/A/16/Z) and the Advanced Pain Discovery Platform (2107HM001/EL2, funded by UKRI and Versus Arthritis as part of the UKRI Strategic Priorities Fund (SPF), a co-funded initiative by UKRI (MRC, BBSRC, ESRC), Versus Arthritis, the Medical Research Foundation and Eli Lilly and Company Ltd (Grant MR/W027003/1)). ACT receives funding from the MRC and vs. Arthritis funding to the PAINSTORM consortium as part of the Advanced Pain Discovery Platform (MR/W002388/1). ACT is a member of the DOLORisk consortium funded by the European Commission Horizon 2020 (ID633491), which received funding from European Union’s Seventh Framework Program (FP7/2007–2013). ACT is member of the International Diabetic Neuropathy Consortium (IDNC) research program, which is supported by a Novo Nordisk Foundation Challenge Program grant (Grant number NNF14OC0011633). ACT is supported by Academy of Medical Sciences Starter Grant (SGL022\1086). MS is supported by the Medical Research Council Clinician Scientist Training Fellowship, British Society for Surgery of the Hand Research Fellowship, and Royal College of Surgeons of England Research Fellowship. GB has received support from Diabetes UK (19/0005984), MRC and Versus Arthritis (MR/W002388/1), and Wellcome Trust (223149/Z/21/Z).
Author information
Authors and Affiliations
Contributions
AS and ESS conceptualised the study. AS acquired funding. GB, ESS and AS planned the statistical aspects of the protocol and sample size calculations. MT developed the MRI sequences and analyses. ESS wrote the manuscript with input from AS. All authors (ESS, MT, GB, MS, ACT, AS) reviewed drafts of the manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Ethical approval has been obtained from South Central - Berkshire Research Ethics Committee (22/SC/0377). All participants will provide informed written or electronic consent before participating in the study.
This study is part of a larger Wellcome Fellowship awarded to AS (222101/Z/20/Z) and has undergone independent peer review.
Consent for publication
Not applicable.
Competing interests
AS has received a rising star award grant by Ono pharmaceuticals (unrelated to this work), and lecturing fees for postgraduate lectures. GB receives fees for RNA-seq consulting by Ivy farm and for Sc RNA-seq consulting by coding.bio. All other authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
E., SS., M., T., AC., T. et al. Mechanisms of neurodynamic treatments (MONET): a protocol for a mechanistic, randomised, single-blind controlled trial in patients with carpal tunnel syndrome. BMC Musculoskelet Disord 25, 590 (2024). https://doi.org/10.1186/s12891-024-07713-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07713-6