
Abstract
Purpose
Review the literature and describe the complications associated with each of the anterior tibial tendon transfer (ATTT) techniques described.
Methods
A systematic review of the literature was performed with the keywords ‘’clubfoot’’, ‘’Ponseti’’ and ‘’anterior tibial’’. Studies in patients with clubfoot recurrence, who underwent ATTT, whose method of tendon fixation was different from the classical method, were included.
Results
Six studies were included in this systematic review, which described multiple techniques for tibialis anterior fixation: bone anchors, interference screws, endobotton, K-wires, transosseous suture, and suture to the plantar fascia. In the papers that described postoperative complications, no major complications were reported, however the samples are generally small.
Conclusion
Several options have now emerged for tendon fixation in tendon transfers around the foot and ankle, including ATTT for treatment of relapsed clubfoot. To our knowledge this is the first paper that questioned the potential complications associated with the use of these new techniques. Due to the scarcity of published works in favor of other fixation methods, we believe that the traditional method is the optimal one for the transfer of the tendon of the tibialis anterior muscle.
Similar content being viewed by others


Introduction
Clubfoot is one of the most frequent congenital musculoskeletal deformities, with an incidence of 1 to 7 per 1000 live births [1, 2]. The Ponseti technique has become the most widely accepted method of management of congenital clubfoot and has largely outdated traditional surgical management. Successful serial casting and meticulous bracing produce a well-corrected foot, requiring no invasive surgical intervention [2].
After complete correction with Ponseti method, 11 to 48% of patients tend to relapse and is usually a consequence of poor compliance with bracing [3]. Clubfeet have been explained by theories considering alterations in development, teratologic causes, intrauterus malpositioning, enviroment agents; none of these is strongly supported by literature. Despite this, relapse is a process caused by the same biologic mechanism that causes the deformity intrauterus [4]. Studies demonstrate differences in the posteromedial tissues in the leg and foot with connected tissue formed by wavy dense collagen and different cells, with some features similar to muscle tissue. The theory implicates possible “contractions” that drive the foot into the clubfoot position. This is more important when baby is born, and progressively milder as the child growths. The foot abduction brace is the most efficient tool to prevent relapses up to four years of age. Relapses are rare after 4 years and as the child grows, the foot can have difficulties to adapt to the stretching of soft tissues necessary to gain length [4]. This is the second obstacle to maintain correction, depending on how hypoplastic calf is and it is worst with growth spurts.
Relapses are detected with loss of dorsiflexion, and then a discrete equinus and varus deformity of the heel appears, frequently without an increase in the adductus and cavus of the forefoot [3, 4].
Anterior tibial tendon transfer (ATTT) is a widely advocated treatment for the treatment of clubfoot relapses, especially when performed in association with Ponseti’s method [5]. In the study by Zionts and co-workers the probability of undergoing an ATTT after the Ponseti method was 29% at age six [6]. In congenital clubfoot there is an imbalance between the inverters and everters of the foot, which contributes to the recurrence of the deformity [5]. Thus, the goal of ATTT is to restore this balance through the more lateral insertion of this tendon.
Different techniques of ATTT are described in the literature [7]. Classic ATTT technique described by Ponseti consists of detachment of the whole anterior tibial tendon, without opening extensor retinaculum, and reinserting it through a tunnel to the third cuneiform. Tendon fixation is performed by pull out technique with button at the plantar surface of the foot [8]. Sometimes, there is a pressure on the plantar surface of the foot, causing erhitema and some irritation. That happens when foot is not held in maximum dorsiflexion and abduction positioning after the transfer, and protected by positioning in the cast.
Multiple methods of anterior tibial tendon fixation after transfer have been described in the literature recently, including the use of anchors or interference screws [9,10,11,12,13]. However, little has been discussed about the potential complications associated with each of the techniques, such as loss of fixation or tension, infection, and skin bruises.
Thus, the purpose of this study is to review the literature and describe the complications associated with each of the techniques described.
Methods
A systematic review of the literature was conducted. The keywords “clubfoot”, “Ponseti” and “anterior tibial” were used to search the PubMed, ScienceDirect, Scielo and Lilacs databases.
Inclusion criteria were patients with relapsing clubfoot who underwent ATTT, whose tendon fixation was different from the classic pull-out techniques described by Ponseti, in patients that were treated initially by Ponseti Method.
Papers where the method of fixation of the tibialis anterior tendon was not described and in which the procedure was performed for pathologies other than relapsed clubfoot were excluded.
Each potentially eligible article was reviewed, as were its references, and additional titles meeting the inclusion criteria articles were included.
Table 1 summarizes the quality of the selected studies using the methodological index for non-randomized studies (MINORS)*.
Results
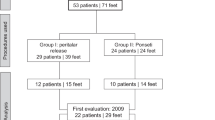
The literature review with the keyword’s “clubfoot”, “Ponseti” and “anterior tibial” yielded 229 results in four databases: 37 results in PubMed, 188 in ScienceDirect, 3 in Lilacs and 1 in Scielo. After exclusion of duplicate articles and those irrelevant to the topic, the abstracts of the articles of interest were reviewed, as were their references, to identify additional articles (Fig. 1). Five articles met the inclusion criteria (Table 2). Were evaluated type of technique, material and complication after the procedure.

Article selection algorithm
It was found that in some papers the anterior tibial tendon fixation technique was not described. Additionally, most of the papers with ATTT in the relapsed clubfoot use the classic pull-out technique, with an external button, first described by Ponseti [7, 16,17,18,19]. The prospective study by Mindler and colleagues aimed to study the biomechanics of the foot after ATTT in children with relapsed clubfoot [3]. The ATTT was performed in 25 feet. The tendon was fixed with an endobutton combined with a biotenodesis screw. Unfortunately, postoperative complications were not reported in this study, so no conclusions can be drawn about this form of fixation. However, it is important to highlight their conclusions regarding the improvement of gait and mobility of the foot after ATTT. Forefoot supination in relation to the hindfoot and tibia was reduced during swing and at initial contact, and heal showed less dynamic varus and adduction. In kinect there was na increase of the power o maximum ankle dorsiflexion.
Another one that refer to the type of fixation is the one proposed by Pedraza et al. Also Pedraza et al. applied this type of fixation in their alternative ATTT technique. They carried out a prospective, longitudinal, and observational study [14]. The patients were divided into two groups according to the type of distal fixation used: 20 patients (32 feet) with external plantar button fixation and 14 (22 feet) with suture to the plantar fascia. They reported significant differences according to the characteristics in superficial infection and pain in distal fixation after removing the cast, these being significantly higher in the group with plantar button. These differences probably explain why the group treated with suture to the plantar fascia had better tolerance to an early start of physical therapy after surgery.
Rhee et al. published their case series of 23 patients (34 feet) for ATTT using endobutton technique. They showed that they had a percentage of complications of 14.7% of which recurrence occurred bilaterally in 1 patient (5.9%) and there was a loss of fixation of the suture button (2.9%) in another case. Other complications included a cast-related pressure sore (2.9%) and an infection (2.9%) requiring irrigation with debridement along with hardware removal [11].
Yasin et al. described a different technique to avoid the skin complications related to the use of an external button for anterior tibial fixation. After making a bone tunnel in the lateral cuneiform and passing the anterior tibial tendon with the sutures, they used a K-wire from lateral to medial, crossing perpendicularly the bone tunnel and the anterior tibial tendon with the sutures, to anchor it after tensioning. This technique was used in 26 feet, and the authors report no cases of anterior tibial anchorage or tension loss or K-wire infection. Only in 3 cases there was slight skin erosions in the K-wire region, which resolved spontaneously within the first week after wire removal [12].
Also, Ploeger and his colleagues described a different technique of tibialis anterior tendon fixation for the treatment of clubfoot recurrence. These authors make a perforation of the lateral cuneiform, without reaching the plantar cortex, and anchor the tendon in that area, with a transosseous suture in the medial and lateral cortices, with the ends of the tendon preparation sutures knotting in the dorsal region of the lateral cuneiform. In this study 26 feet were included; no complications related to the fixation technique were reported. At 12 months follow-up 3 feet relapsed [15].
Recently, Ayub and colleagues published a series of patients who underwent ATTT with anchor tendon fixation. In this study, of the 77 feet submitted to ATTT, the authors report that there was no case of anchor failure; they had one case with recurrence of dynamic supination probably related to poor tendon tensioning; they also report one case of superficial infection, which was washed and debrided without the need to remove the anchor. Additionally, in 7 cases there was a need for repeat treatment with serial casts for recurrent loss of dorsiflexion and/or abduction, and in 4 cases a new surgical intervention was required to improve the position of the foot [13].
Those studies are all observacional and retrospective.
Discussion
Some authors are concerned about the classic fixation technique with an external button since skin perforation in the plantar region of the foot may be associated with infection or skin irritation associated with pressure from the button [11, 12, 20].
A recent study reported on a series of cases undergoing anterior or posterior tibial transfer with fixation by an external plantar button. Nine adult patients with multiple comorbidities (diabetes, history of amputation at different levels in the foot, history of chronic kidney disease or peripheral arterial disease) were included. No complications have been documented with this method of fixation. The authors state that this technique is not only safe for children, especially those with clubfoot, but is also safe for patients with a predisposition to skin complications (diabetes or peripheral arterial disease) [21]. This study corroborates the safety of this procedure.
Additionally, there is also some risk of injury to the plantar nerves and vessels when the surgeon performs the bone tunnel and the passage of the sutures from the tendon to the plantar region [10,11,12,13,14, 20]. The study by Radler et al. concludes that this technique is safe, and that nerve damage can be minimized if the drilling of the bone is directed towards the mid-region of the plantar surface; additionally, the use of a blunt needle to pass the sutures may be beneficial [22].
Another concern associated with the use of external button is the early failure of fixation associated with suture breakage or after removal of the button, since in this technique the maintenance of tension depends exclusively on the healing of the tendon to bone [10, 14, 23]. The strength of the fixation between surgery and during the post-operative immobilization and rehabilitation period is crucial to allow bone-tendon integration. Some studies have shown some vulnerability at the bone-tendon interface in the early stages of healing and suggest that this process requires 8 to 26 weeks [24]. Thus, there may be some advantage in using fixation methods that are maintained for longer periods of time, compared to the standard 6 weeks of external button fixation. However, there is already a lot of experience with this form of fixation, with very good long-term results reported in the literature and no reports of complications or failure [25].
Current publications report that there are complications associated with the use of new fixation devices in foot tendon transfers, namely interference screws. The only article that used an interference screw for tibialis anterior fixation and met the inclusion criteria for this review does not describe postoperative complications. Clanton et al. in their case series of 31 patients who underwent different tendon transfers in the foot, using bioabsorbable screws, demonstrated a complication rate of 39%. According to the authors, all the complications reported were most likely related to the tendon transfer procedure itself, and not directly related to the bioabsorbable screw [26]. There are several problems described in the literature with the use of this method of fixation, including screw breakage, screw loosening, inflammatory reactions, and tendon laceration during screw insertion [26]. Additionally, these materials are associated with high costs. Moreover, cuneiform ossification is a limitation in younger children [20].
Rhee and colleagues in their work using endobutton, concluded that using button suture in ATTT is a safer procedure, with theoretical advantage of providing stronger fixation and reducing the risk of skin pressure necrosis compared to the standard external button technique [11]. The results of this study are corroborated by the results of a biomechanical study in cadavers, where a comparison of traditional external button fixation and internal suspension was performed in ATTT. The results showed that the internal button fixation has significantly less displacement of the tendon within the bone tunnel than the external button technique, both with dynamic and static loading [10]. Nevertheless, it is not known how clinically significant this difference is and the price of these suspension systems are much higher compared to the traditional technique.
It is not a lesser fact than in a survey made to the members of the Pediatric Orthopedic Society of North America (POSNA), Hosseinzadeh et al. report that the preferred technique is a transfer of the tendon to the lateral cuneiform (73%), and the majority (72%) use a button as the method of fixation. However, it does not refer to which type of button [27].
In recent years the use of suture anchors has grown exponentially. Fennel et al. in a cadaveric study recommend suture anchors as they would be easier to insert and less traumatic to the bone than the bone tunnel technique [28]. However in vivo situation is very different because pull-out fixation also depends on integration of the tendon into the bone tunnel.
The only paper that was found that reported the use of anchors in ATTT only mentions one case in which the correction of dynamic supination was incomplete due to inadequate tendon tensioning, and they do not report other complications related to implant failure [13]. However, we have case reports of complications by different experienced surgeons. According to their experience, they did not have optimal results. They also required to perform revision surgery due to loosening of the anchor. The photos are shown in Figs. 2 and 3, and 4.

Loosening and infection of an anchor suture. Cortesy by Dr Rafael Batalha from Brazil

Loosening and exposition of the suture anchor. Cortesy of Dr Rodrigo Branco from Brazil

Immediate post-operative X-ray (left) and X-ray 4 months post-operative (right), demonstrating loosening of the bone anchor. Cortesy by Dr Cristina Alves from Portugal / Ponseti International Meeting Barcelona 2014
Other tendon fixation techniques have also been described, either with K-wires [12] or with transosseous suture [15]. In these studies, no complications related to the type of fixation were described, and they do not require specific material that increases the cost of the procedure. Still, they are small case series, so their effectiveness and safety cannot be extrapolated.
The classic technique of anterior tibial fixation with pull-out and external button is inexpensive, technically simple, and effective, as shown in several studies [7, 16, 18, 21, 25].
Gray and colleagues, in a prospective study, compared a group with relapsed clubfoot after treatment with Ponseti’s method, with an indication for ATTT (24 feet), with a group of patients with the same initial treatment but who had no relapse (18 feet). They concluded that ATTT is an effective procedure, which restores the balance of eversion and reversal force. Additionally, they found that this procedure results in similar function and satisfaction as children with clubfoot treated with Ponseti’s method who did not relapse. In this study, the anterior tibial tendon was fixed in the lateral cuneiform with the classic technique over a plantar external button and no postoperative complications were reported [16].
Agarwal et al. compared three different techniques (ATTT for third cuneiform – classic Ponseti technique, ATTT for the cuboid, and split transfers to cuboid) and found no statistically significant differences in foot and ankle function between the different techniques, however the technique described by Ponseti tended to show better dorsiflexion and eversion compared to other techniques [7]. In all techniques the tendon was fixed with the classic pull-out technique and the authors report that no major complications were observed in any of the groups [7].
Also, Thompson et al., retrospectively evaluated 137 feet undergoing ATTT for clubfoot recurrence. The plantar pull-out technique was used for fixation of the tibialis anterior. The authors denied postoperative complications, including loss of tendon tension, postoperative infections, or neurovascular damage [17].
In another study, two groups undergoing ATTT for clubfoot relapse (35 feet) were compared: one group treated initially with manipulations according to Ponseti’s technique and another group treated initially with posteromedial release [18].
The percentage of relapse was similar in both groups, reinforcing the fact that posteromedial release does not reduce the incidence of relapse. On the other hand, relapses in feet initially treated with extensive posteromedial release had higher stiffness when compared to those treated with Ponseti’s method. The ATTT was performed with the classic pull-out technique and there is no reference to postoperative complications related to the method of tendon fixation. The clinical outcomes assessed at the end of skeletal maturity were significantly different in the 2 series of patients, with better clinical outcomes in the group of patients initially treated with Ponseti’s method, this difference probably being related to the increased foot stiffness in the group of patients initially undergoing extensive posteromedial releases [18].
Holt et al. demonstrated that the treatment algorithm based on serial casts to regain correction, new Achilles tenotomy and ATTT is effective in the long term [25]. They demonstrated that ATTT improves foot function in adult patients who had been treated for recurrence of idiopathic clubfoot during childhood, with a follow-up of 37 to 55 years. They used the traditional fixation method, which confirms the effectiveness and safety of this technique.
Masrouha and Morcuende studied relapses after ATTT, a retrospective study in which they observed that of 66 patients, ten had recurrence after ATTT [19]. In all of them they used the traditional fixation method. The authors conclude that the recurrence would be related to performing the ATTT at an early age or neurologic deficits and not necessarily due to the fixation method used.
Conclusion
Several options have now emerged for tendon fixation in tendon transfers around the foot and ankle, including ATTT for treatment of relapsed clubfoot. To our knowledge this is the first paper that questioned the potential complications associated with the use of these new techniques, such as loss of fixation or tension, infection, and skin bruises. They are severe because compromise the results of surgery. Due to the scarcity of published works in favor of other fixation methods, we believe that the traditional method is the optimal one for the transfer of the tendon of the tibialis anterior muscle.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Ponseti IV, Smoley EN. Congenital club foot: the results of treatment. J Bone Joint Surg. 1963;45:261–75.
Zionts LE, Ebramzadeh E, Morgan RD, Sangiorgio SN. Sixty years on: Ponseti method for clubfoot treatment produces high satisfaction despite inherent tendency to relapse. J Bone Joint Surg Am. 2018;100:721–8. https://doi.org/10.2106/JBJS.17.01024.
Mindler GT, Kranzl A, Radler C. Normalization of Forefoot Supination after Tibialis Anterior Tendon transfer for dynamic clubfoot recurrence. J Pediatr Orthop. 2020;40:418–24. https://doi.org/10.1097/BPO.0000000000001542.
Ponseti I. Relapsing clubfoot: causes, prevention, and treatment. Iowa Orthop J. 2002;22:55–6.
Radler C, Mindler GT. Treatment of severe recurrent clubfoot. Foot Ankle Clin. 2015;20:563–86. https://doi.org/10.1016/j.fcl.2015.07.002.
Zionts LE, Jew MH, Bauer KL, Ebramzadeh E, Sangiorgio SN. How many patients who have a clubfoot treated using the Ponseti Method are likely to Undergo a Tendon transfer? J Pediatr Orthop. 2018;38:382–7. https://doi.org/10.1097/BPO.0000000000000828.
Agarwal A, Jandial G, Gupta N. Comparison of three different methods of anterior tibial tendon transfer for relapsed clubfoot: a pilot study. J Clin Orthop Trauma. 2020;11:240–4. https://doi.org/10.1016/j.jcot.2018.09.001.
Holt JB, Westerlind B, Morcuende JA. Tibialis anterior tendon transfer for relapsing idiopathic clubfoot. JBJS Essent Surg Tech. 2015;5:e16. https://doi.org/10.2106/JBJS.ST.O.00015.
Núñez-Pereira S, Pacha-Vicente D, Llusá-Pérez M, Nardi-Vilardaga J. Tendon transfer fixation in the foot and ankle: a biomechanical study. Foot Ankle Int. 2009;30:1207–11. https://doi.org/10.3113/FAI.2009.1207.
Pathy R, Sturnick DR, Blanco JS, Dodwell ER, Scher DM. Biomechanical comparison of suture-external button fixation vs internal suspension fixation for Tendon transfers of the feet. Foot Ankle Int. 2019;40:845–52. https://doi.org/10.1177/1071100719839691.
Rhee C, Burgesson B, Orlik B, Logan K. Suture button technique for Tibialis Anterior Tendon transfer for the treatment of residual clubfoot. Foot Ankle Orthop. 2020;5:1–8. https://doi.org/10.1177/2473011420923591.
Yasin ES, Amin HE, Ghani HA. A new anchoring technique for tibialis anterior tendon transfer. J Pediatr Orthop B. 2020;29:379–81. https://doi.org/10.1097/BPB.0000000000000691.
Ayub AAA, Firth GB, Green GL, Bijlsma P, Ramachandran M. Tibialis anterior tendon transfer using bone anchor for dynamic supination in congenital talipes equinovarus. J Pediatr Orthop B. 2023;32:15–20. https://doi.org/10.1097/BPB.0000000000000997.
Pedraza LAML, Cuevas JGL, Anaya VC, Linage RG, Moreno EMS. Complicaciones asociadas a la fijación distal de transferencia del tibial anterior a la tercera cuña del pie en pacientes pediátricos con pie equino varo aducto congénito. Comparación De Dos diferentes técnicas. Acta Méd Grupo Ángeles. 2021;19:333–9. https://doi.org/10.35366/101724.
Ploeger MM, Wimmer MD, Rommelspacher C, Bornemann R, Placzek R. [Minimally invasive tibialis anterior tendon transfer in shuttle technique for the treatment of clubfoot recurrence in adolescent patients]. Oper Orthop Traumatol. 2022;34:431–7. https://doi.org/10.1007/s00064-022-00776-5.
Gray K, Burns J, Little D, Bellemore M, Gibbons P. Is tibialis anterior tendon transfer effective for recurrent clubfoot? Clin Orthop Relat Res. 2014;472:750–8. https://doi.org/10.1007/s11999-013-3287-x.
Thompson GH, Hoyen HA, Barthel T. Tibialis anterior tendon transfer after clubfoot surgery. Clin Orthop Relat Res. 2009;467:1306–13. https://doi.org/10.1007/s11999-009-0757-2.
Farsetti P, Caterini R, Mancini F, Potenza V, Ippolito E. Anterior tibial Tendon transfer in relapsing congenital Clubfoot Long-Term Follow-Up study of two series treated with a different protocol. J Pediatr Orthop. 2006;26:83–90. https://doi.org/10.1097/01.bpo.0000188999.21427.fb.
Masrouha KZ, Morcuende JJ. Relapse after Tibialis Anterior Tendon transfer in idiopathic clubfoot treated by the Ponseti Method. J Pediatr Orthop. 2012;32:81–4. https://doi.org/10.1097/BPO.0b013e31823db19d.
Meyer Z, Polk J, Zide J, Kanaan Y, Riccio A. Lateral cuneiform ossification and Tibialis Anterior Tendon Width in Children ages 3 to 6: implications for interference screw fixation of Tibialis Anterior Tendon transfers in Children. J Pediatr Orthop. 2022;42:229–32. https://doi.org/10.1097/BPO.0000000000002077.
Cook HR, McKeon K, Proal JD, Garada F, Atves JN. Tendon transfer via self-made nonproprietary external button: technique paper and case series. Foot Ankle Surgery: Techniques Rep Cases. 2022;2:100246. https://doi.org/10.1016/j.fastrc.2022.100246.
Radler C, Gourdine-Shaw MC, Herzenberg JE. Nerve structures at risk in the plantar side of the foot during anterior tibial tendon transfer: a cadaver study. J Bone Joint Surg Am. 2012;94:349–55. https://doi.org/10.2106/JBJS.K.00004.
Wu KW, Huang SC, Kuo KN, Wang TM. The use of bioabsorbable screw in a split anterior tibial tendon transfer: a preliminary result. J Pediatr Orthop B. 2009;18:69–72. https://doi.org/10.1097/bpb.0b013e328329429a.
Hjorthaug GA, Madsen JE, Nordsletten L, Reinholt FP, Steen H, Dimmen S. Tendon to bone tunnel healing - A study on the time-dependent changes in biomechanics, bone remodeling, and histology in a rat model. J Orthop Res. 2015;33:216–23. https://doi.org/10.1002/jor.22756.
Holt JB, Oji DE, Yack HJ, Morcuende JA. Long-term results of tibialis anterior tendon transfer for relapsed idiopathic clubfoot treated with the ponseti method a follow-Up of thirty-seven to fifty-five years. J Bone Joint Surg Am. 2015;97:47–55. https://doi.org/10.2106/JBJS.N.00525.
Clanton TO, Betech AA, Bott AM, Matheny LM, Hartline B, Hanson TW, et al. Complications after tendon transfers in the foot and ankle using bioabsorbable screws. Foot Ankle Int. 2013;34:486–90. https://doi.org/10.1177/1071100713477625.
Hosseinzadeh P, Kelly DM, Zionts LE. Management of the relapsed clubfoot following treatment using the Ponseti method. J Am Acad Orthop Surg. 2017;25:195–203. https://doi.org/10.5435/JAAOS-D-15-00624.
Fennell CW, Ballard JM, Pflaster DS, Adkins RH. Comparative evaluation of Bone Suture Anchor to bone tunnel fixation of Tibialis Anterior Tendon in Cadaveric Cuboid bone: a Biomechanical Investigation. Foot Ankle Int. 1995;16:641–5. https://doi.org/10.1177/107110079501601011.
Acknowledgements
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
AM (0009-0009-3991-7995) Conceptualization, Data curation, Investigation, Methodology, Visualization, Writing – Original Draft Preparation, Writing – Review & Editing; LBR (0009-0006-1247-1880) Data curation, Investigation; DCP (0009-0005-83165699) Writing – Review & Editing; MPN (0000-0001-5892-2532) Conceptualization, Formal Analysis, Methodology, Validation, Writing – Review & Editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This study was performed at the Hospital do Servidor Público Estadual de São Paulo, Sao Paulo, SP, Brazil.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Moreira, A., Benjamin Ravetti, L., Carrapeiro Prina, D. et al. Anterior tibial tendon transfer in idiopathic clubfoot: pull-out vs. other fixations – a systematic review. BMC Musculoskelet Disord 25, 638 (2024). https://doi.org/10.1186/s12891-024-07621-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07621-9