
Abstract
Background
Little is known about why patients with low back pain (LBP) respond differently to treatment, and more specifically, to a lumbar stabilization exercise program. As a first step toward answering this question, the present study evaluates how subgroups of patients who demonstrate large and small clinical improvements differ in terms of physical and psychological changes during treatment.
Methods
Participants (n = 110) performed the exercise program (clinical sessions and home exercises) over eight weeks, with 100 retained at six-month follow-up. Physical measures (lumbar segmental instability, motor control impairments, range of motion, trunk muscle endurance and physical performance tests) were collected twice (baseline, end of treatment), while psychological measures (fear-avoidance beliefs, pain catastrophizing, psychological distress, illness perceptions, outcome expectations) were collected at four time points (baseline, mid-treatment, end of treatment, follow-up). The participants were divided into three subgroups (large, moderate and small clinical improvements) based on the change of perceived disability scores. ANOVA for repeated measure compared well-contrasted subgroups (large vs. small improvement) at different times to test for SUBGROUP × TIME interactions.
Results
Statistically significant interactions were observed for several physical and psychological measures. In all these interactions, the large- and small-improvement subgroups were equivalent at baseline, but the large-improvement subgroup showed more improvements over time compared to the small-improvement subgroup. For psychological measures only (fear-avoidance beliefs, pain catastrophizing, illness perceptions), between-group differences reached moderate to strong effect sizes, at the end of treatment and follow-up.
Conclusions
The large-improvement subgroup showed more improvement than the small-improvement subgroup with regard to physical factors typically targeted by this specific exercise program as well as for psychological factors that are known to influence clinical outcomes.
Similar content being viewed by others
Introduction
Low back pain (LBP) remains one of the most common and incapacitating health conditions worldwide [1]. There is strong evidence to recommend exercise programs after the acute phase, at least for reducing pain and disability [2]. However, the treatment effects for any exercise program are moderate at best for non-acute and non-specific LBP [3] and initial reviews/meta-analyses have not demonstrated the superiority of one type of exercise program over another [3, 4]. Consequently, to increase the positive impact of any treatment for LBP, research needs to determine who is likely to benefit from these treatments (e.g., specific, matched exercise interventions) based on clinical presentation and to identify the mechanisms of benefit responsible for clinical improvement.
One active exercise modality, lumbar stabilization exercise programs (LSEPs), has a solid scientific foundation and has been in use for several years [5,6,7]. Interestingly, although the quality of the evidence is low [8], two meta-analyses support the effectiveness of the two components that make up most LSEPs, namely coordination/stabilization exercises and strength/resistance exercises [8, 9]. Effectively, LSEPs target motor control and coordination of the paraspinal and abdominal muscles and may also progressively overload muscles to enhance trunk muscle endurance [5,6,7].
As the most recent Cochrane systematic review on the topic points out [10], an evidence-based patient/intervention linkage is still not established for identifying patients who respond best to a LSEP. A preliminary clinical prediction rule (CPR), at the derivation stage (n = 54 participants), has been proposed [11], but its formal validation was unsuccessful due to a lack of statistical power [12]. Our group has more recently conducted a cohort (observational) study to derive CPRs of success (or large improvement) at the end of the eight-week treatment (n = 110 participants) and at the six-month follow-up (n = 100 participants), using disability as the main clinical outcome [13]. Several candidate predictors of clinical success were measured at baseline for the CPRs development but were also measured at mid-treatment (psychological variables) as well at the end of treatment (physical and psychological variables) and six-month follow-up (psychological variables). Some of these measures may explain clinical improvement for such a specific exercise program, such as decreased aberrant movements or pain during movements, increased trunk muscle endurance or decreased fears, psychological distress and illness perceptions, to name a few. The design of this study does not allow identification of the corresponding mechanisms of benefit as this would require a randomized controlled trial (RCT) [14]. However, as a preliminary step toward identifying these mechanisms, the present study aims at exploring how subgroups of patients showing large and small clinical improvements in terms of disability also differ in terms of physical and psychological changes during treatment.
Materials and methods
Most of the study methodology is summarized here. The reader is referred to Larivière, Rabhi [13] for more details.
Design of the study
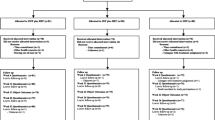
A per-protocol prospective cohort/observational study was carried out with three assessments during the intervention (T0, T4 and T8 weeks) and one assessment at six-month follow-up (T34) (Fig. 1).
Participants
Participants were recruited and assessed from July 2012 to August 2016 (preliminary study or phase 1) and from July 2018 to October 2020 (phase 2). They were French- or English-speaking and aged between 18 and 65 years. They had lumbar or lumbosacral pain for at least four weeks (non-acute phase), with or without radicular pain. They had a minimum score of 12% on the Oswestry Disability Index (ODI) [15] to allow a minimal clinically important change of 10% [16] to occur. Exclusion criteria were: a specific lumbar pathology (fracture, infection or tumor) or scoliosis; surgery on the pelvis or spinal column; systemic or degenerative disease; thoracic or neck pain that is more severe than LBP; pregnancy; starting an exercise program within the last six months; litigation relative to the back injury. A final exclusion criterion was the presence of one positive neurological sign in two of three test categories: (a) reduced Achilles and patellar tendon reflexes, (b) reduced strength in lumbosacral myotomes, (c) reduced sensation in lumbosacral dermatomes.

From Larivière, Rabhi [13]. Four categories of measures (OUT, PHY, PSY, NRM) were collected at different times during (T0, T4, T8) and following (T34) the lumbar stabilization exercise program. PHY and NRM measures are more burdensome and were consequently only collected at T0 and T8. NRM measures were not considered in the present study
Lumbar stabilization exercise program (LSEP)
An eight-week individualized LSEP (two, 30-min sessions/week) was provided in local physiotherapy clinics. No co-intervention was allowed except medication. The exercise program has been thoroughly described elsewhere in a supplementary file linked to a previous publication ( [17]; see Additional file 1). Briefly, The LSEP comprised three distinct phases: (1) Pain Management. over a maximum period of two weeks: This involved isolated contractions of the transversus abdominis (TrA) and lumbar multifidus (LuM) muscles followed by gradual incorporation of TrA/LuM co-contractions during low-load exercises.; (2) Early Impairment and Functional Level: Exercises emphasized quality of movement control; (3) Moderate/Advanced Impairment and Functional Level: As patients progressed, the program shifted to muscle endurance. Exercises were designed with higher volume and intensity, all while maintaining co-contractions of TrA and LuM. All the participants reached the third (final) phase during the 8-week program. The participants were also encouraged to do the exercises at home.
In order to standardize the information given to participants on their condition, the Back Book booklet [18], or its French translation (Guide du dos : ISBN: 978-2-923465-03-6), was given to participants at their first clinical visit. The booklet aimed to change beliefs and behaviours (resuming activities) related to back pain.
Home-exercise adherence
Home-exercise adherence was assessed twice: once after the exercise program (T8), to measure adherence during the 8-week program, and once at six-month follow-up (T34), to measure adherence following the 8-week program. Questions about home-exercise adherence were not asked during the 8-week treatment so as not to influence participant behavior [19]. The question was “How many times have you done your exercises as prescribed in the last week?”. The physiotherapists’ prescription was based on each participant’s needs. Exercises were generally prescribed every day during phase I (pain management and motor control of deep muscles), and three times a week during phases II (initiation of exercises with emphasis on quality of movement control) and III (endurance development with emphasis on quantity). Based on the most common definition of adherence, i.e. “the extent to which the patient follows medical instructions” [20], the frequency per week was divided by the physiotherapist’s recommendation to obtain a ratio. The ratio may vary between 0 and 1, 1 being given when the frequency was equal to or higher than prescribed. Every participant reached phase III, wherein the prescribed frequency was generally three times a week. Consider this scenario: If the recommended exercise frequency was three sessions per week (as typically observed during week eight of the clinical program), and the patient actually completed only 2 sessions per week, the resulting adherence ratio would be 0.66 (equivalent to 2 out of 3 sessions).
Assessments
A detailed description of the questionnaires used to measure the clinical outcomes (OUT) and psychological (PSY) variables and of the tests used during the physical examination (PHY) is provided in the Supplementary file. These variables are summarized in Table 1.
To reduce the likelihood of spurious findings at the derivation stage of the CPRs, the potential variables were selected according to a sound theoretical rationale using well-known theoretical models, namely the neuromuscular spine instability model [45, 46], the fear-avoidance model of pain [47] and the common-sense model of illness [48, 49], the latter being used to predict treatment adherence [50]. They were classified as Class-A, B and C variables, depending on their relationship with the theoretical background (or potential mechanisms of benefit) of the LSEP. Class A were physical variables specifically (theoretically) associated with the treatment, either in direct or indirect relation to lumbar stability. Class B are psychological variables potentially related to adherence and, as such, may influence outcomes through adherence to the home exercise program [51, 52]. Class C were the other physical variables, namely the range of motion at different joints here, that were not theoretically associated with this treatment and, as such, may be associated with other exercise programs. This A-B-C classification can be used as our current study hypotheses, namely that the large-improvement group (LIG) would show more improvement in Class-A and Class-B variables than the small-improvement group (SIG), while this would not be case for Class-C variables.
Clinical outcome (OUT) measures
The ODI [15], a self-report measure of disability, was used to define subgroups. Pain intensity was measured for the last week preceding each time point, using an 11-point (0 to 10) numeric pain rating scale (NPRS). To relate pain to activities, participants were also asked whether they had experienced increased pain (yes/no) during general activity or exercise. Finally, to get an aggregate measure of physical and psychological factors, the Subgroups for Targeted Treatment (STarT) Back Screening Tool [24] was used to assess the risk of unfavorable prognosis.
Physical assessment (PHY measures) for Class-A and Class-C variables
The physical examination comprised tests that can be theoretically related to lumbar segmental instability (LSI) or motor control impairments (MCI) [53,54,55], all with acceptable interrater reliability [kappa > 0.6; intraclass correlation coefficients - ICC > 0.70; [53]], as detailed in the Supplementary file. PHY testing covered different dimensions as follows: (1) LSI (n = 4) (2), MCI (n = 7) (3), posture and range of motion (ROM) (n = 6) (4), trunk muscle endurance (TME) (n = 4) and (5) physical performance tests (PPT) (n = 4). Regarding MCI tests, only symptoms caused by these tests were considered because the assessment of clinical signs (alignment, movements) is less reliable [56]. MCI tests are named “motor control impairment” because they are used within a clinical system whose overall goal is to determine whether the individual can actively control the kinematic chain in a manner that generally favours movement in the extremities and stability in the spine. Measures taken from both sides of the body (e.g., right and left lateral trunk flexion; left and right lower extremity measurements) were managed with the goal of retaining the measurements most associated with impairments. Specifically, only the minimal ROM (exception: lateral trunk flexion) and TME scores across left and right sides, as well as the maximal scores during PPT (related to slow movements) and MCI tests were selected for further analyses.
Psychological assessment (PSY measures) for Class-B variables
Patient-reported outcome measures included variables from the fear-avoidance model (pain catastrophizing, fear-avoidance beliefs of physical activity, psychological distress, habitual physical activity) and variables theoretically related to home-exercise adherence [57,58,59,60]: illness perception and outcome expectations related to the exercise program.
Statistics
The sample size was determined to have enough statistical power for the derivation of the CPRs, as detailed elsewhere [13], using preliminary findings [21] derived from 64 participants distributed in four subgroups (see next paragraph), namely large improvement (n = 31), moderate improvement (n = 5), small improvement (n = 12), and dropouts (n = 16). The intent was to have enough participants in the ‘large’ and ‘small’ subgroups to derive the CPRs. These numbers were also considered suitable for the purpose of conducting subgroup analyses based on ANOVAs for repeated measures.
At two time points (T8 or T34), three subgroups of participants were defined according to their level of improvement using ODI relative to baseline (T0): (1) large-improvement group (LIG) (2), moderate-improvement group, and (3) small-improvement group (SIG). For each participant, the ODI change score (e.g., ODI = ODIT0 - ODIT8) and the corresponding percentage [eg, ODI% = ((ODIT0 - ODIT8) / ODIT0) × 100] were calculated. A 50% improvement threshold with the ODI has been used previously [11] and more recently substantiated as a valid criterion for defining clinical success in participants with LBP [61]. Also considered was a clinically important change of 10 points in ODI scores [16]. These criteria were used to define the three subgroups:
-
Large-Improvement Group (LIG): ODI% ≥ 50.
-
Moderate-Improvement Group: ODI% < 50%, but ODI ≥ 10.
-
Small-Improvement Group (SIG): ODI% < 50% and ODI < 10.
For continuous PHY and PSY measures, two-way ANOVAs for repeated measures on the TIME factor were modulated based on available data at the four time points as follows: for PHY measures, 2 SUBGROUP (SIG: n = 45; LIG: n = 54) × 2 TIME (T0 and T8) ANOVAs; for PSY measures, 2 SUBGROUP × 4 TIME (T0, T4, T8 and T34).
For categorical PHY and PSY variables, a mixed statistical model is not available; thus, only the TIME factor was studied, for each subgroup (SIG and LIG) separately. Although many tests produce dichotomous scores (0 = negative test; 1 = positive test), MCI test scores have three levels (-1: pain decreases; 0: same pain; 1: pain increases). These scores were first dichotomized to separate participants with a positive test (score of 1) from other participants (0 assigned to scores of 0 and − 1). The McNemar test was then applied to the PHY variables (time T0 versus T8) while the Cochran Q test was applied to the PSY variables (T0, T4, T8 and T34) in order to compare the proportion of positive tests between the measurement times.
Because there was no control group composed of participants who did not receive the treatment, it was not possible to attribute the TIME effect to time or to treatment, which is why “time/treatment effect” is used in the following text.
For a clearer interpretation of the magnitude of the effects (for continuous variables), effect sizes were calculated using formulations analogous to Cohen’s d, namely the Hedges’ gs (for independent groups) and gav (for repeated measures), allowing for comparisons between within-subjects and between-subjects effects [62]. Like Cohen’s d, a g value of 0.2–0.5 is interpreted as a “low” effect, 0.5–0.80 “average” and > 0.8 “strong” [62]. To facilitate interpretation, g values to describe the TIME effect were calculated so that negative values indicate a decrease over time.
Results
Participants characteristics, home-exercise adherence and effect of the LSEP on clinical outcomes
The participants meeting the criteria for LIG, moderate improvement and SIG at T8 were 54 (23 males + 31 females), 11 (4 M + 7 F) and 45 (23 M + 22 F), respectively. At T34, they were 53 (25 M + 28 F), 11 (1 M + 10 F) and 36 (16 M + 20 F), respectively.
Demographic, anthropometric and clinical characteristics of the participants are described in Table 2, which demonstrates that all characteristics were equivalent between the LIG and SIG. The sex distribution was also equivalent between the LIG (23 M, 31 F) and SIG (23 M, 22 F), as tested with the Wald Chi-square test (P = 0.397). For the duration of the self-reported LBP, 98% (108/110) of participants had chronic pain (3 months or more), distributed as follows [63]: less than one month (n = 0), 1–3 months (n = 2), 3–6 months (n = 2), 6–12 months (n = 12), 1–5 years (n = 40), > 5 years (n = 54).
As it was a per-protocol observational study, all the 110 participants attended at least 14 out of the 16 physiotherapy treatments over the eight-week LSEP. One-hundred participants reached the six-month follow-up. The ratio of home-exercise adherence did not differ between subgroups at either T8 (SIG: 0.79 ± 0.31; LIG: 0.82 ± 0.27; P = 0.604) or T34 (SIG: 0.43 ± 0.40; LIG: 0.55 ± 0.39; P = 0.165).
For all participants as well as for the three subgroups (large, moderate and small improvement), a detailed description of the effect of the LSEP on ODI and NPRS outcome measures is provided elsewhere [13]. For the study population as a whole, the LSEP generated strong clinical effects. The ODI decreased significantly (P < 0.05) from baseline to T8 (n = 110; Cohen’s d = -1.24) and from baseline to T34 (n = 100; d = -1.24). Significant improvements were also observed for NPRS, with corresponding d scores showing strong effect sizes (-1.70 at T8 and − 1.32 at T34).
Clinical outcome (OUT) measures
Continuous variables
Results corresponding to the ODI are not considered here as the ODI was used to determine the LIG and SIG. A statistically significant SUBGROUP (SIG, LIG) × TIME (T0, T8) interaction was observed for pain intensity (NPRS) and the STarT Back screening tool, as illustrated in Fig. 2. For both measures, the LIG showed progressively lower scores than the SIG as time elapsed, reaching moderate to strong effect size.

Statistically significant SUBGROUP × TIME interactions obtained for the Numeric pain rating scale (NPRS) and prognostic screening tool (STarT Back). Standard deviations were not shown for clarity. Significant differences as detected with post hoc tests are identified with the corresponding g values (effect sizes) for between-subgroup differences and by horizontal lines for between-time differences. For example, the horizontal lines on the upper left plot indicate significantly higher pain intensity at T0 comparatively to T4, T8 and T34 as well as higher pain at T4 than at T8
Dichotomous variables
The proportion of LIG participants having pain during physical activity (ActRelPain) decreased over time (77, 56, 25, and 23% for times T0, T4, T8, and T34, respectively), which appears to be better than the decrease obtained in the SIG (70, 59, 48, and 41%), but no nonparametric test allows for this two-factor (SUBGROUP × TIME) comparison. Although each of the comparisons (Cochran’s test) led to a significant TIME main effect (P < 0.001), post hoc tests (McNemar), combined with an adjustment of alpha for the number of comparisons (n = 6, so P = 0. 05/6 = 0.00833), were significant only for the LIG (T0 = T4; T0 < T8 and T34; T0 < T8 and T34; T8 = T34).
Physical assessment (PHY measures)
Continuous variables
The SUBGROUP (SIG, LIG) × TIME (T0, T8) ANOVAs revealed six SUBGROUP × TIME interactions (Table 3), as shown in Fig. 3. In all cases, the SIG and LIG were not different at T0, but all measures showed a more favorable effect for the LIG than for the SIG.
The effect of time/treatment, without interaction with the SUBGROUP factor, was also statistically significant for six other variables (Table 3), all indicating improvement over time. Although the corresponding effect sizes were small for most of them, i.e., for TME-Abdominals (g = 0.15; from T0: 56 ± 55 s to T8: 65 ± 68 s), PSLR-Pain ROM-min (g = 0.18 from T0: 72 ± 15° to T8: 74 ± 14°), PelvisFlx-ROM (g = 0.35; from T0: 77 ± 17° to T8 : 83 ± 15°), LumbLatFlx-ROM-Min (g = 0.31; from T0: 23 ± 9° to T8: 25 ± 10°), and MCIP-HipER-Pas-ROM-min (g = 0.27; from T0: 59 ± 10° to T8: 62 ± 10°), it was average for ASLR-Act/5-max (g = -0.53; from T0: 0.91 ± 1.20 /5 to T8: 0.39 ± 0.76 /5).
Dichotomous variables
For the vast majority of these tests, the LIG showed a significant improvement from T0 to T8, whereas the SIG showed no effect (Table 4).
Psychological assessment (PSY measures)
The SUBGROUP (SIG, LIG) × TIME (T0, T4, T8, T34) ANOVAs revealed three statistically significant interactions (Table 5; Fig. 4). They included fear-avoidance beliefs about physical activity (FABQ-AP), pain catastrophizing (PCS) and illness perceptions (B-IPQ). These interactions all behave similarly as LIG and SIG were equivalent at T0, but the LIG showed more improvements over time compared to the SIG, reflected in the differences between groups, detected as early as T4, increased until T8 and finally stabilized at T34 (Fig. 4).

SUBGROUP × TIME interactions obtained for the continuous PHY variables. Standard deviations were not shown for clarity. Significant differences obtained with post hoc tests are identified with the corresponding g values (effect sizes). TME: trunk muscle endurance; PPT: physical performance test

Statistically significant SUBGROUP × TIME interactions obtained for continuous PSY variables. Standard deviations were not shown for clarity. Significant differences as detected with post hoc tests are identified with the corresponding g values (effect sizes) for between-subgroup differences and by horizontal lines for between-time differences. For example, the horizontal lines on the lower left plot indicate significantly higher FABQ-PA scores at T0 comparatively to T4, T8 and T34 as well as higher scores at T4 than at T34. FABQ-AP: fears-avoidance beliefs about physical activity; PCS: pain catastrophizing scale; B-IPQ: Brief illness perception questionnaire
Other SUBGROUP effects were observed (Table 5), but without interacting with the TIME factor, for almost all the variables related to psychological distress (PDIcog, PDIdep, PDIang, PDIsoma, PDItot). Given the absence of significant interaction, these variables were more favorable in the LIG from the start and for all measurement times, but the effect sizes were small (g between 0.20 and 0.50).
The effect of time/treatment, without interaction with the SUBGROUP factor, was also statistically significant for a majority of the continuous PSY measures investigated (Table 5), indicating improvement over time. These included all variables related to psychological distress (PDItot and scores on the five subscales) and treatment expectations, although post-hoc analyses did not reach statistical significance for the latter. Effect sizes at T8 (relative to T0) were strong (g between − 0.93 and − 1.16) for FABQ-AP, PCS and B-IPQ.
Discussion
The main findings of the present study indicate that participants in the LIG showed greater improvements than those in the SIG, both with regard to the physical factors targeted by this specific exercise program and in some psychological factors known to potentially influence clinical outcomes. Taken together, these findings support our hypotheses and suggest that both physical and psychological variables may have influenced the improvement in back pain related disability (ODI).
Ideally, mediation analyses are conducted to confirm the presence of mechanisms of benefit of a given treatment, provided that a randomized controlled trial (RCT) design is used so the intervention-outcome and intervention mediator effects can be assumed to be unconfounded [14]. As concluded in a recent review on this topic [64], very few RCTs have evaluated the mechanisms of benefit underlying different exercise programs in participants with chronic LBP. Although the present study is not an RCT, it does allow, through the comparison of large-improvement (LIG) and small-improvement (SIG) subgroups, to test specific hypotheses related to the variables that may contribute to clinical improvement during a LSEP. This study design did not include randomization, so it cannot be ascertained if all potential confounders were equivalent between our LIG and SIG. However, it should be recalled that this study adopted a per-protocol approach, which is good practice for CPR development. In other words, participants who failed to attend clinical appointments were rejected, representing seven cases here [13]. Even home-exercise adherence was equivalent between groups at T8 and T34, rejecting adherence as a potential mediating factor. Also, these groups were equivalent at baseline for general characteristics (demographic, anthropometric), clinical outcome measures (ODI, NPRS, StarTBack) as well as for all variables (physical and psychological) tested. Of particular note, the groups were equivalent at baseline for the StartBack screening tool, an aggregate measure of the most recognized prognostic factors for LBP disability.
Although the subgroups were determined on the basis of self-reported disability, a greater decrease in pain symptoms was also observed in the LIG than in the SIG during the LSEP and up to the six-month follow-up. Consistent with these results, the proportion of LIG participants having pain during physical activity (ActRelPain) significantly decreased over time, contrary to the SIG. Therefore, although the targeted physical and psychological variables were related to self-reported disability in the present study, it might be expected that similar findings would be observed if pain intensity was used as the clinical outcome measure.
Physical assessment (PHY measures)
Participants in the LIG showed a reduction in symptoms with several PHY measures intended to provoke pain through movement (MCI tests, ASLR and PSLR tests, PLE test), and in aberrant movements, while similar improvements were not seen in the SIG (Table 4). These findings confirm our hypotheses concerning Class-A variables, namely that the LIG would show more improvement in these variables than the SIG as the LSEP is theoretically designed to improve these Class-A variables. We did not assess spine motion during pain-provocation tests and, as such, cannot conclude that any improvements were related to spine motion. To the authors knowledge, only one study looked at the effect of a similar LSEPs (reported as a Pilates program; twice a week during six months) on lumbar MCI tests [65]. After the intervention, lumbar MCI decreased more in the exercise group compared to the non-exercise group, which concurs with the present findings, but their MCI tests looked at signs, not symptoms. The present findings do, however, fit with the theoretical foundation for LSEPs, which aim to improve the dynamic stabilization of the spine through improvements in motor coordination [66] and, potentially, in the passive properties of the paraspinal connective tissues [67, 68]. Participants who showed improvement with LSEPs may be more likely to fit at the ‘loose control’ end of a spectrum theorized by van Dieën [69, 70], suggesting that “enhancement of muscle activity” is required to optimize the loading of spine tissues (potentially a source of pain provocation) in these participants. In other words, there would be an association among improved motor control and reduction in abnormal tissue loading, which, in turn, allows tissue repair or healing. With improved tissue healing, the patient is able to move about more freely, thus reducing disability. Effectively, it is thought that tissue repair would be possible by a better control of the relative movement between the lumbar vertebrae during the treatment, avoiding the exacerbation of the lesions at the source of the LBP and thus allowing the time necessary for this repair [71]. Unfortunately, tissue repair remains to be demonstrated and there is no way to measure these intervertebral movements, which makes this hypothesis untested.
The LIG improved more than the SIG regarding several physical tests requiring maximal performance of the participants (PPT and TME variables) (Table 3; Fig. 2). These results support the hypothesis that a LSEP improves muscular fitness, at least in terms of endurance (TME variables) and possibly in terms of muscle coordination and power (PPT variables), and that these improvements are associated with treatment success. Several studies demonstrate the positive effect of a LSEP on trunk muscle endurance [72,73,74,75]. Given that these performance measures could be influenced by pain-related psychological variables (PCS, FABQ-AP), additional correlational analyses were performed to assess this possibility. Yet, statistically significant (P < 0.05) but weak correlations were obtained between ∆OSW (∆ = T8-T0) and the ∆PPT (r = 0.21 to 0.35) and ∆TME-Back (r = -0.31) variables, but these correlations were only slightly decreased (by 0.03 to 0.10 points) when adjusting for ∆PCS or ∆FABQ-AP, thus rejecting this possibility. These positive results are at odds with the conclusion of a systematic review that investigated the correlation between changes observed with different performance measures (strength, mobility, endurance) and observed clinical changes (pain, perceived disabilities) during different exercise programs [76]. Their overall conclusion was that their results do not support the notion that the clinical effects of exercise therapy are directly attributable to changes in the musculoskeletal system. Strength was not directly measured in the present study but no study had related endurance to self-reported disability in this review [76]. It is possible that our approach of contrasting two very different subgroups (excluding the “clinical improvement” subgroup lying in between) may have made the results more noticeable. On the other hand, the study of our mobility measures led to the same conclusion as the Steiger, Wirth [76] review, as discussed in the next paragraph.
The lack of a significant interaction for the ROM measures (Table 3) demonstrates that although an improvement in mobility was observed during the LSEP (hip flexion and internal rotation, lumbar lateral flexion), this would not be associated with LSEP success. This is not surprising as there is no scientific evidence establishing a relationship between mobility and lumbar instability, which also explains why LSEP do not include mobility exercises. In other words, these results confirm our hypotheses concerning these Class-C variables, namely that the LIG would not show more improvement in these variables than the SIG given that the LSEP is not theoretically designed to improve these Class-C variables. However, a meta-analysis showed that trunk-focussed exercises, which encompass motor control / core stabilization, strength/resistance and flexibility of the trunk, generated improvements in the trunk (lumbar or hip) ROM that were associated with a reduction in pain and disability [77], suggesting that LSEP should be combined with trunk flexibility exercises to further improve clinical outcomes.
Psychological assessment (PSY measures)
The magnitude of treatment effects varied as a function of scores on measures (FABQ-AP, PCS, B-IPQ) of pain-related psychological variables (Table 5; Fig. 4), revealing greater improvement in the LIG compared with the SIG. These findings confirm our hypotheses concerning these Class-B variables, namely that the LIG would show more improvement in these variables than the SIG as the LSEP is theoretically designed to indirectly improve these Class-B variables. Whereas the subgroups were equivalent at T0 in all of these cases, a gap widened between them from one measurement time to the next (T4 and T8) and stabilized at the 6-month follow-up (T34), with effect sizes exceeding the thresholds of 0.5 (average) and 0.8 (strong) in several cases. However, it is important to remember that these effects are probably not specific to a LSEP, i.e., they are possible for any type of exercise program as well as for some non-exercise interventions.
The LIG showed a greater decrease in their fears and beliefs about physical activity (FABQ-AP) and in pain catastrophizing (PCS) than the SIG. This supports the idea that LSEP allows for very gradual exposure to activity, beginning with motor control exercises, that is conducive to reducing pain and movement-related fears, as proposed by the fear-avoidance model [47] and as demonstrated for different exercise programs [78,79,80,81].
These variables have rarely been considered to study the effects of an LSEP. No effects on FABQ-AP had been detected following a LSEP inspired by the Australian approach [82, 83]; thus, the effects observed here and in another study [84] may possibly be attributable to the development of trunk muscle endurance (20–30 repetitions) that characterizes the McGill approach, as the present LSEP combines both schools of thought. Moreover, FABQ-AP was selected in one of the predictive models (model 9; FABQ-AP ≥ 6.5/24) tested to develop the CPR for success that we have recently derived [13] and the CPR for failure (FABQ-AP < 9/24) of Hicks, Fritz [11], both underlying LSEPs with a component emphasizing the development of trunk muscle endurance. This component is not trivial because lumbar stabilization exercises do not contain vigorous physical activities, nor do they contain movements other than the adoption of static lumbar postures in a prolonged and constrained (neutral spine posture) manner. Effectively, these exercises promote the control of the lumbar spine in a neutral posture, which could have been interpreted by the participants as a way to limit lumbar movements and physical activity. This, in turn, would have had the potential to heighten the fears and beliefs about physical activity, but the opposite was fortunately observed here. It thus appears that the load imposed on the lumbar structures (including the muscles) during the various postures, when maintained in such a way as to develop muscular endurance, would be sufficient to induce a shift in cognition and then, a decrease of these fears. This hypothesis is supported by the positive effects also observed on FABQ-AP [78, 85] and PCS [78], up to the 6-monh follow-up, following a Pilates exercise program, a form of exercise very comparable to the present LSEP. Taulaniemi, Kankaanpaa [85] hypothesized that this slowly progressing Pilates-type programme provides “safe” movement control, which in turn might give the participants positive experiences of movement (or decreased threat perception). Studies with longer-term follow-up would test whether this experience of success is sufficient for these participants, after eventually stopping their home exercises, to resume these exercises on their own, if these fear-avoidance beliefs are still no longer a barrier. To resume the LSEP, participants probably also need to feel competent enough to do the exercises by themselves. Unfortunately, only self-efficacy to overcome barriers to exercise was measured in the present study (not reported here as not relevant), not self-efficacy to perform the stabilization exercises per se.
Illness perceptions (B-IPQ) showed the same pattern as FABQ-PA and PCS, showing more improvement in the LIG than the SIG. Interestingly, a previous exploratory study on home exercise adherence revealed that illness perceptions was predictive of the global rating of change (GROC) measured at T8 and T34, which in turn was the main predictor of home exercise adherence measured at T34 [86]. More specifically, negative illness perceptions were associated with a lower GROC. GROC represents the fourth stage of the common-sense self-regulatory model [48], a model that appears well suited to predict adherence behaviours [87]. This fourth stage consist of the appraisal to help them decide whether they were closer to their goal (e.g., recovery or managing pain) or not.
Illness perceptions are not typically assessed in research examining the effects of exercise programs. To exclude the possibility that the observed effect was explained only by the effect also observed on pain intensity, the correlation between ∆B-IPQ (T8-T0) and ∆ODI was calculated (n = 105 participants) without and with adjustment for ∆NPRS, and the correlations, always significant (P < 0.001), were 0.53 and 0.41, respectively. Thus, the effect on these perceptions goes beyond symptom improvement and appears to play a role in adherence to the home-based LSEP, as discussed earlier.
Study limitations
As mentioned above, the study design and statistical model used for this study cannot confirm the direction of causality among study variables. Another important limitation is that several dependent variables were tested, raising the risk of generating type I statistical errors (false positive). Consequently, these findings should be interpreted with caution as some of the statistically significant differences (possibly 5%) may have occurred by chance. However, the fact that the results were consistent across several measures lends them a certain credibility, although it might be expected that some measures (e.g., TME measures) or concepts (e.g. fear-avoidance and pain catastrophizing; PDI subscales and total scores) may share some common variance, which may at least partly explain these consistent findings. It’s also worth noting that most participants (98%) suffered from chronic pain (3 months or more), and that a large proportion of the sample (49%) had been experiencing pain for more than five years. Consequently, the findings of this study might not be generalizable to individuals experiencing more acute ( < less than 4 weeks) or subacute (4–12 weeks) pain. In spite of these limitations, the present study showed novel and consistent (across several measures) findings suggesting that both physical and psychological factors may have influenced the improvement in back pain related disability following a LSEP. Future research should further investigate these potential mechanisms of benefit using a RCT study design and mediation analyses, allowing more definitive conclusions to be drawn, in terms of causality, and better informing clinical intervention.
Conclusions
The large-improvement subgroup showed more improvement than the small-improvement subgroup with regard to physical factors typically targeted by this specific exercise program as well as for psychological factors that are known to influence clinical outcomes. Taken together, these findings suggest that a lumbar stabilization exercise program may have influenced the improvement in back pain related disability (ODI) by improving different physical and psychological factors.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–67.
Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–83.
Hayden JA, van Tulder MW, Malmivaara AV, Koes BW. Meta-analysis: exercise therapy for nonspecific low back pain. Ann Intern Med. 2005;142(9):765–75.
Smith BE, Littlewood C, May S. An update of stabilisation exercises for low back pain: a systematic review with meta-analysis. BMC Musculoskelet Disord. 2014;15(1):416.
Barr KP, Griggs M, Cadby T. Lumbar stabilization: a review of core concepts and current literature, part 2. Am J Phys Med Rehabil. 2007;86(1):72–80.
McGill S. Low back disorders. Evidence-based prevention and rehabilitation. 1st ed. Champaign, U.S.A.: Human Kinetics; 2002 2002.
Richardson C, Hodges P, Hides J. Therapeutic exercise for lumbopelvic stabilization. 2eds ed. Sydney: Churchill Livingstone; 2004 2004.
Owen PJ, Miller CT, Mundell NL, Verswijveren S, Tagliaferri SD, Brisby H, et al. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br J Sports Med. 2020;54(21):1279–87.
Searle A, Spink M, Ho A, Chuter V. Exercise interventions for the treatment of chronic low back pain: a systematic review and meta-analysis of randomised controlled trials. Clin Rehabil. 2015.
Saragiotto BT, Maher CG, Yamato TP, Costa LO, Costa LC, Ostelo RW, et al. Motor Control Exercise for nonspecific low back Pain: a Cochrane Review. Spine (Phila Pa 1976). 2016;41(16):1284–95.
Hicks GE, Fritz JM, Delitto A, McGill SM. Preliminary development of a clinical prediction rule for determining which patients with low back pain will respond to a stabilization exercise program. Arch Phys Med Rehabil. 2005;86(9):1753–62.
Rabin A, Shashua A, Pizem K, Dickstein R, Dar G. A clinical prediction rule to identify patients with low back pain who are likely to experience short-term success following lumbar stabilization exercises: a randomized controlled validation study. J Orthop Sports Phys Ther. 2014;44(1):6–B13.
Larivière C, Rabhi K, Preuss R, Coutu MF, Roy N, Henry SM. Derivation of clinical prediction rules for identifying patients with non-acute low back pain who respond best to a lumbar stabilization exercise program at post-treatment and six-month follow-up. PLoS ONE. 2022;17(4):e0265970.
Lee H, Herbert RD, McAuley JH. Mediation Anal JAMA. 2019;321(7):697–8.
Fairbank JCT, Couper J, Davies J, O’Brien J. The Oswestry low back pain disability questionnaire. Physiotherapy. 1980;66(8):271–3.
Ostelo RW, Deyo RA, Stratford P, Waddell G, Croft P, Von Korff M, et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine. 2008;33(1):90–4.
Boucher JA, Preuss R, Henry SM, Dumas JP, Lariviere C. The effects of an 8-week stabilization exercise program on lumbar movement sense in patients with low back pain. BMC Musculoskelet Disord. 2016;17(1):23.
Burton AK, Waddell G, Tillotson KM, Summerton N. Information and advice to patients with back pain can have a positive effect. A randomized controlled trial of a novel educational booklet in primary care. Spine (Phila Pa 1976). 1999;24(23):2484–91.
Jordan JL, Holden MA, Mason EEJ, Foster NE. Interventions to improve adherence to exercise for chronic musculoskeletal pain in adults (Review). Cochrane Database Systematic Review; 2010 2010. Contract No.: CD005956.
Haynes RBS. D.L. Compliance in health care. Baltimore: Johns Hopkins University; 1979.
Fairbank JCT, Pynsent PB. The Oswestry Disability Index. Spine. 2000;25(22):2940–52.
Childs JD, Piva SR, Fritz JM. Responsiveness of the numeric pain rating scale in patients with low back pain. Spine. 2005;30(11):1331–4.
Damsgard E, Thrane G, Anke A, Fors T, Røe C. Activity-related pain in patients with chronic musculoskeletal disorders. Disabil Rehabil. 2010;32(17):1428–37.
Hill JC, Dunn KM, Lewis M, Mullis R, Main CJ, Foster NE, et al. A primary care back pain screening tool: identifying patient subgroups for initial treatment. Arthritis Rheum. 2008;59(5):632–41.
Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A fear-avoidance beliefs questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52(2):157–68.
Sullivan MJL, Bishop SR, Pivik J. The Pain Catastrophizing Scale: Development and validation. Psychol Assess. 1995;7(4):524–32.
Ilfeld FWJ. Further validation of a psychiatric symptom index in a normal population. Psychol Rep. 1976;39(3f):1215–28.
Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception Questionnaire. J Psychosom Res. 2006;60(6):631–7.
Baecke JAH, Burema J, Frijters JER. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr. 1982;36(5):936–42.
Resnick B, Zimmerman SI, Orwig D, Furstenberg A-L, Magaziner J. Outcome expectations for Exercise Scale: Utility and Psychometrics. J Gerontol B Psychol Sci Soc Sci. 2000;55(6):S352–6.
Waddell G. Clinical evaluation of disability in low back pain. In: Frymoyer JW, editor. The adult spine: principles and practice. 2nd ed. Philadelphia: Lippincott-Raven; 1997. pp. 171–83.
Mens JM, Vleeming A, Snijders CJ, Koes BW, Stam HJ. Reliability and validity of the active straight leg raise test in posterior pelvic pain since pregnancy. Spine (Phila Pa 1976). 2001;26(10):1167–71.
Ng JK, Kippers V, Richardson CA, Parnianpour M. Range of motion and lordosis of the lumbar spine: reliability of measurement and normative values. Spine. 2001;26(1):53–60.
Saur PMM, Ensink RBM, Frese K, Seeger D, Hildebrandt J. Lumbar range of motion: reliability and validity of the inclinometer technique in the clinical measurement of trunk flexibility. Spine. 1996;21(11):1332–8.
Waddell G, Somerville D, Henderson I, Newton M. Objective clinical evaluation of physical impairment in chronic low back pain. Spine (Phila Pa 1976). 1992;17(6):617–28.
Stanton TR, Fritz JM, Hancock MJ, Latimer J, Maher CG, Wand BM, et al. Evaluation of a treatment-based classification algorithm for low back pain: a cross-sectional study. Phys Ther. 2011;91(4):496–509.
Kasai Y, Morishita K, Kawakita E, Kondo T, Uchida A. A new evaluation method for lumbar spinal instability: passive lumbar extension test. Phys Ther. 2006;86(12):1661–7.
Van Dillen LR, Sahrmann SA, Norton BJ, Caldwell CA, McDonnell MK, Bloom NJ. Movement system impairment-based categories for low back pain: stage 1 validation. J Orthop Sports Phys Ther. 2003;33(3):126–42.
Van Dillen LR, Sahrmann SA, Caldwell CA, McDonnell MK, Bloom N, Norton BJ. Trunk rotation-related impairments in people with low back pain who participated in 2 different types of leisure activities: a secondary analysis. J Orthop Sports Phys Ther. 2006;36(2):58–71.
Van Dillen LR, Sahrmann SA, Norton BJ, Caldwell CA, Fleming D, McDonnell MK, et al. Effect of active limb movements on symptoms in patients with low back pain. J Orthop Sports Phys Ther. 2001;31(8):402–13.
Hicks GE, Fritz JM, Delitto A, Mishock J. Interrater reliability of clinical examination measures for identification of lumbar segmental instability. Arch Phys Med Rehabil. 2003;84(12):1858–64.
Novy DM, Simmonds MJ, Lee CE. Physical performance tasks: what are the underlying constructs? Arch Phys Med Rehabil. 2002;83(1):44–7.
McGill SM, Childs A, Liebenson C. Endurance times of low back stabilization exercises: clinical targets for testing and training from a normal database. Arch Phys Med Rehabil. 1999;80(8):941–4.
Ito T, Shirado O, Suzuki H, Takahashi M, Kaneda K, Strax TE. Lumbar trunk muscle endurance testing: an inexpensive alternative to a machine for evaluation. Arch Phys Med Rehabil. 1996;77:75–9.
Panjabi MM. The stabilizing system of the spine. Part I. function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383–9.
Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J Spinal Disord. 1992;5(4):390–7.
Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–32.
Leventhal H. The role of theory in the study of compliance to high blood pressure regimens. In: Haynes BRM, Tilmer ME, O.E., editors. Patient compliance to prescribed antihypertensive medication regimens: a report to the National Heart Lung and Blood Institute. Washington DC: National Heart, Lung, and Blood Institute; 1980.
Leventhal H, Owa RD, Brissette I. The common-sense model of self-regulation of health and illness. The self-regulation of health and illness behaviour. Routledge; 2012. pp. 56–79.
Coutu M-F, Marchand A, Dupuis G, O’Connor K, Turgeon L, Nielson T. Une piste pour favoriser l’adhésion Au plan de soins. Revue francophone de clinique comportementale et Cogn. 2004;9(4):17–24.
Hicks GE, Benvenuti F, Fiaschi V, Lombardi B, Segenni L, Stuart M, et al. Adherence to a community-based exercise program is a strong predictor of improved back pain status in older adults: an observational study. Clin J Pain. 2012;28(3):195–203.
Mannion AF, Helbling D, Pulkovski N, Sprott H. Spinal segmental stabilisation exercises for chronic low back pain: programme adherence and its influence on clinical outcome. Eur Spine J. 2009;18(12):1881–91.
Denteneer L, Stassijns G, De Hertogh W, Truijen S, Van Daele U. Inter- and intrarater reliability of clinical tests Associated with functional lumbar Segmental Instability and Motor Control Impairment in patients with Low Back Pain: a systematic review. Arch Phys Med Rehabil. 2017;98(1):151–64.e6.
Ferrari S, Manni T, Bonetti F, Villafane JH, Vanti C. A literature review of clinical tests for lumbar instability in low back pain: validity and applicability in clinical practice. Chiropr Man Ther. 2015;23:14.
Alqarni AM, Schneiders AG, Hendrick PA. Clinical tests to diagnose lumbar segmental instability: a systematic review. J Orthop Sports Phys Ther. 2011;41(3):130–40.
Van Dillen LR, Sahrmann SA, Norton BJ, Caldwell CA, Fleming DA, McDonnell MK, et al. Reliability of physical examination items used for classification of patients with low back pain. Phys Ther. 1998;78(9):979–88.
Hall AM, Ferreira PH, Maher CG, Latimer J, Ferreira ML. The influence of the therapist-patient relationship on treatment outcome in physical rehabilitation: a systematic review. Phys Ther. 2010;90(8):1099–110.
Jack K, McLean SM, Moffett JK, Gardiner E. Barriers to treatment adherence in physiotherapy outpatient clinics: a systematic review. ManTher. 2010;15(3):220–8.
Beinart NA, Goodchild CE, Weinman JA, Ayis S, Godfrey EL. Individual and intervention-related factors associated with adherence to home exercise in chronic low back pain: a systematic review. Spine J. 2013;13(12):1940–50.
Thompson E, Broadbent J, Bertino MD, Staiger PK. Do Pain-related beliefs influence treatment adherence? A systematic review. Clin J Pain. 2015.
Fritz JM, Hebert J, Koppenhaver S, Parent E. Beyond minimally important change: defining a successful outcome of physical therapy for patients with low back pain. Spine (Phila Pa 1976). 2009;34(25):2803–9.
Lakens D. Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Front Psychol. 2013;4:863.
Deyo RA, Dworkin SF, Amtmann D, Andersson G, Borenstein D, Carragee E, et al. Report of the NIH Task Force on Research Standards for Chronic Low Back Pain. Phys Ther. 2015;95(2):e1–18.
Wun A, Kollias P, Jeong H, Rizzo RR, Cashin AG, Bagg MK, et al. Why is exercise prescribed for people with chronic low back pain? A review of the mechanisms of benefit proposed by clinical trialists. Musculoskelet Sci Pract. 2020;51:102307.
Taulaniemi A, Kankaanpaa M, Tokola K, Parkkari J, Suni JH. Neuromuscular exercise reduces low back pain intensity and improves physical functioning in nursing duties among female healthcare workers; secondary analysis of a randomised controlled trial. BMC Musculoskelet Disord. 2019;20(1):328.
Tsao H, Galea MP, Hodges PW. Driving plasticity in the motor cortex in recurrent low back pain. Eur J Pain. 2010;14(8):832–9.
Lariviere C, Henry SM, Preuss R. Structural remodeling of the lumbar multifidus, thoracolumbar fascia and lateral abdominal wall perimuscular connective tissues: a search for its potential determinants. J Anat. 2021;238(3):536–50.
Reeves ND. Adaptation of the tendon to mechanical usage. J Musculoskelet Neuronal Interact. 2006;6(2):174–80.
van Dieen JH, Reeves NP, Kawchuk G, van Dillen LR, Hodges PW. Analysis of Motor Control in patients with Low Back Pain: a key to Personalized Care? J Orthop Sports Phys Ther. 2019;49(6):380–8.
van Dieen JH, Reeves NP, Kawchuk G, van Dillen LR, Hodges PW. Motor Control Changes in Low Back Pain: divergence in presentations and mechanisms. J Orthop Sports Phys Ther. 2019;49(6):370–9.
McGill SM. Low back exercises: evidence for improving exercise regimens. Phys Ther. 1998;78(7):754–65.
Gopika S, Dinakaran R. Effect of eight-week core stabilization program on core muscle endurance and function in female staff nurses. Natl J Physiol Pharm Pharmacol. 2017:1.
Sandrey MA, Mitzel JG. Improvement in dynamic balance and core endurance after a 6-week core-stability-training program in high school track and field athletes. J Sport Rehabil. 2013;22(4):264–71.
Hoppes CW, Sperier AD, Hopkins CF, Griffiths BD, Principe MF, Schnall BL, et al. The efficacy of an Eight-Week Core Stabilization Program on core muscle function and endurance: a Randomized Trial. Int J Sports Phys Ther. 2016;11(4):507–19.
Javadian Y, Behtash H, Akbari M, Taghipour-Darzi M, Zekavat H. The effects of stabilizing exercises on pain and disability of patients with lumbar segmental instability. J Back Musculoskelet Rehabil. 2012;25(3):149–55.
Steiger F, Wirth B, de Bruin ED, Mannion AF. Is a positive clinical outcome after exercise therapy for chronic non-specific low back pain contingent upon a corresponding improvement in the targeted aspect(s) of performance? A systematic review. Eur Spine J. 2012;21(4):575–98.
Prat-Luri A, de Los Rios-Calonge J, Moreno-Navarro P, Manresa-Rocamora A, Vera-Garcia FJ, Barbado D. Effect of trunk-focused exercises on pain, disability, quality of life and trunk physical fitness in low back pain and how potential effect modifiers modulate their effects: a systematic review with meta-analyses. J Orthop Sports Phys Therapy. 2023(0):1–26.
Marshall PW, Kennedy S, Brooks C, Lonsdale C. Pilates exercise or stationary cycling for chronic nonspecific low back pain: does it matter? A randomized controlled trial with 6-month follow-up. Spine (Phila Pa 1976). 2013;38(15):E952–9.
Mannion AF, Muntener M, Taimela S, Dvorak J. A randomized clinical trial of three active therapies for chronic low back pain. Spine. 1999;24(23):2435–48.
Smeets RJ, Vlaeyen JW, Kester AD, Knottnerus JA. Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J Pain. 2006;7(4):261–71.
Woby SR, Watson PJ, Roach NK, Urmston M. Are changes in fear-avoidance beliefs, catastrophizing, and appraisals of control, predictive of changes in chronic low back pain and disability? EurJPain. 2004;8(3):201–10.
Unsgaard-Tondel M, Fladmark AM, Salvesen O, Vasseljen O. Motor control exercises, sling exercises, and general exercises for patients with chronic low back pain: a randomized controlled trial with 1-year follow-up. Phys Ther. 2010;90(10):1426–40.
Lee HS, Kim DJ, Oh Y, Min K, Ryu JS. The effect of individualized gradable stabilization exercises in patients with chronic low back pain: case-control study. J Back Musculoskelet Rehabil. 2016;29(3):603–10.
Alrwaily M, Schneider M, Sowa G, Timko M, Whitney SL, Delitto A. Stabilization exercises combined with neuromuscular electrical stimulation for patients with chronic low back pain: a randomized controlled trial. Braz J Phys Ther. 2019;23(6):506–15.
Taulaniemi A, Kankaanpaa M, Rinne M, Tokola K, Parkkari J, Suni JH. Fear-avoidance beliefs are associated with exercise adherence: secondary analysis of a randomised controlled trial (RCT) among female healthcare workers with recurrent low back pain. BMC Sports Sci Med Rehabil. 2020;12:28.
L’Heureux J, Coutu M-F, Berbiche D, Larivière C. Adherence to a home exercise programme following a clinical programme for non-acute non-specific low back pain: an exploratory study. Eur J Physiotherapy. 2019;22(5):299–308.
Jones CJ, Smith HE, Llewellyn CD. A systematic review of the effectiveness of interventions using the common sense Self-Regulatory Model to improve adherence behaviours. J Health Psychol. 2016;21(11):2709–24.
Acknowledgements
The authors would like to thank Sophie Bellefeuille, Marilee Nugent, Cynthia Appleby, Mélanie Clavet and Amir Chitour for data collection, Michel Goyette and Daniel Marineau for technical assistance in the laboratory, as well as Hakim Mecheri for data management preceding statistical analyses. Thanks to Khalil Rabhi, biostatistician, for his advice on statistical analysis. This project would not have been possible without the participation of eight private PhysioExtra clinics in the Montreal area.
Funding
This study was funded [#2010-0022 and #2016-0013) by the Institut de recherche Robert-Sauvé en santé et en sécurité du travail (IRSST), located in Montreal, Canada.
Author information
Authors and Affiliations
Contributions
Conception and design of the work: CL, RP, M-FC, SMH, MJS. Acquisition and analysis: CL, NR. Interpretation of data: CL, RP, M-FC, NR, SMH, MJS. Writing – review & editing: CL, RP, M-FC, NR, SMH, MJS. Approved the submitted version: CL, RP, M-FC, NR, SMH, MJS. Agreed to be personally accountable for the author’s own contributions and ensured the accuracy or integrity of any part of the work: CL, RP, M-FC, NR, SMH, MJS.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures and the informed written consent were approved by the ethics committees of the Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal (CRIR). Ethical registration numbers: CRIR-738-0512 and CRIR-1315-0318 for preliminary and final studies, respectively. Informed consent to participate in the study was obtained from all participants.
Consent for publication
Informed consent for publication of identifiable information/ images in open access journal was obtained from all study participants.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Larivière, C., Preuss, R., Coutu, MF. et al. Disability reduction following a lumbar stabilization exercise program for low back pain: large vs. small improvement subgroup analyses of physical and psychological variables. BMC Musculoskelet Disord 25, 358 (2024). https://doi.org/10.1186/s12891-024-07480-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07480-4